
Abstract
Objective
To describe a layered reconstructive technique for full-thickness alar deficiency in unilateral Tessier 1 nasal clefts.
Design
Technical note illustrated by a 2-case series with medium-term follow-up.
Setting
Single tertiary academic plastic and craniofacial surgery center.
Patients, Participants
Two pediatric patients aged 2 and 4 years with unilateral Tessier 1 alar clefts demonstrating full-thickness deficiency of lining, structural support, and external cover.
Interventions
Layered reconstruction using a hinged cutaneous lining flap, auricular cartilage graft support, and dorsal nasal transposition flap for external cover.
Main Outcome Measure(s)
Clinical contour stability, nostril patency, scar quality, need for revision, and caregiver-reported satisfaction.
Results
At 3 and 3.5 years follow-up, both patients demonstrated stable alar contour, maintained nostril patency, no collapse or notching, and no secondary revisions.
Conclusions
The described layered technique provides a feasible reconstructive option for selected Tessier 1 alar clefts with full-thickness deficiency and demonstrated encouraging medium-term stability.
Keywords
Introduction
Tessier 1 nasal clefts are uncommon deformities of the alar unit with variable expression. 1 Their reported incidence is low, representing only a small proportion of craniofacial clefts in most series. Most reported reconstructions rely on local tissue rearrangement, including rotation and transposition of the alar margin.2-4 Although effective when native tissue and cartilage are preserved, these techniques depend on redistribution of often limited alar tissue and may place tension across the alar rim, increasing the risk of distortion, notching, or recurrence in more severe defects.
The ala is a composite structure, and durable reconstruction depends on restoration of internal lining, structural support, and external cover. In the present context, full-thickness deficiency refers to alar rim discontinuity with loss of one or more of these essential components, rendering tension-free repair by local rearrangement alone unreliable. Failure to restore any of these elements predisposes to secondary deformity, most commonly notching or collapse. 5
Published technical descriptions remain comparatively sparse for clefts with true full-thickness loss of lining, structural support, and external cover, in which local rearrangement alone may not provide a stable repair.
The present report describes a layered reconstructive technique that restores all 3 components using predominantly local tissue. Unlike previously described approaches based primarily on tissue rearrangement, this method is specifically intended for clefts with true full-thickness deficiency of the alar unit, where redistribution alone is unlikely to provide a stable repair.
Methods
Two pediatric patients with unilateral Tessier 1 alar clefts underwent reconstruction using the described technique. Both presented with a full-thickness deficiency of the alar unit, involving internal lining, structural support, and external cover at the cleft site. At the time of surgery, the patients were aged 2 years (female) and 4 years (male), respectively. This technical note illustrates the operative approach and medium-term outcomes in 2 patients with long-term follow-up.
Indications for this approach were clinical evidence of alar rim discontinuity with associated deficiency of lining, inadequate structural support, and insufficient local tissue to permit tension-free repair by local rearrangement alone. Accordingly, the technique is primarily intended for unilateral Tessier 1 clefts in which restoration of all 3 components of the alar unit is required and simple redistribution is unlikely to provide a stable repair.
This study was conducted in accordance with institutional ethical standards. Ethical approval was waived by the institutional review board because of the descriptive nature of the report, and written informed consent for publication of clinical images was obtained from the patients’ legal guardians.
Surgical Technique
Lining
A small distally based cutaneous flap is elevated from the external alar skin immediately adjacent to the cleft margin. The flap is typically designed from the cleft margin, where adjacent skin allows turnover for lining without compromising the final external contour or scar placement. The flap is turned inward on its pedicle to create the internal nasal lining. Dissection is kept thin to preserve subdermal vascularity, providing a reliable vascularized lining without the need for grafts.
Support
The lateral alar segment is first mobilized with a partial-thickness incision through the cutaneous and cartilaginous layers, with preservation of the internal lining and its vascularity. Controlled inferior rotation of this segment restores the alar rim to its anatomic position and reestablishes the alar arch without compromising perfusion.
Auricular cartilage is then harvested and selectively contoured to recreate the native alar convexity while minimizing graft visibility and excessive rigidity. Conchal cartilage is preferred because its natural curvature closely approximates the native alar arch. The graft is placed over the newly created lining and secured to the medial and lateral alar remnants, spanning the cleft. Fixation is performed using buried horizontal mattress absorbable sutures placed through the residual alar cartilage–soft tissue complex to ensure stable positioning and minimize graft visibility. By bridging the defect, the graft restores continuity of the alar arch and provides resistance to contractile forces.
Cover
A transposition flap is elevated from the lower nasal dorsum and rotated to resurface the external defect. Flap dimensions are determined after freshening the defect margins and completing lining reconstruction. Slight oversizing is incorporated to facilitate tension-free inset and compensate for anticipated soft-tissue contraction. The flap is inset without tension, restoring contour with an appropriate color and texture match. The extent of lining turnover and dorsal flap recruitment must be carefully balanced, as creation of the internal lining increases the effective external defect; inadequate flap recruitment risks tension, distortion, or alar retraction.
The dorsal donor site is closed primarily without tension, with no observed contour deformity or growth restriction during follow-up.
Closure
Reconstruction is completed by sequential inset of the lining, cartilage framework, and external flap. Scar placement is planned to preserve the alar rim and avoid tension across the reconstructed margin. The stepwise sequence of the layered reconstructive technique is illustrated in Figure 1, and a representative intraoperative application is shown in Figure 2.
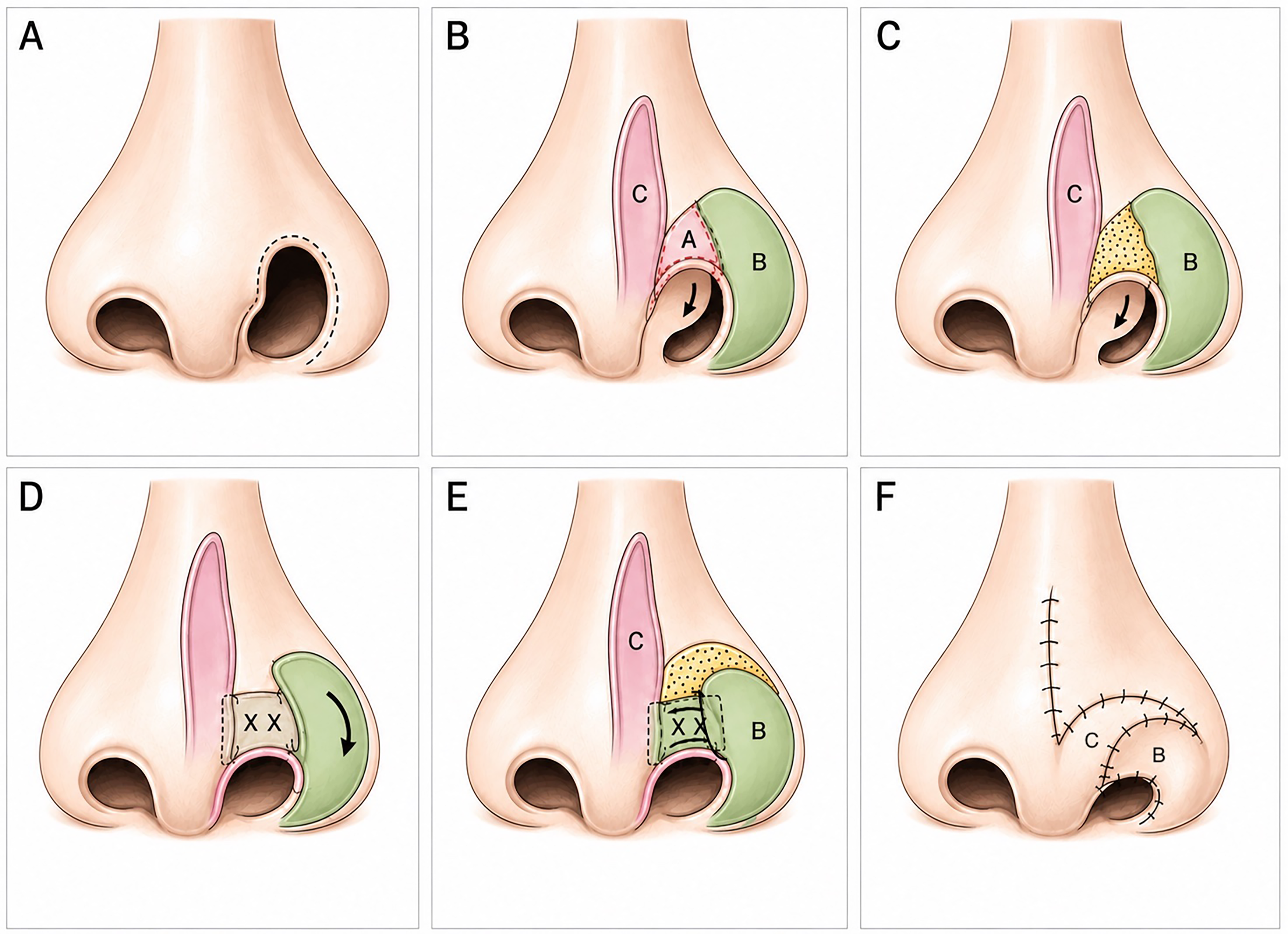
Stepwise layered reconstruction of a Tessier 1 alar cleft. (A) Preoperative appearance demonstrating a full-thickness alar cleft with discontinuity of the alar rim. (B) Flap design. Flap A: hinged cutaneous flap for internal lining; Flap B: lateral alar flap; Flap C: dorsal nasal transposition flap. (C) Flap A is turned inward to reconstruct the internal lining. (D) Placement of auricular cartilage graft to restore structural support and reconstitute the alar arch. (E) Inferior rotation of the lateral alar flap (Flap B) to restore alar position and rim contour. (F) Rotation and inset of the dorsal nasal flap (Flap C) to provide external cover and complete reconstruction.
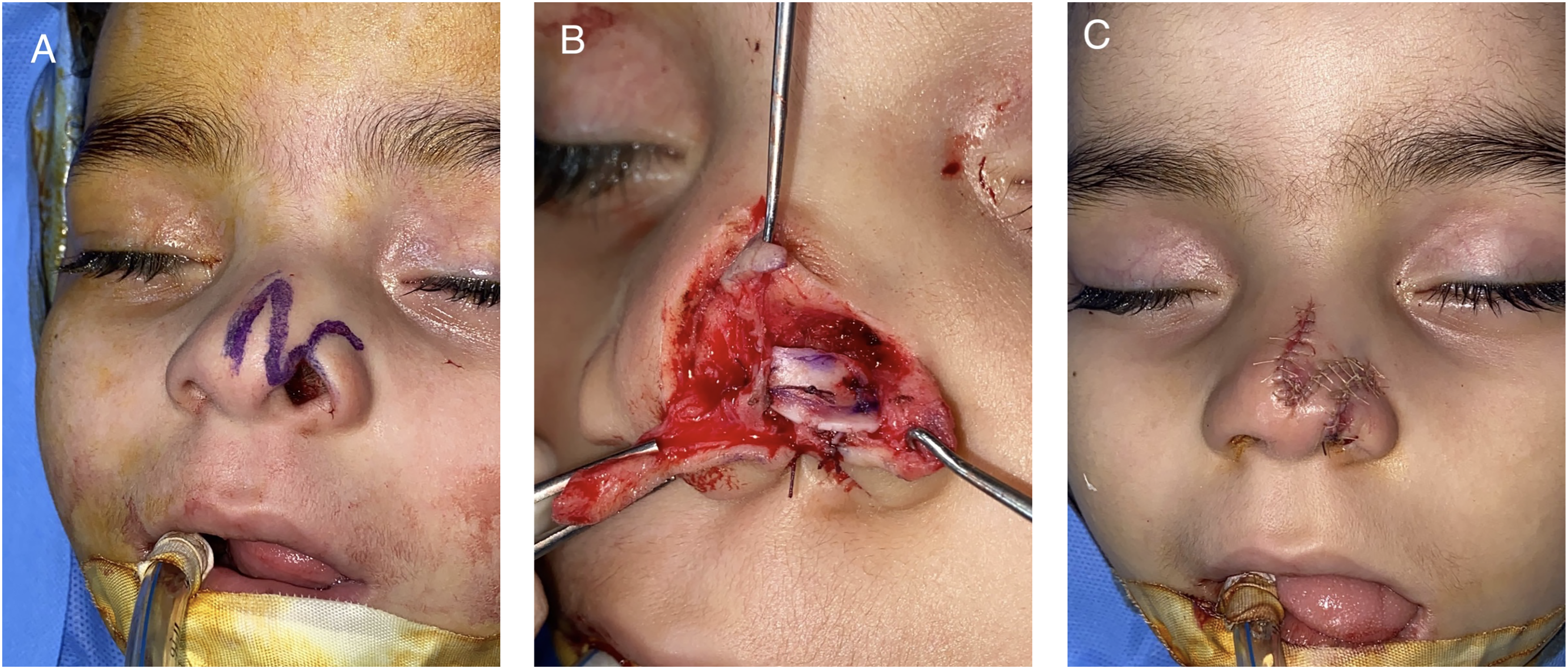
Intraoperative application of the layered reconstructive technique. (A) Tessier 1 alar cleft demonstrating a full-thickness defect, with preoperative markings of the lateral alar flap and dorsal nasal flap. (B) Intraoperative view following creation of internal lining using a hinged cutaneous flap and placement of the auricular cartilage graft. The lateral alar segment is mobilized, and both the alar flap and dorsal nasal flap are elevated. (C) Final inset. The lateral alar segment has been rotated inferiorly to restore alar position, and all flaps are inset to achieve layered reconstruction with restoration of contour and alar rim continuity.
Results
At final follow-up of 3 years in the female patient and 3.5 years in the male patient, both demonstrated stable alar contour with maintained nostril patency. There was no evidence of collapse, notching, progressive asymmetry, or scar-related distortion of the alar margin. Symmetry was assessed clinically by comparison with the contralateral alar contour in frontal and basal views. Representative preoperative and 3-year postoperative outcomes are shown in Figure 3.

Preoperative and long-term postoperative outcomes. (A, B) Preoperative frontal and basal views demonstrating a full-thickness Tessier 1 alar cleft with disruption of the alar rim, loss of contour, and asymmetry of the nostril aperture. (C, D) Three-year postoperative frontal and basal views demonstrating restoration of a smooth alar contour, improved symmetry of the nostril aperture, and a continuous alar rim without evidence of collapse or notching.
Caregiver-reported outcomes were obtained at final follow-up using a single-item 10-point visual analog scale for esthetic symmetry and functional stability. In both patients, caregivers assigned scores of 9/10 for esthetic symmetry and 10/10 for functional stability. Caregivers reported no functional breathing concerns during follow-up.
No donor-site complications, including auricular morbidity, were observed. No immediate postoperative complications, including wound infection, wound dehiscence, or partial flap compromise, were encountered. No secondary revisions were required during the follow-up period.
Discussion
Reconstruction of Tessier 1 alar clefts has largely relied on techniques of local tissue redistribution.2-4 These methods assume relative adequacy of the native alar framework and remain effective in appropriately selected cases. However, in defects characterized by true full-thickness deficiency, redistribution alone may be insufficient to restore all components of the alar unit.
The present technique is based on a fundamental reconstructive principle: restoration of lining, structural support, and external cover.5,6 A hinged cutaneous flap provides vascularized lining and reduces the risk of contracture. An auricular cartilage graft restores structural continuity and maintains alar contour under physiologic forces. A dorsal transposition flap recruits additional tissue without tension, avoiding distortion of the alar rim and preserving the alar–facial groove in contrast to alar-based rotation flaps. This layered approach is combined with controlled repositioning of the residual alar segment, allowing simultaneous correction of tissue deficiency and malalignment.
Compared with previously described approaches, the present technique offers distinct advantages and limitations. Alar rotation and advancement flaps are effective when native lining and structural support are largely preserved, but may be insufficient in defects involving simultaneous loss of lining, support, and external cover. Composite auricular grafts provide lining and cartilage in a single unit; however, graft survival may become less predictable with increasing defect size. 7 Forehead flap reconstruction provides reliable vascularized tissue for larger or more complex deficiencies and can be combined with cartilage grafting, but typically requires staged reconstruction and creates an additional donor site. 5 In contrast, the present approach uses predominantly local nasal tissue and auricular cartilage in a single-stage reconstruction while preserving the alar–facial groove and avoiding a distant facial donor-site scar. Nevertheless, its applicability depends on the availability of adjacent nasal tissue and requires further evaluation in larger cohorts and longer follow-up.
The durability of the reconstruction, maintained for up to 3.5 years, supports the structural basis of the technique. Although based on a limited number of cases, the observed maintenance of contour, symmetry, and nostril patency suggests that restoration of framework integrity may contribute to stable medium-term contour maintenance beyond surface correction alone. Continued follow-up into adolescence remains necessary to assess behavior during periods of rapid facial growth and skeletal maturation. The long-term behavior of the auricular cartilage graft relative to the growth of the native nasal framework remains an important consideration. Differential growth, graft warping, or late asymmetry may become apparent during adolescence and could necessitate secondary revision. Continued longitudinal assessment through skeletal maturity is therefore necessary when counseling families and evaluating the durability of this reconstructive strategy.
Adequate dorsal nasal skin must be available for flap recruitment. Excessive recruitment may distort adjacent nasal subunits or create undue donor-site tension, thereby limiting applicability in larger deficiencies and necessitating alternative methods of tissue replacement.
This technique is not intended for all alar clefts, but specifically for cases with full-thickness deficiency in which restoration of lining, support, and cover cannot be reliably achieved by redistribution alone. Milder deformities with preserved lining and support may be adequately managed with local tissue rearrangement, whereas more extensive defects, including bilateral Tessier 1 or higher-grade clefts, may require additional tissue recruitment or staged reconstruction.
Given the limited sample size, these findings should be interpreted as a technical proof-of-concept demonstrating feasibility and medium-term durability rather than comparative superiority. Further validation in larger series and multicenter experience will be necessary to define reproducibility and broader applicability.
Limitations
This technical note is limited by the small sample size, reliance on caregiver-reported single-item satisfaction scores, and the absence of objective outcome assessment, including anthropometric measurements and 3-dimensional photogrammetric analysis. Although stability was maintained through early childhood, continued follow-up into adolescence remains necessary to evaluate behavior during periods of rapid facial growth and skeletal maturation. Reproducibility across a broader range of cleft severity and among different surgeons remains to be established in larger series. Furthermore, the long-term interaction between auricular cartilage grafts and the growing nasal framework remains incompletely understood, and growth-related contour changes may not become evident until later adolescence.
Conclusions
In alar clefts characterized by full-thickness deficiency, effective reconstruction requires restoration of lining, structural support, and external cover. The described layered technique appears to represent a feasible reconstructive option for selected Tessier 1 alar clefts with full-thickness deficiency and demonstrated encouraging medium-term stability in this small case series.
Footnotes
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.