
Abstract
Objective
This study evaluated the incidence, frequency, types, and risk factors of complications following staged autologous costal cartilage reconstruction for microtia at an academic hospital in Surabaya, Indonesia.
Design
Retrospective descriptive study.
Setting
Academic hospital in Surabaya, Indonesia, serving as a national referral center for microtia.
Participants
Medical records of 122 unique patients with microtia who underwent autologous costal cartilage reconstruction between January 2014 and December 2024 were reviewed. Patients with incomplete records were excluded.
Interventions
Two-stage autologous microtia reconstruction using a costal cartilage framework. Stage-2 elevation was performed using either a temporoparietal fascia flap (TPF) or retroauricular fascial flap (RFF).
Main Outcome Measures
Incidence and type of postoperative complications involving the reconstructed ear, donor site, and neck.
Results
Postoperative complications occurred in 38 of 122 patients (31.1%), with 47 discrete complication events recorded. Complications were more frequent after stage 1 (27 events) than stage 2 (20 events). Stage–1 complications included skin necrosis (18.1%), cartilage exposure (9.0%), cartilage resorption (7.2%), and donor-site hypertrophic scar (5.4%). Stage–2 complications included skin necrosis (7.4%), synechiae (4.4%), auricular hypertrophic scar (4.4%), donor-site hypertrophic scar (7.4%), and wire exposure (1.4%). In stage 2, complications occurred in 25 of 57 TPF patients (43.8%), whereas no complications were observed in 10 RFF reconstructions.
Conclusions
Autologous microtia reconstruction carries a notable complication risk, particularly after stage 1. Smoking, tissue quality, and flap selection may influence outcomes. Careful planning, counseling, flap selection, and postoperative care are essential to minimize complications and optimize results.
Keywords
Introduction
Microtia is a congenital malformation involving the partial or complete absence of the external ear. Globally, microtia prevalence ranges from 1.5 to 17.4 per 10 000 live births, with rates higher among Asian populations compared to other ethnic groups.1–3 Surgical reconstruction aims to restore ear anatomy and improve psychosocial well-being. 4 Reconstruction is usually performed using either autologous costal cartilage or porous polyethylene implants (PPE). 5 At present, autologous costal cartilage is considered the gold standard for auricular framework reconstruction. Nonetheless, information on its long-term outcomes and complication rates remains limited, underscoring the need for further study.6,7
Complication rates in microtia reconstruction vary widely between studies, reflecting differences in technique, follow-up, and patient selection. Individual studies report rates from 0% to 33%. Pooled data from 9415 patients across 253 articles show a rate of 16.2%. A U.S. national surgeon survey found an average complication rate of 13.58%, ranging from 1% to 75%. Rates depended on the reconstruction technique and the surgical stage. 6
In recent years, alloplastic materials like MedPor® are increasingly used instead of autologous costal cartilage for auricular reconstruction. The advantages include earlier intervention, shorter surgery, and precise framework design. However, it is important to note that MedPor® carries higher infection rates (0.62%) and a significant risk of graft extrusion (11.8%). Similarly, silicone frameworks also have higher explantation rates (5.3%) and unsatisfactory cosmetic outcomes (5.3%). 7 These complications highlight the need for adequate soft tissue coverage. Notably, using a well-vascularized temporoparietal fascia flap (TPF) flap with skin grafts can significantly reduce implant exposure and improve results.5,8
Complication rates in microtia reconstruction vary and may be influenced by factors such as smoking, tissue condition, and coverage technique. More studies are needed to clarify these patterns. Better data will guide surgical planning and improve patient outcomes. Accordingly, our study examines complication rates and types in staged microtia reconstruction at our institution and seeks factors that could improve results.
Methods
This descriptive retrospective study was conducted at a tertiary academic hospital and approved by the institutional review board. Medical records of patients who underwent microtia reconstruction between January 2014 and December 2024 were reviewed. All microtia reconstructions were conducted by a single board-certified plastic and reconstructive surgeon holding specific training in craniomaxillofacial surgery and over 5 years of operative experience.
Study Population and Sampling
The target population included patients with microtia who had reconstruction between January 2014 and December 2024. We used consecutive sampling by reviewing all available medical records from this period. Our inclusion criteria were patients diagnosed with microtia who underwent reconstruction with autologous costal cartilage. We excluded patients with incomplete or missing records.
Among the 122 patients included in this study, a total of 138 ears were affected due to the presence of bilateral cases. A total of 55 stage-1 procedures and 67 stage-2 procedures were performed during the study period. As the analysis was conducted per procedure, some patients contributed to both stage-1 and stage-2 groups. Postoperative complications were recorded separately for each stage, with a total of 27 complications observed in stage 1 and 20 complications in stage 2.
Data Collection and Variables
Data were collected from hospital records. Variables included age, sex, affected side, microtia grade, number of surgical stages, type of flap for ear elevation, postoperative complications, and timing of complications.
Data Analysis
All data were entered into Microsoft Excel and analyzed descriptively. We summarized categorical variables—such as patient demographics, side affected, microtia grade, number of stages, and complications—using frequencies and percentages. Complications were organized by reconstruction stage and surgical techniques to compare outcomes between different groups.
A total of 122 unique patients were included in this study, consisting of 106 unilateral and 16 bilateral microtia cases (total of 138 ears). Complication analysis was performed on a per procedure basis, where stage-1 and stage-2 reconstructions were recorded and analyzed separately. Therefore, some patients may be represented in both stage-1 and stage-2 groups if they underwent both procedures during the study period. In cases of bilateral microtia, each reconstructed ear was considered as an independent unit of analysis for surgical outcomes and complications.
Ethical Considerations
Institutional review board approval was obtained. Patient anonymity and confidentiality were maintained.
Result
The demographic and clinical characteristics of the patients are summarized in Table 1. A total of 122 unique patients with microtia were included in this study. The mean age at first surgery was 16.53 ± 8.12 years. Most patients were male, accounting for 92 cases (75.41%), while 30 patients (24.59%) were female. In terms of laterality, unilateral microtia was the predominant presentation, observed in 106 patients (86.87%), whereas bilateral microtia was identified in 16 patients (13.13%).
Demographic Characteristics of Patients from 2014 to 2024.
The annual distribution of surgical procedures showed a clear increasing trend over the study period (Table 1). During the early years (2014–2017), the number of surgeries remained low, ranging from 2 to 4 cases per year. A gradual increase was noted from 2018 to 2019, followed by a marked rise from 2020 onward. The highest number of procedures was recorded in 2024 (32 cases, 26.23%), reflecting increased case referrals and surgical activity at the center.
Within this cohort and across the study period, postoperative outcomes were evaluated. Complications occurred in 38 individuals (31.1%), with a total of 47 discrete complication events documented. Among the 38 individuals who experienced postoperative complications, smoking exposure was identified in 12 patients (eight active smokers and four passive smokers), comprising nine males and three females. Notably, some patients experienced more than one complication, reflecting the multifactorial nature of adverse outcomes following microtia reconstruction.
Stage–1 Reconstruction
In stage-1 cohort (n = 55), a total of 27 postoperative complication events were recorded. Ear-related complications were the most frequent, accounting for 21 events (38.1%). The most common ear complication was skin necrosis (10 cases, 18.1%), followed by cartilage exposure (5 cases, 9.0%) and cartilage resorption (4 cases, 7.2%). Less frequent ear complications included wound infection (1.8%), pressure injury (1.8%), and swelling (1.8%).
Donor-site chest complications occurred in five cases (9.0%), consisting of hypertrophic scarring (5.4%) and wound infection (3.6%). One neck complication was observed (1.8%), presenting as hypertrophic scarring.
Stage-2 Reconstruction
In stage-2 cohort (n = 67), a total of 20 postoperative complication events were documented. Ear-related complications accounted for 15 events (22.3%). These included skin necrosis (7.4%), synechiae formation (4.4%), auricular hypertrophic scarring (4.4%), wound infection (1.4%), pressure injury (1.4%), swelling (1.4%), and one case of wire exposure (1.4%).
Donor-site chest complications were observed in five cases (7.4%), all of which presented as hypertrophic scarring. No neck complications were recorded during stage 2.
The distribution of complications across surgical stages is summarized in Table 2. Ear complications following stage-1 and stage-2 microtia reconstruction are shown in Figure 1.

Ear complication following microtia reconstruction: (A) skin necrosis; (B) cartilage exposure; (C) pressure injury; (D) swelling.
Postoperative Complication of Microtia Reconstruction.
Note: n represents the number of procedures performed at each stage. Some patients may be included in both Stage-1 and Stage-2 groups if they underwent both procedures during the study period. In bilateral cases, each reconstructed ear was considered independently.
Discussion
Microtia reconstruction is a multi-staged surgical procedure often accompanied by a significant risk of postoperative complications. In this study, complications occurred in 38 out of 122 patients (31.1%). Complications were more frequent after stage 1 (27 events) than stage 2 (20 events). This finding aligns with previous reports indicating that the initial operative stage, involving costal cartilage harvesting and primary ear framework insertion, carries greater morbidity.4,5 Although alloplastic materials such as MedPor® and other implants have been increasingly used in some centers for auricular reconstruction, they are not available in Indonesia. Their use requires international importation, which substantially increases cost and limits feasibility for routine clinical practice. Consequently, autologous costal cartilage remains the primary reconstructive material in our setting.
Auricular skin necrosis (Figure 1A) was the most prevalent complication during both stages. In Stage 1, 18.1% of patients developed necrosis, with smoking both active and passive, being the most frequently associated factor. In a previous study, seven of 96 patients (7.29%) undergoing microtia reconstruction were reported to have partial skin necrosis in the postoperative period. Notably, the incidence in our cohort (18.1%) was more than double that previously reported (7.29%), indicating a substantially higher rate of this complication in our series.
Smoking exposure was identified in a subset of patiens with complications, including 12 of 38 patients (eight active smokers and four passive smokers). However, smoking history was not consistently documented for all patients, and formal comparison between smokers and non-smokers or between male and female patients could not be performed. Nevertheless, the relatively high incidence of skin necrosis observed in this cohort compared with the previous report may be influenced by population-level factors.
Previous studies have reported a high prevalence of smoking in Indonesia, reaching 33.8% in the general population in 2018, 9 which places Indonesia among the countries with the highest smoking rates in Southeast Asia. 10 According to a World Health Organization (WHO) report, smoking prevalence among adult males in Indonesia was 62.9%, whereas the prevalence among females was considerably lower at 4.8% during the same period. 11 Consistent with these epidemiological patterns, smoking exposure among patients who developed postoperative complications was identified predominantly in males, with nine males and three females among the 12 patients with documented smoking exposure who developed complications. Although causal inference cannot be established due to incomplete smoking data in patients without complications, smoking in this study should be interpreted as a potential associated factor rather than an independent predictor of postoperative complications. Biologically, tobacco use may exacerbate the risk of microtia-related surgical complications by impairing wound healing and increasing the likelihood of flap-related compromise, primarily through tissue hypoxia and nicotine-induced vasoconstriction, which are critical concerns in microtia reconstruction.12–14
Cartilage exposure (9%) and resorption (7.2%) in stage 1 further underscore the need for adequate soft-tissue coverage and tension-free closure (Figure 1B). A study of 206 autologous ear reconstructions reported 15 cases (7.2%) of cartilage exposure, often tied to mechanical pressure from helmets or sleeping. 15 This suggests the need for stricter postoperative instructions and protective measures (Figure 1C).6,16 Cartilage resorption, though less common, was also reported in 6% in a previous study on long-term complications. Framework resorption usually results from hematoma, infection, or skin pressure. 17
Wire exposure was reported in one case (1.4%); another study found it in 19 (22.6%) of 84 cases using wire. When preparing an auricular frame, wires are buried in cartilage to prevent surface exposure, yet exposure often occurred regardless. In these instances, auricle thinning was observed, caused by atrophy of the skin and underlying cartilage. Thus, the buried wire became exposed as the thinning auricle made the wire relatively larger, eventually tearing through the cartilage and skin. 18
The swelling of the auricle (Figure 1D) induced by food allergy was reported in one case during stage-1 (1.8%) and stage-2 (1.4%) reconstruction. This swelling was triggered by immune dysregulation in response to specific allergens, leading to inflammatory skin reactions. 19 There are still no earlier studies on this microtia complication; therefore, further research is needed.
In stage-2 reconstruction, hypertrophic scarring and synechia of the auricle were among the notable complications. Each was reported in around three cases (4.4%) during the second stage of reconstruction. In a preceding study, hypertrophic scars were also detected in three out of 125 patients (2.4%) and were also present in the postauricular area after the second surgery. 20 Hypertrophic scarring in this region remains unpredictable, often with no clear causative factors, necessitating further research.21,22 Synechia formation following microtia reconstruction is associated with differences in auricular protrusion across regions. Auricular protrusion can be assessed using the cephaloauricular angle (CAA), with an ideal CAA of 30°–40° in Asian populations, 23 whereas in Western countries the ideal range is 20°–35°. 24 From this, it can be concluded that since the CAA in Asian populations is generally wider than in Caucasians, even a slight postoperative decrease in the angle following microtia reconstruction may indicate the presence of synechia.
The choice of ear elevation technique evolved over the study period. During the earlier phase of this series, the TPF was routinely used for stage-2 ear elevation, particularly in patients requiring greater auricular projection. With increasing experience, the retroauricular facial flap (RFF) was subsequently adopted in selected patients due to its shorter operative time, less extensive dissection, and faster postoperative recovery, allowing for earlier hospital discharge. Beginning in 2024, the RFF became the preferred ear elevation technique in our institution when adequate elevation and soft-tissue coverage could be achieved without the use of TPF.
In this study, the use of the TPF in stage 2 was associated with a higher incidence of skin necrosis (see Table 3). This differs from a prior study, which reported partial grafted skin and fascial flap necrosis in one of 29 patients (3.4%) with a history of TPF and in one of 43 patients (2.3%) with a history of RFF. 25 Generally, the use of RFF is considered more favorable during the second stage of reconstruction due to fewer donor site complications, such as reduced visible scarring and lower risk of alopecia, common concerns with the long incision of TPF. 26 In our study, the TPF was predominantly used due to the higher cephaloauricular angle (CAA) standards observed in Asian populations. The TPF offers greater capacity for ear elevation than the RFF, primarily because of its larger flap size. Nonetheless, our center is actively refining the RFF technique to achieve ear elevation comparable to that of TPF while minimizing donor-site morbidity.
Postoperative Complication of Stage-2 Microtia Reconstruction Technique.
Donor site complications, such as hypertrophic scarring, were reported in 9% of stage-1 cases and 7.4% of stage-2 cases. This is consistent with the anterior chest having a higher predilection for keloid formation. Keloids tend to recur following excision, whereas the development of new hypertrophic scars after excision of a previous hypertrophic scar is uncommon. 27 Previous research has also shown that postoperative incisional tension plays a pivotal role in both wound healing and scar formation. Prolonged tension at the surgical site can stimulate surrounding tissues, exacerbate the inflammatory response, and promote neovascularization within granulation tissue, ultimately leading to excessive collagen synthesis and the development of hypertrophic scars. 28
Despite the postoperative complications observed in some cases, the majority of microtia patients following reconstruction demonstrated no complications postoperatively, as illustrated in Figure 2.
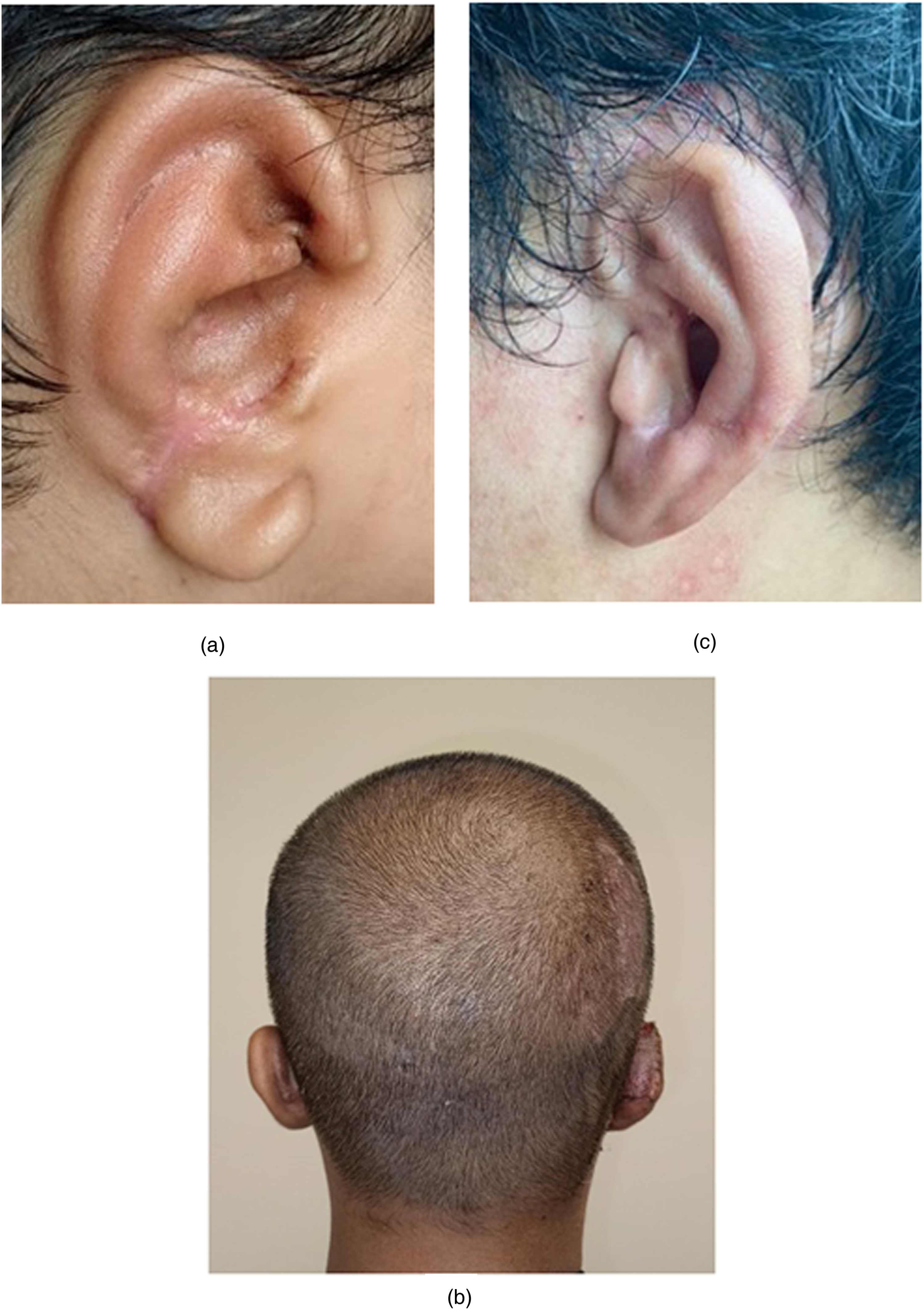
Representative postoperative outcomes without complications following staged autologous costal cartilage microtia reconstruction. (A) Lateral view following stage-1 reconstruction. (B) Posterior view following stage-2 reconstruction. (C) Lateral view demonstrating 6 months of follow-up after all stages of ear reconstruction.
Overall, this study highlights the multifactorial nature of complications in microtia reconstruction. Factors such as smoking exposure, pressure-related injury, and postoperative hygiene may be associated with adverse outcomes, reflecting the complex interplay between patient-related, procedural, and postoperative factors. While causal relationships cannot be established due to the retrospective and descriptive design of this study, these findings underscore the importance of meticulous surgical technique, comprehensive preoperative counseling, and optimized postoperative care. Future prospective studies with standardized data collection and multivariable analysis are warranted to better define independent risk factors and guide further improvement in clinical outcomes.
Limitations
This study has several limitations that should be considered when interpreting the results. First, its retrospective design relied on medical record review, and incomplete documentation may have led to underreporting of complications. Key patient variables, including age, sex, and smoking history, were not consistently recorded, which precluded formal risk factor or regression analyses. Second, this was a single-center study, and the findings may not be generalizable to institutions with different patient populations or reconstructive practices. Third, the sample size limited detailed comparative analysis between reconstruction stages and elevation techniques. In addition, the selection of ear elevation technique was not randomized and evolved over time, with TPF predominantly used in earlier cases and retroauricular fascial flaps (RFF) increasingly adopted in later cases. Finally, follow-up duration was relatively short, limiting assessment of long-term outcomes such as framework stability and late complications. Future prospective, multicenter studies with standardized data collection and longer follow-up are warranted to better define independent risk factors and optimize surgical decision-making.
Conclusion
Microtia reconstruction remains a complex, multi-staged procedure with a notable risk of complications, particularly during the first operative stage. This study highlights the importance of recognizing both patient-related and procedure-specific risk factors, such as smoking exposure, flap selection, postoperative pressure, and tissue handling, which may be associated with adverse outcomes. The relatively high incidence of skin necrosis, cartilage exposure, and hypertrophic scarring observed in our cohort highlights the need for careful surgical planning, meticulous technique, and through patient education. While the RFF demonstrated favourable donor site outcomes, the TPF may be preferred in cases requiring greater auricular elevation, especially in Asian populations with higher cephaloauricular angle (CAA) standards. Further prospective study are warranted to refine flap selection criteria, optimal surgical techniques, and establish evidence-based postoperative care protocols to improve long-term outcomes in microtia reconstruction.
Footnotes
Acknowledgments
The authors gratefully acknowledge all participants who were willing to participate in this research and all the authors who contributed to this original research.
Ethical Statement
This study received ethical approval from Airlangga University Hospital (No. 136/KEP/2024) on September 4, 2024.
Authors Contributions
Conceptualization: ILP; data collection: CDT, IFA; visualization: IFA; methodology: ILP, CRT, RP; writing-original draft preparation: CDT, IFA; writing-review and editing: ILP, IFA; project administration, IFA. All authors have critically reviewed and approved the final draft and are responsible for the content and similarity index of the article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.