
Abstract
Objective
To compare parent-proxy and child self-reported quality of life (QoL) for children with cleft lip and palate (CLP) by adoptive status from China.
Design
Observational multi-site study.
Setting
Six North American cleft treatment clinics.
Participants
Children with CLP ages 8.0-10.99 years and their parents (adopted from China, N = 87; not adopted, N = 167).
Outcome Measures
Pediatric QoL Inventories (PedsQL): Parent, Child, Family Impact Module (FIM); CLEFT-Q.
Results
Multivariate analyses of covariance, adjusted for age, race, and socioeconomic status main effects (adoptive status, sex, and interactions of adoptive status with sex) and results were not significant by adoptive status, sex, or the interactions of adoptive status with sex for CLEFT-Q, Parent PedsQL FIM outcomes, or Parent/Child PedsQL subscale outcomes (Ps > .159). Parent-proxy PedsQL School was higher for females regardless of adoptive status (MD = -4.82, CI = -9.53, -.11, P = .045). Child PedsQL Social QoL was higher for children adopted from China (MD = 8.91, CI = 1.18, 16.64, P = .024), where females who were adopted reported higher PedsQL social scores than females who were not adopted (MD = 11.83, CI = 3.09, 20.57, P = .008). Females who were adopted reported higher Cleft-Q Social scores than males who were adopted (MD = -6.95, CI = -18.54, -.54, P = .038).
Conclusions
Child and Family QoL was comparable between children with CLP, aged 8-10 years, who were and were not adopted. Being adopted may confer some protection for social functioning, particularly for females who are adopted.
Introduction
Children with cleft lip and/or palate (CL/P) are frequently adopted, often from foreign countries. 1 Although the rate of international adoptions has slowed in recent years, many of these children continue to be treated by cleft teams in North America. Despite the large numbers of children with CL/P who have been adopted, predominantly through international adoption agencies, there is limited information available on the combined impact of having a CL/P and being adopted on quality of life (QoL).
QoL, defined by the World Health Organization as “individuals’ perceptions of their position in life in the context of the culture and value systems in which they live, and in relation to their goals, expectations, standards, and concerns,” has been identified as an essential component of overall well-being. 2 Issues related to medical conditions and their treatment (called health-related QoL) have been investigated for their impact on QoL with most chronic medical conditions showing an association with poorer QoL.3–7
Quality of Life and Cleft Lip and/or Palate
In keeping with these investigations, the influence of CL/P on children's health-related QoL has received considerable attention in recent years.8–15 Specific factors potentially impacting health-related QoL for children with CL/P include the longitudinal nature of treatment, frequent surgeries, residual lip scarring and nasal asymmetries, speech and hearing problems, and extensive dental needs. 15However, to date, findings regarding the effect of these issues on QoL have been mixed. Multiple studies have shown that a diagnosis of CL/P has limited to no impact on QoL for affected individuals.8–10,13,16–18 Others report specific areas of QoL as impacted by the presence of CL/P with self-esteem, social functioning, speech, and appearance-related distress as the most frequent areas affected.10,12,19–25 Sex and age have also been identified as salient variables when looking at QoL with females and adolescents/adults (using either self- or parent-report) reporting poorer QoL than males or younger children,12,18,26 though results by sex have been inconsistent.17,18
Several researchers have specifically studied oral health-related QoL in individuals with CL/P. Locker et al 27 compared children age 11-14 years with orofacial conditions to a group of children with dental problems. Global oral health-related QoL did not differ between the groups, but children with orofacial conditions reported poorer social well-being characterized by being teased, feeling left out, and avoiding talking with other children. Other studies have shown children and young adolescents to have poorer oral health-related QoL than their peers with severity increasing with age.14,24,28–31 Broder and her colleagues28,32 found that children diagnosed with CL/P reported poorer oral health-related QoL when their surgeon identified surgical interventions recommended for the next year when compared with peers who did not have surgery recommended. There was a noted steady improvement in oral health-related QoL over time across both groups regardless of recommendations or related surgical interventions.
Quality of Life and Adoption
Research on adopted children without CL/P has not often investigated QoL specifically, but the larger body of research on this population has demonstrated some concerns related to increased internalizing and externalizing behavior problems, social skills deficits, drug use, school performance, and referrals for mental health services.33–37 These risks have been identified for both internationally and domestically adopted individuals 34 with adoption after 18-24 months of age along with prior institutionalization and/or neglectful or abusive early care increasing risk.35,38–40
QoL research focused on children with CL/P who were adopted is limited and has generally focused on children adopted from China. Van Veen et al 41 evaluated QoL for 29 children with CL/P under 8 years of age (Mean = 5.8 years) in the Netherlands who were adopted from China compared to 29 Dutch children with CL/P. They reported slightly lower overall parent-proxy QoL with significant differences in satisfaction with treatment and acceptance by peers and family/friends compared to children with CL/P who were not adopted. Salinero et al 42 used a similar approach to compare 64 individuals adopted from China (with the exception of 1 child adopted from India) and 114 non-adopted individuals with cleft lip and palate (CLP) (Mean age = 13 years) using a self-report instrument, the CLEFT-Q. Most appearance scores from the CLEFT-Q were equivalent between the 2 groups, with the exception of a lower rating for global facial appearance for individuals who were adopted. The Speech Function and Speech Distress scales were rated more negatively for individuals who were adopted. Based on the clinical interview, there were no differences in mood, anxiety, or behavior concerns. Finally, Everhart et al 43 conducted interviews with 9 parent–child dyads where the child had been adopted from China prior to 2 years of age. The authors highlighted the resiliency of families with children who are adopted, but also emphasized the social, emotional, and speech challenges faced by these children.
Family Quality of Life
The presence of a child with CL/P in a family frequently results in increased family stress.44–46 Early feeding challenges, fears for the future, sharing information about the cleft with family and friends, and obtaining accurate information about treatment options are some of the hurdles faced by new parents.47–49 There is little information on how adopting a child with CL/P affects family adaptation or QoL. Information on families who adopt children either domestically or internationally suggests that factors such as early adversity, deprivation, and institutional placement may negatively influence placement security and increase disruptions to the adoptive family.50,51 It is possible that the addition of cleft-related treatment including both surgeries and the need for therapeutic treatments such as speech or developmental interventions may further stress the family system and decrease perceived family well-being and parental health-related QoL. However, it is also possible that actively choosing to adopt a child with CL/P mitigates some of the family stress experienced by families who learn their child has CL/P in utero or at birth when this is an unexpected diagnosis. Further, the resources needed to pursue international adoption in particular may be indicative of a lower risk of stress and negative QoL impact related to environmental and social factors for these families (eg, poverty, neighborhood violence, lower education level). There is also some evidence in the cleft literature that family stress eases as the children move beyond the initial surgical interventions, with possible increases or temporary spikes in stress levels when a new surgery is recommended or a new medical problem is identified.52,53 How these various strains affect a family who has adopted a child with CL/P is just now being explored. Losier et al 54 studied attachment security and parental sensitivity in children with CL/P who were adopted and found no differences in attachment security and low levels of behavior problems. They reported that prior parenting experience and maternal sensitivity were protective and may have eased the challenges of parenting a child with CL/P who was adopted. Everhart et al 43 interviewed families and children with CL/P who were adopted from China and identified family acceptance of the child as protective along with encouraging knowledge of CL/P treatment, cultural identity, and providing social-emotional support. Neither paper focused specifically on the impact of adopting a child with CL/P on parental or family QoL, which is an area to be investigated in the current paper.
Hypotheses
The current study compared QoL for children 8-10 years of age with cleft lip and cleft palate (CLP) by adoptive status. We chose this age range to provide a more focused assessment of QoL on middle school children from both parent and child perspectives. Children who are 8-10 years old are able to read and complete questionnaires independently. They have the capacity to think about themselves, how they perform, and how they are viewed by others; peer relationships are becoming increasingly important.55,56 Based on the currently available literature, we hypothesized that: (1) The presence of CLP would have a similar impact on parent perceptions of family QoL regardless of adoption status; (2) Children with CLP who were adopted would report similar scores for appearance and speech compared to children with CLP who were not adopted; (3) Children with CLP will have parent-proxy and self-reported generic QoL scores that are similar regardless of adoption status; and (4) Children with CLP will report similar cleft-specific psychosocial QoL regardless of adoption status.
Methods and Materials
Human Subjects Protection
All procedures were approved by each site's Institutional Review Board (IRB). All parents provided written informed consent, and all minors provided verbal and/or written assent as specified by the site IRB.
Participants
Children, ages 8-10 years old (N = 359), with a confirmed diagnosis of CL/P were recruited between 2016 and 2019 across 6 North American sites, representing large and small cleft treatment teams from a wide geographic area. Children were eligible if: (1) they were between the ages of 8.0 and 10.99 years; (2) parents provided consent and child provided assent; (3) were able to read and understand English or Spanish; and (4) were willing to complete the study questionnaires. Children were excluded if: (1) Child or parent were unwilling to provide consent/assent; (2) Child had a medical condition that might have a greater impact on psychological adjustment, appearance, or learning than the cleft diagnosis (eg, cardiac problems, multiple congenital problems, head injury, significant prematurity [< 34 weeks gestational age]); (3) Child had a craniofacial syndrome with potentially greater impact on psychological adjustment, appearance, or learning than CL/P (eg, craniosynostosis or related syndromes, craniofacial microsomia, Treacher Collins syndrome, 22q11.2 deletion syndrome, Fetal Alcohol syndrome) or (4) Child had a significant cognitive impairment precluding reliable responses to questionnaires. Pierre Robin Sequence without tracheotomy and Van der Woude syndrome were not exclusionary.
Parents/legal guardians of children with CL/P (N = 392) also participated. Parents/legal guardians were eligible to participate if: (1) they were at least 18 years old, were willing to provide written informed consent, and (2) were able to read English or Spanish. Parents/legal guardians of a child with cognitive impairment or who did not provide assent were eligible to complete parent questionnaires. Parent/legal guardian exclusion criteria included: (1) Factors that would preclude the participant's full compliance with or completion of the study (eg, visual impairment, significant cognitive or psychiatric problems); and (2) Parent was unwilling to provide consent for self or child participation in the study. Both parents could participate so long as eligibility criteria were met. Data from the parent/legal guardian who identified as the child's primary caregiver were used in analysis.
Any child who was legally adopted was eligible to participate in the study if proper consent/assent was provided. One hundred and thirteen children were adopted: 13 with cleft lip with or without alveolus (CL ± A), 2 with cleft palate (CP) and 98 with cleft lip and palate (CLP). Given the small number of children with CL ± A and CP who were adopted, only children with CLP are included in this study. Of the 98 children with CLP who were adopted, 87 were adopted from China. To increase the comparability of the group of children who were adopted internationally, only the children who were adopted from China were included. This adjustment resulted in a sample size of 87 children who were adopted from China and 167 children who were not adopted.
Measures
Family Medical History Interview and Chart Review Form
Parents were interviewed about their child's medical history, and a chart review was performed to obtain information about the child's cleft diagnosis and treatment history. For the purposes of this study, caregivers provided demographic information (race and ethnicity), caregiver education, and occupation. Socioeconomic status (SES) status was determined using the Hollingshead Four Factor Index. 57 Two scores are generated by the Hollingshead Four Factor Index: a continuous score, which ranges from 8 to 66 (higher continuous scores indicates higher SES), and a categorical score, which ranges from 1 (high SES) to 5 (low SES). Average SES scores (Category 3) range from 30 to 39. We also recorded the age at primary lip and palate closure and the total number of cleft-related surgeries performed to date. When 2 procedures were performed within the same operating room visit (eg, PE tubes with palate closure), it was counted as 1 cleft-related surgery.
Appearance and Speech Function
CLEFT-Q. 58 The CLEFT-Q is a self-report measure developed for persons with CL/P ages 8 to 29 years. For all scales, total raw scores are converted to Rasch Transformed scores on a scale of 0-100 where higher values indicate less distress about appearance, speech, and psychosocial functioning. The CLEFT-Q has acceptable reliability and validity with good ability to discriminate by cleft type. 59 Clinical risk for was defined as a child falling in the lowest tenth percent (and ties) of responses for each scale.
The CLEFT-Q includes 6 scales that assess how the individual feels about their appearance: Face (9 items), Lip (9 items), Lip Scar (7 items), Nose (12 items), Nostril (6 items), and Dental (8 items); 2 measures that assess speech: Speech Distress (10 items) and Speech Function (12 items) at the time of administration. Each appearance-related item scale asks how much a child likes various features (eg, How much do you like….how your nostrils look in the mirror). Appearance items are rated on a 4-point scale (not at all, to very much). The speech scales ask the child to respond to statements such as “It is hard for my friends to understand my speech” or “I get teased about my speech” using a 3-point scale (‘never,’ ‘sometimes,’ ‘always’) based on their experiences in “the past week.”
Health-Related Quality of Life Outcomes
CLEFT-Q Psychosocial outcomes. The CLEFT-Q scales measuring psychosocial outcomes, including Psychological, Social, and School functioning based on experiences during the past week, were used to provide a cleft-specific measure of health-related QoL. The Psychological scale assesses mood (“I am happy with my life”) and self-confidence (“I am proud of myself”). The Social scale assesses friendship (“My friends accept me”) and cleft-related social perceptions (“it's okay when people look at my face”). The School scale assesses social acceptance in school (“I feel accepted at school”; “I get asked to join activities and games at school”) and mood while in the school setting (“I am happy at school”). All items are rated from 1 to 4; Not at all, A little bit, Quite a bit, Very much. Total scores are transformed to Rasch scores on a scale of 0-100 with a higher score indicating better QoL. Clinical risk was defined as a child falling in the lowest tenth percent of responses for each scale.
Pediatric Quality of LifeTM (PedsQL). 60 The PedsQL is a widely used, 23-item, reliable, and valid measure of health-related QoL in the past month with parallel parent-proxy and child versions. We used the Parent and Child forms (Version 4.0 ages 8-12 years) obtaining ratings from both reporters for the Physical (ease of doing daily activities such as running and pain), Emotional (feelings of fear, anger, worry), Social (acceptance by peers), and School Functioning (attention, focus, missing school because of illness or doctor appointments) subscales (5 items each) and the Total Score for this study.
Pediatric Quality of LifeTM Family Impact Module (PedsQL FIM). 61 This reliable and valid parent-report measure consists of 36 Likert-scale items that assess how pediatric chronic health conditions impact parental health-related QoL and family functioning. The Total score (average of 36 items), Parent health-related QoL (Parent HRQoL) Summary Score (the average of the physical, emotional, social, and cognitive scales; 20 items), and Family Functioning Summary Score (the average of the daily activities and family relationship scales; 8 items) were used in this study.
The PedsQL and PedsQL FIM items are rated on a 5-point scale from never to almost always. Scale totals are transformed into standardized scores ranging from 0 to 100. Higher scores indicate more positive ratings of QoL and lower treatment burden. Clinical risk cutoffs for the Parent and Child PedsQLs, and the PedsQL FIM were determined based on published norms (1 SD below the mean).62,63 The cutoff for the Parent PedsQL was a score less than 65.42, and for the Child PedsQL, a score less than 69.71. For the PedsQL FIM, the cutoff was 63.94.
Statistical Methods
The SPSS software (Version 30.0.0.0) 64 was used for statistical analysis. Alpha was set at P < .05. The Bonferroni adjustment was applied for multiple comparisons.
Descriptive statistics (frequencies, percentages, means, and standard deviations) were calculated, and continuous variables were examined for equality of variance. Chi-Square was used to compare categorical data and analysis of variance for continuous variables. The Welch statistic is reported when equality of variance is violated.
Multivariate Analysis of Covariance
A series of multivariate analysis of covariance (MANCOVA) tests was run using Adoptive Status (yes/no), child sex at birth (male/female), and the interactions of adoptive status/sex as independent variables. Child age, race (white/other), and family SES were identified a priori as adjustment variables for all analyses based on findings from previous research on children who were not adopted. 65 Outcome variables are as follows:
Appearance and Speech. Two separate MANCOVAs were run. The first assessed appearance and included the CLEFT-Q Face, Nose, Nostril, Lips, Lip Scar, and Teeth as outcome variables. The second MANCOVA focused on speech outcomes using the CLEFT-Q Speech Distress and Speech Function scales.
Health-related QoL. MANCOVAs assessing QoL outcomes included the Parent-reported PedsQL FIM Family Health-Related, Family Impact and Total composite scales; and Parent and Child PedsQL Physical, Emotional, Social and School QoL subscales. Cleft-specific psychosocial QoL was evaluated using the CLEFT-Q Psychological, Social, and School measures.
MANCOVA results are reported as Wilks’ lambda due to heterogeneity of variance and unequal cell sizes. 63 Univariate analyses are based on F scores after Bonferroni correction. Bonferroni adjusted P-Values are still reported with alpha < .05 because SPSS adjusts the Bonferroni correction so it is comparable to alpha < .05. 66 Effect sizes are reported as partial eta squared (ηp2): ηp2 = 0.01, small effect size; ηp2 = 0.06, medium effect size; and ηp2 = 0.14, large effect size. 67
Results
Descriptive Statistics
A total of 254 participants were included in the analysis. There were 227 parent–child pairs; 23 parent-only enrollees; and 4 child-only enrollees. Of the total enrollees, 167 children were residing with a biological parent or guardian, and 87 were residing with their adoptive parents. Child age did not differ by adoptive status (P = .448). Children who were adopted were more likely to be female (Chi-square = 14.85, P < .001) and reside in homes of higher SES than children who were not adopted (Welch = 93.06, P < .001) (Table 1).
Descriptive Data by Adoptive Status of Participants.
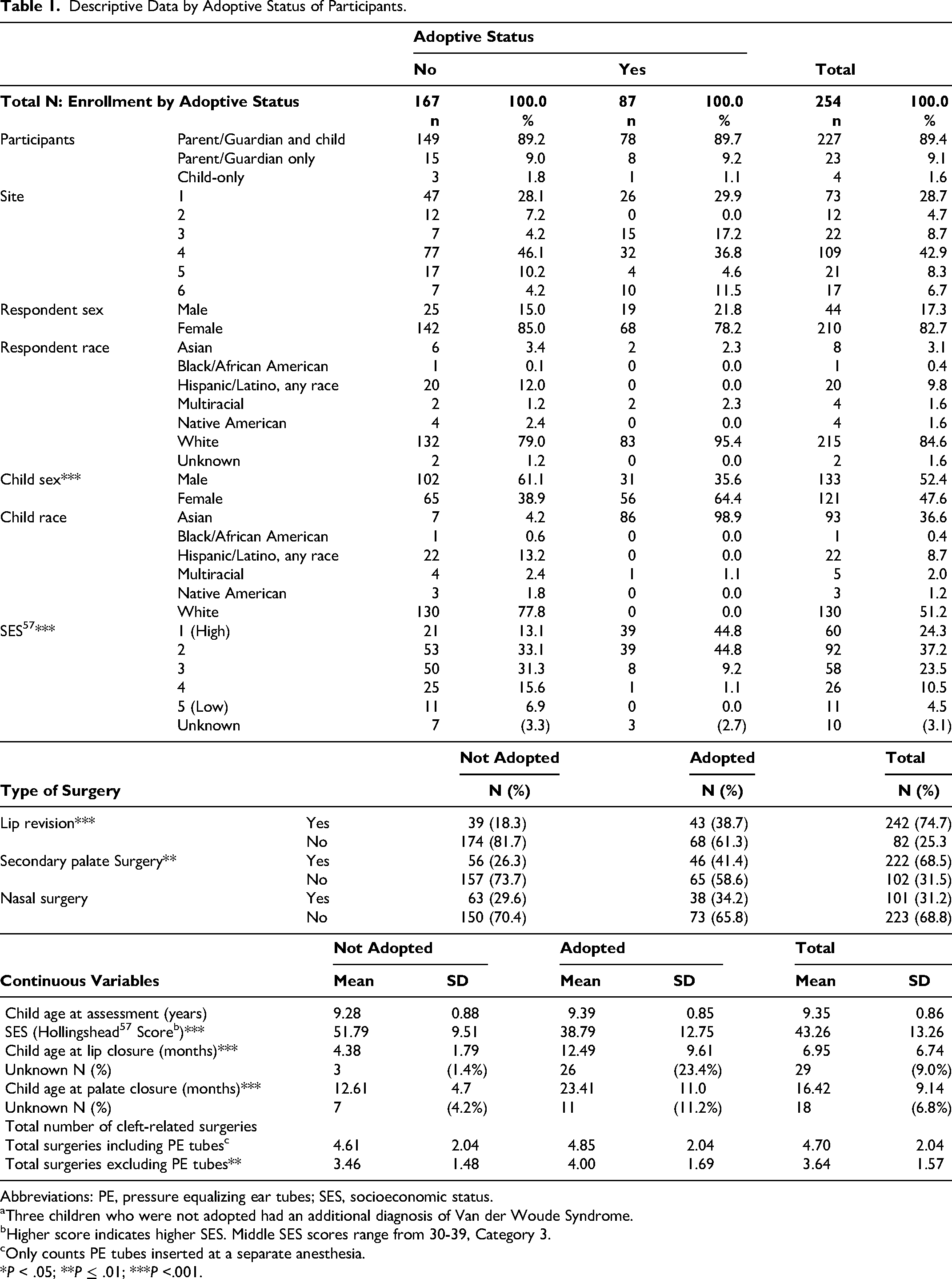
Abbreviations: PE, pressure equalizing ear tubes; SES, socioeconomic status.
Three children who were not adopted had an additional diagnosis of Van der Woude Syndrome.
Higher score indicates higher SES. Middle SES scores range from 30-39, Category 3.
Only counts PE tubes inserted at a separate anesthesia.
*P < .05; **P ≤ .01; ***P <.001.
Surgical Interventions. Primary cleft lip and palate surgeries were performed at an older age for children who were adopted compared to those who were not adopted: CL surgery Mean difference (MD) = 8.31 mos. (F(1227) = 108.09, P < .001, ηp2 = .32) and CP surgery MD = 11.51 mos. (F(1234) = 121.87, P < .001, ηp2 = .342). Children who were adopted were more likely to have a lip revision (Chi-square = 9.82, P = .002) and require a secondary palate surgery (Chi-square = 4.48, P = .034). Children who were adopted from China also had more cleft-related surgeries, excluding pressure equalizing tubes, than children who were not adopted, after adjusting for age (MD = .57, F(1251) = 7.63, P = .006, ηp2 = .03) (Table 1).
Unadjusted Outcomes. Valid scores were available for 98-99% of parent-proxy outcome instruments and 96-98% of child self-report outcome instruments (Supplemental Table 1). There were a few significant differences in unadjusted scores based on adoptive status. Children who were adopted reported significantly lower scores on the CLEFT-Q Psychological scale (F (1214) = 9.51, P = .003). Parents of children who were adopted reported higher physical QoL on the PedsQL Physical scale (Welch = 5.44, P = .020) (Supplemental Table 2).
Clinical Risk. There were minimal differences in clinical risk for PedsQL FIM by adoptive status (not adopted, 13.6%; adopted, 12.8%). Although not statistically significant, children who were not adopted fell into the clinical risk category more often than children who were adopted (Parent PedsQL Clinical Risk: not adopted, 13.8%; adopted, 5.8% (Odds Ratio = 2.38) and Child PedsQL Clinical Risk: not adopted, 19.6%; adopted, 11.4% (Odds Ratio = 1.72). There were also a few differences in the percentage of children who reported scores in the lowest 10% on the CLEFT-Q scales. Although also not statistically significant, children who were not adopted were more likely to report low scores on the CLEFT-Q Teeth scale (11.7% to 5.1%, Odds Ratio = 2.31) (Supplemental Table 2).
CLEFT-Q Facial and Dental Outcomes
Figure 1 shows mean scores for the CLEFT-Q appearance scales after adjusting for SES, race, and child age (International means provided for comparison but not included in analyses). After adjustment for SES, race, and age, MANCOVA results were not significant by adoptive status, sex, or the interactions of adoptive status by sex on CLEFT-Q appearance and dental outcomes using Wilks’ lambda (all P's > .346). Additionally, there were no significant univariate effects (all P's > .121) (Supplemental Table 3).
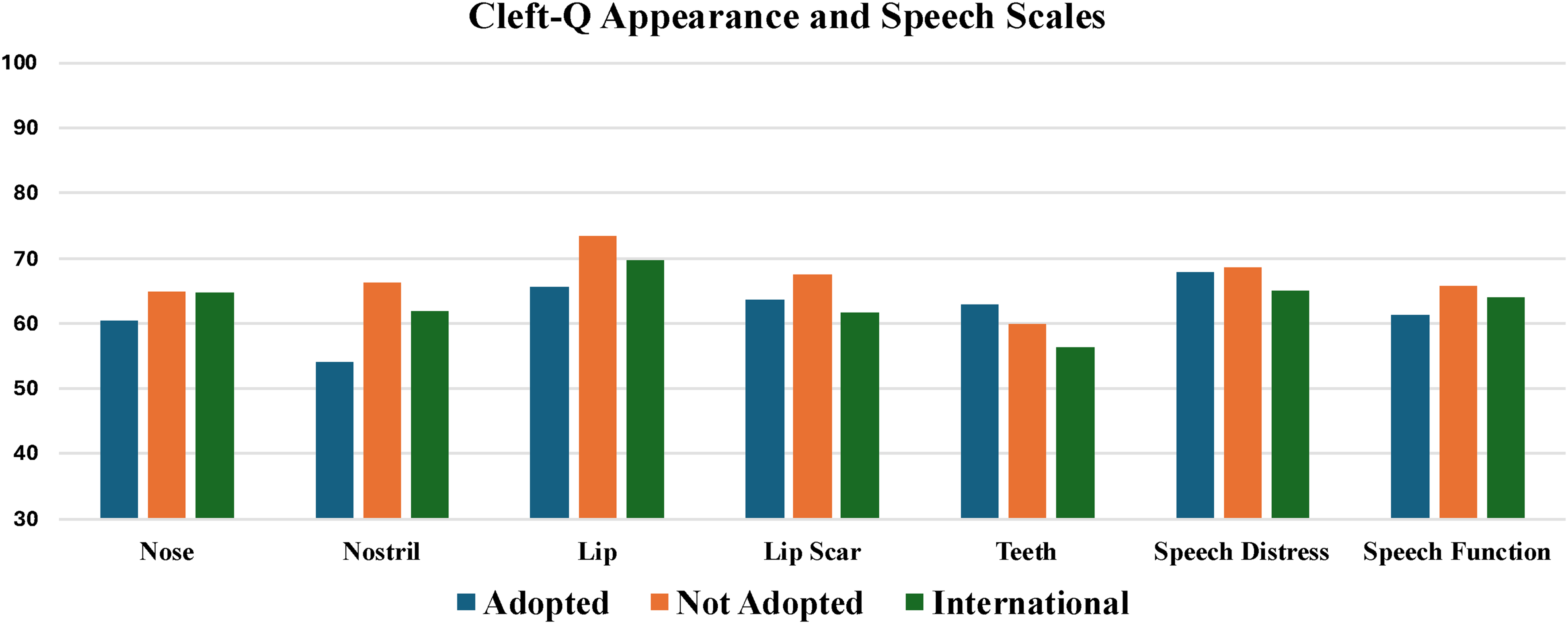
CLEFT-Q appearance and speech mean scores adjusted for child age and race and family SES. Normative data for CLEFT-Q from Klassen et al. 59
CLEFT-Q Speech Outcomes
After controlling for SES, race, and child age, there were no significant effects by adoptive status, sex, or the interaction of adoptive status and sex on self-reported speech outcomes for children with CLP using Wilks lambda (all P's > .268). Additionally, there were no significant univariate effects (P's > .131) (Supplemental Table 3). Figure 1 provides mean scores after adjustment for SES, age, and race for the speech outcomes.
Health-Related Quality of Life
Parent PedsQL Family Impact. Using Wilks’ lambda, there were no significant effects of adoptive status, child sex, or the interactions between adoptive status and sex on family QoL after adjusting for SES, parent race, and child age (all P's > .578). There were no significant univariate effects for adoptive status, sex, or the interactions of adoptive status with sex (all P's > .567) (Supplemental Table 4). Figure 2 provides adjusted mean scores for the PedsQL FIM by adoptive status of child.
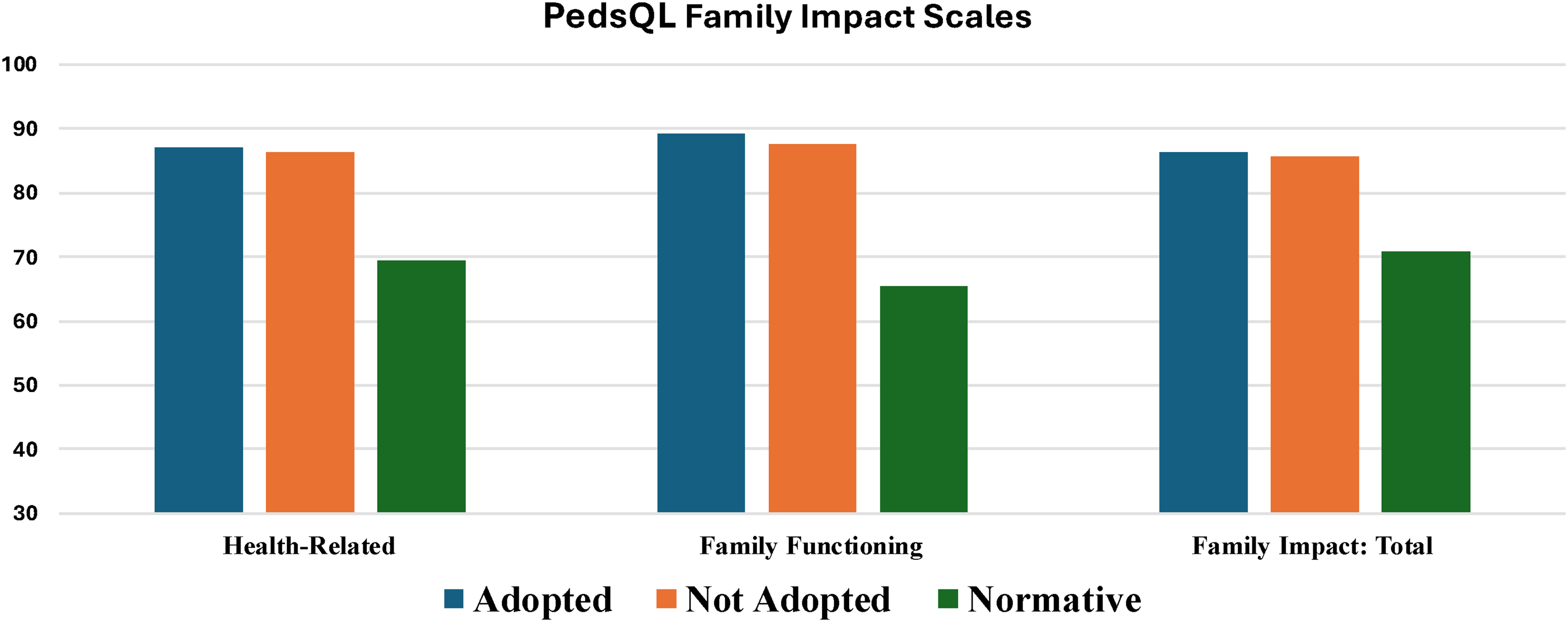
PedsQL FIM mean scores by adopted Status adjusted by SES, child age, and parent race. Normative data from a community sample. 63 .
Parent PedsQL. After adjusting for SES, child race, and child age, there were no significant effects of adoptive status, sex, or the interactions of adoptive status and sex on the Parent PedsQL using Wilks’ lambda (P's > .164). There was a significant effect of sex on the Parent PedsQL School scale (F1,228 = 4.07, P = .045, ηp2 = .02) (Table 2). Male children received lower scores on the School scale than females (MD = -4.82, CI = -9.53, -.11, P = .045). This was true for males who were not adopted and males who were adopted (Table 3).
Parent and Child PedsQL and Child CLEFT-Q MANCOVA.
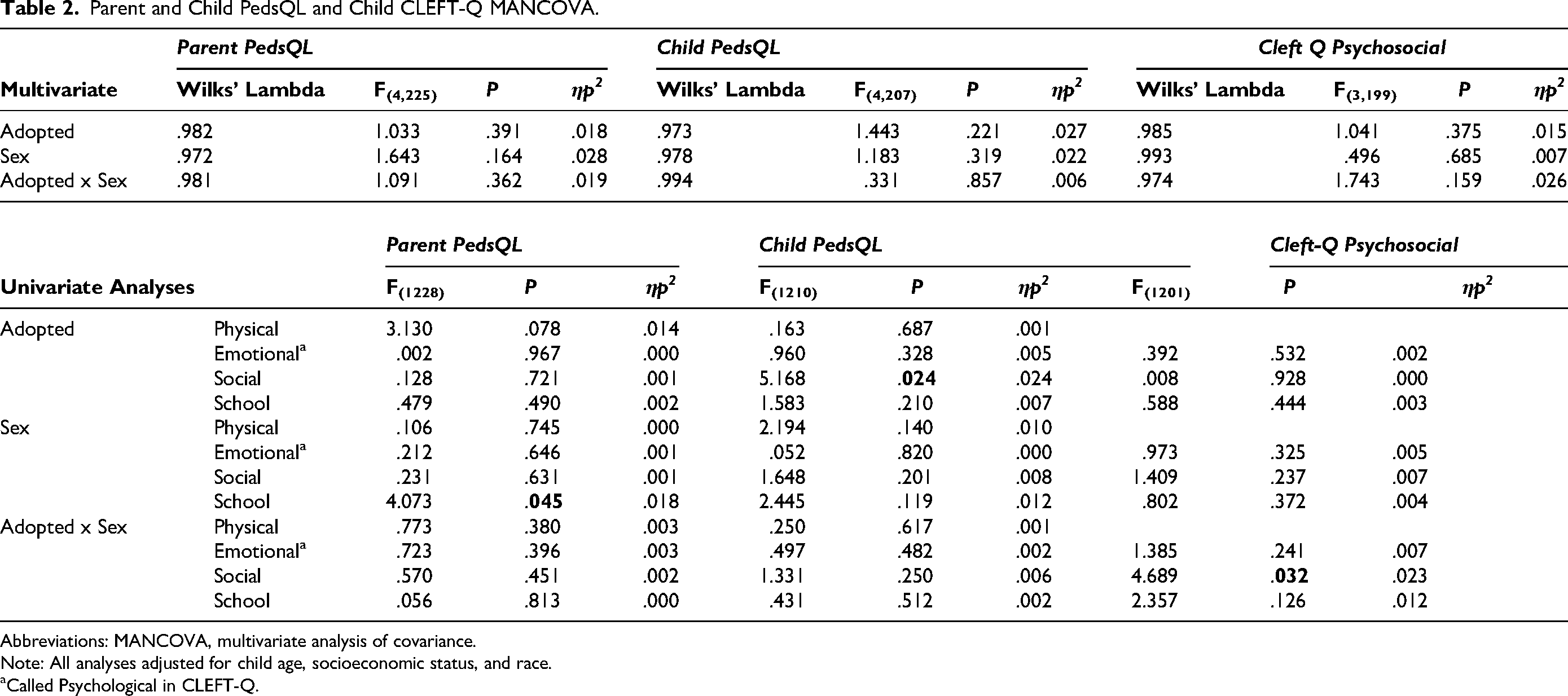
Abbreviations: MANCOVA, multivariate analysis of covariance.
Note: All analyses adjusted for child age, socioeconomic status, and race.
Called Psychological in CLEFT-Q.
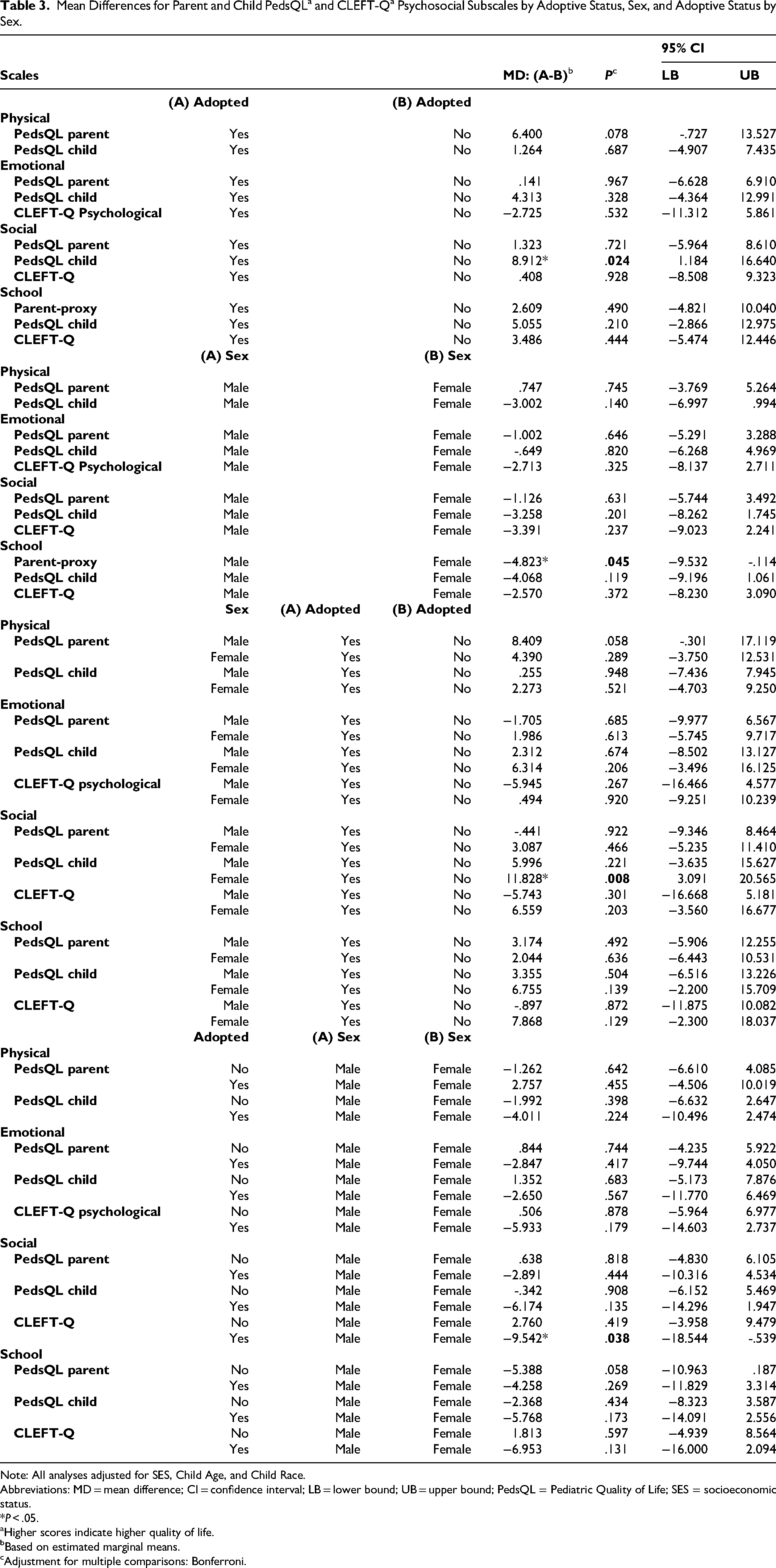
Note: All analyses adjusted for SES, Child Age, and Child Race.
Abbreviations: MD = mean difference; CI = confidence interval; LB = lower bound; UB = upper bound; PedsQL = Pediatric Quality of Life; SES = socioeconomic status.
*P < .05.
Higher scores indicate higher quality of life.
Based on estimated marginal means.
Adjustment for multiple comparisons: Bonferroni.
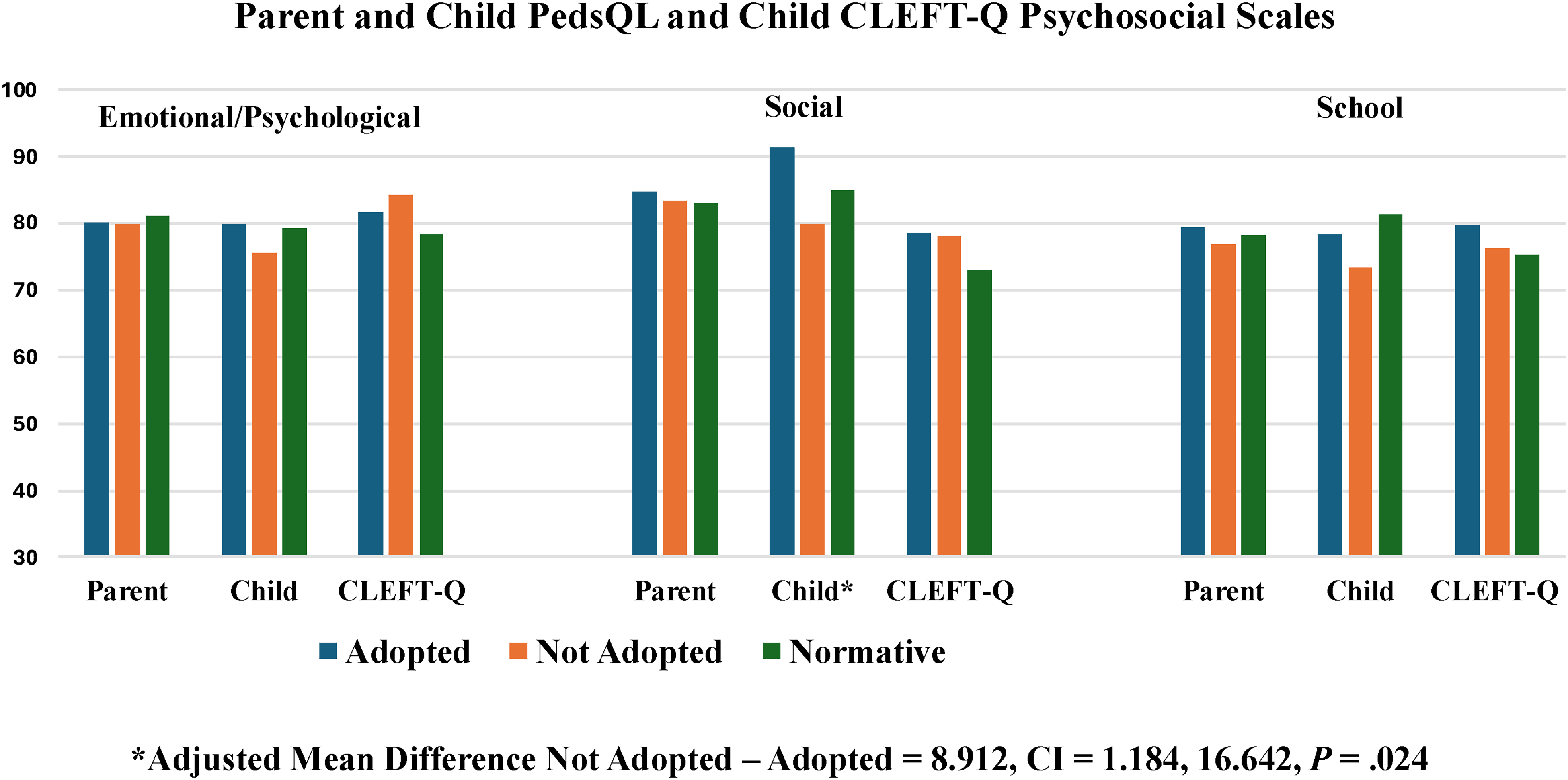
Child PedsQL. After adjusting for SES, race, and child age, there were no significant multivariate effects of adoptive status, sex, or adoptive status by sex on the Child PedsQL scales using Wilks’ lambda (P's > .221). There was a univariate effect of adoptive status on the Child PedsQL Social Scale. (F1,210 = 5.17, P = .024, ηp2 = .02) (Table 2). Children who were adopted reported higher Child PedsQL Social scores than children who were not adopted (MD = 8.91, CI = 1.18, 16.64). Although both male and female children who were adopted reported higher PedsQL Social scores than male and female children who were not adopted, results were larger and significant for females (Adopted-Not adopted Male MD = 6.0. P = .221; Adopted-Not adopted Female MD = 11.83, CI = 3.09, 20.57, P = .008). There was little difference in Child PedsQL Social scores between males and females who were not adopted (MD = -.34, P = 9.08). Males who were adopted reported lower Child PedsQL Social scores than females who were adopted, but those differences were not significant (MD = -6.17, P = .135; Table 3).
CLEFT-Q: Psychosocial Scales. Using Wilks’ lambda there were no significant effects of adoptive status, sex, or the interaction of adoptive status with sex on CLEFT-Q psychosocial outcomes after controlling for SES, race, and age (all Ps > .159). There were significant effects of the interaction of adoptive status and sex on CLEFT-Q Social Function (F(1, 201) = 4.69, P = .032, ηp2 = .023) (Table 2). Specifically, males who were adopted reported significantly lower Cleft-Q Social scores than females (MD = -9.54, CI = -18.54, -.54, P = .038), while males who were not adopted reported non-significantly higher scores than females who were not adopted (MD = 2.76, P = .419) (Table 3).
Figure 3 provides a visual comparison of mean scores for Parent and Child PedsQL and CLEFT-Q Psychosocial scores by adoptive status.
Discussion
The goal of the present study was to compare the impact of adoption from China to an American home on QoL outcomes for children with CLP as well as the impact of adoption on family QoL. There are a number of factors that place children adopted from China at increased risk for poorer outcomes, including institutional placement, older age at adoption, older age at initial surgeries, surgical complications including fistulae or unsatisfactory appearance of the lip increasing the need for repeat surgeries, and increased risk for speech issues.1,68–70 Despite these risks, the few previous studies of children with CLP adopted from international settings, most frequently China, have generally reported QoL outcomes that are equivalent to those of children who were not adopted.41–43 Hence, we hypothesized that there would be few differences in family and child QoL based on adoptive status.
Similar to other cohorts of children described in the literature,1,68–70 the children adopted from China in this study underwent lip and palate surgery at a later age than children who were not adopted, were more likely to have a secondary lip revision and require a secondary palate surgery, and had more total lip, palate, and nasal surgeries than their peers who were not adopted. Perhaps because the children who were adopted had the revision surgeries that were needed, their self-reports on the CLEFT-Q appearance measures were similar to the results of the children who were not adopted and higher than the international norms reported for the CLEFT-Q. Adjusted mean scores did not differ significantly between the 2 groups and the number of children in the lowest 10th percentile of CLEFT-Q appearance scores did not differ significantly between the 2 groups. Children who were adopted were more than twice as likely to be satisfied with the appearance of their teeth, which may be indicative of more careful attention to dental care by families of adopted children due to their higher SES.
Although there may also be a significant impact on a family adopting a child with CLP from China, we hypothesized that this impact would have decreased by the age of the children in this study. We do not know the exact ages at adoption for the children in this study; however, based on existing literature, most children adopted from China are placed in their adoptive families between 18 and 30 months of age or older.1,41–43,68–70 By 8-10 years of age, families have time to adjust to the presence of the adopted child in the family. The first set of surgeries including revision surgeries has typically been completed, and most children are in third to fourth grade. While there are stresses associated with this stage of a child's development, cleft-specific needs are often quiescent. Previous research has shown that the impact on family QoL of having a child with CLP is higher during infancy and preschool ages, 8 but diminishes as children get older. 48 At 8-10 years of age, we assumed that the impact on family QoL would be mitigated for both groups. This hypothesis was supported in that parents of both adopted and non-adopted children reported similar health-related, family functioning, and total QoL. Similar to previous research on children with CL/P, primary caregivers in both groups reported substantially higher family QoL compared to the normative mean of the PedsQL FIM instrument.61–63,71 However, parent health-related QoL and parent-reported family functioning for parents of children who were and were not adopted were similar in magnitude to the scores reported by the parents of 5-year-old children from the Cleft Collective Study. 48 This data adds additional support to idea that the family stress related to CLP decreases for parents as the children get older.
Generic and cleft-specific QoL psychosocial outcomes were equivalent for children who were or were not adopted. The few significant differences in QoL that did occur generally favored children who were adopted with some limitations. Children who were adopted reported better social QoL than children who were not adopted; however, this difference was strongly driven by females who were adopted. Females who were adopted reported higher scores on both the generic and cleft-specific QoL social measures than females who were not adopted as well as higher than males who were adopted, particularly on the cleft-specific social scale of the CLEFT-Q. Even when differences were not significant, females who were adopted tended to report better QoL with regard to emotional and school functioning than females who were not adopted as well as males who were adopted.
The reason females adopted from China reported higher QoL scores than females who were not adopted as well as males who were and were not adopted is not clear. The cumulative evidence from the QoL literature on children with CLP indicates that differences in QoL by sex are not common in children between the ages of 8 and 11, but that when they do exist, they are limited to specific areas of functioning, with reporting poorer QoL than boys.13,17,72–75 Most commonly, lower scores are limited to emotional well-being at this age.18,72,74 In general, children in the 8-11 year age group with or without CLP tend to report higher QoL scores than older children.75–78
Females who are adopted from China may receive more focused emotional support from their families than females who are not adopted as a means of countering the effects of adoption. Using qualitative interviews, Everhart and colleagues 43 observed that both parents of children adopted from China and the children themselves reported that having a cleft was simply a part of the child's lived experience and that having surgeries was viewed as part of that experience. Children perceived their adoptive identity as a source of pride. Families encouraged social participation even while acknowledging that questions related to both the cleft and racial identity could be challenging. Reframing the questions as curiosity rather than criticism or bullying helped children feel positively about their social experiences.
Similar to the families in this study, families adopting children from international settings are generally of higher SES, which is also a potentially protective factor relative to QoL. Higher SES may provide families of children who are adopted internationally with the resources to provide more intensive services including speech therapy and educational support than the families of children who were not adopted. There may be more opportunities for cultural engagement and family-centered activities when stress related to income is less present. There is also some evidence of differences in the way families who have adopted a child from an international setting interact with their child. There may be more focus on the child's needs, as well as a strong effort to foster positive self-perception and pride in the child's accomplishments. Additionally, parents of children who are adopted may be less hesitant to talk about the child's cleft and more be accepting of it as simply a part of the child. 43
The children in this study were between 8 and 11 years of age, which is an age when QoL scores are often higher based on both parent and child self-report.13,17,72–75 It is possible that differences between the 2 groups may emerge as the children move into adolescence. Older teenage females often report dissatisfaction with appearance, greater peer harassment, and stigma experiences, all of which can impact emotional well-being.22,79,80 Adoptive status may also become more salient during adolescence, though there is limited research on this issue for adolescents with CLP. Additionally, there may also be an impact on QoL during adolescence, if children who are adopted continue to require more surgical interventions than children who are not adopted. 81
Future Directions
Further research into the ways adoption is protective of children's perceptions of their own QoL is indicated. Additional qualitative studies may provide insight into the ways parents of children adopted internationally support the emotional and social development of their children. There is also limited information on behavioral outcomes of children with CLP who are adopted from China. Studies investigating internalizing and externalizing behaviors, frequency of attention-related problems, and social functioning at home and at school will help elucidate factors that may be associated with QoL. As this study focused on middle school children, further research is needed to investigate QoL during adolescence for children who are adopted. Finally, while this study focused specifically on international adoptions, there is little information about the QoL or behavior adjustment of children with CLP who are adopted domestically. The broader literature on adoption suggests that children without CLP adopted domestically may be at higher risk of poor outcomes than the children adopted from international countries. 34 Determining if this is also true for children with CLP should be the focus of future research.
Strengths and Limitations
One strength of this study is the large sample size that is representative of 6 cleft treatment teams in North America. Additionally, we used both generic and cleft-specific QoL measures based on both parent and self-report allowing for a rich data set covering social, emotional, school, and physical aspects of QoL. Nonetheless, a major limitation of this study is that subjects were not recruited to study QoL issues related to adoptive status. Rather, subjects were recruited based on a diagnosis of isolated CL/P and age. Consequently, critical data related to adoption was not collected including age at adoption, environment prior to adoption, and motivation for adoption. An additional limitation is that the current study is focused on children with CLP who were adopted from China due to the small number of children adopted from other settings and the limited number of children with CL ± A and CP who were adopted. It will be necessary to include a larger number of clinics to increase the number of children who are adopted with these conditions. Nevertheless, the data does provide a broad examination of QoL outcomes for children with CLP who are adopted and treated across North America.
Conclusions
Children with CLP who are adopted and their parents report QoL outcomes that are similar or in some cases better than their non-adopted peers with CLP. The impact of CLP on parental health-related QoL and family functioning is similar for families in which children were adopted and not adopted when the children are between 8 and 11 years of age. Being adopted conferred some protection for social functioning, particularly for females who were adopted.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656261462270 - Supplemental material for Quality of Life for Children with Cleft Lip and Palate and Their Families: The Effect of Adoption from China
Supplemental material, sj-docx-1-cpc-10.1177_10556656261462270 for Quality of Life for Children with Cleft Lip and Palate and Their Families: The Effect of Adoption from China by Kathleen A. Kapp-Simon, Meredith Albert, Canice E. Crerand, Claudia Crilly Bellucci, Celia E. Heppner, Suzanne Woodard and Amy L. Conrad in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-docx-2-cpc-10.1177_10556656261462270 - Supplemental material for Quality of Life for Children with Cleft Lip and Palate and Their Families: The Effect of Adoption from China
Supplemental material, sj-docx-2-cpc-10.1177_10556656261462270 for Quality of Life for Children with Cleft Lip and Palate and Their Families: The Effect of Adoption from China by Kathleen A. Kapp-Simon, Meredith Albert, Canice E. Crerand, Claudia Crilly Bellucci, Celia E. Heppner, Suzanne Woodard and Amy L. Conrad in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-docx-3-cpc-10.1177_10556656261462270 - Supplemental material for Quality of Life for Children with Cleft Lip and Palate and Their Families: The Effect of Adoption from China
Supplemental material, sj-docx-3-cpc-10.1177_10556656261462270 for Quality of Life for Children with Cleft Lip and Palate and Their Families: The Effect of Adoption from China by Kathleen A. Kapp-Simon, Meredith Albert, Canice E. Crerand, Claudia Crilly Bellucci, Celia E. Heppner, Suzanne Woodard and Amy L. Conrad in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-docx-4-cpc-10.1177_10556656261462270 - Supplemental material for Quality of Life for Children with Cleft Lip and Palate and Their Families: The Effect of Adoption from China
Supplemental material, sj-docx-4-cpc-10.1177_10556656261462270 for Quality of Life for Children with Cleft Lip and Palate and Their Families: The Effect of Adoption from China by Kathleen A. Kapp-Simon, Meredith Albert, Canice E. Crerand, Claudia Crilly Bellucci, Celia E. Heppner, Suzanne Woodard and Amy L. Conrad in The Cleft Palate Craniofacial Journal
Footnotes
Acknowledgements
Funding for this project was provided by a grant from the Cleft Palate Foundation (Kapp-Simon, PI). We thank Farah Sheikh, M.S.W., R.S.W; Jennifer Litteral, M.A.; Hillary M. Kapa, M.P.H.; Hailey Umbaugh, B.S.; Emily Kuhlmann, Ph.D.; Kristina Butler, Ph.D.; Alessia Portante, B.S.; Ashlyn Parides, Ph.D.; Dennis Burchette, Ph.D. who helped with data collection and/or data compilation/cleaning. We extend our appreciation to the children and families who took part in this study.
Author Contributions
All authors participated in the original conception of the broader study. KAKS, MA, and CCB were involved in the design of the current study. KAKS conducted statistical analysis and drafting of paper. ALC participated in the analysis. All authors reviewed the final manuscript and provided critical comments.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Cleft Palate Foundation, American Cleft Palate-Craniofacial Association.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Human Subjects Protection
This study was conducted in compliance with all Human Subjects Protection requirements of the 6 participating treatment centers. Primary Site Certificate of Approval from Western Institutions Review Boards, Shriners Hospitals for Children, Protocol Number: 20160678.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.