
Abstract
Background
This study compares clinical and radiographic outcomes in alveolar bone grafting (ABG) using iliac crest bone graft (ICBG) alone, demineralized bone matrix (DBM) with recombinant human bone morphogenetic protein-2 (rhBMP-2), and ICBG with recombinant human bone morphogenetic protein-2 with demineralized bone matrix (rhBMP2/DBM).
Purpose
We evaluated differences in clinical success and radiographic bone formation among grafting techniques for secondary alveolar cleft repair.
Study Design, Setting, and Sample
Retrospective cohort study of patients undergoing secondary ABG for cleft alveolus between 2017 and 2023 at a tertiary children's hospital.
Independent Variable
Type of grafting technique: ICBG alone, DBM with rhBMP-2, or ICBG with rhBMP-2.
Main Outcome Variables
The primary outcome was radiographic success (bony bridging on cone-beam computed tomography). Secondary outcomes included vertical bone height and reoperation.
Covariates
Age, sex, cleft laterality, and graft type.
Analyses
Descriptive statistics and comparative analyses were performed. Statistical significance was set at P < .05.
Results
A total of 432 patients (527 clefts) were included: 196 ICBG, 284 DBM + rhBMP-2, and 47 ICBG + rhBMP-2. Radiographic success was highest in the ICBG + rhBMP-2 group (89.4%) compared with ICBG (65.3%; P = .001) and DBM + rhBMP-2 (61.6%; P < .001). Mean vertical bone height was greater in the ICBG + rhBMP-2 group (7.4 ± 2.6 mm) versus ICBG (4.7 ± 1.9 mm; P < .001) and DBM + rhBMP-2 (4.4 ± 1.2 mm; P < .001).
Conclusions and Relevance
ICBG combined with rhBMP-2 demonstrates improved radiographic bone formation and vertical height compared with alternative grafting strategies, without increasing reoperation rates.
Keywords
Introduction
Alveolar bone grafting (ABG) is a critical component of the cleft care pathway, providing osseous continuity of the maxillary arch to facilitate tooth eruption, orthodontic movement, and long-term dental rehabilitation.1–4 Traditionally, autologous iliac crest bone graft (ICBG) has been considered the gold standard due to its osteogenic, osteoinductive, and osteoconductive properties.5–7 However, donor-site morbidity, postoperative pain, increased operative time, and hospital resource utilization have prompted ongoing investigation into alternative grafting strategies.8,9
Recombinant human bone morphogenetic protein-2 (rhBMP-2), commonly delivered with a carrier such as demineralized bone matrix (DBM), has emerged as a synthetic alternative to autologous grafting in ABG. RhBMP-2 promotes osteoinduction without the need for donor-site harvest and has demonstrated favorable short-term outcomes in achieving alveolar cleft ossification. Prior studies suggest comparable rates of graft incorporation and revision when recombinant human bone morphogenetic protein-2 with demineralized bone matrix (rhBMP-2/DBM) is used in appropriately selected patients, though concerns remain regarding cost, dosing, and variability in bone quality.10–12
Despite low revision rates reported for both ICBG and rhBMP-2-based techniques, the ultimate success of ABG is not solely defined by the need for reoperation. Adequate bone volume and quality are essential to support the eruption of permanent dentition, orthodontic alignment, and future implant-based dental rehabilitation.13,14 Subtle differences in graft performance may therefore have meaningful downstream implications for functional and esthetic outcomes, highlighting the need for comparative evaluation beyond revision alone. As such, radiographic assessment with cone-beam computed tomography (CBCT) can be useful to objectively evaluate graft quality, including alveolar bone formation and alveolar vertical height.15–18
The purpose of this study is to compare alveolar graft success among patients undergoing ABG with ICBG alone, rhBMP-2/DBM, and a combined approach of ICBG augmented with rhBMP-2. Radiographic measurements from CBCT are critical in ABG because they allow precise 3-dimensional quantification of the cleft defect and the graft volume. By evaluating graft outcomes across these commonly utilized techniques, this study aims to clarify relative effectiveness in achieving durable alveolar bone suitable for long-term dental rehabilitation and to inform evidence-based decision-making in cleft care.
Methods
Study Design and Participants
A retrospective cohort study was conducted including patients who underwent secondary ABG with a history of unilateral cleft lip at a single tertiary craniofacial center between 2017 and 2023 with 4 independent surgeons. Ethical review and institutional board approval were waived for this study by the Children's Hospital Los Angeles Institutional Review Board (IRB CHLA-24-00017). Inclusion criteria consisted of patients with an alveolar cleft who underwent ABG using 1 of the following grafting strategies: ICBG alone, rhBMP-2/DBM alone, or a combined approach utilizing ICBG augmented with rhBMP-2. Graft selection was driven mostly by surgeon preference, though patient factors, particularly younger age, also influenced the choice, with some surgeons opting for DBM when patients were considered too small to safely provide sufficient autologous cancellous bone. Patients were required to have pre- and postoperative CBCT imaging obtained at least 6 months following surgery to allow for adequate assessment of graft incorporation. Patients lacking postoperative imaging or those with incomplete clinical records were excluded.
Operative Technique
The procedure is performed under general anesthesia following infiltration of local anesthetic at the cleft site. Sulcular incisions are made parallel to the alveolar cleft and extended into the gingival papillae. A vertical releasing incision is then created over the first molar of the minor segment to facilitate advancement of the gingivoperiosteal flap. Subperiosteal dissection is carried medially along the piriform aperture. The nasal mucosa is carefully separated from the buccal and palatal mucosa surrounding the cleft and subsequently reapproximated to close the oronasal fistula, which then constitutes the apex of the cleft defect. In patients receiving rhBMP-2/DBM, a small absorbable collagen sponge containing rhBMP-2 (INFUSE Bone Graft; Medtronic, Fridley, Minn., USA) is saturated with 2.1 mg of rhBMP-2 solution for 15 min and then rolled into 2 mL of DBM putty (Progenix; Medtronic). This rhBMP-2/DBM construct is then packed into the cleft defect and secured by layering an additional 2-3 mL of DBM putty over the sponge to the level of the gingiva. For patients undergoing iliac crest bone grafting, the anterior superior iliac spine (preferred laterality, usually ipsilateral) is infiltrated with local anesthetic, and approximately 5 mL of cancellous bone is harvested via a percutaneous osteotrephine technique. The cleft defect is filled with cancellous iliac crest bone to the level of the gingiva. For patients undergoing a combined grafting approach, ICBG harvest is performed in standard fashion as described above. Following preparation of the alveolar cleft site with meticulous soft tissue dissection and nasal floor closure, the cancellous iliac crest bone is placed to reconstruct the alveolar defect and establish bony continuity. rhBMP-2/DBM is then applied adjunctively within and around the grafted site to augment osteoinductive potential and optimize graft consolidation. The mucoperiosteal flaps are then advanced and closed in a layered fashion. Postoperative analgesia for autologous ICBG patients includes placement of Gelfoam (Baxter Healthcare, Hayward, California, USA) and a bupivacaine slow-release infusion catheter at the donor site.
Radiographic Assessment
At the time of the study execution, the Carestream 9300 machine provided the highest CBCT image resolution at the lowest radiation dose. 3D CBCT imaging was performed to obtain volumetric measurements of alveolar bone defects and grafts (Dolphin Imaging software, version 11.8, Chatsworth, California, USA). Radiographic graft success was assessed using CBCT imaging obtained a minimum of 6 months postoperatively. All CBCT scans were reviewed using standardized imaging software by investigators blinded to graft type. Two independent reviewers performed the volumetric measurements, and the average of their assessments was used for analysis to ensure reliability. Successful alveolar bone formation was defined as continuous mineralized bone spanning the alveolar cleft between the cleft-adjacent teeth. Figure 1 demonstrates an example CBCT image showing radiographic measurement of alveolar bone formation.
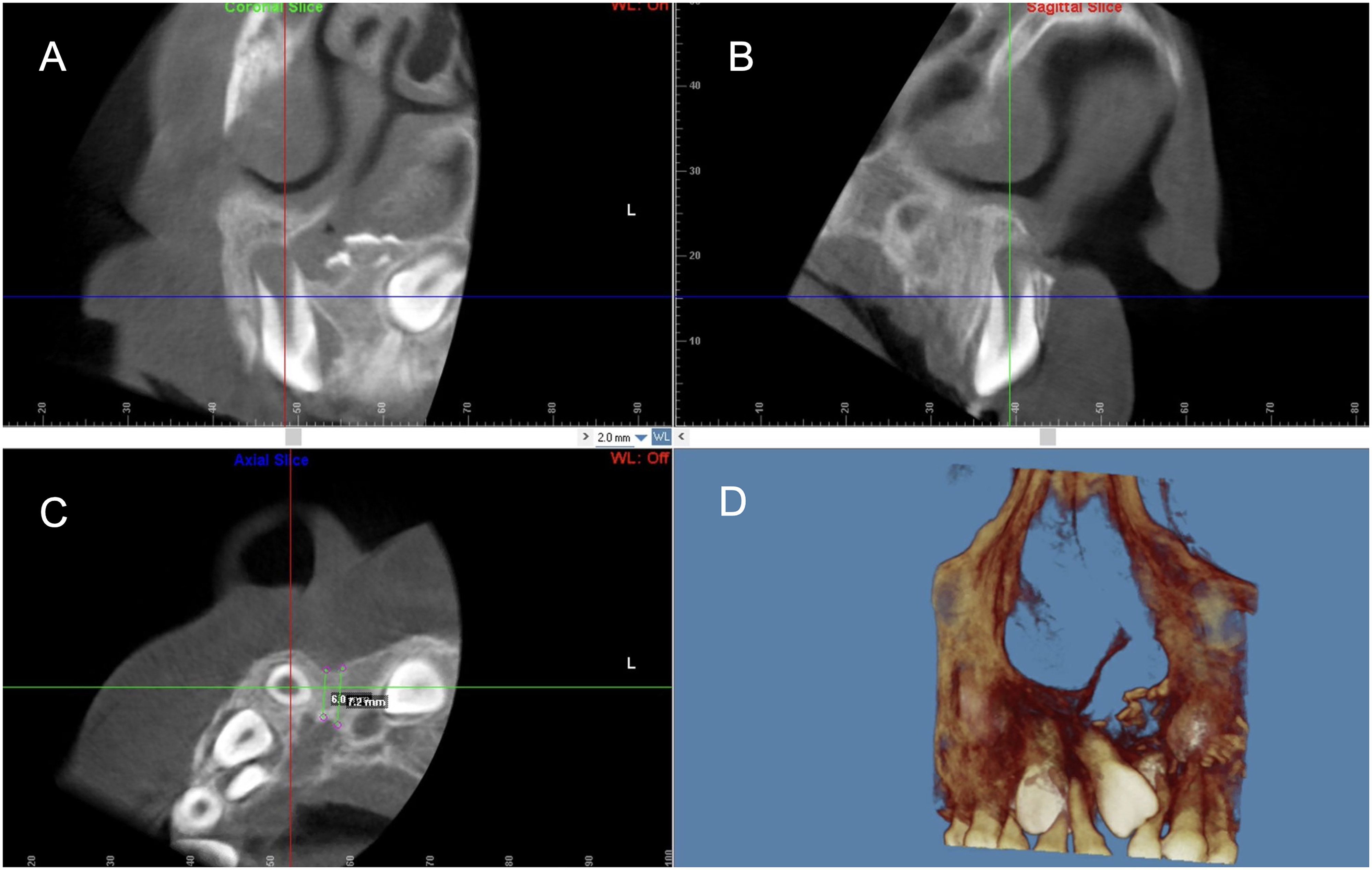
Cone-Beam Computed Tomographic Image Showing Radiographic Measurement of Alveolar Bone Formation. (A) Coronal Slice Demonstrating the Vertical Height of Mineralized Bone at the Alveolar Cleft Site, Measured From the Cementoenamel Junction (CEJ) of the Cleft-Adjacent Tooth to the Apex of the Corresponding Tooth Root. (B) Sagittal Slice Showing the Extent of Bone Formation Along the Alveolar Ridge in the Anterior-Posterior Dimension. (C) Axial Slice Illustrating the Cross-Sectional Width of the Bone Graft and the Spatial Relationship of Adjacent Teeth. (D) 3-Dimensional Reconstruction of the Maxilla Highlighting the Alveolar Cleft and Surrounding Dentoalveolar Structures for Overall Spatial Context.
Vertical height was quantified by measuring the height of mineralized bone at the graft site, defined as the distance from the cementoenamel junction of the cleft-adjacent tooth to the apex of the corresponding tooth root. Measurements were obtained in the sagittal and coronal planes at standardized locations to ensure reproducibility. In each case, slices were oriented along the long axis of the cleft-adjacent tooth and perpendicular to the dental arch, and measurements were obtained at the midpoint of the alveolar cleft defect in both sagittal and coronal planes to ensure uniformity across patients. To confirm true osseous integration, Hounsfield unit measurements were obtained within the grafted region and compared to adjacent native alveolar bone, with only regions demonstrating attenuation consistent with mineralized bone included in height calculations. Any areas of radiolucency or attenuation inconsistent with bone were excluded from measurement.
Statistical Analysis
Descriptive statistics were used to summarize patient demographics, graft characteristics, and follow-up duration. Continuous variables were reported as means with standard deviations, while categorical variables were reported as frequencies and percentages. Reoperation rates and radiographic alveolar bone formation were compared across graft groups. Vertical height measurements were analyzed as continuous outcomes. Appropriate comparative statistical tests were selected based on data distribution. All statistical analyses were performed using Stata software, Version 18.0 (Stata Corp, College Station, Texas, USA). Statistical significance was established at a P-value of less than .05.
Results
Patient Characteristics
A total of 432 patients undergoing ABG were included, accounting for 527 primary grafting procedures between 2017 and 2023. Among these procedures, 196 (37.2%) utilized ICBG alone, 284 (53.9%) utilized rhBMP-2/DBM, and 47 (8.9%) utilized a combined approach of ICBG augmented with rhBMP-2. Mean age was 9.8 ± 1.6 years in the ICBG cohort, 10.1 ± 1.8 years in the DBM + rhBMP-2 cohort, and 10.0 ± 1.7 years in the ICBG with rhBMP-2/DBM cohort, with no statistically significant difference between groups (P = .21). Surgeon-level variation was assessed across the 4 participating surgeons using a chi-square test, and no statistically significant differences in outcomes were identified among surgeons across the 3 treatment groups (P = .11). All patients had adequate postoperative follow-up (17.8 ± 14.2 months) to assess clinical outcomes and underwent CBCT imaging at least 6 months postoperatively.
Reoperation Rates
The overall reoperation rate across all patients was 4.1%. There was no statistically significant difference in reoperation across technique cohorts. Reoperation was indicated in 9 (4.6%, P = .692) patients in the ICBG cohort, 14 (4.9%, P = .705) patients in the rhBMP-2/DBM group, and 1 (2.1%) patient in the ICBG + rhBMP-2 cohort.
Radiographic Outcomes
Radiographic evaluation using postoperative CBCT imaging demonstrated significant differences in osseous outcomes between graft cohorts, with an average imaging interval of 17.8 ± 14.2 months after surgery. Successful alveolar bone formation was observed in 88.9% of patients in the ICBG + rhBMP-2 cohort, which was significantly higher than that observed in the ICBG-alone cohort (65.3%; P = .001) and the rhBMP-2/DBM cohort (61.6%; P < .001).
Quantitative assessment of graft quality revealed that mean alveolar vertical height was greatest in the ICBG + rhBMP-2 cohort (7.4 ± 2.6 mm). This height was significantly greater compared with both the ICBG-alone cohort (4.7 ± 1.9 mm; P < .001) and the rhBMP-2/DBM cohort (4.4 ± 1.2 mm; P < .001). Vertical height measurements were obtained only from regions demonstrating radiographic attenuation consistent with mineralized bone, confirming true osseous integration. A summary of clinical and radiographic outcomes is provided in Supplemental Table 1.
Discussion
The present study demonstrates that the combination of iliac crest bone grafting augmented with rhBMP-2 was associated with significantly higher rates of alveolar bone formation and greater alveolar vertical height compared with ICBG or rhBMP-2/DBM alone.
From a clinical standpoint, the distinction between clinical graft success and radiographic graft quality is critical. The absence of revision surgery does not necessarily equate to sufficient bone stock for orthodontic tooth movement, eruption of permanent dentition, or implant-based dental rehabilitation. CBCT-based evaluation allows for a more granular assessment of graft integration and volume, which is relevant in the pursuit of comprehensive dental restoration. 15 As demonstrated by this study, the improved bone continuity and height observed in the ICBG + rhBMP-2 cohort may therefore translate into greater flexibility in orthodontic planning and improved candidacy for dental implants in adulthood. Liu et al similarly reported that combining rhBMP-2 with ICBG significantly enhances alveolar bone formation compared with ICBG alone, supporting the additive osteoinductive effect of rhBMP-2 observed in our cohort. 19
The enhanced radiographic outcomes seen with graft augmentation in ABG likely reflect the complementary biologic functions of autologous bone and rhBMP-2. Autologous ICBG inherently provides osteogenic cells, an osteoconductive scaffold, and native cytokine milieu that supports early cell survival, vascular ingrowth, and matrix deposition. This triad of osteogenesis, osteoconduction, and early mechanical stability is regarded as the clinical gold standard because it supplies all 3 essential elements for bone repair. Autograft also contains native extracellular matrix that binds growth factors and supports host cell recruitment and differentiation, leading to predictable bone bridge formation over time. 20
In contrast, rhBMP-2 is a potent osteoinductive growth factor belonging to the transforming growth factor-β superfamily, which does not itself contain living cells or a robust scaffold but instead drives host mesenchymal stem/progenitor cell differentiation toward an osteoblastic lineage via canonical BMP signaling. Mechanistically, rhBMP-2 binds BMP receptors on local progenitor cells, activating type I/II serine/threonine kinase complexes and downstream Smad1/5/8 transducers. This, in turn, upregulates osteogenic transcription factors such as RUNX2 and osterix, driving commitment toward osteoblasts and deposition of bone matrix proteins like alkaline phosphatase and osteocalcin.20,21 This osteoinductive stimulus amplifies recruitment and differentiation of host cells from surrounding tissues and bone marrow, increasing bone formation even when initial cellularity is limited.
When combined, these mechanisms can be synergistic: the autograft supplies not only cells and scaffold but also a provisional matrix that retains and localizes rhBMP-2, enhancing the recruitment of host progenitors and accelerating their osteogenic differentiation while maintaining structural support. In contrast, rhBMP-2/DBM alone depends entirely on host progenitor recruitment and differentiation, making it more susceptible to variability in local biologic conditions such as vascularity and progenitor cell availability.20–22
Despite these advantages, the use of rhBMP-2 must be considered in the context of cost, regulatory considerations, and potential complications. Although no differences in clinical failure were observed in this study, the financial burden associated with rhBMP-2 and concerns regarding postoperative edema or ectopic bone formation warrant judicious patient selection. Notably, rhBMP-2 is highly regulated due to safety concerns, including reports of severe complications with off-label use and theoretical tumorigenic potential; in the short term and more commonly, excessive swelling is frequently encountered in the immediate postoperative period. Preclinical studies show that aberrant BMP signaling can enhance cell proliferation and invasiveness in certain cancers, although no direct causal link to malignancy in patients has been proven.23–25 Regulatory guidance therefore emphasizes strict dosing, approved indications, and careful patient selection to minimize these risks.
While this study does provide valuable insights, several limitations should be acknowledged. The retrospective design introduces inherent selection bias, and graft choice may have been influenced by surgeon preference or patient-specific factors not fully captured in the dataset. Additionally, although CBCT provides a robust assessment of osseous outcomes, functional dental outcomes were not directly evaluated. Future prospective studies correlating radiographic graft quality with definitive dental outcomes will be essential to refine indications for graft augmentation and to establish evidence-based algorithms for alveolar cleft reconstruction.
Conclusion
Our findings demonstrate that augmentation of iliac crest bone grafting with recombinant human bone morphogenetic protein-2 is associated with increased rates of alveolar bone formation and significantly greater alveolar bone height compared with either modality alone. Although overall clinical graft success rates were comparable across techniques, the superior radiographic bone quality observed with the combined approach may have important implications for long-term dental rehabilitation. Enhanced bone continuity and height may improve the feasibility of dental implant placement and orthodontic movement across the repaired alveolar cleft, supporting the use of ICBG with rhBMP-2.
Footnotes
Acknowledgements
None.
Ethical Approval
Ethical review and institutional board approval were waived for this study by the Children's Hospital Los Angeles Institutional Review Board (IRB CHLA-24-00017).
Author Contributions
All authors contributed to the study conception and design, data acquisition, analysis and interpretation, manuscript drafting and revision, and approved the final version for publication.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.