
Abstract
This letter is about a recent publication in the Cleft Palate Craniofacial Journal titled: “Posterior Positioning of Levator Veli Palatini with Intact Nasal Layer and Side-by-Side Bilateral Buccinator Flaps: Modified Approach for Palatal Lengthening” in which the authors present a ‘modified’ technique combining both palatal lengthening with buccinator flaps and velar muscles posterior positioning. However, earlier publications including two peer-reviewed articles and a book chapter had already introduced the same conceptual combination, yet these were not cited.
We discuss the technical differences among these procedures, as well as the potential advantages and disadvantages of each. These differences include whether buccinator flaps are used to lengthen only the oral mucosa or both the oral and nasal layers, and whether the velar muscle is dissected in isolation or maintained attached to either the nasal or oral mucosa during retropositioning. Current evidence remains insufficient to determine whether oral-only or dual-layer lengthening provides superior outcomes, or which muscle dissection technique achieves more reliable velopharyngeal competence, as existing studies are limited by relatively small and heterogeneous cohorts, variations in assessment methods, and inconsistent follow-up durations. Further comparative studies are needed to clarify the optimal technique for combining buccinator palatal lengthening with muscle repositioning.
Keywords
We read with interest the article by Hoghoughi et al titled “Posterior Positioning of Levator Veli Palatini with Intact Nasal Layer and Side-by-Side Bilateral Buccinator Flaps: Modified Approach for Palatal Lengthening.” 1 The authors, in the introduction, briefly reviewed the literature on the available surgical methods for VPI treatment. They mentioned the pharyngeal procedures and critically outlined the cons of such obstructive procedures. Then they mentioned the Furlow double-opposing Z-plasty which is considered one of the muscle posterior positioning techniques; however, it is important for the authors to mention also the other popular muscle repositioning techniques of Sommerlad's palate re-repair 2 which they already used in the study. Then, the buccinator flap-based palatal lengthening techniques were mentioned, citing the first report of this technique by Hill et al in 2004, 3 the “buccinator sandwich pushback” and the “double-opposing buccal flap” by Mann et al in 2011. 4 It should be noted that both these are essentially the same technique described under different nomenclature.
There are two approaches to improve the palatal function in patients with VPI, the first, by techniques of posterior positioning of the muscles as Sommerlad midline re-repair “secondary intravelar veloplasty, IVVP” or secondary Furlow double-opposing palatoplasty, the second approach is by palatal lengthening with buccinator flaps. The idea of combining both posterior muscle positioning together with lengthening with buccinator flaps could theoretically provide the best outcome as it provides both lengthening of the mucosal envelope of the palate and posterior muscle positioning and plication. So, we strongly agree with the authors in their use of a “combined” approach for the treatment of VPI. To our knowledge, there are two previously published papers and one book chapter of using such “combined” modified approach which may be worth citation given its conceptual and technical similarities. These include our own series of cases published in the same journal. 5 These techniques, including the authors’ method, and their differences are summarized in Table 1.
Comparison of the Surgical Techniques Used in Published Studies of the Combined Approach.
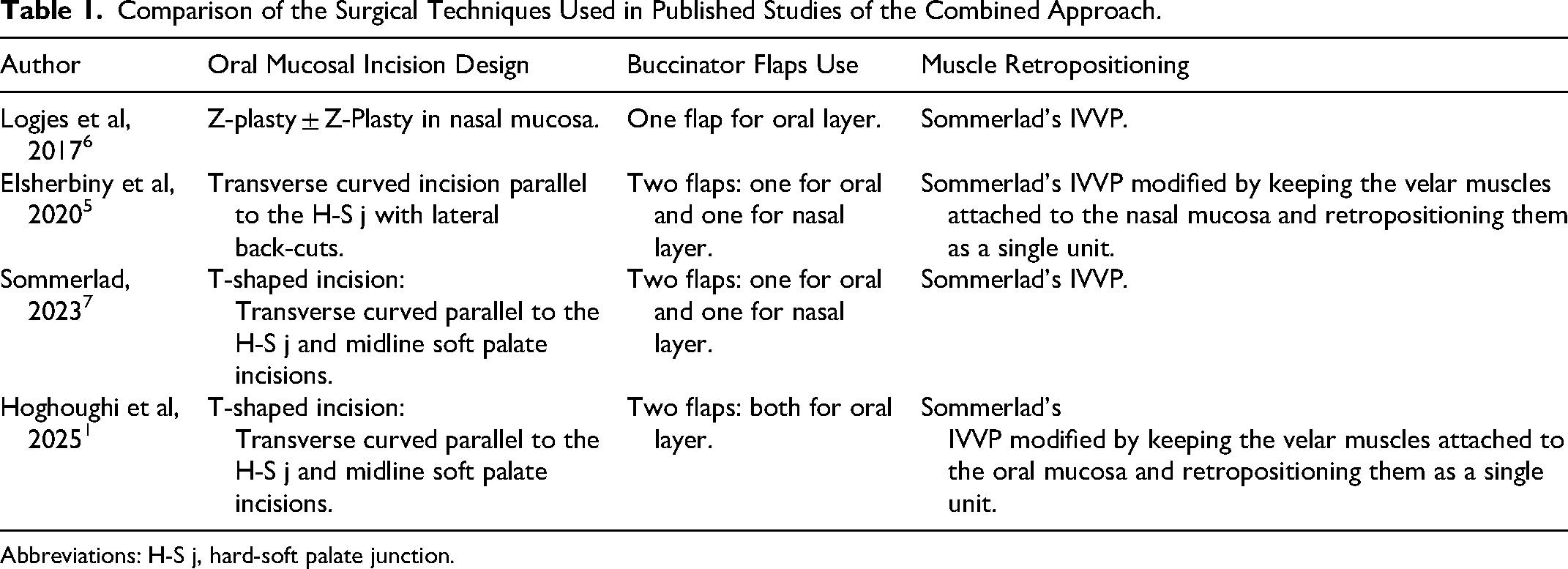
Abbreviations: H-S j, hard-soft palate junction.
The first report was by Logjes et al in 2017 where they treated 42 cases utilizing a Z-plasty of the oral mucosa (60-degree angles) and a single buccinator flap between the two limbs of the Z-plasty for oral mucosal lengthening combined with Sommerlad's muscle posterior positioning. The advantages of this design include the additional lengthening achieved with the Z-plasty, and the authors also claim that a more posterior position of the flap is achieved, allowing the pedicle to be located in the retromolar trigone to prevent potential trauma of the pedicle by biting and the lack of need for pedicle division. 6 Although we have never observed problems with the conventional design of biting the pedicle, even we don’t use bite blocks.
Sommerlad in 2023, in a book chapter, described his experience of performing bilateral buccinator flaps for both oral and nasal mucosal lengthening, together with secondary IVVP for muscle dissection and retropositioning separating the muscles from both the oral and nasal mucosa via a midline soft palate incision in addition to the transverse incision for insetting the buccinator flaps (so it is a T-shaped or arrow-shaped incision). 7
We had observed Sommerlad performing the “combined” procedure during a workshop using his technique, after which we modified the approach and published a study in 2020 including 30 patients treated using a combination of bilateral buccinator flaps for both oral and nasal mucosal lengthening, together with Sommerlad-type intravelar veloplasty for muscle dissection and posterior positioning, which we summarized using the notation (Bs + Re:IVVP) but without separating the velar muscles from the nasal mucosa, as both are posteriorly moved as one unit. We added lateral back-cuts which aid in increasing the soft palate release and retropositioning. Our technique of performing the muscle posterior positioning without separating it from the nasal mucosa offers several advantages including reduced operative time by avoiding the most tedious part of Sommerlad's muscle dissection and the formation of a nasal-side bulge after muscle plication (as the nasal mucosa remains attached to the muscle and therefore is not truly redraped, but instead tends to curl and bulge, unlike when it is dissected from the muscle layer), which aid in velopharyngeal closure. The nasal mucosa is pliable enough to allow effective tightening of the attached muscles without restriction. 5
The authors in 26 patients used two buccinator flaps to lengthen the oral mucosa, without providing a clear justification why they did not lengthen the nasal layer. While we agree that oral mucosal scarring and tethering may have a greater impact on limiting palatal excursion, given the thicker submucosal component of the oral mucosa, this does not negate the importance of nasal mucosal lengthening to free the soft palate completely from anterior tethering and maximize velar lengthening to allow unrestricted velar muscle sling movement. Based on our intraoperative observations, release of the nasal mucosa and its retropositioning are consistently needed to allow unrestricted movement of the reconstructed levator sling. There is a controversy regarding whether nasal layer lengthening is required. Although, in theory, a short palate implies shortening of all its layers, including both the oral and nasal mucosa; therefore, lengthening of both layers appears conceptually necessary. The muscle posterior positioning used by the authors was Sommerlad-type intravelar veloplasty but without separating the velar muscles from the oral mucosa, as both are posteriorly moved as one unit. It is doubtful that keeping the muscles attached to the thick, scarred oral and submucosal layers would hinder muscle plication.
The authors assumed that one of the advantages of using both flaps for lengthening the oral side only is “reducing palate thickness compared to the buccinator sandwich technique, minimizing palatal bulging and interference with food consumption.” In our experience, we have not encountered such complaints among our patients, a cohort that currently exceeds 100 cases and we are not aware of reports of such complaints in the existing literature.3–7 Moreover, we have observed gradual flattening and stretching of the oral-side buccinator flap over time using the sandwich two-flap technique, and the oral flap usually becomes almost the same level of the native soft palate oral mucosa with time. We attribute this to the posterior active pull by the repaired muscle behind the buccinator flaps which forms repeated force on the mucosa causing its flattening and stretching. The role of the buccinator flaps extends beyond simple lengthening; it serves to release scar bands and interpose a more pliable tissue at the fulcrum of the palate (hard-soft palate junction), thereby improving the palatal excursion and functional outcomes. 5
Comparison of the results of these studies provides no clear evidence demonstrating the superiority of one technique over another regarding whether oral-only or dual-layer lengthening, or the method of muscle dissection and retropositioning, provides superior speech outcomes. The published series involve relatively small patient cohorts (26-42 cases), and there is considerable variation in case selection criteria, severity, speech assessment methods, and follow-up duration, all of which make meaningful comparison of outcomes difficult.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.