
Abstract
Objective
To compare speech outcomes following primary cleft palate repair using modified Sommerlad palatoplasty (MSP) versus Sommerlad–Furlow modified palatoplasty (SFP).
Design
Retrospective cohort study.
Setting
A high-volume tertiary cleft center.
Patients
Patients who underwent primary cleft palate repair before 5 years of age between 2011 and 2021 were retrospectively reviewed.
Participants
Patients treated with MSP or SFP and with complete follow-up records were included. Participants were stratified by age at surgery as younger than 1.5 years or 1.5 years and older.
Interventions
Primary cleft palate repair with MSP or SFP.
Main Outcome Measure(s)
Postoperative speech outcomes, particularly velopharyngeal competence (VPC), and factors associated with speech performance.
Results
A total of 1265 patients were included, of whom 874 underwent surgery before 1.5 years of age and 391 at 1.5 years or older. In the younger group, surgical technique and cleft type were significantly associated with speech outcomes. After adjustment for baseline differences, SFP achieved a significantly higher VPC rate than MSP in patients with Veau III cleft palate (84.4% vs 73.0%, P = .027). In the older group, sex, cleft type, and surgical technique were not significantly associated with speech outcomes.
Conclusions
In this cohort, speech outcomes after primary palatoplasty were influenced by surgical technique and cleft type. For patients with Veau III cleft palate who underwent repair before 1.5 years of age, SFP was associated with superior speech outcomes compared with MSP.
Keywords
Introduction
Cleft palate is one of the most common congenital anomalies in the craniofacial region, affecting critical physiological functions including speech, feeding, breathing, and craniofacial growth. 1 Patients with cleft palate develop abnormal speech due to the lack of proficient velopharyngeal closure function. 2 Primary palatoplasty aims to obtain the velopharyngeal closure function and provide a normal physiological basis for subsequent speech development.2-4
Although recent literature has reported significant improvement in the speech outcome of primary palatoplasty, velopharyngeal insufficiency (VPI) still occurs in 5% to 40% of patients.5-7 Numerous techniques are being applied for primary cleft palate repair, but the optimal technique remains controversial.4,8,9 The comparison of different palatoplasty techniques reveals valuable insights into the critical surgical maneuvers that matter to the outcome and the direction for further modification.
Reviewing the development of palatoplasty techniques helped us understand the key to the impact of different surgical methods on prognosis. In the 19th century, von Langenbeck first described his bi-pedicle technique, 10 which is still in use today.11,12 However, the original von Langenbeck palatoplasty does not reconstruct the levator veli palatini muscle, and a lateral relaxation incision was used in all patients.13,14 These are potentially harmful to the patient’s speech development and maxillary growth.15,16 In 1986, Furlow described the double-opposing Z-plasty method for the repair of cleft palate. 17 This technique effectively extends the length of the soft palate and reconstructs the levator veli palatini.17-19 In 2003, Sommerlad described his technique, involving intrinsic dissection and radical transposition of velar muscles under the microscope, and reported a satisfactory outcome. 20 From von Langenbeck palatoplasty, to double-opposing Z-plasty, and then to Sommerlad palatoplasty, the evolution history of palatoplasty clearly shows the transition from simple cleft closure to the pursuit of levator veli palatini function reconstruction, which provides an important surgical idea for reducing the incidence of VPI and optimizing speech effects. In 2015, Shi proposed the Sommerlad-Furlow modification technique, which theoretically combined the advantages of radical muscle reconstruction and velum lengthening achieved by double-opposing Z-plasty. In previous studies conducted at our center, we observed comparable velopharyngeal function between patients undergoing Furlow palatoplasty and the Sommerlad-Furlow modification technique. Both procedures yielded high rates of adequate velopharyngeal function, at 84% and 82.1%, respectively, with no significant differences in speech outcomes. 7 However, the speech outcomes of Sommerlad's palatoplasty and Sommerlad-Furlow modification technique have not yet been directly compared. A comparison of outcomes and prognostic factors between these 2 techniques could provide valuable insights, such as whether velum lengthening remains necessary when the levator veli palatini muscle sling is fully restored. In our center, modified Sommerlad's palatoplasty (MSP) and Sommerlad-Furlow modified palatoplasty (SFP) have been performed with large case numbers, lending us an opportunity to scrutinize their potential advantages and disadvantages over each other. Therefore, our study reviewed the 2 surgical techniques and further analyzed the factors affecting the effect of speech outcome. Does the SFP that combines the advantages of muscle reconstruction and velum lengthening obtain better speech outcome than the MSP that only performs muscle reconstruction? What are the factors affecting the prognosis of the SFP? Our data may provide a reference for further evolution of primary cleft palate repair technique.
Patients and Methods
Subject Enrollment
This study is a retrospective study that has been approved by the Ethics Committee (WCHSIRB-D-2019-055). All patients’ custodians signed informed consent before surgery. The inclusion criteria were as follows: (1) with nonsyndromic cleft palate with or without cleft lip, (2) less than 5 years at the time of palatoplasty, (3) follow-up time: younger patients were followed until the age of 5, while older patients (operated between 1.5 and 5 years) were followed for at least 1 year postoperatively, and (4) with complete speech evaluation records. Patients with submucous cleft palate, hypotonia, central neural disorders, hearing impairment, or other nasopharyngeal surgeries, including tonsillectomy and adenoidectomy, were excluded.
At present, many studies have shown that patients performed cleft palate repair before 18 months of age can obtain better velopharyngeal function.21-23 Therefore, enrolled patients were divided into the young group (≤1.5 years) and the aged group (1.5-5years). Data collection covered age at operation, gender, surgical technique, cleft type (Veau I, II, III, IV), 24 velopharyngeal function, speech intelligibility, articulation disorders, hypernasality, and nasal air emission.
Surgery Techniques
All procedures were performed by 2 senior authors (Q.Z. and J.L.), each with over 10 years of experience in cleft palate repair. Since 2011, we have implemented a modified technique combining elements of Sommerlad and Furlow palatoplasty, termed Sommerlad-Furlow modified palatoplasty (SFP). Patients were retrospectively assigned to either the MSP or SFP group based on detailed operative records. Both surgeons followed standardized protocols for each technique, developed through regular team discussions. Cases with significant deviations from these protocols were excluded from the study.
The MSP was performed according to the description of Sommerlad B.C. 20 with the aid of 3X loupes instead of a microscope. The oral mucosa was incised along the cleft palate edge, and the oral mucosal flap was pulled to expose the muscle layer and nasal mucosa. The oral mucosa of the velum was raised, the velum muscle was dissected from the nasal mucosa and transposed to a horizontal position. Both oral and nasal layers were closed in straight-line. In order to better identify the soft palate muscle, the nasal layer was sutured in straight-line. Then the soft palate muscle on both sides was separated from the nasal musculomucosal layer, and the muscle was sutured to reconstruct the levator sling. Finally, the oral layer was closed. The length of the relaxation incision on both sides was determined according to the degree of suture tension (Figure 1).
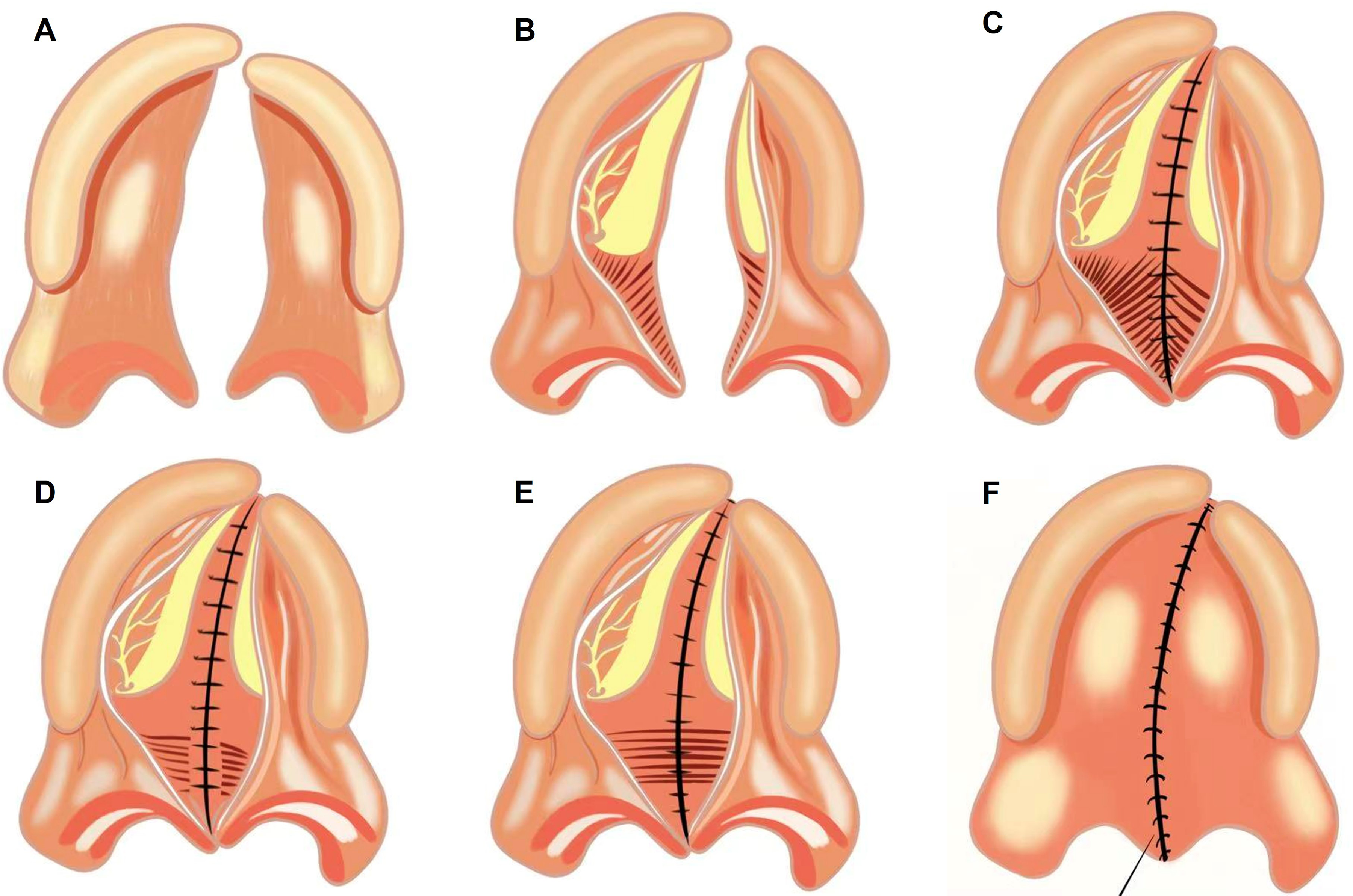
The surgical procedures of MSP.
The SFP was performed as previously described 25 : Firstly, incisions were made along the edge of the cleft following the Sommerlad technique. The oral mucosa was raised with the musculature attached to the nasal mucosa. The soft palate muscle and medial pterygoid plate were completely exposed. The nasal layer was detached from the hard palate, and dissection extended into the Ernst space. Then, a nasopharyngeal incision was made on the medial pterygoid plate, and the mucoperiosteum was stripped from the plate. The nasal mucosa was sutured from the junction of the soft and hard palate to the front end of the hard palate. After completing this step, the complete cleft palate on the nasal side became an incomplete cleft palate. Next, the soft palate muscle was separated from the nasal musculomucosal layer on the left side as described by Sommerlad, while the muscle on the right side was left on the nasal mucosa. Then, according to Furlow's technique, nasal-side mucosal Z-plasty flaps were designed, crossed, and sutured. The dissected palatal muscular flap was sutured to the surface of the right myomucosal flap. Finally, the oral layer was closed in straight-line (Figure 2).
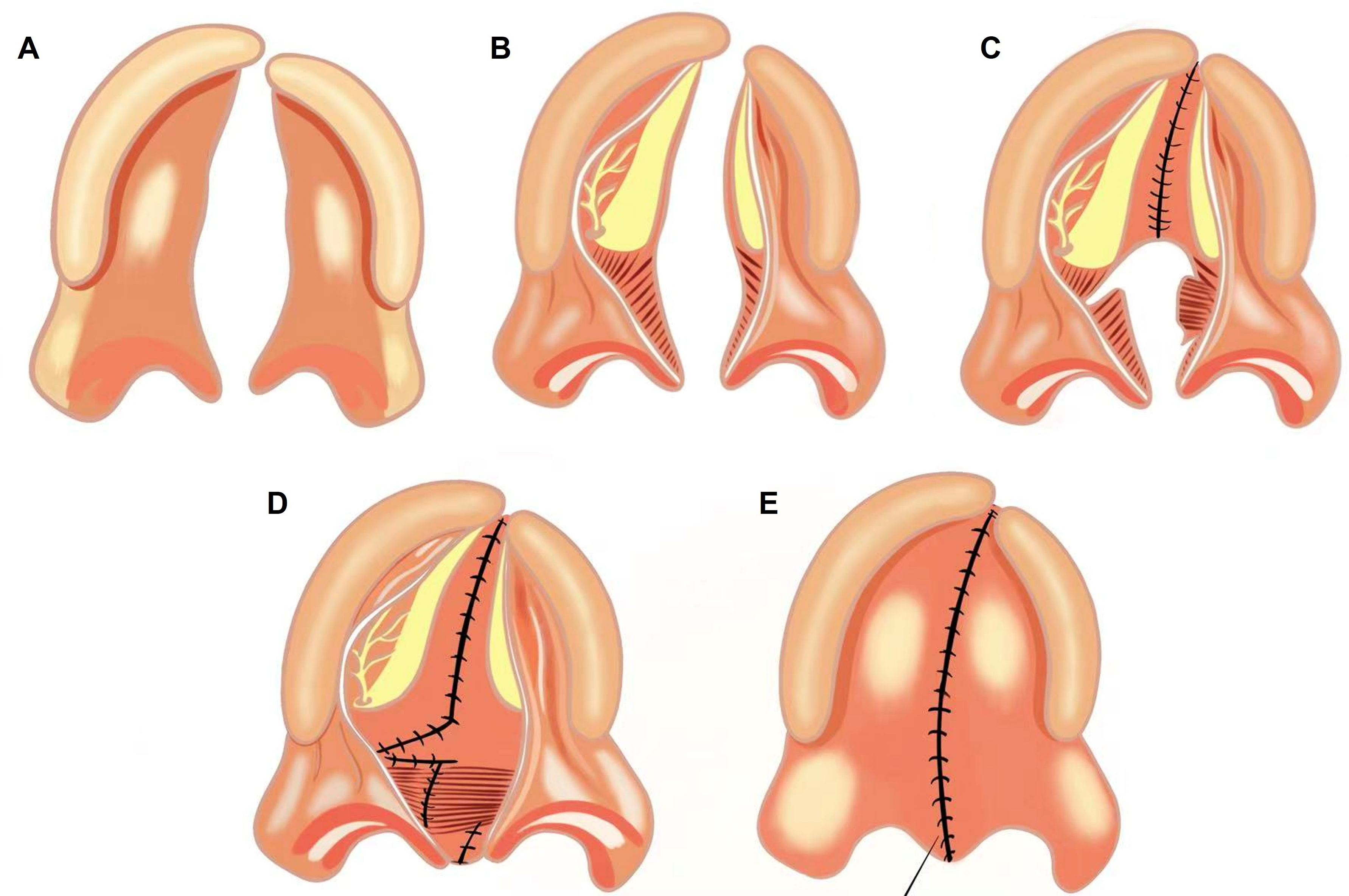
The surgical procedures of SFP.
Speech Evaluation
The examination of velopharyngeal function included perceptual speech assessment and nasopharyngoscopy (Olympus OTV-S1; Olympus Medical, Tokyo, Japan) examination. When the patient was at least 5 years old and at least 1 year after surgery, standardized perceptual speech evaluation and nasopharyngoscopy examination were independently performed by 2 experienced speech therapists, each with over 10 years of specialization in cleft care.
Evaluations followed Henningsson's standardized criteria, 26 focusing on nasal resonance, nasal emission, consonant articulation, and speech intelligibility, 27 and the procedure has been described in detail in our previous study. 28 Hypernasality severity and nasal emission were rated 0 (normal) through 1 (mild) and 2 (moderate) to 3 (severe). Consonant articulation was categorized as either normal or abnormal (including omission and compensatory errors). Speech intelligibility was categorized as either clear or unclear. In this study, we simplified the scores of hypernasality and nasal emission: scores of 0 indicated normal, while scores ≥1 indicated abnormal.
Patients who exhibited signs of hypernasality or nasal air emission during the perceptual assessment subsequently underwent nasoendoscopy for further evaluation. Altogether, nasoendoscopy was performed in approximately 27.7% of the total patient cohort. The nasopharyngoscopy examination procedure was as described in the previous study. 29 The morphology of the palatopharynx during resting and continuous vocalization was recorded. The velopharyngeal closure ratio was calculated as [1 − (residual gap size/resting gap size)] × 100%.
The primary outcome of this study was postoperative velopharyngeal function, categorized as either velopharyngeal competence (VPC) or VPI. Patients with hypernasality or nasal air emission in perceptual speech assessment and with a velopharyngeal closure ratio less than 100% by nasopharyngoscopy examination were diagnosed with VPI.
Statistical Analyses
Statistical analyses were performed with IBM SPSS Statistics 26. T-test was used to compare continuous variables such as age. Pearson's Chi-square analysis was used to compare the proportions of categorical variables, including gender, cleft type, hypernasality, nasal air emission, speech intelligibility, articulation, and velopharyngeal function. The above 2 univariate analyses were used to analyze the correlation between velopharyngeal closure function and potential prognostic factors (Tables 1 to 3). For factors with statistical differences in univariate analysis, binary logistic regression analysis was used to determine the impact of parameters on velopharyngeal function after surgery (Table 3). Due to the different factors affecting the postoperative velopharyngeal function in the 2 groups, we followed up in different ways for further analysis. In the young group, Pearson's Chi-square analysis was used to analyze the differences in postoperative VPC rates among patients with different surgical techniques and different cleft types (Table 4). In the aged group, the receiver operating characteristic (ROC) curve analysis and Youden index were utilized to determine the best cut-off value for the significant prognostic factor (Figure 1). A P-value <.05 was considered significant.
Clinical Characteristics of all Patients Included in the Study.
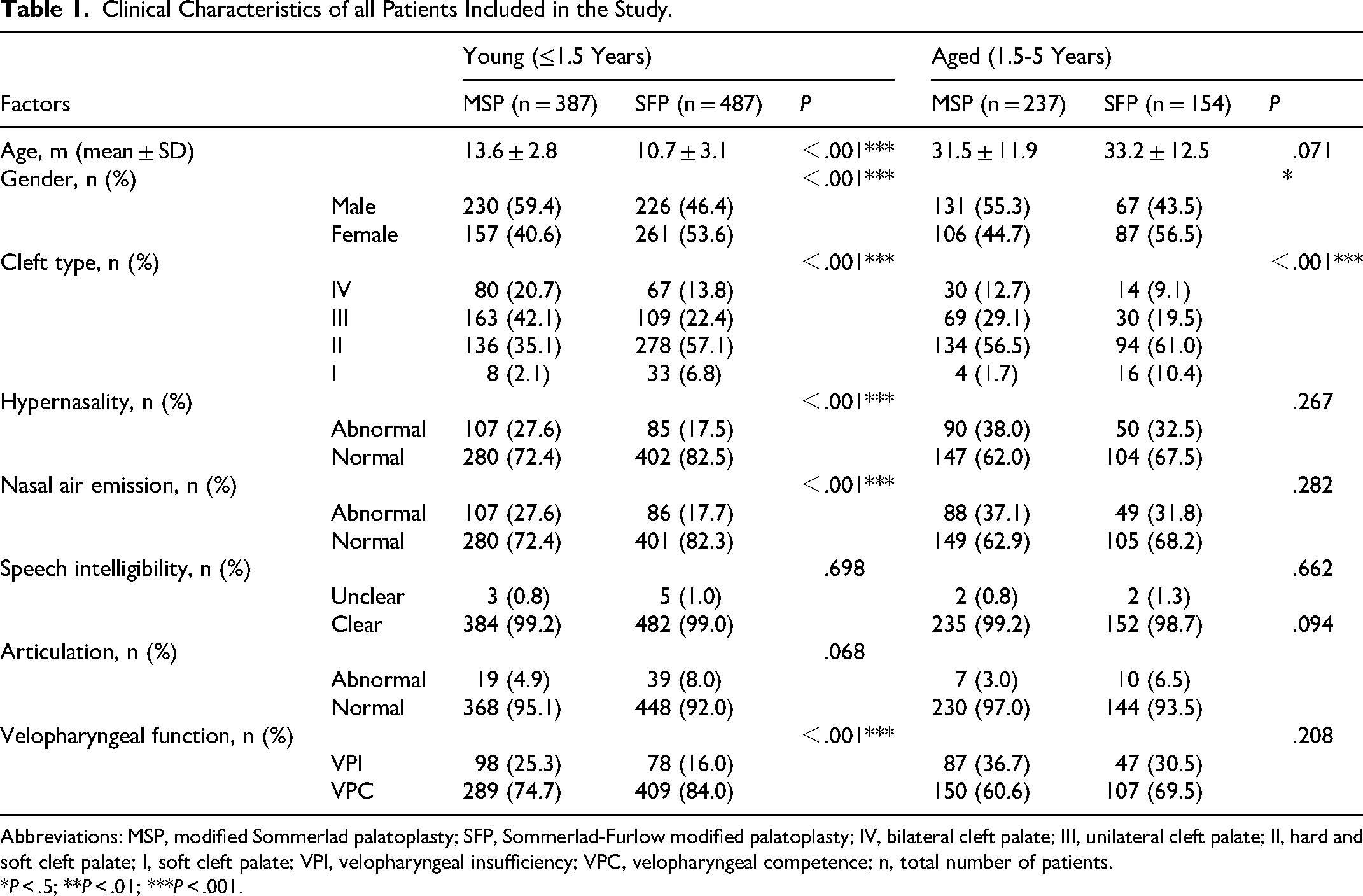
Abbreviations: MSP, modified Sommerlad palatoplasty; SFP, Sommerlad-Furlow modified palatoplasty; IV, bilateral cleft palate; III, unilateral cleft palate; II, hard and soft cleft palate; I, soft cleft palate; VPI, velopharyngeal insufficiency; VPC, velopharyngeal competence; n, total number of patients.
*P < .5; **P < .01; ***P < .001.
Analysis of Potential Risk Factors for Postoperative VPI in Patients Under 1.5 Years Old.
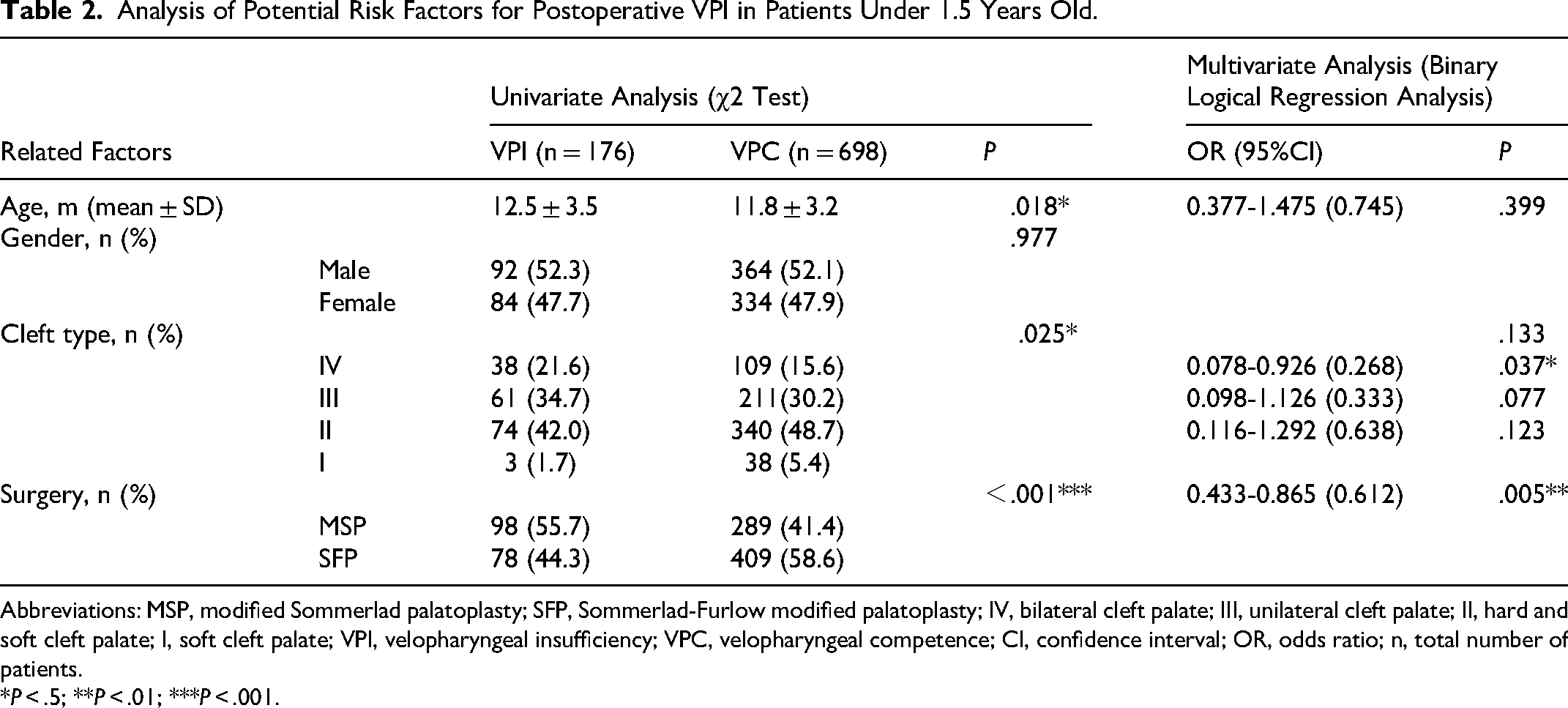
Abbreviations: MSP, modified Sommerlad palatoplasty; SFP, Sommerlad-Furlow modified palatoplasty; IV, bilateral cleft palate; III, unilateral cleft palate; II, hard and soft cleft palate; I, soft cleft palate; VPI, velopharyngeal insufficiency; VPC, velopharyngeal competence; CI, confidence interval; OR, odds ratio; n, total number of patients.
*P < .5; **P < .01; ***P < .001.
Analysis of Potential Risk Factors for Postoperative VPI in Patients Aged 1.5 to 5 Years.
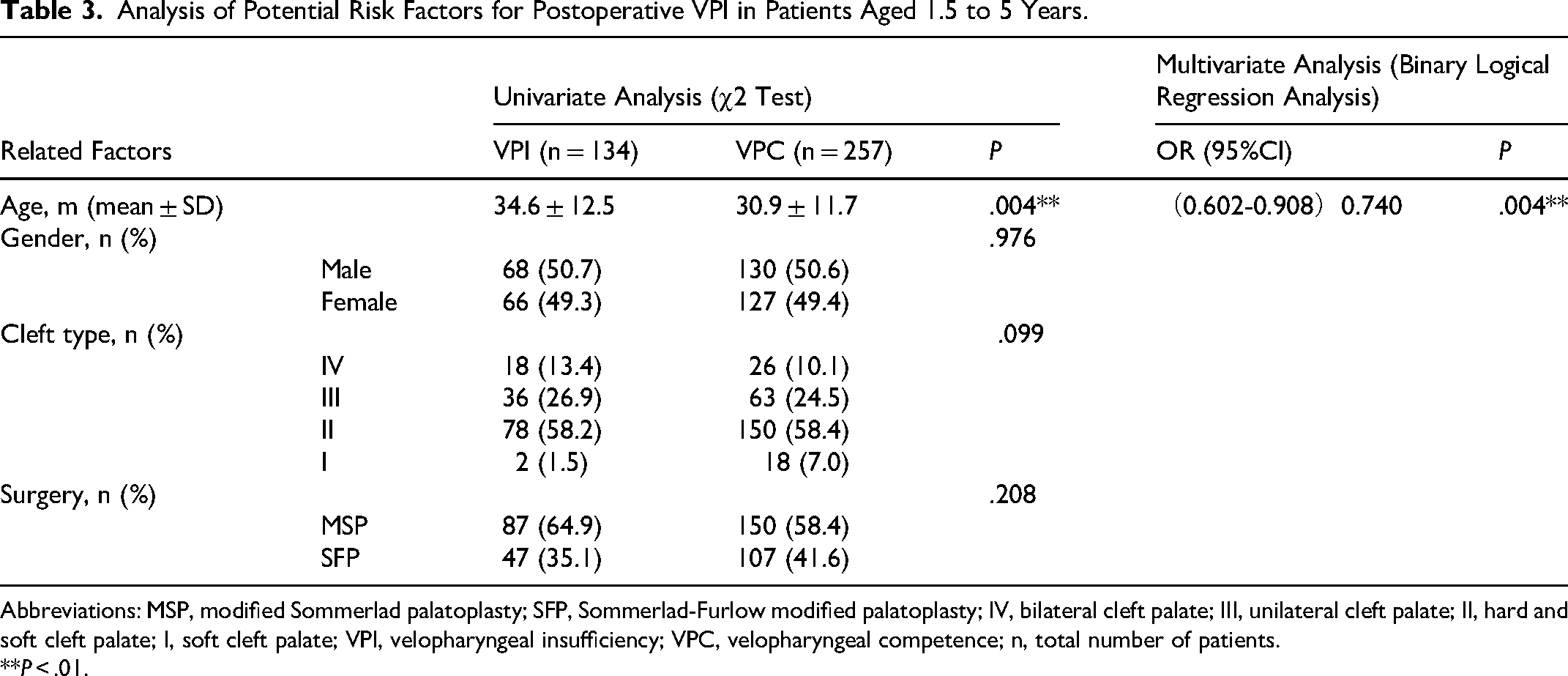
Abbreviations: MSP, modified Sommerlad palatoplasty; SFP, Sommerlad-Furlow modified palatoplasty; IV, bilateral cleft palate; III, unilateral cleft palate; II, hard and soft cleft palate; I, soft cleft palate; VPI, velopharyngeal insufficiency; VPC, velopharyngeal competence; n, total number of patients.
**P < .01.
The Incidence of Postoperative VPC in Patients Under 1.5 Years Old With Different Surgical Techniques and Different Cleft Types.
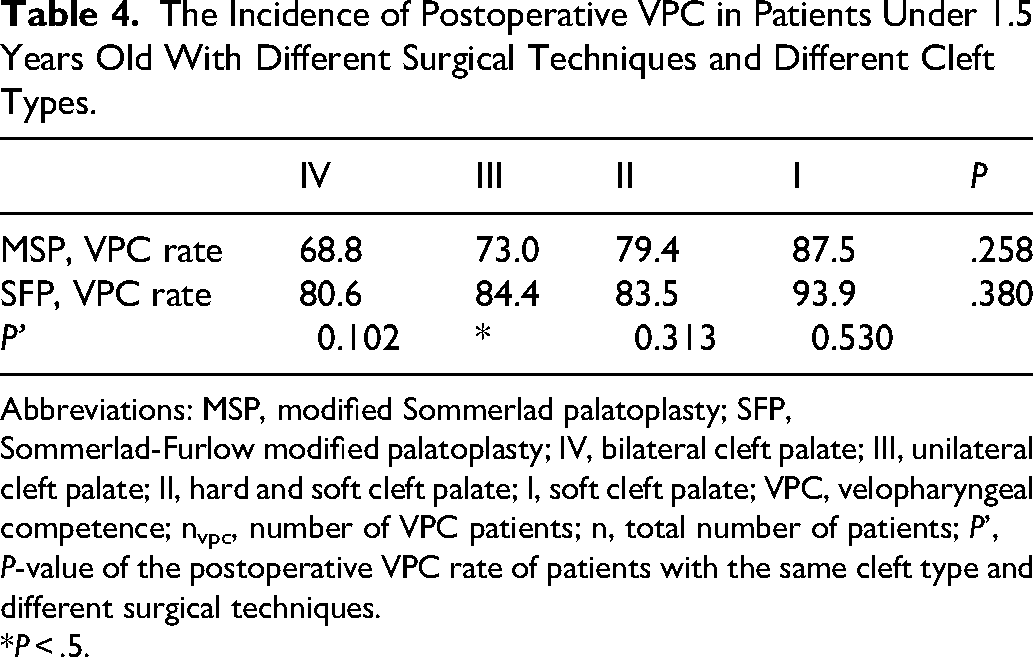
Abbreviations: MSP, modified Sommerlad palatoplasty; SFP, Sommerlad-Furlow modified palatoplasty; IV, bilateral cleft palate; III, unilateral cleft palate; II, hard and soft cleft palate; I, soft cleft palate; VPC, velopharyngeal competence; nvpc, number of VPC patients; n, total number of patients; P’, P-value of the postoperative VPC rate of patients with the same cleft type and different surgical techniques.
*P < .5.
Results
This study initially recruited 1878 patients who had palatal repair with either technique from 2011 to 2021, but 613 (32.64%) patients were eliminated according to the subject enrollment criteria. About 874 were operated on below the age of 1.5 years, and 319 between 1.5 and 5 years. Detailed characteristics of the enrolled cohort were illustrated in Table 1.
In the young group, SFP yielded a significantly lower rate of VPI, hypernasality, and nasal air emission as compared with MSP (Table 1). Considering the significant difference in age, gender, and cleft type distribution between MSP and SFP cases, univariant analyses and multivariant logistic regression analyses were performed to confirm the impact of surgical technique on speech. Surgical technique (P = .005) was significantly associated with velopharyngeal function (Table 2). The incidence of postoperative VPI in patients undergoing MSP was higher than that in patients undergoing SFP (Table 2). In addition, patients with Veau IV cleft demonstrated higher risk of VPI (P = .037, 95%CI = 0.268, Table 2). In order to analyze the differences in postoperative VPC rates among patients with different surgical techniques and different cleft types, further subgroup analyses revealed that SFP yielded a superior VPC rate over MSP only among patients with Veau III cleft (SP 73.0%, SFP 84.4%, P = .027, Table 4).
In the aged group, age was significantly associated with velopharyngeal function (Table 3). ROC curve analysis indicated age at surgery of 2.86 years as a suitable cut-off value for further subgroup comparison (Figure 3). Subsequently, patients were divided into subgroups A (palatalplasty operated before 2.86 years) and B (palatalplasty operated after 2.86 years) (Figure 4).
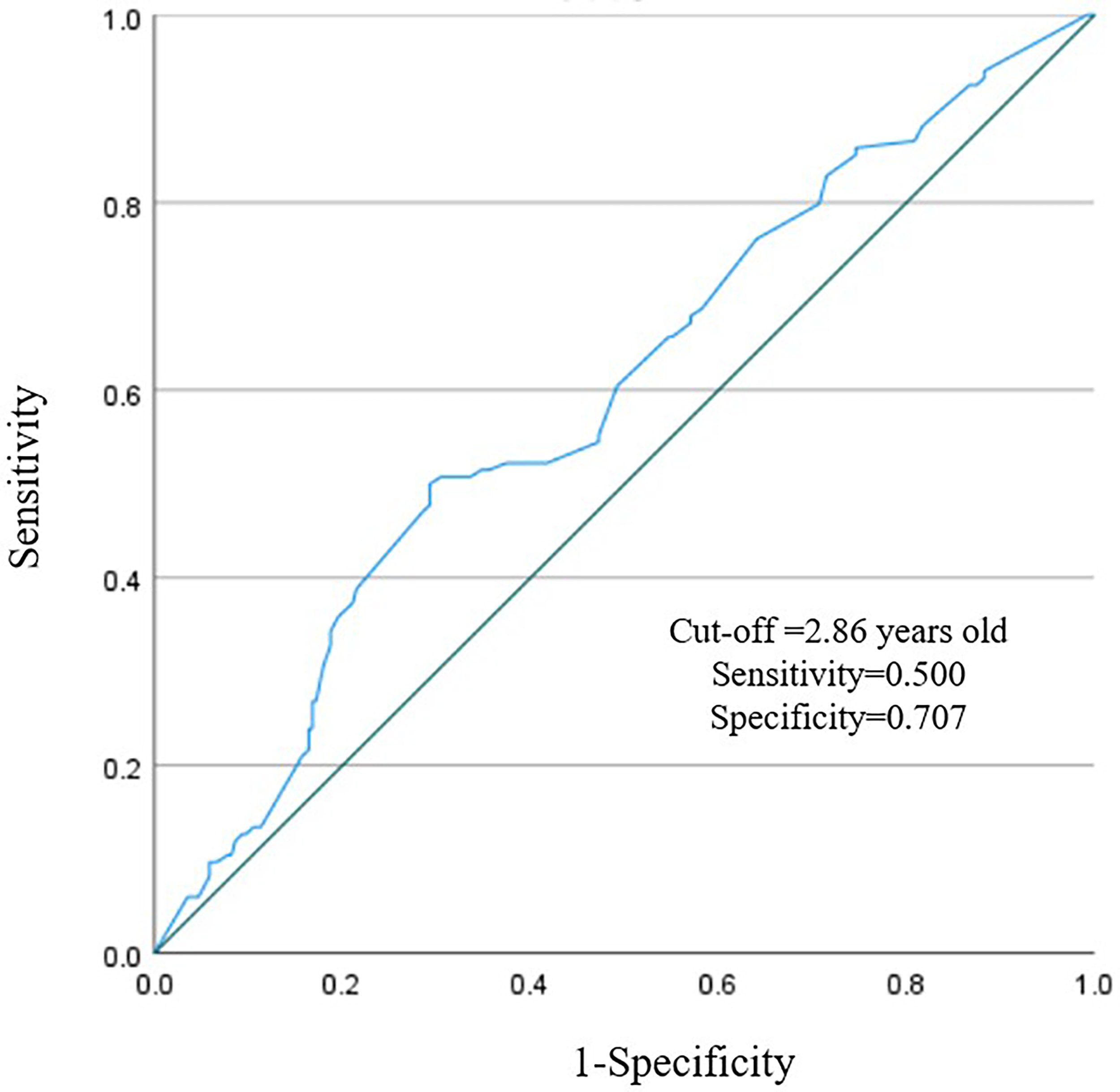
ROC curve was used to calculate the optimal cut-off value of age.
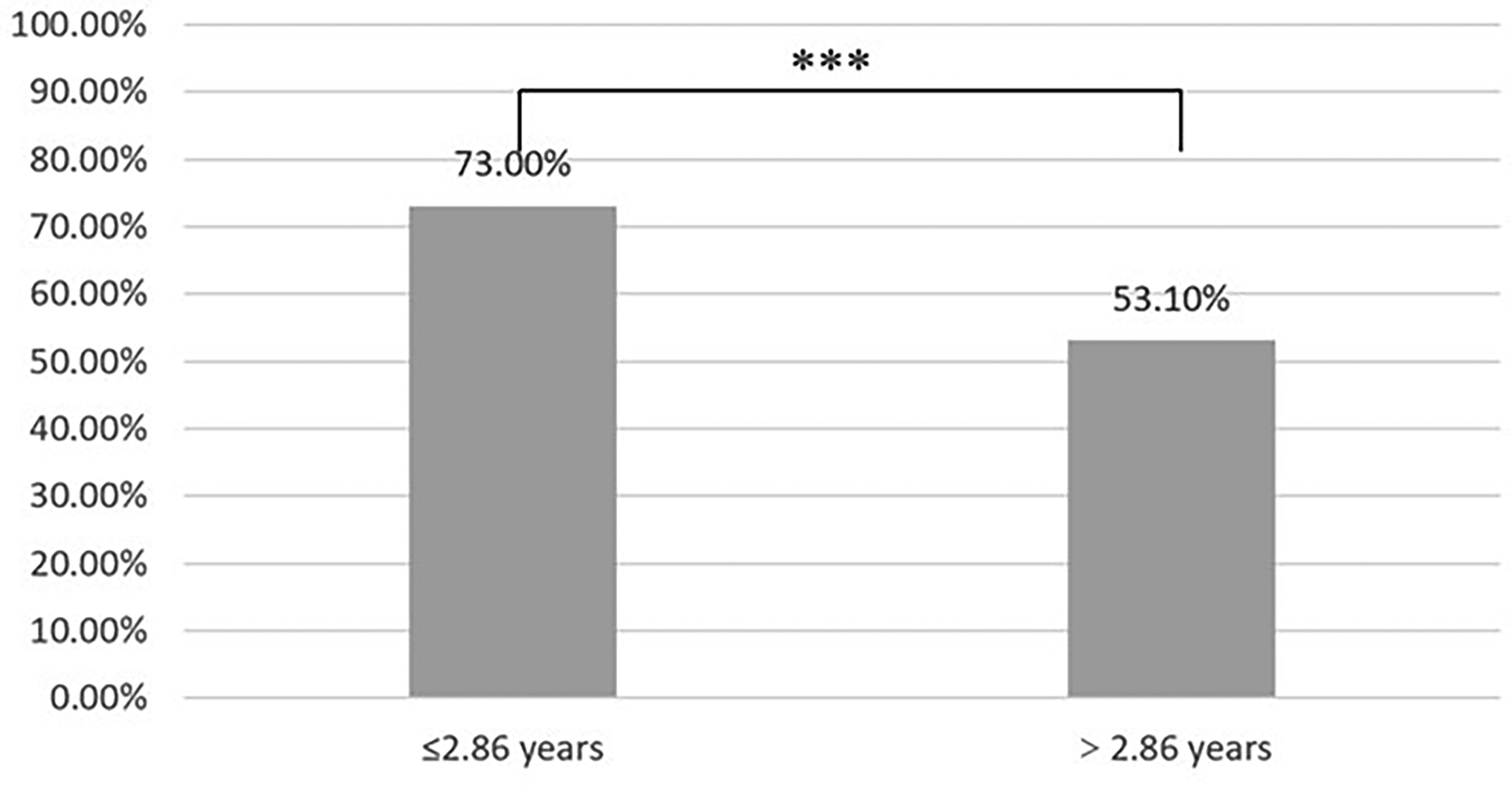
Comparison of the rate of VPC among patients between 1.5 and 5 years.
Discussion
Primary repair plays a vital role in the sequential treatment of cleft lip and palate. Primary palatoplasty affects the following development of speech, hearing, feeding, craniofacial growth, and mental health.21,30 An ideal primary treatment is supposed to balance all the above factors.
Since von Langenbeck proposed the bi-pedicle technique in the 19th century, numerous surgical techniques have been used for the treatment of cleft palate, such as double-opposing Z-plasty and Sommerlad palatoplasty. With the advancement of surgical techniques, more and more surgeons have paid attention to the importance of reconstructing the levator veli palatini muscle and increasing the length of the soft palate for better velopharyngeal closure after surgery.20,31-33 Kriens first proposed that the abnormal localization of the levator veli palatini and the loss of the integrity of the supporting structure are the main reasons for the impairment of speech function after palate repair. 31 Numerous studies showed that reconstruction of the levator veli palatini muscle affects velopharyngeal function, and incomplete muscle mobilization is associated with poor speech outcomes.20,32,33 When performing palatoplasty, the importance of palatal length is often emphasized. 34 Randall et al. showed that patients with longer palates demonstrated better speech outcomes. 34
The SFP was designed to combine the benefits of radical muscle reconstruction and velum lengthening. Z-plasty lengthening introduces extra closure tension and risk of fistulae formation. We extended our dissection into the Ernst space to achieve tension-free closure of the nasal layer Z-plasty. The oral layer was closed in straight-line to reduce the risk of relaxing incision and impact on maxillary growth. Our center has compared velopharyngeal function between patients who underwent Furlow palatoplasty and the Sommerlad-Furlow modified technique. The 2 techniques obtained adequate velopharyngeal function, without significant difference in speech outcomes. 7 This study found that for patients younger than 1.5 years old, SFP achieved better speech outcomes than MSP in patients with Veau type III cleft palate.
The timing of surgery profoundly impacts speech outcomes and has been a subject of significant controversy. Multiple studies showed that patients who undergo surgery after 1.5 years consistently show less favorable results, regardless of surgical technique or cleft severity.21-23 Recent findings from the Timing of Primary Surgery (TOPS) trial reported a lower rate of VPI at 5 years in infants undergoing repair at 6 months compared with 12 months 35 ; however, subsequent analyses have noted that this result was influenced by specific dichotomization of ordinal speech outcomes and may vary under alternative analytic approaches. 36 In addition, the higher rate of secondary speech surgery in the earlier group and the observed increase in maxillary arch constriction underscore the need for balanced interpretation. 37 Therefore, although emerging evidence suggests potential benefits of earlier repair within the first year of life, the optimal timing of palatoplasty remains under discussion. As our study aimed to compare surgical techniques rather than determine timing, we adopted 1.5 years as a clinically meaningful threshold to distinguish early from delayed repair. Delayed surgeries were associated with increased hypernasality and nasal air emission, irrespective of the surgical method, and although speech intelligibility remained high across aged groups, late timing likely diminished velopharyngeal function. These findings emphasize that early primary palatoplasty (≤1.5 years) is critical, particularly for complex cleft types, as delaying surgery significantly compromises the likelihood of achieving optimal VPC.
In addition, in our study, we found that the velopharyngeal function of young patients was more sensitive to the surgery technique and cleft type as compared with aged patients. The more severe the cleft palate, the higher the probability of postoperative VPI, suggesting that the reconstruction of the levator veli palatini and the lengthening of the soft palate were affected by the preoperative soft palate conditions. A significant difference between the MSP and SFP was only observed among those with Veau III cleft. We speculated that the extra benefit of velum lengthening in SFP over MSP was unnecessary for Veau I and II clefts, while it was insufficient to improve speech outcome for more severe Veau IV clefts. More severe a cleft usually demonstrates shorter velum, wider cleft, and deeper pharynx, which limits the extent of velum lengthening during Z-plasty. 32
This study has several limitations. First, it spans over a decade of data collection, during which changes in surgical techniques and epidemiological characteristics may have impacted the comparability of different surgical groups. From 2011 to 2013, MSP was the primary technique used for cleft repair. However, between 2014 and 2021, SFP became more commonly performed. Additionally, with advancements in prenatal ultrasound technology, the proportion of patients presenting with severe cleft lip and palate decreased over time. 38 To address this, we applied binary logistic regression analysis to minimize the influence of confounding factors. Second, our analysis focused exclusively on velopharyngeal function, neglecting other critical aspects, such as the impact of palatoplasty on maxillofacial growth and development, which are equally important for a comprehensive evaluation. Furthermore, as a retrospective study, it was limited by a high rate of postoperative loss to follow-up. Future research should include more rigorously controlled prospective studies to address these limitations.
Conclusions
After multivariate adjustment, SFP demonstrated a potential advantage in speech outcomes over MSP in patients with Veau III cleft palate undergoing repair before 1.5 years of age.
Footnotes
Ethical Approval and Informed Consent
The experimental protocols were approved by the Institutional Review Board (IRB) of West China Stomatology Hospital, Sichuan University (no. WCHSIRB-D-2019-055), in accordance with institutional ethical guidelines and regulations.
Author Contributions
Jingtao Li conceived the idea of writing this manuscript. Yixuan Huang and Jinfeng Dou drafted the manuscript and took the table. Xu Cheng and Bing Shi critically revised the manuscript. All authors contributed to the article and approved the submitted version.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the R&D Program of West China Stomatology Hospital, Sichuan Medical Association Young Scholar Creative Research Program (grant number LCYJ2022-YF-2, No. Q23038).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and/or analyzed during the study are available from the corresponding author upon reasonable request.