
Abstract
Objective
To investigate the self-perception of adults with cleft lip and palate during the treatment process, analyzing correlations among sociodemographic variables, cleft types, surgical history, and satisfaction reported through the CLEFT-Q.
Design
Observational, cross-sectional, and prospective study based on primary and secondary data. Correlation tests identified associations between clinical and psychosocial factors and self-perception scores obtained through the instrument.
Setting
National tertiary referral hospital for craniofacial anomaly treatment, in an outpatient setting.
Participants
Fifty adults aged 18-29 years, of both sexes, with cleft lip and palate, without associated syndromes. Palate clefts and cognitive impairments that hindered assessment were excluded.
Interventions
Administration of the CLEFT-Q, composed of 13 scales covering appearance, facial function, and health-related quality of life, complemented by clinical and sociodemographic data from medical records.
Main Outcome Measures
CLEFT-Q.
Results
The lowest mean scores were observed for nose (42.8 ± 24.9) and nostrils (44.3 ± 30.2), and the highest for jaw (71.0 ± 27.1) and lip scar (65.0 ± 25.3). Rhinoplasty was associated with higher esthetic satisfaction (P = .004; P = .022). The number of palate repair correlated negatively with speech and eating domains.
Conclusions
Self-perception was related to clinical variables, particularly cleft type and surgical history. The CLEFT-Q proved essential for patient-centered care, broadening the understanding of subjective outcomes in craniofacial treatment.
Introduction
Cleft lip and palate (CLP) is a congenital craniofacial malformation that occurs in approximately 1 in every 700 live births.1-3 Depending on the type and extent of the cleft, individuals may present varying degrees of functional impairment, such as difficulties in feeding during early infancy and altered speech and dental anomalies.4-7 Beyond functional limitations, CLP may be associated with emotional and psychosocial consequences, including reduced self-esteem, social withdrawal, and impaired communication particularly when functional or esthetic concerns persist despite treatment.6,7 Individuals with clefts often report greater concern with facial appearance—particularly the nose and nostrils—and that dissatisfaction with appearance may affect interpersonal relationships, while corrective surgeries can improve self-perception.8-11
Considering these factors, patient-reported outcome measures (PROMs) have emerged as essential tools to assess patient perspectives throughout treatment. PROMs allow systematic evaluation of how individuals perceive their appearance, function, and quality of life, complementing traditional clinical assessments and supporting patient-centered care. In line with the International Consortium for Health Outcomes Measurement recommendations, PROMs have become central to the comprehensive appraisal of cleft care. The CLEFT-Q is currently recommended as part of the international standard set of outcome measures, reinforcing its relevance for clinical benchmarking and research.12-17
Studies1,9 using the CLEFT-Q have shown that appearance-related domains tend to yield lower scores, while psychological and school-related domains often present higher scores. Treatment type also influences patient perception, with surgical interventions generally associated with higher satisfaction and active orthodontic treatment linked to temporarily lower scores. Importantly, psychosocial vulnerability has been associated with significantly poorer scores across appearance, speech, and psychosocial domains, even in the absence of objective clinical discrepancies. These findings demonstrate that incorporating the CLEFT-Q into clinical practice not only reveals aspects of self-perception that may be overlooked in routine evaluations but also informs clinical decision-making, supports individualized care, and enhances overall patient management.1,9
Prior to the development of cleft-specific PROMs, several instruments were used to assess quality of life in individuals with craniofacial conditions. Among these, the Youth Quality of Life-Facial Differences and the Youth Quality of Life-Craniofacial Surgery were designed to evaluate psychosocial impact in adolescents with visible facial differences and those undergoing craniofacial surgery. Although valuable in capturing emotional and social dimensions, these instruments were not specific to cleft lip and/or palate and did not comprehensively assess functional domains such as speech, eating, and treatment-related outcomes.
During treatment, individuals with cleft lip and/or palate undergo multiple consultations within the service responsible for their care and are followed by a multidisciplinary team that provides interventions according to their clinical and developmental needs. Treatment protocols vary depending on the type and extent of the cleft. At a tertiary referral center for craniofacial anomalies in Brazil, surgical interventions typically begin at 3 months of age with lip repair in cases involving the lip and at 12 months of age with palate repair when the palate is affected. 8
Throughout development, patients may require additional procedures such as secondary lip revision, alveolar bone grafting (ABG), correction of velopharyngeal dysfunction, rhinoplasty, septoplasty, or orthognathic surgery. In addition to surgical management, patients receive longitudinal follow-up with professionals from multiple disciplines, including speech-language pathologists, dentists, psychologists, physiotherapists, and nutritionists to monitor development and provide necessary therapeutic interventions.
Although previous studies have explored patient-reported outcomes in pediatric populations and specific surgical contexts, fewer investigations have examined young Brazilian adults and the relationship between cumulative surgical history and self-perceived outcomes. In this context, the present study aims to investigate patient-reported outcomes in adult individuals with CLP treated at a referral center, examining associations between CLEFT-Q scores, cleft type, and surgical history.
Methods
Observational, cross-sectional with prospective data collection. The prospective nature of the study derived from the planned and direct data collection, obtained through the administration of the CLEFT-Q instrument to the participants.
The study was approved by a local Institutional Research Ethics Committee in accordance with national ethical guidelines and standards for research involving human participants.
Participants
The study included 50 adult patients, aged between 18 and 29 years, from a tertiary referral center for craniofacial anomalies in Brazil, with cleft lip (CL) or CLP, regardless of gender, race, or educational level, who were undergoing treatment at the institution at the time of data collection, conducted during June 2024 to July 2025.
Participants were recruited using a convenience sampling approach, based on the study's inclusion criteria and their attendance at routine outpatient appointments during the data collection period. Individuals with isolated cleft palate, those whose level of comprehension did not allow adequate participation in the proposed methods, and those with associated syndromes and/or anomalies were excluded from the study.
Individuals with isolated cleft palate were excluded in order to maintain greater homogeneity in surgical trajectories and esthetic involvement, since these patients typically follow distinct functional and reconstructive protocols compared to those with lip involvement.
Procedures
Data collection was conducted in a single session lasting approximately 60 min, after obtaining informed consent from the participants and was carried out by a psychologist experienced in CLP care. The CLEFT-Q instrument and secondary data sources were exclusively used. Authorization for the use of the instrument was obtained from the McMaster Industry Liaison Office. The version administered in this study corresponded to the officially translated Brazilian Portuguese version provided by the Q-Portfolio.
Participants were approached during routine outpatient visits and were not brought exclusively to the hospital for study purposes, minimizing additional burden and preserving ecological validity. During individual appointments, each participant completed the questionnaire scales in printed format under the direct supervision of the principal investigator.
The CLEFT-Q was specifically developed and validated for individuals with cleft lip and/or cleft palate. For patients with other craniofacial conditions or facial anomalies not related to cleft lip or palate involvement, alternative condition-specific PROMs—such as the FACE-Q—may be more appropriate, as they are designed to assess outcomes in broader facial esthetic and reconstructive contexts. Participants with associated syndromes or cognitive impairments that could interfere with comprehension of the instrument were also excluded to ensure reliability of self-reported responses.
The CLEFT-Q is an international self-report instrument developed by Klassen and Wong Riff to standardize the assessment of outcomes perceived by patients with CLP aged 8 to 29 years. Based on Rasch Measurement Theory, it has strong psychometric properties and consists of 12 independent scales and a checklist organized into 3 domains: appearance, facial function, and health-related quality of life. Scores are converted to a 0-100 scale, with higher values indicating better self-perception, allowing for a comprehensive evaluation of the esthetic, functional, and psychosocial aspects of treatment.
In addition to information obtained through the CLEFT-Q, secondary data extracted from participants’ medical records were analyzed
All participants were followed within a multidisciplinary cleft team that includes psychology as part of routine care. However, the frequency, duration, and intensity of psychological follow-up were not controlled as study variables.
Participants’ economic income was classified according to the minimum wage in Brazil for 2024 (R$1412.00 in January 2024, approximately US$288.00). Those with an income of ½ to 2 minimum wages (mean R$1765.00 / US$359.47) were classified as lower-lower class; 2 to 4 minimum wages (mean R$4236.00 / US$863.24) as upper-lower class; 4 to 9 minimum wages (mean R$9178.00 / US$1871.01) as lower-middle class; and 15 to 30 minimum wages (mean R$31,770.00 / US$6472.73) as middle class. 18
For statistical analysis, reliability and correlation tests were performed between clinical and psychosocial variables and the scores obtained with the CLEFT-Q. Normality of distribution was assessed using the Shapiro-Wilk test. Homogeneity of variances was evaluated using Levene's test. Depending on data distribution, comparisons between groups were conducted using Student's t-test or Mann-Whitney U test. Correlations were examined using Spearman's rho.
Results
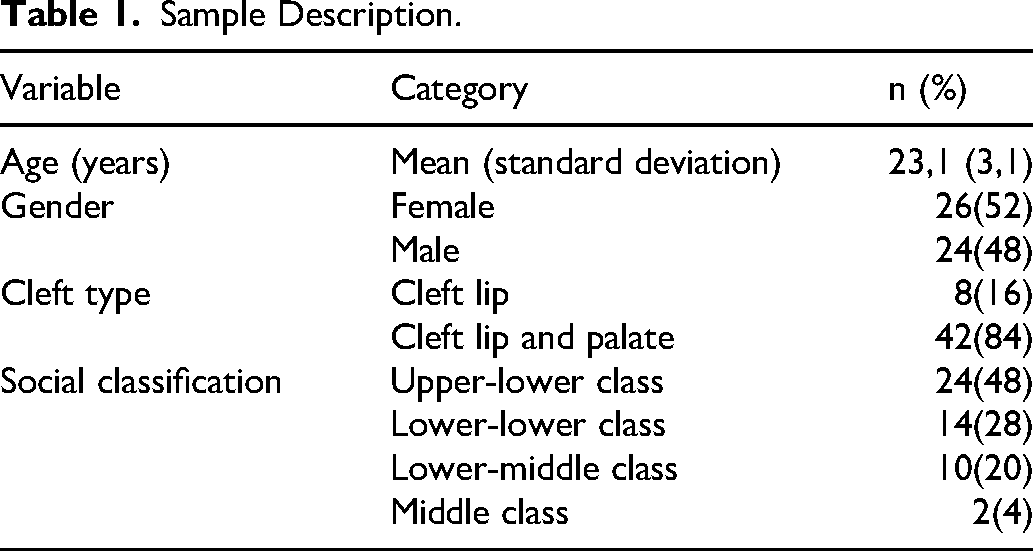
The sample consisted of 50 participants aged between 18 and 29 years (mean = 23.1; standard deviation = 3.1). The sample comprised 26 female participants (52%) and 24 male participants (48%).
Regarding cleft type, the sample was composed predominantly of individuals with CLP (n = 42; 84%), followed by CL (n = 8; 16%).
In terms of socioeconomic profile, the most frequent category was upper-lower class, represented by 24 participants (48%), followed by lower-lower class with 14 participants (28%), lower-middle class with 10 (20%), and middle class with 2 (4%). All participants provided this information during interviews conducted by the hospital's Social Service Department as part of the social assessment process.
The sample also showed wide regional diversity, including participants from 46 different cities across various regions of Brazil—South, Southeast, Central-West, and North/Northeast—demonstrating the heterogeneity and national representativeness of the study's sociodemographic profile. The detailed sample characteristics are presented in Table 1.
Sample Description.
All 50 participants underwent lip repair, with a mean age at the first procedure of 11.8 months (min = 3 months; max = 19.9 years) and a median age of 5 months. Thirty participants (60%) underwent only primary cleft repair, 15 (30%) underwent 2 surgical interventions (mean age = 12 years), and 4 (8%) underwent tertiary cleft repair (mean age = 12.4 years). Only 1 participant (2%) did not undergo cleft repair at the hospital where the study was conducted.
Of all participants, 42 underwent palate repair. Of these, 29 (58%) underwent a single procedure (mean age = 1.8 years), 7 (14%) underwent secondary palate repair (mean age = 3.15 years), 3 (6%) underwent tertiary palate repair (mean age = 5.3 years), 1 (2%) underwent 4 surgical interventions (mean age = 6.6 years), and 2 (4%) underwent 6 palate repair (mean age = 15.8 years).
Columella lengthening surgery was performed in 9 participants (18%), with a mean age of 6.4 years. ABG was performed in 38 participants (76%), with a mean age of 14 years (range: 8.5-20.3 years). Rhinoplasty was performed in 13 participants (26%) at a mean age of 21 years, and orthognathic surgery in 11 participants (22%) at a mean age of 20.7 years. Only 6 participants (12%) underwent veloplasty or pharyngeal flap procedures.
Description of the CLEFT-Q
Table 2 presents the descriptive analysis of the CLEFT-Q scale scores for the overall sample in this study. The results show a wide variability in participants’ responses, reflecting different perceptions regarding appearance, function, and quality of life.
Description of the CLEFT-Q Scales.
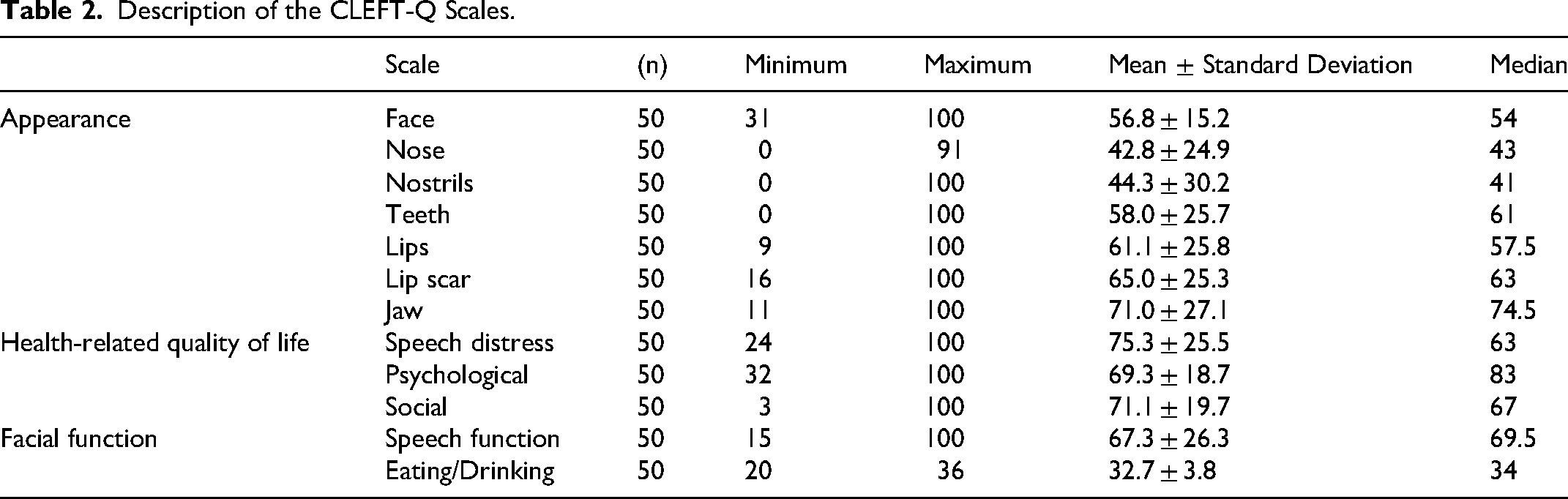
In the appearance domain, the lowest mean scores were identified in the nose (42.8 ± 24.9) and nostrils (44.3 ± 30.2) scales, suggesting lower satisfaction regarding these aspects. Conversely, the highest mean scores were observed for jaw (71.0 ± 27.1), lip scar (65.0 ± 25.3), and lips (61.1 ± 25.8), indicating greater satisfaction among participants in these areas. The face (56.8 ± 15.2) and teeth (58.0 ± 25.7) scales showed intermediate values.
In the facial function domain, the speech distress scale had a mean score of 75.3 (± 25.5), indicating that most participants reported minimal negative impact in this aspect. The score for speech function was 67.3 (± 26.3). For the eating/drinking scale, which is presented as a checklist and has a maximum score of 36 points (indicating absence of complaints), the mean score was 32.7 (± 3.8), close to the maximum value. This result shows that, in the analyzed sample, most participants reported little to no difficulty related to eating and drinking.
Within the health-related quality of life domain, the highest mean scores were observed in the social (71.1 ± 19.7) and psychological (69.3 ± 18.7) scales.
It is important to note that the results presented refer to the overall sample. As each cleft type involves distinct treatment protocols and trajectories, a detailed analysis of CLEFT-Q scores by cleft type was performed (Table 3) to highlight the specific characteristics and needs of each subgroup.
Descriptive Analysis of the CLEFT-Q Scales According to Cleft Types.
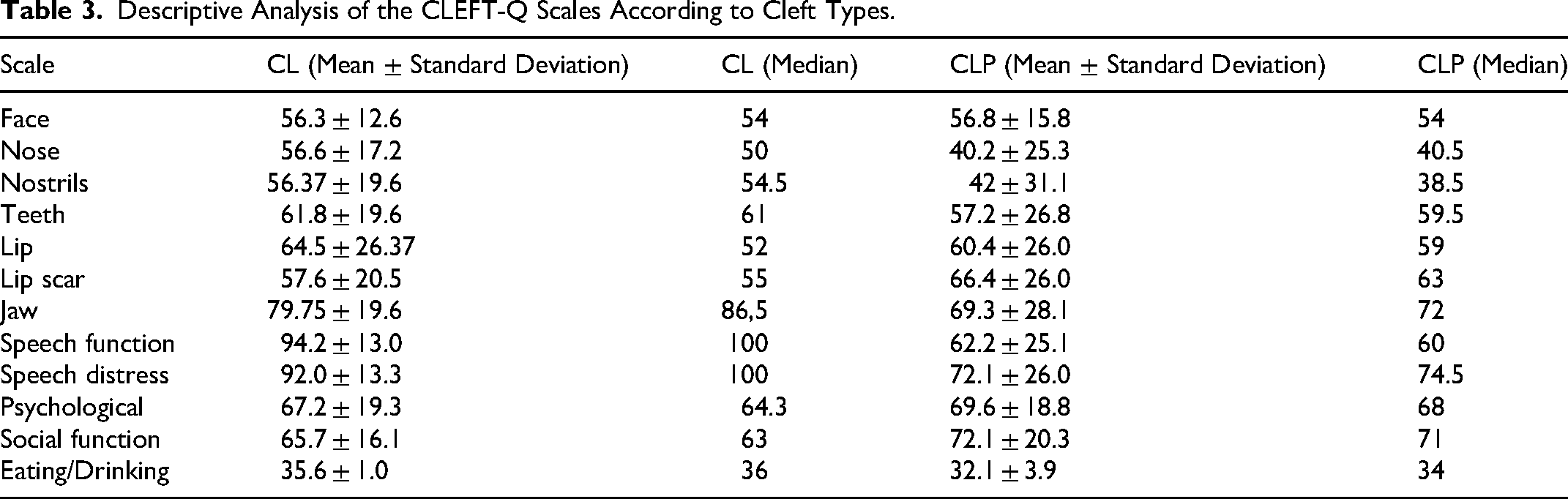
The table presents the mean scores and the median of the CLEFT-Q scales according to cleft type. Among participants with CL, the highest values were observed in the speech function (94, 100), speech distress (92.0, 100), and jaw (79.7, 86.5) scales. Intermediate values were found for lips (64.5, 52), teeth (61.8, 61), and psychological (67.2, 64.3) scales. The lowest means occurred in the nose (56.6, 50), nostrils (56.4, 54.5), and scar (57.6, 55) scales.
In the group with CLP, the highest scores were found in the social function (72.1, 71), psychological (69.6, 68), and jaw (69.3, 72) scales. Intermediate values appeared in the lips (60.4, 59), scar (66.4, 63), and teeth (57.2, 59.5) scales. The lowest means were observed for the nose (40.2, 40.5), nostrils (42.4, 38.5), and face (56.8, 54) scales.
In the eating/drinking checklist, the mean score was 35.6, and the median score was 36 for the CL group and 32.1 ± 3.9 and 34 for the CLP group. Considering that the maximum possible score for this scale is 36 points, the results indicate that both groups presented values close to the upper limit.
Lip repair
Regarding lip repair, most participants underwent a single surgical intervention. Although a relevant proportion (38%) underwent more than 1 lip surgery, no statistically significant differences were found when correlating the esthetic perception of the lips (P = .654) or scar (P = .688) scales according to the CLEFT-Q scores.
Palate repair
As previously described, most patients underwent a single palate repair (58%), but a considerable proportion (26%) required 2 or more palate surgeries, highlighting the complexity of the treatment process. The mean age for primary palate repair was 1.80 years. When correlating the number of palate repair with the speech function (P < .001), speech distress (P < .001), and eating/drinking scales (P = .002), the number of palate repair was found to be directly associated with poorer functional outcomes in the speech and feeding dimensions.
Alveolar Bone Grafting
Regarding the association between the performance of the procedure in patients with alveolar ridge involvement and the perception of dental appearance scale, participants who had not undergone the procedure presented a mean score of 56.7 (SD = 28.9), whereas those who had undergone ABG presented a mean score of 58.1 (SD = 26.8). Despite the numerical difference, statistical analysis revealed no significant difference (t(45) = –0.153; P = .879). The assumptions of normality (Shapiro-Wilk, P = .215) and homogeneity of variances (Levene, P = .835) were met, ensuring the validity of the test.
Rhinoplasty
Among the 50 participants evaluated, only 13 (26%) had undergone rhinoplasty, while 37 (74%) had not undergone the procedure at the time of data collection. The mean age of participants who had the surgery was approximately 21 years. In the nose and nostrils appearance domains of the CLEFT-Q, significant differences were observed between groups.
For the nose appearance scale, the group without rhinoplasty had a mean score of 36.9 (SD = 23.2), while the group that underwent surgery had a mean of 59.6 (SD = 22.4). For the nostrils appearance scale, the non-surgical group showed a mean of 38.6 (SD = 29.4), whereas the surgical group had a mean of 60.6 (SD = 27.0).
Inferential analysis indicated statistically significant differences between groups in both the Student's t-test (nose: t = –3.06; df = 48; P = .004; nostrils: t = –2.37; df = 48; P = .022) and the Mann-Whitney test (nose: U = 108; P = .003; nostrils: U = 145; P = .034). The Shapiro-Wilk test indicated normal distribution for the nose appearance scale (W = 0.983; P = .679) and violation of normality for the nostrils appearance scale (W = 0.947; P = .026).
Orthognathic Surgery
Although patients who underwent orthognathic surgery showed higher esthetic satisfaction scores for the jaw, the difference between groups did not reach statistical significance (P = .088).
Quality of Life and Sociodemographic Factors
Analysis of the CLEFT-Q quality-of-life dimensions showed that, overall, participants presented moderate to high scores on the psychological function, social function, and speech distress scales.
When comparing sexes, the female group exhibited higher mean scores across all evaluated dimensions. In the speech distress scale, women obtained a mean score of 80.5 (SD = 24.2), whereas men scored 69.6 (SD = 26.2). For psychological function, women presented a mean of 68.0 (SD = 16.1), and for social function, a mean of 72.3 (SD = 21.7), compared with 69.8 (SD = 17.8) among men. However, none of these differences reached statistical significance (P > .05), indicating that sex was not a determining factor for perceived quality of life in this sample.
Correlation analysis revealed a significant positive association between age and social function (ρ = 0.317; P = .025), indicating that older individuals reported better social performance. Age showed no significant correlation with psychological function (ρ = 0.281; P = .067) or speech distress (ρ = 0.032; P = .828).
Social level showed no significant associations with any of the evaluated dimensions: psychological function (ρ = –0.062; P = .689), social function (ρ = 0.100; P = .490), and speech distress (ρ = 0.109; P = .450).
Discussion
The treatment of CLP is a long and multidimensional process that requires continuous follow-up and the integrated work of a multidisciplinary team. Each surgical stage represents not only an anatomical intervention but also a symbolic milestone in the reconstruction of the individual's body image and identity. The analysis of this study's results demonstrates that the different surgeries exert distinct impacts on the domains assessed by the CLEFT-Q, encompassing not only functional and esthetic aspects but also psychosocial dimensions relevant to well-being and quality of life.
Lip repair, considered the first surgical intervention in the treatment protocol, was performed in all participants, with a median age of 5 months—different from the age recommended. 8 Although the institutional protocol indicates that the procedure should be performed from 3 months of age, the variation observed may be related to individual clinical conditions such as weight, nutritional status, and comorbidities, as well as to factors related to access to health services, which can influence referral time and surgical availability. 19
Authors have pointed out that there is no absolute consensus on the ideal age, although early surgery tends to favor more satisfactory esthetic and functional outcomes. 20 Despite individual differences and the variable number of interventions, no statistically significant differences were observed in satisfaction scores regarding lip or scar appearance, suggesting that esthetic perception depends more on the surgical technique used, quality of healing, and patient expectations than on the number of procedures performed.
Regarding palate repair, the ideal timing of surgery remains widely debated. The American Cleft Palate-Craniofacial Association recommends performing the surgery before 18 months of age, although most specialized centers perform it between 12 and 18 months. However, recent multicenter evidence has demonstrated a subgroup of patients undergoing palatoplasty as early as 6 months of age, suggesting emerging trends in earlier intervention. Observational studies indicate that later surgery, after 13 or 15 months, may compromise speech outcomes, although it exerts less negative impact on midfacial growth.19-24
In the present study, more than one-quarter of the sample required multiple palate repair, and this condition was associated with poorer functional scores, especially in the speech and feeding domains. These findings reinforce the cumulative impact of reoperations and the decisive role of the primary surgical technique in the effectiveness of treatment—both functionally and in the patient's subjective perception of communicative ability. 25
ABG was performed in 76% of the sample to restore the continuity of the alveolar ridge, facilitate tooth eruption, improve nasal symmetry, and close oronasal fistulas. The literature indicates that the timing of ABG should be guided primarily by dental development rather than chronological age, particularly the stage of eruption of the permanent canine adjacent to the cleft. While the procedure is commonly reported to occur between 8 and 12 years of age, earlier grafting based on dental development, especially prior to canine eruption, has been associated with improved outcomes and greater predictability in graft integration. 26 The mean age observed in the present study (14.08 years) exceeded the ideal range described, which may have influenced participants’ reported esthetic perception. Nevertheless, no statistically significant differences were identified in the teeth appearance scale between groups with and without the procedure, although grafted patients presented slightly higher means. These results suggest that dental esthetic perception depends more on orthodontic alignment and smile harmony than on the presence of the graft itself, although ABG remains a fundamental component of dental rehabilitation, corroborating the observations of other studies. 26
Orthognathic surgery, performed after completion of craniofacial growth, represents one of the final stages of the treatment process, mainly indicated for the correction of maxillary hypoplasia and the restoration of occlusion and facial harmony. This intervention has a positive impact on both esthetics and function as well as on patients’ quality of life.20,26,27 In the present study, satisfaction scores with the maxilla and mandible were higher among participants who underwent the procedure, although the difference did not reach statistical significance. This finding suggests a positive trend, possibly limited by the small sample size and variation in time since surgery. Previous studies 28 have indicated that orthognathic surgery improves facial harmony and occlusion, but psychosocial effects are strongly related to expectations and the psychological support provided during recovery.
Rhinoplasty, considered one of the most relevant steps in the treatment protocol, directly influences nasal symmetry, respiratory function, and esthetic self-perception—factors closely related to self-esteem and quality of life. Although there is no absolute consensus on the ideal timing, it is generally agreed that early rhinoplasty performed together with primary lip repair improves immediate appearance and facilitates social integration, whereas definitive surgery should be postponed until growth completion to ensure more stable outcomes.20,27 Recent studies highlight the importance of incorporating PROMs such as the CLEFT-Q, which can capture the functional, esthetic, and psychosocial impact of rhinoplasty, providing stronger evidence for clinical decision-making. 29
Although most participants (74%) had not undergone rhinoplasty, the operated group presented significantly higher mean scores on the nose and nostrils appearance scales, indicating a direct positive impact on esthetic self-perception. These findings are consistent with the studies29,30 who reported a significant increase in facial satisfaction and quality of life after secondary rhinoplasty. Beyond its functional and esthetic benefits, the procedure also carries symbolic meaning, representing the culmination of the treatment journey and promoting a sense of completeness and re-appropriation of one's self-image.
Furthermore, it is important to emphasize that irregularities in adhering to the ideal surgical timeline can influence perceived outcomes and reinforce the need to ensure continuity and comprehensive cleft care. Interruptions in surgical stages, long intervals between procedures, or lack of psychological support during the process can compromise not only technical results but also the patient's subjective experience of treatment.
The peer assessment is commonly reported in literature, but self-perception proved to be a key component in understanding the experience of individuals with CLP. Authors 21 observed, self-perception of one's own image is an important indicator of psychological health, and its improvement is associated with strengthened self-esteem and social belonging. The application of the CLEFT-Q in this study highlighted its clinical usefulness by capturing discrepancies between technical assessment and patients’ subjective perception. Another study 16 found that routine use of this instrument could modify therapeutic decisions in up to 16% of cases, precisely because it reveals subjective dimensions that do not emerge in conventional evaluations.
When compared with published normative values for individuals with CL, the scores observed in the present sample were generally comparable across most appearance-related domains. Mean scores for lips (64.5 vs 64.8 normative), teeth (61.8 vs 60.4), and jaw (79.7 vs 77.6) were closely aligned with normative data. Similarly, the nostrils scale showed the sample mean was aligned with the normative mean (56.4 vs 57.9 normative); the nose scale presented the sample mean was aligned when compared to normative values (56.6 vs 62.4). The cleft scar score was also modestly lower in the present sample (57.6 vs 61.8 normative).
In contrast, the psychological scale demonstrated a more noticeable discrepancy, with lower mean scores in the current study (67.2) compared to normative values (76.2), suggesting comparatively reduced psychological well-being in this sample. The face and social scales were not directly reported in the present subgroup analysis, and speech-related scales are not available in the normative dataset for isolated CL, precluding direct comparison in these domains.
When compared with published normative values for individuals with CLP, several domains in the present sample demonstrated scores comparable to reference data, while others showed more marked discrepancies. Social function (72.1 vs 71.6 normative), jaw (69.3 vs 64.7), lips (60.4 vs 58.2) and cleft scar (66.4 vs 57.2) scores are similar or aligned with the normative mean values.
In contrast, lower scores were observed in the nose (40.2 vs 53.5 normative), nostrils (42.4 vs 49.7), and face (56.8 vs 60) scales. The psychological scale showed the sample mean was aligned with the normative mean (69.6 vs 72.1), although the difference was modest.
This study 16 reinforces that successful treatment of CLP should not be measured exclusively by clinical or functional parameters but also by the patient's self-perception, which uniquely reflects the impact of treatment on personal and everyday life. In general, the results suggest that participants’ quality of life was not directly related to sex or socioeconomic status but showed a positive association with age, possibly reflecting a process of maturation, resilience, and adaptation throughout adulthood. These findings underscore the importance of a multidisciplinary and patient-centered approach, in which therapeutic success is understood as an integral process encompassing the physical, esthetic, emotional, and symbolic dimensions of treatment.
Finally, it is recognized that this study presents limitations, such as the sample being restricted to a single reference center, which may limit how much the results can be applied to other contexts; the age range between 18 and 29 years, which does not allow analysis of perceptions at other life stages; and the cross-sectional design, which precludes assessment of changes in self-perception over time. An additional limitation of this study is the absence of stratification according to cleft laterality (unilateral versus bilateral), as the relatively small sample size precluded reliable subgroup analyses; therefore, potential differences in functional and esthetic outcomes related to cleft severity and surgical complexity could not be fully explored. Furthermore, individuals with isolated cleft palate (CP) were excluded from the study in order to maintain greater homogeneity in surgical trajectories and esthetic involvement, which limits the applicability of the findings to this subgroup. Additionally, although comparisons with published normative values were conducted descriptively, no statistical testing was performed to assess the significance of these differences, which limits the strength of inferences regarding the alignment or divergence between sample and normative data.
Nevertheless, the findings contribute to expanding the understanding of the role of subjective perception in treatment processes, emphasizing the need for integrated approaches that unite both the technical and the patient's perspectives.
Conclusion
The results demonstrated that, among the sociodemographic variables, only age showed a significant correlation with the CLEFT-Q domains. Specifically, older participants reported better social function scores. Participants who underwent rhinoplasty showed higher esthetic satisfaction scores, especially in the nose and nostrils appearance domains and individuals who underwent multiple palate repairs presented poorer functional scores.
Footnotes
Ethical Approval and Informed Consent Statements
This study was conducted in accordance with the principles of the ethical standards of the Hospital de Reabilitação de Anomalias Craniofaciais of the University of São Paulo (HRAC-USP), Brazil. Ethical approval was obtained from the Research Ethics Committee of the HRAC-USP (approval number: 6.864.690, issued on June 4, 2024).
Consent for Publication
All participants provided written informed consent for participation in this study, including consent for the publication of anonymized data. No identifiable personal information, images, or videos are included in this manuscript. The written consent forms are securely stored by the principal investigator and were not submitted with the article in order to protect participant confidentiality.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.