
Abstract
Objective
To evaluate and compare the maxillary sinus volume (MSV) and its linear measurements in patients with unilateral cleft lip and palate (UCLP).
Design
Retrospective cohort study.
Results
MSV was smaller on the cleft side (mean = 10607 mm3, SD = 3538 vs. mean 9864 mm3, SD = 3243, p = .03). The volume of the anterior part of the sinus was smaller on the cleft side (median = 4659 mm3, IQR = 3687–6055 vs. median 3368 mm3, IQR = 2693–5352, p = .001), whereas the posterior part volume was not. The linear measurements (maximum length, width and height) did not reveal significant difference between the cleft and the non-cleft side (entire sinus – anterior - posterior parts). The anterior/posterior height ratio was smaller on the cleft side (mean = 0.991, SD = 0.091 vs. mean 0.931, SD = 0.106, p < .001).
Conclusion
The MSV is significantly smaller on the cleft side in young patients with UCLP. This hypoplasia is significantly associated with the anterior part of the maxillary sinus. Additionally, there are indications of a restricted vertical development of the maxillary sinus on the cleft side.
Keywords
Introduction
Cleft lip and palate (CLP) is one of the most significant and prevalent congenital maxillofacial anomalies. A recent study 1 evaluating data from 22 population- and hospital-based surveillance programs affiliated with the International Clearinghouse for Birth Defects Surveillance and Research (ICBDSR) across 18 countries reported a pooled prevalence of 6.4 cases of CLP per 10,000 births. CLP results from failure of fusion among the medial nasal process, the palatal process, and the maxillary process during early fetal development. The medial nasal process is responsible for development of the anterior portion of the maxilla and other midfacial structures. 2 The maxillary sinus (MS), derived from mesodermal structures of the first branchial arch, begins development during the third week of gestation and continues through puberty. Its functions include reducing skull weight, contributing to speech resonance, warming and humidifying inspired air, and absorbing traumatic forces to protect adjacent sensory organs. 3
Studies have shown that alterations of the midfacial structures are common among individuals with cleft lip and palate. 4 The anatomic and functional characteristics associated with CLP present multiple challenges related to medical, dental, and speech care, as affected individuals often experience difficulties related to nutrition, speech, hearing, chronic upper airway infections, dentition, facial morphology, and psychosocial well-being. 5 Furthermore, studies specifically investigating patients with unilateral cleft lip and palate (UCLP) have demonstrated not only that sinus disease, particularly sinusitis, is common in these patients,5–7 but also that individuals with UCLP exhibit a significantly higher incidence of maxillary sinus mucosal thickening compared with non-cleft controls. 8 An additional alteration observed in patients with UCLP is a higher incidence of nasal septal deviation compared with non-cleft controls.9,10 Alterations of the midface also involve the maxilla, which demonstrates reduced depth, length, height, and volume on the cleft side, 11 contributing to the characteristic deformities of alar base depression, alar flaring, and nasal asymmetry.
Individuals with CLP have also been postulated to exhibit maxillary sinus hypoplasia. 12 The etiology of altered maxillary sinus dimensions remains unclear. It has been suggested that, in these patients, the maxillary sinus may develop differently in utero13,14 or that feeding difficulties and altered nasal and sinus airflow may influence sinus development postnatally. 10 A recent study by Whyte and Boeddinghaus 15 concluded that marked anatomic alterations in maxillary sinus dimensions may contribute to the increased prevalence of sinus complications in individuals with cleft conditions. In this context, comparisons of sinus volumes in patients with various craniofacial clefts may be valuable for identifying potential differences relative to individuals without cleft. Moreover, differentiation in sinus volume should be considered during sinus surgery and dental implant treatment as a possible risk factor for sinus complications and may provide clinically relevant information for future treatment planning. In orthodontics, assessment of maxillary tooth movement adjacent to the sinus on the cleft side may also benefit from improved understanding of sinus morphology. Identifying volumetric differences between the cleft and non-cleft sides in individuals with UCLP may contribute further to understanding craniofacial growth, particularly in the nasomaxillary complex.
Evaluation of the complex three-dimensional anatomy of the maxillary sinus is challenging because of its irregular morphology. Historically, lateral cephalometric radiographs were commonly used for airway assessment because of their simplicity, accessibility, and low cost. However, these radiographs have important limitations, including two-dimensional representation of three-dimensional structures, distortion, reduced reproducibility due to difficulties in landmark identification, differences in magnification, and superimposition of craniofacial structures. 10 Therefore, their validity for evaluating the craniofacial complex is questionable compared with three-dimensional imaging using computed tomography (CT) and cone-beam computed tomography (CBCT). CBCT has become the diagnostic modality of choice because of its lower radiation dose, as well as its greater time- and cost-effectiveness compared with conventional CT.
The maxillary sinus is a three-dimensional, irregularly shaped anatomical structure. Consequently, linear measurements of this morphologically complex entity do not provide a reliable estimate of its true size. For this reason, volumetric assessment has been selected in the relevant literature as a more appropriate indicator of sinus variation in patients with UCLP.5,13,16,17 Furthermore, variation in the anterior-to-posterior volumetric ratio of the maxillary sinus in patients with UCLP may be of particular interest for clarifying the extent of cleft-related effects on sinus morphology, considering that the anterior portion of the maxilla is predominantly affected by the cleft. Accordingly, the anterior region of the sinus may represent an anatomical site where this effect is manifested to a greater extent than in the posterior region.
In this context, volumetric comparison of anterior and posterior maxillary sinus segments may help clarify not only whether the cleft affects the maxillary sinus morphology on the cleft side, but also which region of the sinus is most affected. However, major challenges in anteroposterior segmentation of the maxillary sinus include the complexity of sinus anatomy, which may be altered by the cleft,10,18 as well as its location within the maxillary bone, distant from stable and reproducible cranial anatomical landmarks.
Thus, the objectives of this study were to evaluate and compare maxillary sinus volume (MSV) and linear measurements between the cleft and non-cleft sides in patients with UCLP using CBCT. The primary null hypothesis was that no differences exist in MSV or linear measurements between the cleft and non-cleft sides in children with UCLP. For this reason, a comprehensive three-dimensional morphological analysis was performed to evaluate the anatomical characteristics of the maxillary sinus.
Subjects and Methods
Eligibility Criteria
The inclusion criteria of patients in this study were: patients with non-syndromic UCLP; age ranged from 8 to 14 years; no history of orthodontic intervention or secondary alveolar bone grafting.
CBCT images with incomplete sinus imaging, poor quality and maxillary sinus pathology, such as odontogenic cysts, tumors, or any other types of sinus pathology, were not included in this study. Other exclusion criteria were craniofacial syndromes, previous orthodontic expansion treatment, surgical interventions to treat the sinuses, or history of trauma in the area. None of the exam referrals were specifically related to the study.
Sample Size Calculation
Sample size calculation was based on data from a previous similar study, 19 which reported a mean MSV of the non-cleft side of 16,196 mm3, with a standard deviation (SD) of 4884 mm3 and a correlation coefficient of 0.947 between cleft and non-cleft sides. Assuming a difference equal to one-fourth of the SD (1221 mm3; small effect size), a common SD, and a paired-samples t-test design, a total of 20 patients was required to detect a statistically significant difference, with α = 0.05 and 90% statistical power.
The study was approved by the Ethics Committee of the School of Dentistry, National and Kapodistrian University of Athens, Greece (Date of Approval: 04/10/2023, Protocol Number: 602). Screening of patient records (CBCT scans of individuals with unilateral cleft palate) was initiated following ethical clearance.
Patient data were retrospectively collected from the archives of the Department of Orthodontics, School of Dentistry, National and Kapodistrian University of Athens, Greece during the last quarter of 2023. All included patient files contained written informed consent signed by a parent or legal guardian at the time of treatment. Records of patients with UCLP were reviewed, and demographic data were recorded. The age range at the time of CBCT examination was 8 to 14 years. During this period, alveolar bone grafting is commonly performed, and CBCT imaging is therefore routinely indicated for treatment planning.
A total of 63 consecutive cases were reviewed, of which 20 met the inclusion criteria. Forty-three cases were excluded due to mucosal thickening, incomplete sinus visualization, or poor CBCT image quality.
Study Design
The maxillary sinus of the non-cleft side was used as an internal control. The use of matched healthy controls was avoided due to variability in craniofacial maturation and somatic growth among individuals of the same age, 20 as well as differences in imaging protocols across patients. Accordingly, the contralateral side in patients with UCLP was used to minimize interindividual variability. Based on Wang et al., 18 who reported significant differences primarily in the anterior maxilla between cleft and non-cleft sides, a similar analytical approach was adopted to determine whether the anterior, posterior, both, or neither region of the maxillary sinus is affected by CLP.
Orientation of the maxillary sinus and maxilla was standardized using a coordinate system based on stable cranial base landmarks. These landmarks were selected for their reliability, reproducibility on CBCT imaging, and relative stability during growth. The stability of the cranial base as a reference structure during craniofacial development has been confirmed in previous studies21,22 and shown to be minimally influenced by facial growth. 23 Accordingly, cranial base landmarks are widely accepted for constructing reference planes in craniofacial analysis. 22 This approach is particularly appropriate for mild to moderate craniofacial asymmetries, such as those observed in patients with UCLP. 23
Cranial Anatomic Landmarks for Orientation
Porion (Po): the most superior and lateral point of the external auditory meatus.
Orbitale (Or): the lowest point of the inferior orbital rim on the non-cleft side.
Nasion (N): the midpoint of the frontonasal suture.
Sella turcica (S): the center of the pituitary fossa.
Reference Planes for 3D Volume Orientation
Frankfort Horizontal (FH) Plane: plane passing through bilateral Porion and Orbitale on the non-cleft side.
Midsagittal (MS) Plane: plane perpendicular to the FH plane passing through Nasion and Sella.
Coronal (CR) Plane: plane perpendicular to both FH and MS planes passing through Nasion.
Following this protocol, all CBCT datasets were oriented in a standardized three-plane coordinate system.
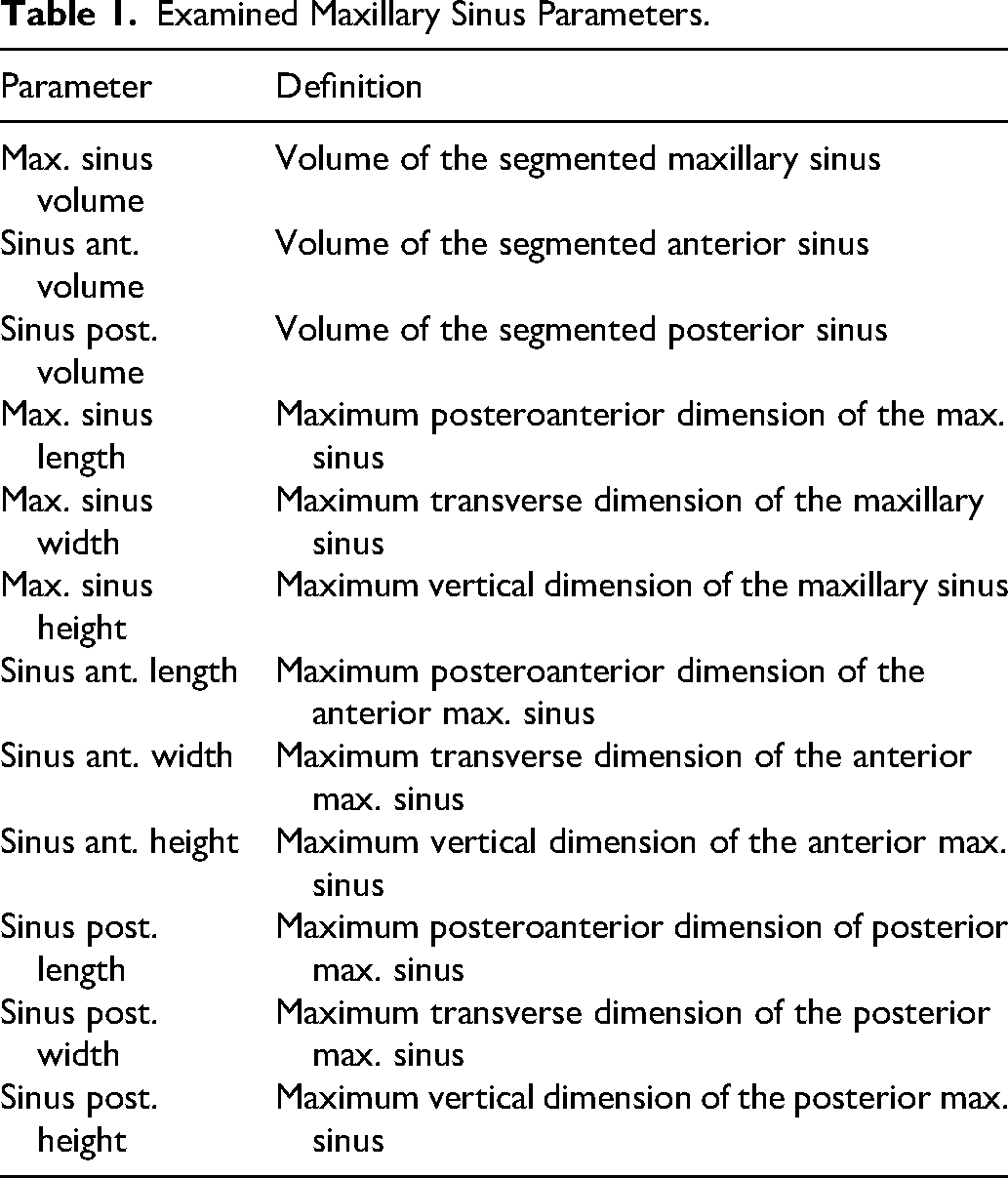
The examined parameters of the maxillary sinus are summarized in Table 1.
Examined Maxillary Sinus Parameters.
CBCT scans were acquired using a NewTom VGi unit (Verona, Italy) for presurgical assessment. The voxel size was 0.3 × 0.3 × 0.3 mm. The field of view (FOV) ranged from 8.2 cm to 15.3 cm. Eight scans (40%) had a FOV height >15 cm, while three scans (15%) had a FOV height between 10 and 15 cm.
All 20 CBCT datasets were exported in Digital Imaging and Communications in Medicine (DICOM) format and imported into Viewbox4 software (dHAL Software, version 4.1.2.1, 64-bit). Manual segmentation of the maxillary sinus was performed using editing masks and reconstruction tools. Each head was individually oriented in three dimensions according to the predefined anatomical landmarks. Each maxillary sinus was then semi-manually segmented and reconstructed.
The maxillary sinus boundary was defined at the narrowest region of the ostium between the uncinate process and the infundibulum. The software allowed manual and semi-automatic editing of segmentation boundaries. Linear measurements included maximum sinus length, width, and height.
To separate the maxillary sinus into anterior and posterior segments, the zygomaticomaxillary suture of the non-cleft side was used as a reference, as asymmetry in zygomatic projection between cleft and non-cleft sides has been previously reported. 24 A plane perpendicular to the midsagittal and axial planes was constructed and adjusted to pass through the most posterior point of the zygomaticomaxillary suture on the non-cleft side. This plane/slice was used to define anterior and posterior sinus compartments (Figures 1 and 2).
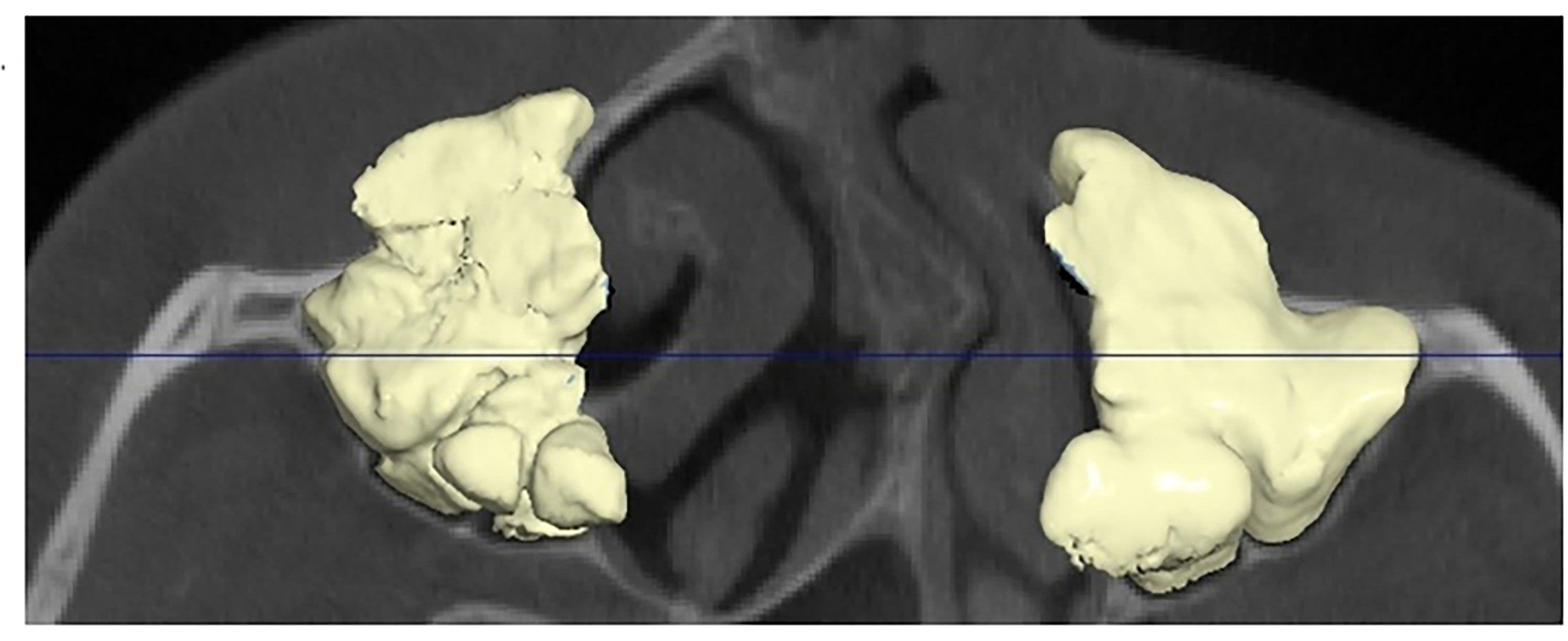
Axial view with segmented max. sinuses.
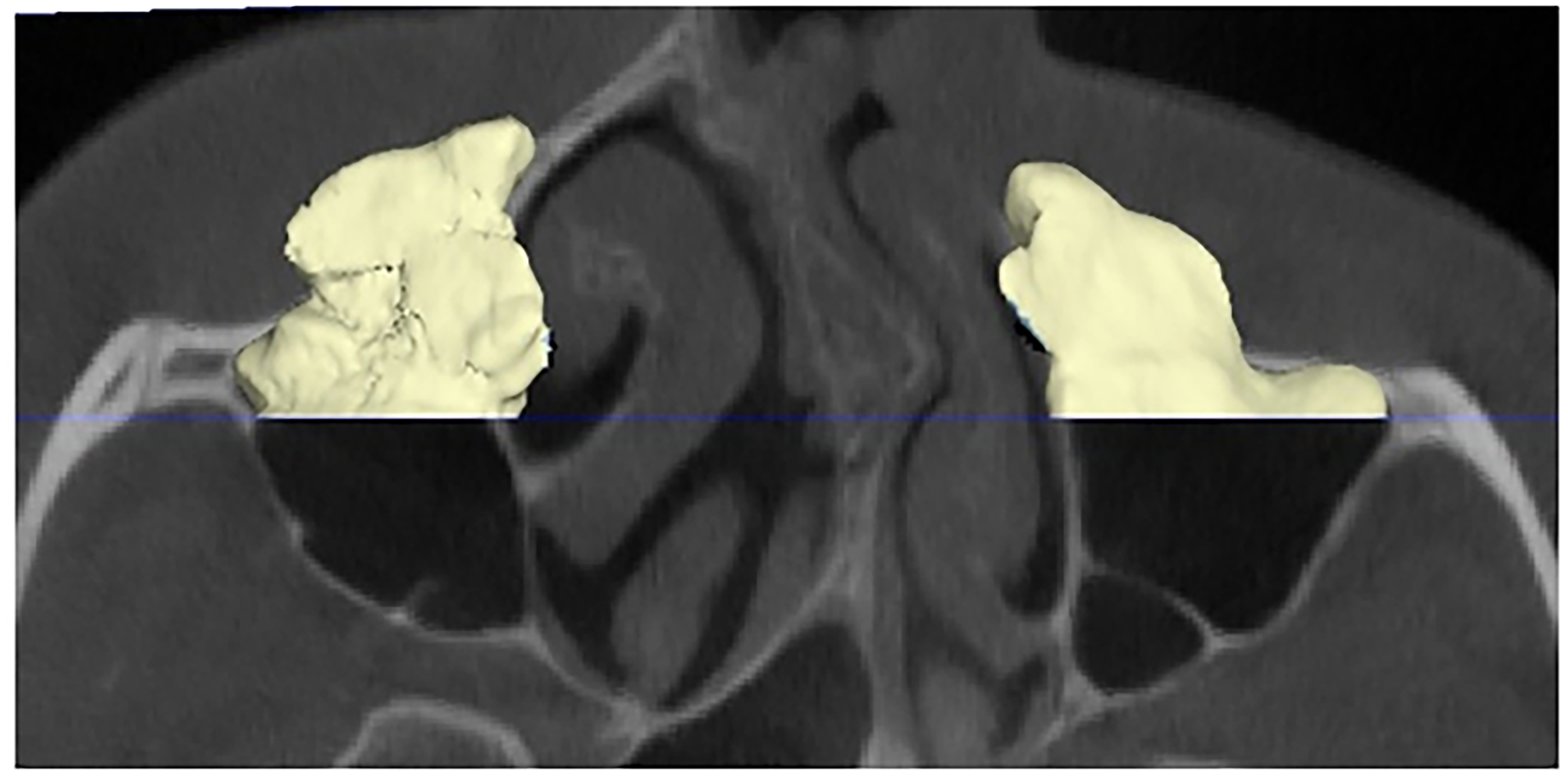
The plane/slice divides both max. sinuses into anterior and posterior sections.
All measurements and landmark placements were repeated twice at a one-month interval by a single examiner (oral radiologist, TV). Mean and median values were used for statistical analysis where appropriate.
Statistical Analysis
Descriptive statistics included absolute and relative frequencies for categorical variables, means with standard deviations (SD) for normally distributed continuous variables, and medians with interquartile ranges (IQR) for non-normally distributed variables, as determined by the Shapiro-Wilk test. Differences between cleft and non-cleft sides were analyzed using generalized linear models with robust standard errors to account for within-subject clustering for normally distributed data. For non-normally distributed variables, median regression with 1000 bootstrap replications was applied.
Intra-examiner agreement was assessed using the concordance correlation coefficient 25 and Bland-Altman limits of agreement. 26 All statistical tests were two-sided, with a significance level set at α = 0.05. Analyses were performed using Stata SE 19.5 (StataCorp, College Station, TX, USA) with an open dataset.
Results
Patients’ Demographics
In accordance with the sample size calculation, 20 images with pairs of semi-manually segmented maxillary sinuses ten male and ten females, were used for analysis. The mean age of the sample was 12.1 years, ranging from 8 to 14 years (Table 2). All CBCT scans were acquired between the years 2016 and 2023.
Characteristics of Included Patients.
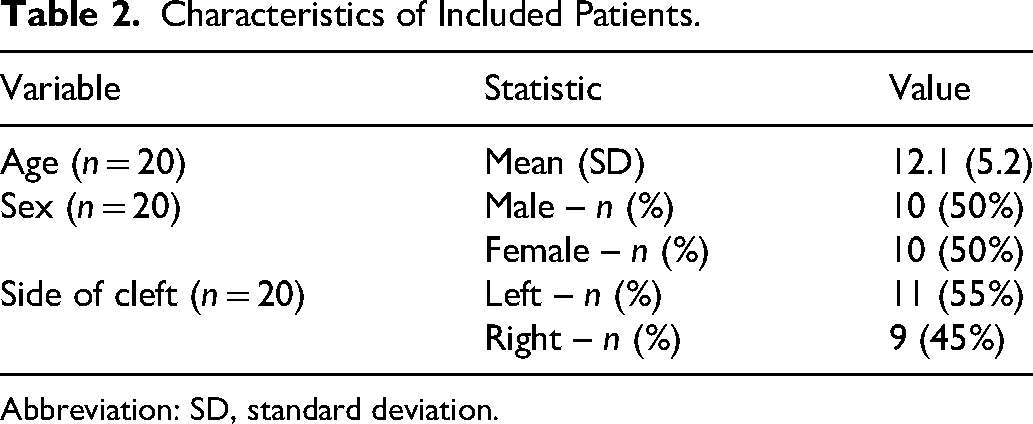
Abbreviation: SD, standard deviation.
Method Error
Repeatability and agreement were found to be excellent for the repeated intra-examiner comparisons (CCCs: 0.90–0.99) (Table 3). However, relatively broad limits of agreement were seen for the intra-examiner comparisons, hence the wide 95% CIs.
Agreement of Repeated Measurements.

Abbreviations: CCC, concordance correlation coefficient; CI, confidence interval.
Comparison of MSVs Between the Cleft and Non-Cleft Sides
A statistically significant difference was found between the mean MSV of the cleft and non-cleft sides, showing that maxillary sinus on the cleft side was significantly smaller (p = .03). A statistically significant difference was also found between the median value of the anterior MSV of the cleft and non-cleft sides, showing again that the anterior part of the maxillary sinus on the cleft side had a significantly smaller volume (p = .001), whereas the comparison of the posterior volumes of the maxillary sinuses did not give a significant result. Similarly, the comparison of the anterior/posterior ratio between the two sides resulted in a statistically significant (p = .03) outcome (Table 4).
Dimensions of Maxillary Sinus Compartments in the Control (Non-Cleft) and Cleft Side.
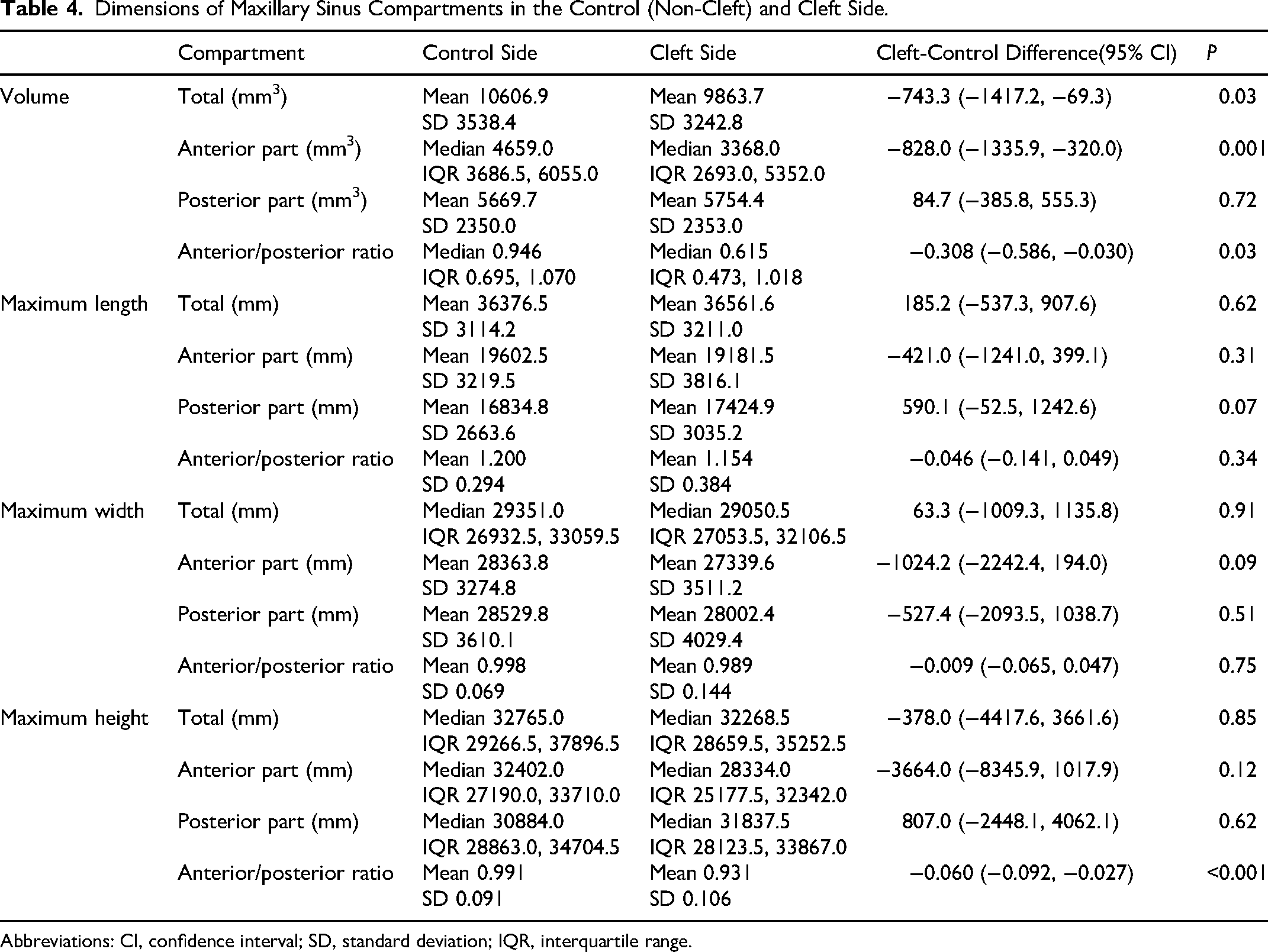
Abbreviations: CI, confidence interval; SD, standard deviation; IQR, interquartile range.
Comparison of Maxillary sinus Linear Measurements Between the Cleft and Non-Cleft Sides
The maxillary sinus length and width comparison between the cleft and non-cleft sides did not reveal a significant difference concerning the linear measurements of either the entire sinuses or the anterior or posterior parts of the sinuses. However, a statistically significant result (p < .001) occurred from the comparison of the anterior/posterior height ratio between the cleft and non-cleft sides (Table 4).
Discussion
In the present study, the non-cleft side demonstrated significantly greater MSV than the cleft side. In contrast, Wang et al. 18 reported no significant differences in maxillary sinus dimensions between the cleft and non-cleft sides. Similar findings have been reported by De Rezende Barbosa et al., 16 Hikosaka et al., 4 and Erdur et al., 5 who also investigated sinus volume in patients with UCLP. Among these studies, Hikosaka et al. 4 observed that the right maxillary sinus tended to be larger than the left in individuals with cleft palate. Likewise, Najm et al. 17 found asymmetry in MSV among patients with UCLP; however, the difference was not statistically significant, in agreement with Nemtoi et al. 27
In contrast to these investigations, several studies have reported findings consistent with the present study. Demirtas et al. 13 found a significant difference in MSV between the cleft and non-cleft sides in patients with UCLP. Similarly, Sehrawat et al. 10 demonstrated significantly reduced MSV on the cleft side and further reported that MSV in patients with UCLP was nearly half that observed in individuals without cleft. Rodrigues et al. 28 likewise found the sinus volume contralateral to the cleft to be larger than that on the cleft side. Similar conclusions were reported by Tunç et al., 29 who showed significantly lower MSV on the cleft side in patients with unilateral cleft palate.
The mean age of participants in studies reporting no significant differences in MSV between cleft and non-cleft sides was generally below 12 years.4,5,16–18,27 In contrast, studies including participants with a higher mean age more frequently demonstrated significant side differences.10,13,28,29 This pattern suggests a possible influence of age on sinus development and volumetric expression.
In the present study, the mean age of the sample was 12.1 years, slightly higher than in studies which did not identify a difference in the volume of sinuses. This observation may be related to age-dependent variation in maxillary sinus growth. According to Rodrigues et al. 28 and Nuñez-Castruita et al., 30 the maxillary sinus undergoes periods of accelerated postnatal growth before approximately 12 years of age. Beyond this period, growth acceleration diminishes, potentially allowing developmental asymmetries to become more evident.
A recent meta-analysis by Srivastav et al. 31 evaluated maxillary sinus characteristics in patients with CLP and found moderate-quality evidence regarding mean MSV differences between cleft and non-cleft sides in UCLP. Their pooled analysis of seven studies did not demonstrate a significant overall difference between sides (95% CI: −0.27 to 0.18). However, because of heterogeneity among included studies, including wide age ranges and varying maturation stages, the influence of developmental age on sinus volume could not be adequately assessed.
In addition to sinus development, Wang et al. 18 reported that although no significant difference in the comparison of the sinuses’ volumes in patients with UCLP between sides was identified, the volume of the maxilla was significantly smaller on the cleft side. Similarly, Agarwal et al. 11 found reduced volume of the segmented maxilla on the cleft side. These findings suggest that cleft-related developmental disturbances may involve hypoplasia of the cleft-side maxilla, potentially influencing maxillary sinus morphology.
A significant difference between anterior and posterior maxillary sinus regions was also identified in the present study. When anterior and posterior sinus volumes were assessed separately, only the anterior region demonstrated significant volume reduction on the cleft side. Similarly, Wang et al. 18 found significantly reduced anterior maxillary volume on the cleft side. Given that the cleft primarily affects the anterior maxilla, these findings support the hypothesis that the anterior portion of the sinus is more directly influenced by the cleft, whereas the posterior region does not show the same trend. The absence of posterior MSV differences and the presence of anterior volumetric differences in the present study support this interpretation.
In the present study, maximum sinus length, width, and height were not significantly affected by the presence of cleft. Wang et al. 18 similarly reported no significant differences in linear maxillary sinus dimensions between sides. Furthermore, linear measurements of the anterior and posterior sinus compartments did not differ significantly between sides. However, the anterior/posterior height ratio was significantly different, suggesting an imbalance in vertical development of the anterior sinus region in children with UCLP, potentially secondary to reduced anterior sinus volume on the cleft side.
Although linear measurements of the maxilla in patients with cleft have been previously reported, data regarding the anterior and posterior compartments of the maxillary sinus remain limited. Wang et al. 18 reported reduced anterior maxillary width on the cleft side, while posterior dimensions did not differ significantly between sides. Similarly, Agarwal et al. 11 reported reduced anterior maxillary height. These observations further support the hypothesis that cleft may be associated with generalized hypoplasia of the anterior craniofacial complex. Nevertheless, both the maxilla and the maxillary sinus exhibit complex and highly variable three-dimensional morphology, and volumetric analysis is therefore preferable to linear measurements as a more representative indicator of anatomical size.
Only two studies have compared patients with UCLP and healthy controls to assess the influence of sex on MSV using CBCT.5,13 Neither found significant sex-related differences in MSV, either between UCLP and control groups 13 or between cleft and non-cleft sides in UCLP patients. 5 The effect of sex was not examined in the present study because of the relatively small sample size and the inclusion of participants at varying developmental stages.
The retrospective design of the present study may introduce confounding and selection bias. 32 The age range of 8–14 years may also represent a limitation, as this interval encompasses the pubertal growth spurt, during which craniofacial development may vary substantially. Although stratification by chronological age could have been considered, chronological age alone does not necessarily reflect skeletal maturity. Furthermore, the requirement for clinically indicated CBCT imaging limited the availability of retrospectively followed participants to those undergoing orthodontic or reconstructive evaluation.
Conclusion
The MSV is significantly smaller on the cleft side in young patients with UCLP and this hypoplasia concerns the anterior part of the sinus. Even though the linear measurements of the maximum length, width and height of the (a) entire maxillary sinus, (b) anterior part of the maxillary sinus and (c) posterior part of the maxillary sinus were found not to be affected by the cleft, there are indications of an existing imbalance in the vertical development of the anterior part of maxillary sinus between the two sides in children with UCLP, possibly as a secondary manifestation owing to the decreased anterior MSV of the cleft side.
Footnotes
Ethics Approval
Prior to treatment, all patients had provided signed informed consent for use of their data in research. Ethical approval was received from the appropriate authorities (National and Kapodistrian University of Athens, School of Dentistry 96483/4.10.2023).
Ethical Approval and Informed Consent Statements
The study received approval from the ethics committee of the National and Kapodistrian University of Athens (PN:96483/4.10.2023). All selected patients’ files included a consent form signed by the parent or legal guardian at the time of treatment.
Author Contributions
In this paper, the conception and design were made by TV. The ethical approval application was written by TV and IS. Methodology was defined by TV and DH. The sample screening was conducted by TV, IS and CL. The acquisition of measurements and the results evaluation was performed by TV. Statistical analysis was conducted by SNP and TV, who also constructed the tables and figures. The manuscript was written by TV with DH, IS, TW and NS providing editing and revisions. All authors approved the final version. TV is the main contributor to this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The dataset for this study is openly available: DOI 10.5281/zenodo.17871759.