
Abstract
Objective
This study aimed to assess public knowledge, attitudes, and awareness concerning cleft lip and/or palate (CL/P) among the general population of North India, seeking to identify existing knowledge gaps, misconceptions, and readiness for awareness initiatives.
Design
A cross-sectional, questionnaire-based survey.
Setting
Dental outpatient department (OPD) of a tertiary healthcare institute in North India.
Patients, Participants
A total of 648 participants (357 males, 291 females; aged 18-75 years), recruited via convenience sampling from the dental OPD visitors between May 2025 and August 2025. Participants were 18 years or above and could read English/Hindi.
Interventions
None.
Main Outcome Measure(s)
Public knowledge of CL/P etiology, risk factors, treatment options, support systems, perceived social impact, and attitudes toward CL/P and public education, measured via a 14-item closed-ended questionnaire.
Results
A majority of respondents (78.86%) reported general awareness of CL/P, but detailed knowledge about etiology (eg, maternal age, smoking, alcohol as risk factors), comprehensive multidisciplinary management (recognized by only 2.16%), and available support systems such as governmental or non-governmental organizations, were significantly limited. Misconceptions about CL/P being acquired or contagious persisted. Positive attitudes included belief in productive lives for affected individuals and willingness to support CL/P initiatives. Knowledge status was significantly associated with gender and education level.
Conclusions
Despite general familiarity, significant knowledge gaps exist regarding CL/P in North India. Targeted public health strategies are urgently needed to correct misconceptions, promote multidisciplinary care awareness, and improve knowledge of available support organizations to enhance access to care and social inclusion.
Keywords
Introduction
Cleft lip and/or palate (CL/P) are among the most frequent congenital craniofacial anomalies that can severely interfere with feeding, speech, and social integration, presenting significant functional, esthetic, and psychosocial challenges for affected children and their families.1,2 Crucially, the nature and severity of these psychological outcomes often correlate with the specific cleft diagnosis. For instance, patient-reported outcomes indicate that youths born with unilateral clefts navigate multidimensional impacts on their psychological well-being throughout adolescence. 3 Conversely, more severe presentations carry an even greater burden, with bilateral orofacial clefts associated with a significantly higher risk of psychiatric morbidity compared to unilateral cases. 4
The lip and palate develop between the fifth and twelfth weeks of intrauterine life; any interruption during this critical embryologic period may prevent the proper fusion of facial prominences, resulting in cleft lip, cleft palate, or both.5–7 The causation of CL/P is multifactorial, involving an interaction between genetic predisposition and environmental influences such as poor maternal nutrition, alcohol or tobacco exposure, and teratogenic drug intake during pregnancy.6,8,9
Globally, the prevalence of CL/P varies across populations and geographic regions.6,8,10 In Asian populations and India, the incidence is 2 and 1.4 per 1000 live births, respectively, compared with 1 per 1000 among Caucasians and about 0.5 per 1000 among African Americans.2,6,11,12 India alone contributes an estimated 35,000 new CL/P cases each year, reflecting a significant share of the global congenital anomaly burden.6,13 Regional studies within India have reported prevalence rates ranging from 0.54 to 2.75 per 1000 live births. 11 Despite this substantial incidence, many children remain untreated due to socioeconomic barriers, limited awareness, and inadequate access to specialized care.9,10,14–17
Comprehensive CL/P management requires a multidisciplinary approach integrating surgery, orthodontics, speech therapy, prosthodontics as well as psychological support and targeted psychiatric screening evaluations.7,9,18–20 Typically, lip repair is performed within the first few months of life, followed by palatal reconstruction, speech therapy, orthodontic correction, and prosthetic or implant-supported rehabilitation in later years.7,18,21 In resource-limited settings such as India, this continuum of care is often fragmented.11,17 Inadequate knowledge about treatment sequencing, insufficient follow-up, feeding difficulties, and delayed presentation frequently worsen outcomes.10,13,15 Kharbanda and Monga 22 have highlighted that the lack of organized cleft care networks and insufficient public awareness are key obstacles to successful rehabilitation.
Although government programs such as the Rashtriya Bal Swasthya Karyakram aim to address these rehabilitation obstacles, comprehensive cleft care in India increasingly relies on a collaborative public-private framework. Modern non-governmental organizations (NGOs) such as Smile Train, Mission Smile, Operation Smile, to name a few, increasingly utilize horizontal and diagonal models of care by working synergistically with local healthcare institutions and state health authorities. However, community awareness regarding the availability and benefits of these collaborative initiatives remains inadequate.23–25
The challenge of inadequate public awareness and understanding regarding CL/P is not isolated to a specific region but is a well-documented global phenomenon. For instance, in high-income contexts like Australia, up to 30% of the general public remains entirely unaware of clefting, with significant knowledge gaps persisting regardless of educational background. 26 Similarly, a recent study from Japan indicates that even when there is a general understanding of the etiology and positive medical prognosis of the condition, children with CL/P still face significant social and psychological hurdles related to appearance, peer relationships, and speech. 27 In developing regions, these knowledge deficits are often more pronounced; a study among antenatal attendees in Nigeria found that only 19.8% possessed adequate knowledge about CL/P, 28 while research in Ethiopia highlighted severe social stigmas, maternal blame, and a concerning lack of awareness even among dental students. 29 A recent systematic review further emphasizes how entrenched cross-cultural and supernatural beliefs profoundly shape societal responses and hinder the acceptance of multidisciplinary care across various global populations. 30 Compounding these public awareness challenges, global assessments indicate a persistent lack of integrated knowledge and standardized clinical experience even among specialized dental providers, such as orthodontists. 31 Collectively, these international findings underscore the universal need for targeted health education.
Most existing Indian studies on CL/P awareness have focused on caregivers, healthcare providers, or specific regional populations. However, no comprehensive assessment has yet evaluated awareness among the general public of North India—a region marked by diverse socioeconomic and demographic characteristics. This questionnaire-based survey sought to identify existing knowledge gaps, misconceptions, and the public's readiness to participate in awareness and support initiatives.
Materials and Methods
Study Design and Setting
This cross-sectional, questionnaire-based survey was conducted at the Department of Dentistry at All India Institute of Medical Sciences (AIIMS), Rishikesh, Uttarakhand, India. The study was specifically designed to evaluate awareness and perceptions of CL/P among the general population visiting the dental outpatient department (OPD).
Sample Size Calculation
The sample size for this study was calculated using the Cochran's sample size formula with a 5% margin of error and 95% confidence level using the awareness percentage as reported by Gantugs et al 32 The minimum required sample size was 177.
Ethical Approval: The study protocol received approval from the Institutional Ethics Committee (Approval number: 177/IEC/IM/NF/2025). Prior to participation, all respondents provided voluntary informed consent and their confidentiality was maintained throughout the study.
Questionnaire Development and Validation
The questionnaire was initially developed by the primary investigators (S.K. and N.K.) in English in accordance with standardized psychometric principles for scale development, progressing from item generation to theoretical analysis.33–35 To maximize accessibility and comprehension for the linguistically diverse North Indian population, the English tool was translated into Hindi to create a side-by-side dual-language (bilingual) instrument. This initial forward translation was performed by an independent bilingual co-investigator (A.D.), followed by a back-translation into English by another investigator (A.C.) blinded to the original version, adhering to established cross-cultural adaptation guidelines. 36 To ensure accurate recognition of the condition rather than relying solely on text descriptions, an illustrative image of a child with CL/P was strategically placed at the beginning of the instrument.
To evaluate the preliminary subjective assessment of the instrument, face validity was initially conducted with a purposive sample of 10 subjects from the target demographic. Based on their feedback regarding semantic ambiguity, the questionnaire underwent 3 iterative rounds of linguistic refinement to optimize layperson comprehension prior to expert review.
Subsequently, this refined draft underwent rigorous content validation by an expert committee comprising 3 bilingual subject experts. The committee evaluated the instrument to resolve any remaining discrepancies, establish semantic and conceptual equivalence, finalize the dual-language formatting, and confirm medical accuracy. The scale-level content validity index based on the average method was calculated to be .98, indicating excellent conceptual agreement and overall content validity among the experts.
Following expert adjudication, the instrument was subjected to formal pilot testing among 30 participants.36,37 This pilot phase confirmed the instrument's clarity, cultural acceptability, and overall feasibility, yielding no further requirements for modification and establishing its readiness for full-scale data collection. The 30 participants from the pilot testing phase were retained and included in the final study sample.
As a result of this comprehensive, multi-stage development and validation process, the finalized questionnaire comprised 14 closed-ended questions categorized into 7 distinct domains: demographics, basic knowledge of CL/P, perceived causes and risk factors, awareness of treatment and management options, understanding of social and emotional impacts, knowledge of available support and resources, and attitudes and beliefs concerning CL/P (Supplemental Appendix A). Furthermore, to accommodate individuals with limited digital literacy or smartphone access, it was unanimously decided to administer the finalized questionnaire exclusively in a paper-based format.
Participants
Participants were recruited using a convenience sampling method. The study included individuals who were over 18 years of age, visited the dental OPD at AIIMS, Rishikesh and were able to read and comprehend English or Hindi. To minimize selection bias within the clinical setting, convenience sampling was conducted consecutively; investigators approached all eligible individuals systematically, ensuring recruitment was entirely independent of the participant's socioeconomic presentation, attire, or outward appearance.
During the initial conversational screening, the investigators initiated contact by asking patients their reason for visiting the dental OPD to establish baseline communication and determine basic study eligibility. Individuals who disclosed they were unable to read the questionnaire were excluded at this stage. Furthermore, in instances of psychiatric impairment where patients exhibited a clear inability to comprehend or respond to the baseline questions, or accompanying caregivers intervened to inform about the patient's condition, the investigators utilized their clinical judgment
38
to exclude the individual from the study
A total of 680 individuals participated in the survey from May 2025 to August 2025 of which 32 were excluded due to incomplete responses, yielding a final analytical sample size of 648. There were 357 males (54.9%) and 291 females (44.8%) between the ages of 18 and 75. Regarding education level, to facilitate robust statistical comparison, the 4 original questionnaire categories were collapsed into 2 primary demographic groups: 66.3% of the participants were college graduates or above, while 33.7% had high school-level education or below (Figure 1). The majority of the participants were from Uttarakhand, followed by Uttar Pradesh and representatives from other North Indian states.
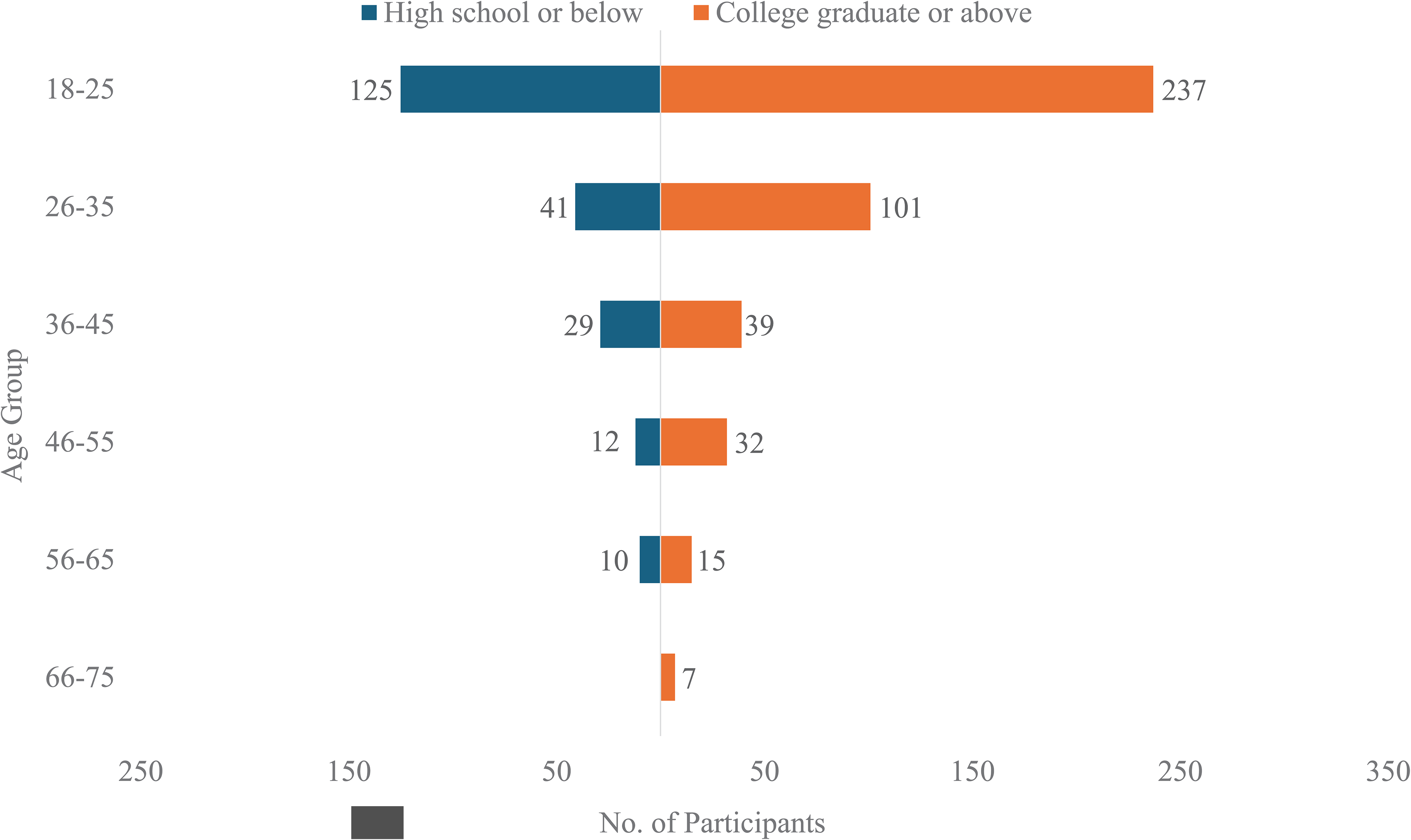
Demographic distribution of participants by age and education level. Pyramid chart depicting the distribution of participants (n = 648) across different age groups and education levels. The chart illustrates that most respondents were between 18 and 35 years of age, with the majority being college graduates or above (66.3%), while 33.7% had high school-level education or below.
Data Collection Procedure
Upon their arrival at the dental OPD, eligible participants were briefed on the study's general logistics and informed consent procedures by one or both investigators (S.K. and N.K.). Following the distribution of questionnaires, support was offered to participants who needed clarification, without providing information that could influence their answers. To maintain the integrity of the data, participants were monitored to prevent any discussion or use of smartphones while responding to the questionnaire.
After the questionnaires were gathered, the investigators resolved any doubts the participants had concerning CL/P. For example, a majority of the participants inquired about the primary objective of the survey. In response, investigators utilized these interactions as an opportunity for health promotion, explaining that the questionnaire served a dual purpose: to collect data and to actively educate the public, empowering them with the knowledge to appropriately guide friends or family members in the future. Additionally, participants frequently required clarification on etiology. For instance, some raised culturally contextualized doubts regarding maternal risk factors, questioning the actual prevalence of women smoking or consuming alcohol, which required investigators to take additional time to explain the concepts of active/passive smoking and alcohol exposure. Strikingly, a small number of participants confidently asserted that CL/P is caused by a pregnant woman's exposure to a lunar eclipse, even questioning the omission of this superstitious belief from the questionnaire's list of causes. In these instances, investigators engaged in culturally sensitive dialogue to clarify the scientifically established etiologies without alienating the respondents.
Statistical Analysis
All collected data were systematically entered into Microsoft Excel (Microsoft Corporation, Redmond, WA, USA) for organization and initial review (S.K and S.R.). Any discrepancies were resolved through team review and discussion (S.K., N.K. and S.R.). Statistical analysis was then performed using IBM SPSS Statistics for Windows, Version 26.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics, including frequencies and percentages, were calculated for categorical variables. Pearson's Chi-square test was applied to assess associations between demographic characteristics and awareness of CL/P. An independent-samples t-test was used to compare mean knowledge scores across the dichotomized education levels (high school or below vs. college graduate or above). A P-value of < .05 was considered statistically significant.
An overall knowledge score was computed for each participant by aggregating 19 specific responses from Section 3 through Section 6 of the questionnaire. A score of 1 was awarded for each correct or affirmative response (eg, “Yes”), while a score of 0 was assigned for “No,” or “Not sure” responses. Notably, for multifaceted items such as Question 7 regarding general treatment awareness, only the primary question (“Do you know if cleft lip and/or palate can be treated?”) was scored, while its respective sub-questions were excluded from this calculation. These 19 item scores were summed to generate a cumulative continuous variable—yielding a maximum possible knowledge score of 19—which was subsequently utilized for comparative statistical analysis.
Results
An overall knowledge score was calculated for each participant to assess awareness and understanding of CL/P. When compared across educational levels, participants with college graduate level education or higher demonstrated significantly higher mean knowledge scores (mean = 11 ± 4.00) than those with only high school-level education or lower (mean = 8.95 ± 4.11). This difference was statistically significant (P < .001; independent-samples t-test) (Table 2).
Discussion
This study aimed to assess public knowledge, attitudes, and awareness concerning CL/P among the general population of North India. The findings highlight a paradoxical scenario in which a majority of respondents (78.86%) reported general awareness of CL/P, yet detailed knowledge about its etiology, comprehensive management, and available support systems remains significantly limited.
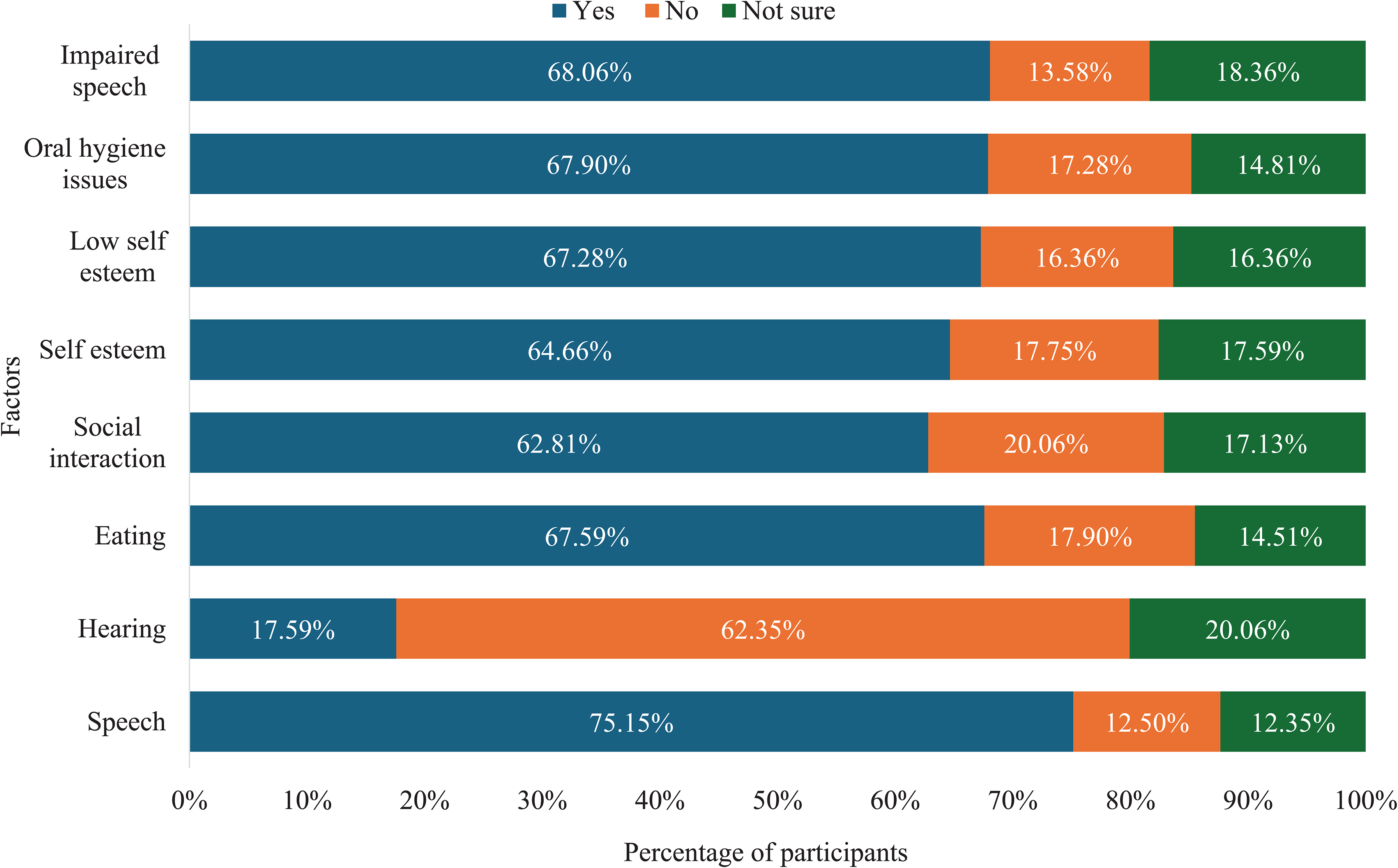
Perceived social and long-term effects of CL/P. Composite bar graph showing respondents’ perceptions of the social, functional, and long-term consequences of CL/P. The most commonly recognized effects included speech impairment (68.06%), oral hygiene problems (67.9%), and low self-esteem (67.28%). Many participants also associated CL/P with feeding difficulties and reduced social interaction.
Association of Sociodemographic Characteristics with Cleft Lip and/or Palate Awareness.
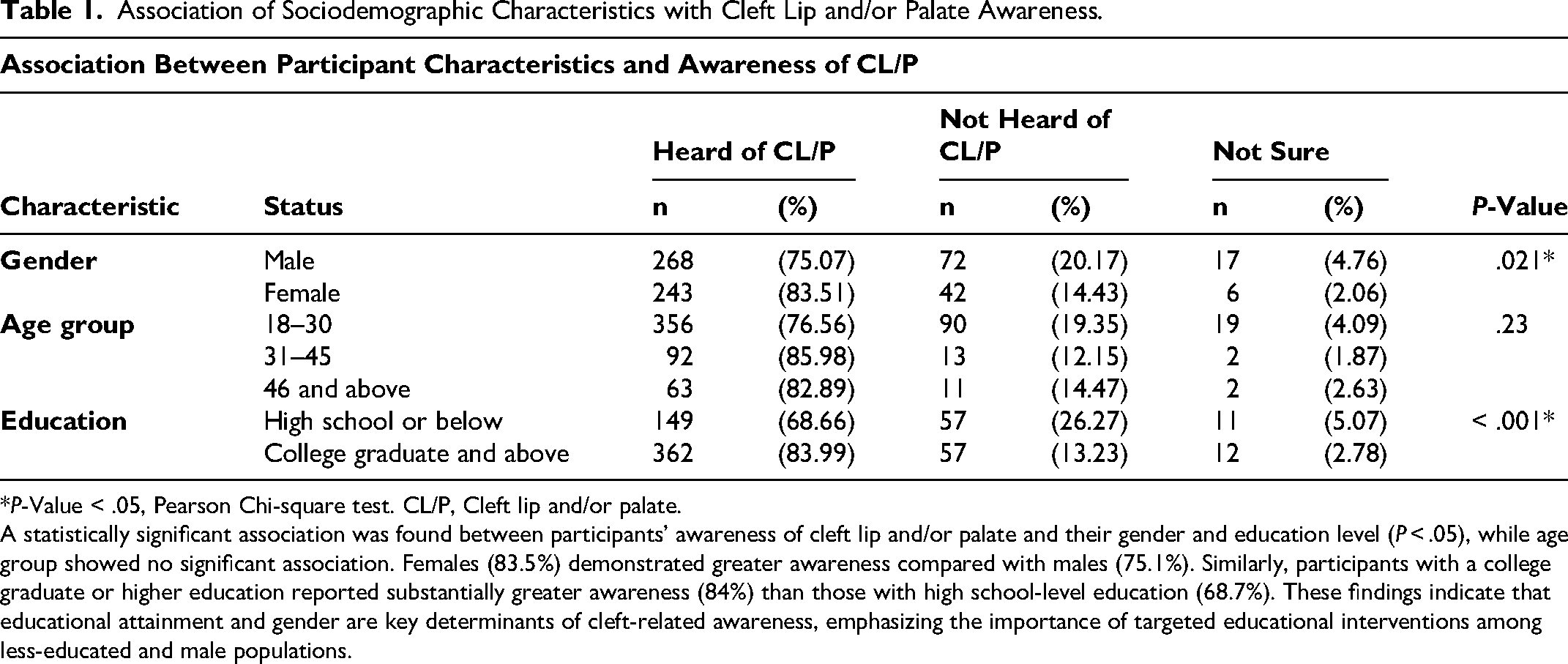
*P-Value < .05, Pearson Chi-square test. CL/P, Cleft lip and/or palate.
A statistically significant association was found between participants’ awareness of cleft lip and/or palate and their gender and education level (P < .05), while age group showed no significant association. Females (83.5%) demonstrated greater awareness compared with males (75.1%). Similarly, participants with a college graduate or higher education reported substantially greater awareness (84%) than those with high school-level education (68.7%). These findings indicate that educational attainment and gender are key determinants of cleft-related awareness, emphasizing the importance of targeted educational interventions among less-educated and male populations.
Comparison of Mean Knowledge Scores Based on Education Level.
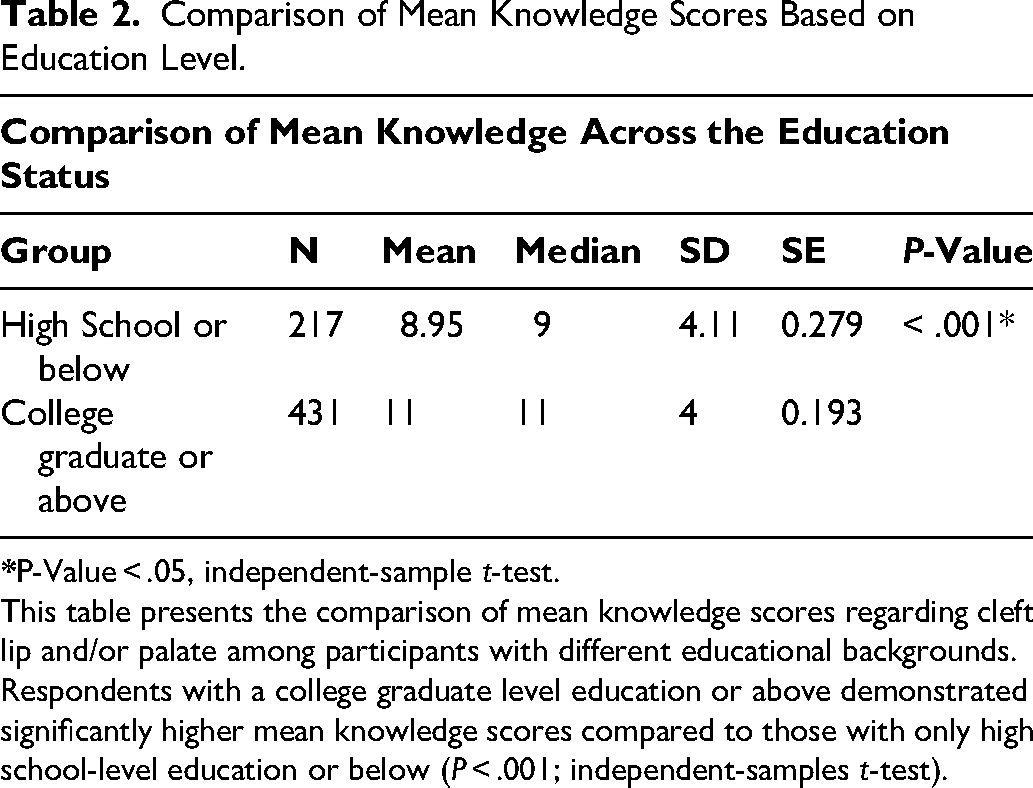
This table presents the comparison of mean knowledge scores regarding cleft lip and/or palate among participants with different educational backgrounds. Respondents with a college graduate level education or above demonstrated significantly higher mean knowledge scores compared to those with only high school-level education or below (P < .001; independent-samples t-test).
A substantial majority of the surveyed population had heard of CL/P, indicating a promising baseline for public health initiatives. While most participants correctly identified CL/P as a birth defect, a notable proportion held misconceptions, believing it to be an acquired or contagious condition. This finding is consistent with prior research suggesting that although general awareness of CL/P as a condition may exist, specific knowledge often falls short. As noted previously, this is a global phenomenon; both high-income nations and developing regions struggle with steep knowledge deficits regarding cleft etiology and comprehensive management, which frequently perpetuates social stigma.26–29 Furthermore, as observed in recent studies from Japan, even when there is a correct understanding of the condition's etiology among professionals like educators, there remains a strong recognition that affected children will still navigate complex social difficulties regarding teasing, appearance, and unclear pronunciation, highlighting the need for collaborative psychosocial support. 27
In contrast to studies from other Indian regions, such as Chennai, where only 19.24% of the population demonstrated awareness of CL/P, 23 this study reveals a higher general recognition in North India. This disparity may reflect regional differences in public health communication, educational outreach, or sociodemographic characteristics. However, our findings align closely with recent assessments from other Indian tertiary care centers, which similarly noted substantial gaps in the public's understanding of cleft etiology and comprehensive management despite baseline familiarity. 40
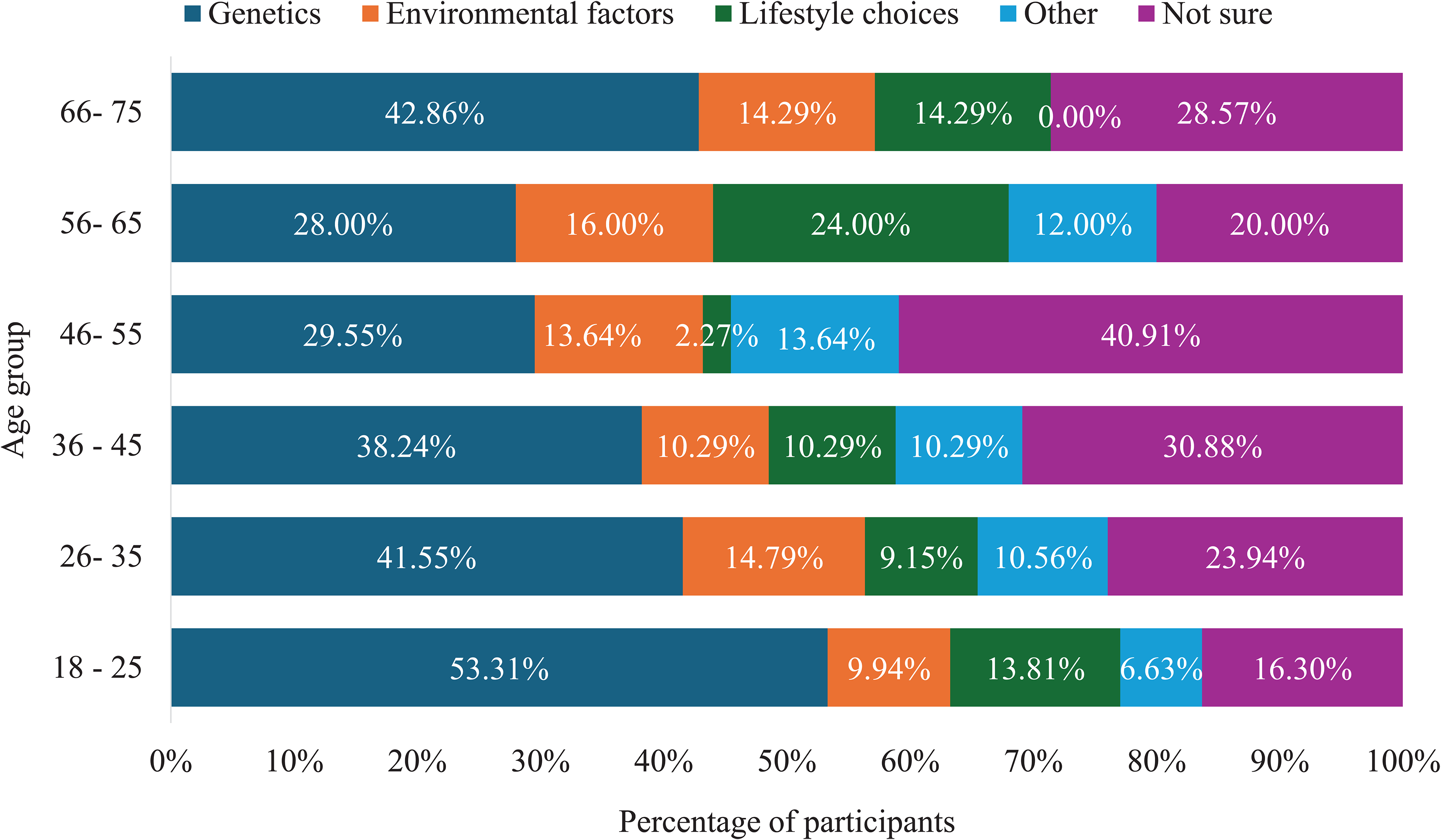
Regarding the perceived causes and risk factors (Figures 3 and 4), nearly half of the respondents attributed CL/P to genetic factors, aligning with the understanding that CL/P has a multifactorial etiology involving both genetic predisposition and environmental influences. 41
Awareness of the cause of CL/P. Bar chart representing respondents’ understanding of the cause of CL/P. The figure shows the proportion who identified it as a birth defect, those who believed it to be acquired or contagious, and those who were unsure.
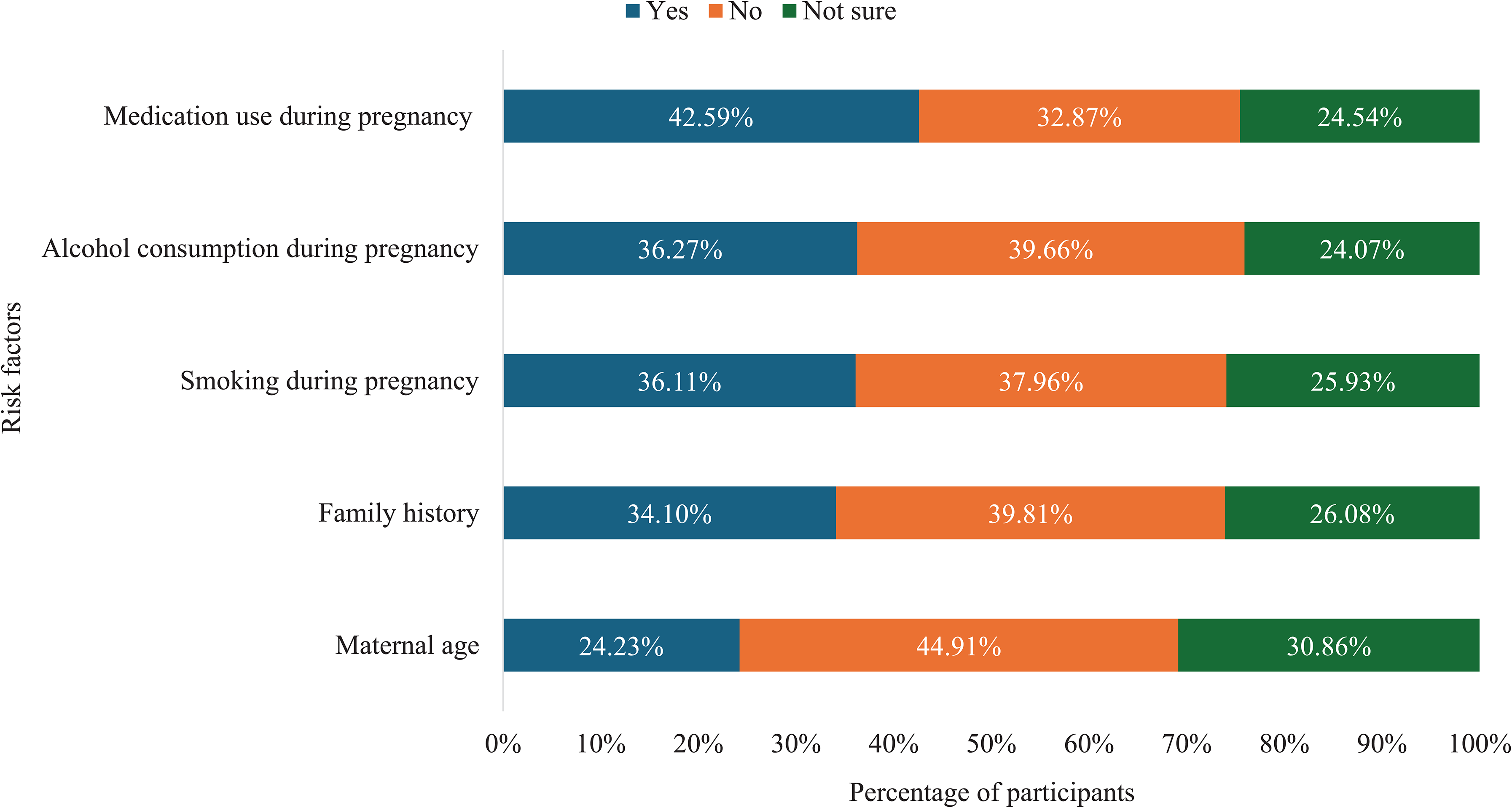
Awareness of risk factors for CL/P. Clustered bar chart depicting public knowledge of potential maternal and environmental risk factors—including maternal age, family history, smoking, alcohol use, and medication intake during pregnancy. The results highlight notable uncertainty regarding specific risk associations.
However, knowledge gaps were evident concerning specific environmental risk factors. Awareness of maternal age, smoking, and alcohol consumption during pregnancy as risk factors was low, with many respondents denying any association or expressing uncertainty. This lack of precise knowledge about modifiable risk factors is concerning, as studies have identified several environmental contributors—such as maternal illness, teratogenic drug use, and nutritional deficiencies that can increase the risk of CL/P.6–8,42 The persistence of uncertainty and attribution to personal or cultural explanations suggests enduring societal misconceptions that may perpetuate stigma and blame toward parents. 43
Educational level was another significant factor influencing awareness. Participants with college graduate education or above exhibited higher mean knowledge scores than those with only high school-level education or below (P < .001). This finding supports existing research indicating that education enhances health literacy, comprehension of medical information, and engagement with preventive care.32,43 Therefore, public health initiatives should prioritize simplified, visually guided, and language-appropriate educational materials to reach individuals with limited formal education and improve community-wide understanding of CL/P.
Furthermore, while 64.66% of respondents accurately associated CL/P with lowered self-esteem, public understanding lacks the clinical nuance regarding how these psychosocial burdens vary by cleft severity. As highlighted in recent literature, the psychological trajectory of affected individuals differs significantly based on the diagnosis; youths with unilateral clefts face distinct multidimensional social challenges, whereas those with bilateral orofacial clefts exhibit a markedly higher risk for severe psychiatric morbidity.3,4 The public's broad, generalized perception of cleft impacts underscores the need for awareness campaigns that educate communities on the specific, escalating support needs associated with more complex bilateral presentations.
The study also revealed significant gaps in public understanding of CL/P management. Although most respondents recognized surgery as the main treatment, only a small fraction were aware of the necessity for a comprehensive, multidisciplinary approach involving surgery, orthodontics, speech therapy, and psychological counseling.
This limited awareness of integrated cleft care parallels findings from other developing regions, where access to specialized services is often fragmented. Recent systematic reviews underscore that this fragmentation is driven not only by logistical barriers but also by entrenched cross-cultural beliefs that can deter families from seeking multidisciplinary treatments in favor of traditional remedies. 30 Compounding this issue is a lack of cohesive, interdisciplinary training among healthcare providers themselves; global trends reveal that even specialized practitioners, such as orthodontists, frequently report limited clinical experience and knowledge regarding the comprehensive management protocols required for CL/P. 31
Despite a majority acknowledging the importance of early intervention, many participants lacked knowledge regarding prenatal diagnosis and the continuum of post-surgical rehabilitation. Parental awareness is essential for promoting timely intervention and adherence to long-term treatment protocols. 41
A particularly striking finding of this study is the alarmingly low awareness of available support systems, including collaborative initiatives between government programs and major international non-NGOs. 24 Fewer than 15% of participants reported knowledge of these resources. This lack of awareness is concerning, as modern foundation-based cleft initiatives rarely operate as isolated, vertical surgical missions. Instead, they actively engage in capacity building, collaborating deeply with local health authorities and tertiary hospitals to build sustainable infrastructure, train local healthcare professionals, and deliver continuous multidisciplinary care. 24 Many Indian institutions offering comprehensive cleft care depend heavily on this integrated network of NGOs, governmental, and philanthropic support. 17 However, the general public remains largely uninformed about the existence of these vital partnerships. This disconnect limits access to care, particularly among economically disadvantaged families or those living in remote areas, where untreated cases and delayed interventions remain common.23,42
Despite these knowledge deficits, the study identified encouraging attitudes within the population. Most participants believed that individuals with CL/P can lead fulfilling and productive lives, and nearly three-fourths expressed willingness to support awareness or treatment initiatives. Moreover, an overwhelming majority emphasized the importance of public education about cleft conditions. These positive perceptions provide a strong foundation for developing future awareness campaigns and community-level programs aimed at reducing stigma and improving early detection.
The present findings highlight the urgent need for regionally tailored public health interventions to enhance CL/P literacy in North India. Communication strategies that extend beyond conventional awareness drives—integrated into maternal and child health programs and supported by media outreach—can help bridge existing knowledge gaps. Collaborative partnerships between government agencies, NGOs, and healthcare institutions can also play a pivotal role in strengthening public awareness, promoting early intervention, and ensuring equitable access to multidisciplinary cleft care.
The qualitative interactions during data collection further underscore the critical need for culturally tailored health education. For instance, the skepticism expressed by participants regarding maternal smoking and alcohol consumption reflects the socio-cultural realities of North India, where female substance use is historically low and highly stigmatized. 44 Consequently, laypersons often struggle to correlate these factors with local cleft incidence, despite recent, extensive meta-analyses unequivocally confirming them as significant environmental teratogens for orofacial clefting. 45 More strikingly, the confident assertion by a few participants that a lunar eclipse causes CL/P highlights the persistent influence of deep-rooted regional folklore. This observation is strongly corroborated by recent literature demonstrating that celestial events and divine retribution remain the most widely believed etiologies among Indian parents.40,46 The fact that participants actively questioned the omission of the lunar eclipse from our questionnaire demonstrates that these are active convictions competing with medical facts. As highlighted by recent qualitative evaluations of regional cleft care, overcoming these entrenched beliefs requires healthcare professionals to move beyond simple information dissemination and engage in culturally sensitive, empathetic dialogue to effectively alleviate parental shock and improve the acceptance of evidence-based care.40,45,46
Limitations
As a cross-sectional, questionnaire-based survey, this study relied on self-reported information, which may introduce response bias. Furthermore, the use of convenience sampling from a single public tertiary care center introduces a potential demographic bias.
While researchers approached the participants uniformly regardless of attire or socioeconomic appearance, the potential for unconscious bias during the recruitment phase cannot be entirely eliminated.
In the Indian healthcare infrastructure, public healthcare centers predominantly serve individuals from lower-to-middle socioeconomic strata seeking subsidized care, whereas the utilization of private healthcare facilities is significantly correlated with higher household wealth and greater educational attainment.47–49 Consequently, our cohort may reflect lower baseline educational levels and health literacy than a broader population inclusive of private-sector patients, potentially limiting the generalizability of the awareness scores. Despite these constraints, the study provides valuable insights into public knowledge and perceptions of CL/P, forming a foundation for future multicenter research with larger and more diverse populations.
Conclusion
This study reveals that while there is a basic public recognition of CL/P in North India, this superficial familiarity masks profound gaps regarding its etiology, modifiable risk factors, and the necessity of comprehensive multidisciplinary care. Furthermore, an alarming lack of public awareness regarding governmental and non-governmental support organizations severely limits access to care for affected families facing socioeconomic challenges. However, the strong foundation of positive public attitudes and widespread agreement on the importance of public education offer a promising avenue for intervention. There is an urgent need for structured, evidence-driven public health programs and collaborative outreach strategies to correct misinformation, improve awareness of multidisciplinary care, and increase the visibility of support organizations, ultimately fostering greater social inclusion and equitable access to treatment.
Supplemental Material
sj-pdf-1-cpc-10.1177_10556656261459726 - Supplemental material for Cleft Lip and Palate Awareness in General Population of North India
Supplemental material, sj-pdf-1-cpc-10.1177_10556656261459726 for Cleft Lip and Palate Awareness in General Population of North India by Sunil Kumari, Nithin K V, Sangeeta Rai, Ashi Chug and Ashutosh Dixit in The Cleft Palate Craniofacial Journal
Footnotes
Acknowledgements
None.
Ethical Considerations
The Institutional Ethics Committee of the AIIMS, Rishikesh, approved the study protocol (Approval No. 177/IEC/IM/NF/2025) on May 2, 2025. Written informed consent was obtained from all participants prior to the interviews.
Consent to Participate
All participants provided informed consent prior to participation. The purpose of the study was explained to them in detail, and they were assured of confidentiality and the voluntary nature of their participation. Written consent was obtained from all participants before completing the questionnaire.
Consent for Publication
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request. The study questionnaire is available as Supplemental Material (Supplemental Appendix A).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.