
Abstract
Objective
To evaluate 3-dimensional pharyngeal airway changes following 2-jaw orthognathic surgery in skeletal Class III patients and to assess their association with surgical movements.
Design
Retrospective observational study.
Setting
Single tertiary care center.
Patients
Twenty-seven adult patients with skeletal Class III malocclusion who underwent Le Fort I maxillary advancement combined with bilateral sagittal split osteotomy mandibular setback.
Interventions
All patients received 2-jaw orthognathic surgery with preoperative (T0) and postoperative (T1, 6 months) computed tomography imaging.
Main Outcome Measures
Three-dimensional airway volumes of the nasopharynx, oropharynx, and hypopharynx were measured. Correlations between airway volume changes and skeletal movements were analyzed.
Results
Significant regional differences in airway changes were observed. The nasopharyngeal airway volume increased (+1979.1 mm3), while the oropharyngeal airway showed minimal change (+336.4 mm3). In contrast, the hypopharyngeal airway demonstrated a significant reduction (−1087.5 mm3). A strong correlation was found between mandibular setback and hypopharyngeal airway reduction at Point B (r = 0.73, P = .023).
Conclusions
Two-jaw orthognathic surgery results in region-specific airway changes. Hypopharyngeal airway reduction is associated with mandibular setback, while maxillary advancement contributes to upper airway enlargement. These findings reflect morphological rather than functional changes, and further studies incorporating functional assessments are required to determine their clinical significance.
Keywords
Introduction
Orthognathic surgery is a well-established modality for correcting dentofacial deformities and improving both facial esthetics and functional occlusion. 1 Skeletal Class III malocclusion, characterized by mandibular prognathism and/or maxillary deficiency, is particularly prevalent in East Asian populations. 2 Surgical correction often involves mandibular setback, maxillary advancement, or bimaxillary surgery.
Beyond skeletal correction, orthognathic surgery alters surrounding soft tissue and airway structures. The mandible, tongue base, hyoid bone, and pharyngeal walls are anatomically interconnected via muscular and ligamentous attachments. 3 Posterior repositioning of the mandible may displace the tongue base posteriorly, potentially reducing retroglossal airway space. 4
Several studies have demonstrated significant airway reduction following isolated mandibular setback.5,6 However, Santagata et al reported that bimaxillary surgery produces more balanced airway outcomes compared to single jaw setback. 7 Irani et al observed postoperative reductions in oropharyngeal and hypopharyngeal volumes at 6-12 months. 8
Mandibular setback has also been implicated as a potential risk factor for obstructive sleep apnea (OSA). 9 OSA is defined by recurrent upper airway collapse during sleep, measured by the apnea-hypopnea index. 10
Historically, airway assessment relied on lateral cephalometric radiographs. 11 However, these provide only 2-dimensional analysis. Cone-beam computed tomography (CBCT) allows volumetric evaluation but is typically performed in upright position. Supine CT may better simulate physiologic airway conditions during sleep. 12
Despite extensive literature, variability persists regarding the relationship between magnitude of skeletal movement and airway alteration. Limited studies have evaluated volumetric airway changes using supine CT in skeletal Class III patients undergoing 2-jaw surgery.
Therefore, the objective of this study was to assess 3-dimensional airway volume changes following 2-jaw orthognathic surgery in skeletal Class III patients using supine CT imaging. Specifically, we aimed to quantify changes in upper, oropharyngeal, and hypopharyngeal airway volumes; evaluate correlations between skeletal movement magnitude and airway volume changes; analyze differences between patients with postoperative airway reduction and those with airway increase; and discuss implications for surgical planning and airway risk assessment.
Materials and Methods
Study Population
This retrospective study included 27 adult patients (11 males, 16 females) diagnosed with skeletal Class III malocclusion and mandibular prognathism who underwent 2-jaw orthognathic surgery. The mean age was 22.3 years (range 18-35 years).
All patients were treated and received both preoperative and postoperative orthodontic treatment at the Department of Orthodontics.
Inclusion Criteria
Skeletal Class III malocclusion requiring bimaxillary surgery.
Completed pre- and postoperative CT imaging.
Minimum 6-month postoperative follow-up
Exclusion Criteria
Craniofacial syndromes
Cleft lip and/or palate
History of facial trauma
Previous airway surgery
Known diagnosis of OSA
Surgical procedure
All Patients Underwent
Le Fort I osteotomy for maxillary advancement
Bilateral sagittal split osteotomy (BSSO) for mandibular setback
Rigid fixation was applied in all cases. Surgical design aimed to achieve optimal occlusion and facial balance. In some cases, minor occlusal plane modification with clockwise rotation of the maxillomandibular complex (MMC) was incorporated.
Ethical Approval
This study was approved by the Institutional Review Board of Chang Gung Memorial Hospital (IRB No. 202101949B0C501). The study was conducted in accordance with the Declaration of Helsinki. This work was supported by Chang Gung Memorial Hospital (CMRPG8M0781).
Imaging Protocol
Preoperative CT scans were obtained approximately 1 month prior to surgery. Postoperative CT scans were obtained at least 6 months after surgery to allow resolution of acute postoperative swelling. All CT scans were performed in the supine position. Patients were instructed to maintain centric occlusion and refrain from swallowing during image acquisition.
Image Reconstruction and Superimposition
Three-dimensional reconstruction was performed using 3D Slicer software. The Frankfurt horizontal plane was used as the reference horizontal plane. Preoperative and postoperative images were superimposed using the anterior cranial base as a stable reference structure to ensure accurate measurement of skeletal displacement.
Airway Segmentation
Airway compartments were defined as follows: Figure 1.
Upper airway: PNS to the inferior border of C1 Oropharyngeal airway: C1 to C2 Hypopharyngeal airway: C2 to C3
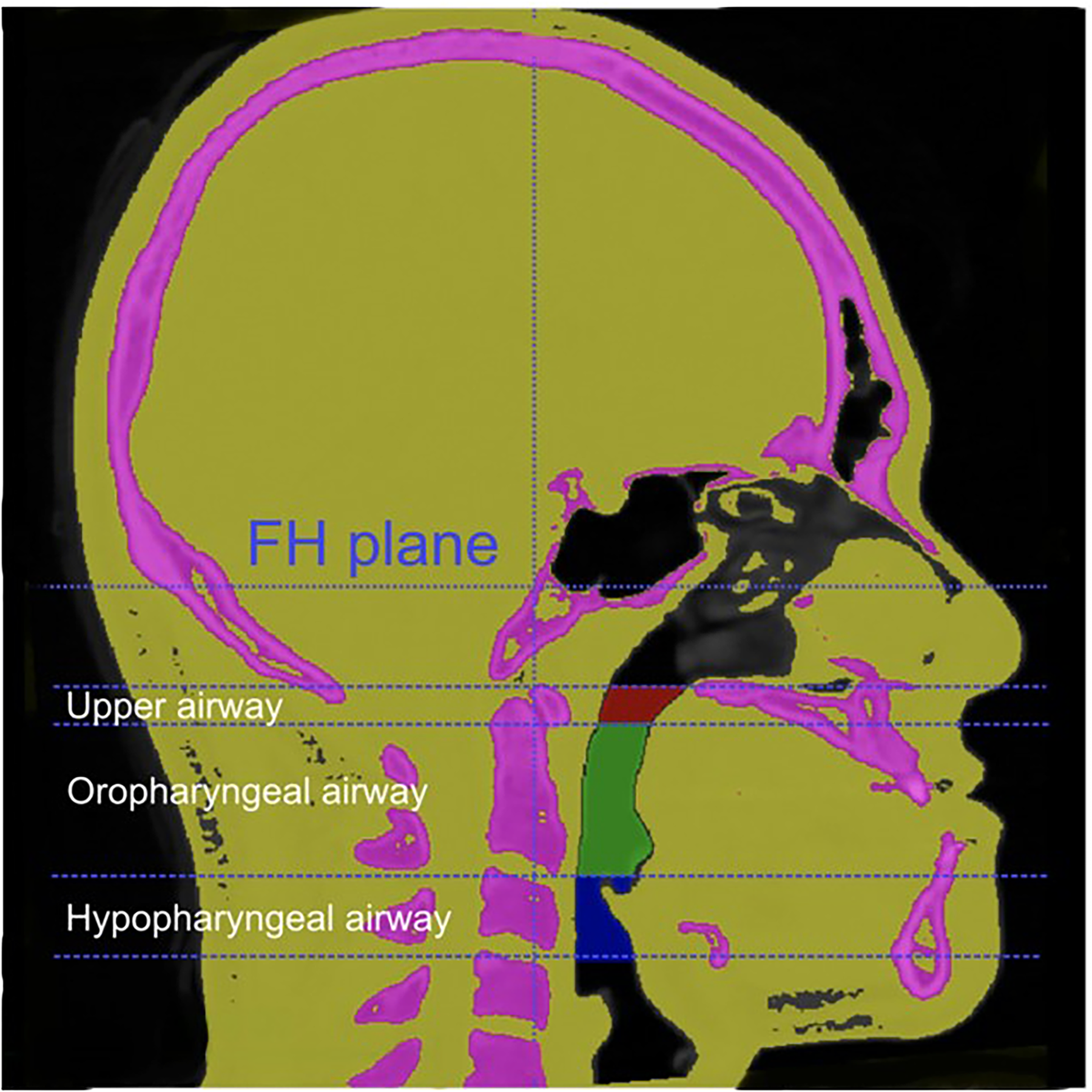
Midsagittal view show different regions of segmental airway in Case-2. The definition of the landmarks: 1. Upper airway (form PNS to C1, in red color): from posterior nasal spine to the most inferior point of first cervical spine. 2. Oropharyngeal airway (from C1 to C2, in green color): from the most inferior point of first cervical spine to the most anterior inferior point of second spine (C2). 3. Hypopharngeal airway (from C2 to C3, in blue color): from the most anterior inferior point of second spine to the most anterior inferior point of third spine (C3).
Airway segmentation was performed using Itk-Snap software. Volumetric calculations were recorded in cubic millimeters Figure 2.
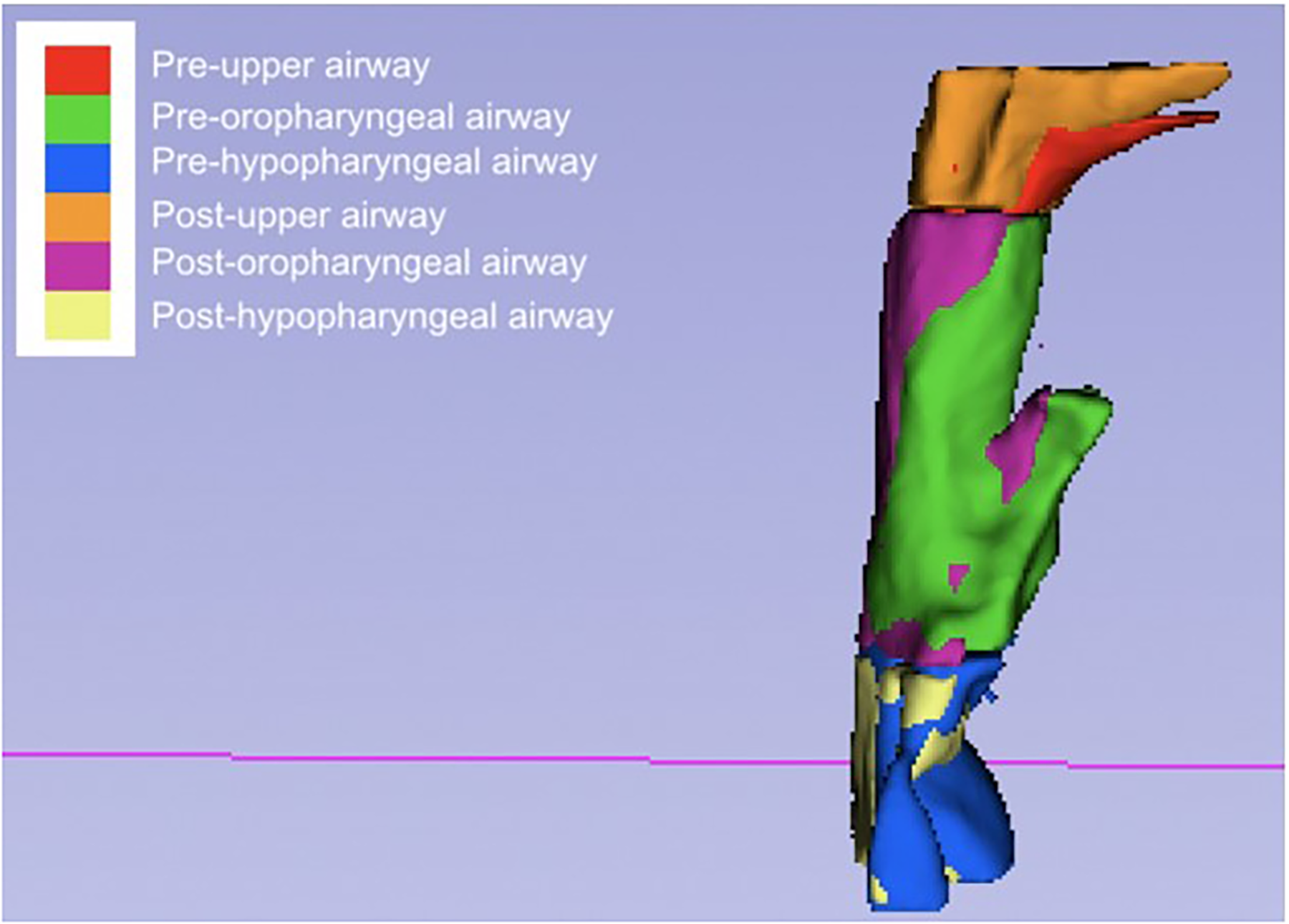
3D model images of superimposition of pharyngeal airway volume in Case-2. We divided the pharyngeal airway in three different regions (Upper airway, Oropharyngeal airway, Hypopharyngeal airway) and represented with separated colors. We could find the postsurgical upper airway and oropharyngeal airway volume increased. On the contrary, postsurgical hypopharyngeal airway decreased. Pre-surgery (T0): 1 month before OGS Post-treatment (T1): 6 months after OGS.
Identified Landmarks
The following landmarks were identified: nasion: the most anterior point on the frontonasal suture, anterior nasal spine (ANS): the tip of the anterior nasal spine, Point A: the deepest midline point in the curved bony outline from the base to the alveolar process of the maxilla, Point B: the most posterior point on the outer contour of the mandibular process in the median plane, Pogonion: the most anterior point of the bony chin in the median plane, upper incisor tip (U1): the tip of the crown of the most anterior maxillary central incisor, lower incisor tip (L1): the tip of the crown of the most anterior mandibular central incisor. Three-dimensional displacement values were calculated. Then we did a superimposition of the presurgical and postsurgical 3D model to analyze.
Grouping and Statistical Analysis
Patients were divided into as follows:
Group A: Decreased total airway volume postoperatively. Group B: Increased total airway volume postoperatively.
Paired t-tests were used to compare pre- and postoperative measurements. Pearson correlation coefficients were calculated to evaluate associations between skeletal displacement and airway volume changes. An unpaired t-test was used to compare skeletal movements between Group A and Group B. Statistical significance was set at P < 0.05.
Results
We present the changes in hard tissue movement as measured by the 3D distance changes of 6 landmarks between pre-surgery and post-surgery. For maxilla advancement, the average amount of movement for the ANS landmark was 2.7 ± 0.96 mm, and for the Point A landmark was 3.12 ± 0.85 mm. For mandible setback, the average amount of movement for the Point B landmark was −6.90 ± 2.00 mm and for the Pogonion landmark was −7.23 ± 2.00 mm (Table 1).
Three-Dimensional Positional Changes of Skeletal and Dental Landmarks (T1–T0).
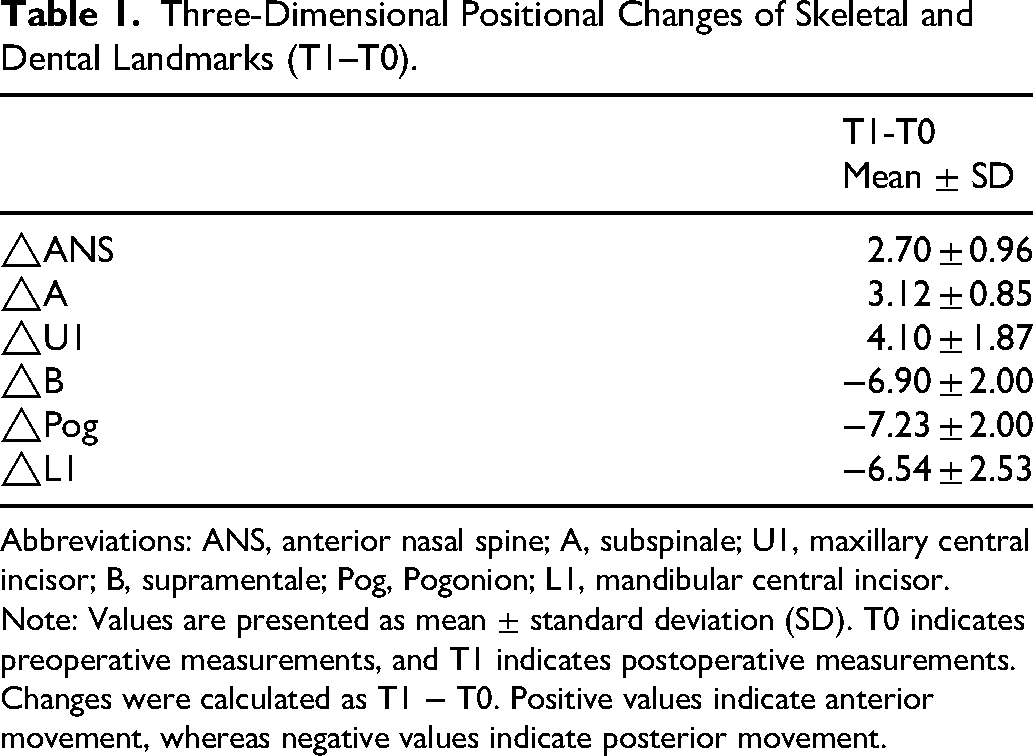
Abbreviations: ANS, anterior nasal spine; A, subspinale; U1, maxillary central incisor; B, supramentale; Pog, Pogonion; L1, mandibular central incisor.
Note: Values are presented as mean ± standard deviation (SD). T0 indicates preoperative measurements, and T1 indicates postoperative measurements. Changes were calculated as T1 − T0. Positive values indicate anterior movement, whereas negative values indicate posterior movement.
The changes in airway volume for the 3D model are presented in Table 2. On average, the upper airway volume increased by 1979.1 mm3, while the oropharyngeal airway volume showed an increase of 336.4 mm3. Conversely, the hypopharyngeal airway volume decreased by 1087.5 mm3. Despite this decrease, the overall airway volume still increased on average by 1228.1 mm3. The changes in airway volume for each individual case are listed in Table 3 which may provide deeper insights into the relationship between surgical intervention and changes in airway volume. The results of this study may inform future surgical planning and patient care.
Changes in Pharyngeal Airway Volume (mm3) Before and After Surgery.
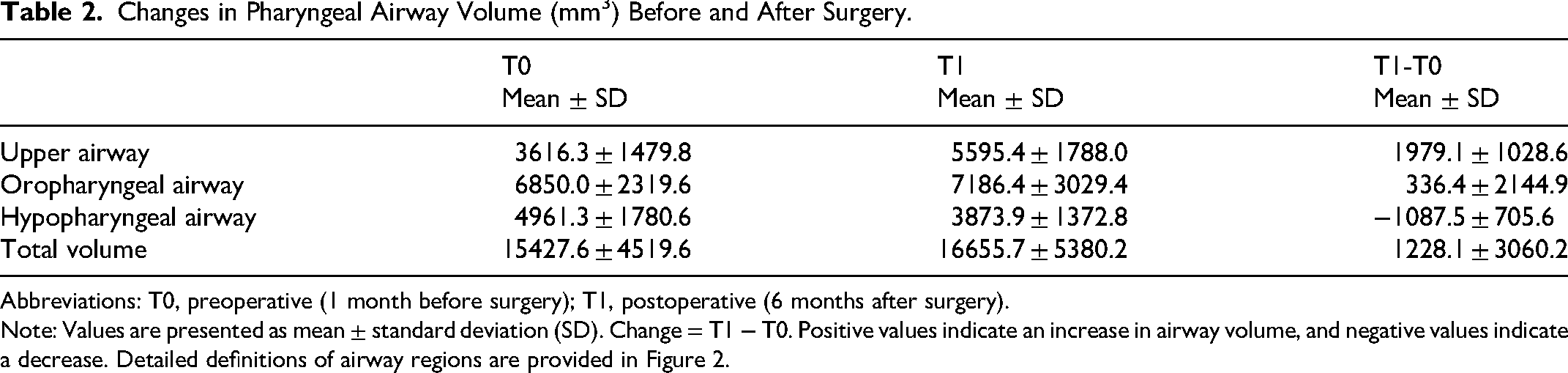
Abbreviations: T0, preoperative (1 month before surgery); T1, postoperative (6 months after surgery).
Note: Values are presented as mean ± standard deviation (SD). Change = T1 − T0. Positive values indicate an increase in airway volume, and negative values indicate a decrease. Detailed definitions of airway regions are provided in Figure 2.
Individual Changes in Three-Dimensional Pharyngeal Airway Volume (mm3).
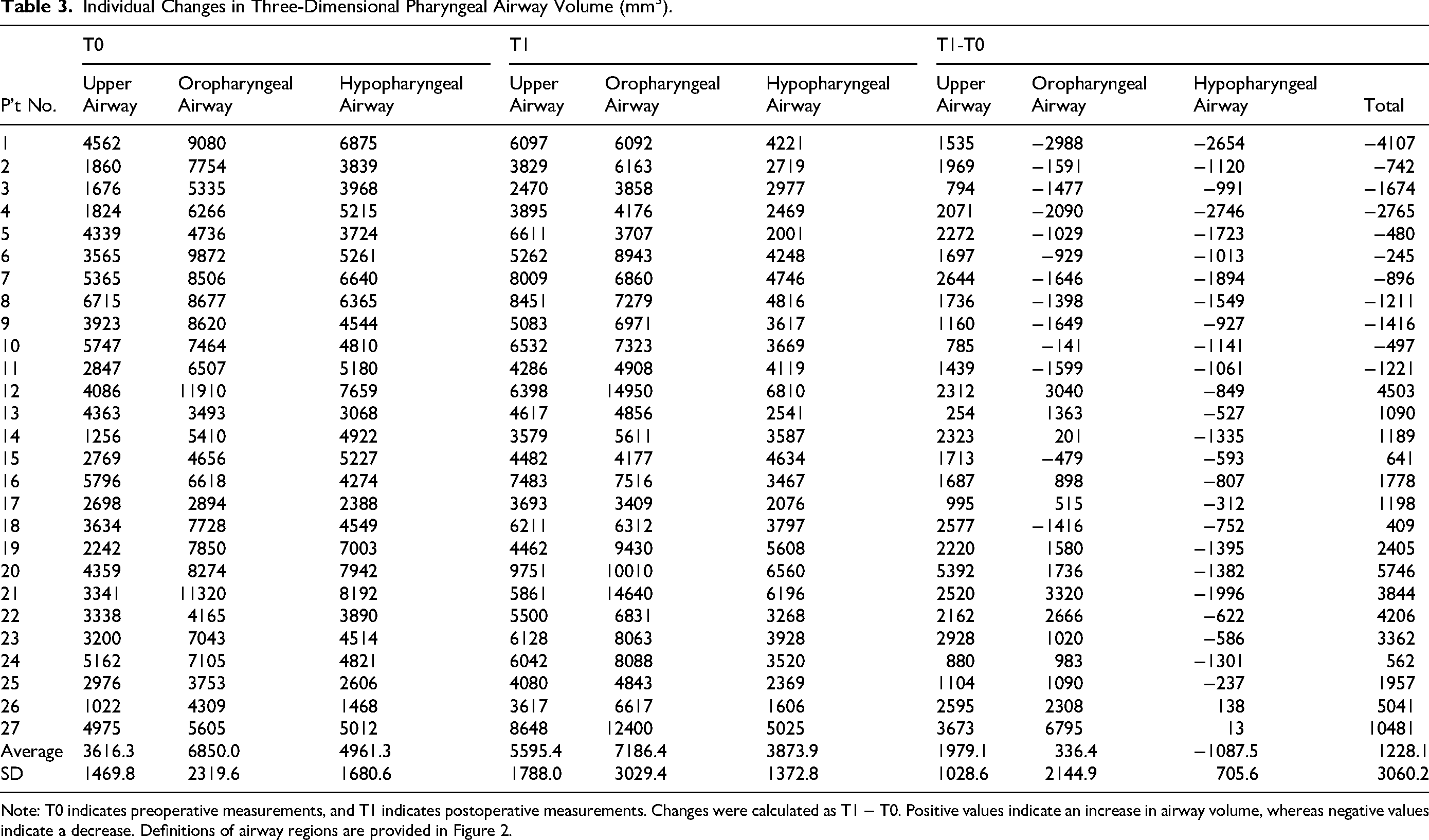
Note: T0 indicates preoperative measurements, and T1 indicates postoperative measurements. Changes were calculated as T1 − T0. Positive values indicate an increase in airway volume, whereas negative values indicate a decrease. Definitions of airway regions are provided in Figure 2.
The correlation between the change in 3D pharyngeal airway volume and the change in 3D distances of the 6 landmarks was calculated and is presented in Table 4. The change in the upper airway showed moderate positive correlation with the movement of the ANS (r = 0.61) and Point A (r = 0.58). The change in the oropharyngeal airway showed only low positive correlation with Pogonion and negligible correlation with the other 5 landmarks. The change in the hypopharyngeal airway showed a high positive correlation with the movement of Point B (r = 0.73) and moderate positive correlation with Pogonion (r = 0.66). The change in the total airway volume showed low positive correlation with the movement of ANS (r = 0.36), Point B (r = 0.31), and Pogonion (r = 0.39).
Correlation Between Three-Dimensional Airway Volume Changes and Skeletal Landmark Movements.
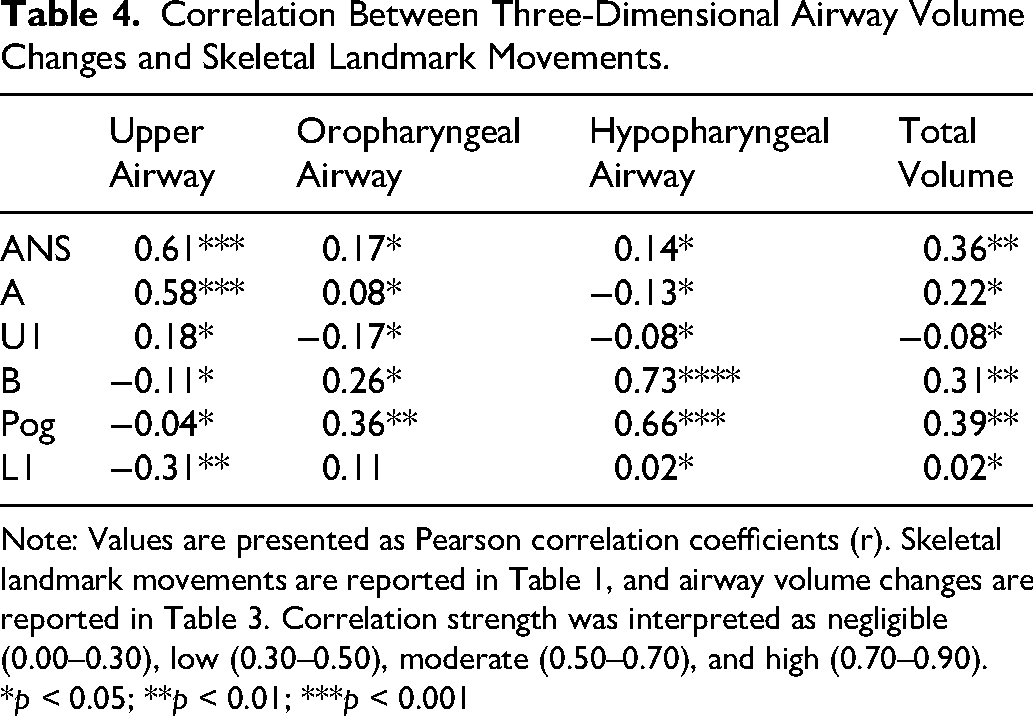
Note: Values are presented as Pearson correlation coefficients (r). Skeletal landmark movements are reported in Table 1, and airway volume changes are reported in Table 3. Correlation strength was interpreted as negligible (0.00–0.30), low (0.30–0.50), moderate (0.50–0.70), and high (0.70–0.90).
*p < 0.05; **p < 0.01; ***p < 0.001
The patients were further divided into 2 groups, Group A and Group B, based on the postsurgical airway volume change. An unpaired t-test was conducted to compare the differences between the 2 groups, with a statistical significance being noted at Point B (P = 0.023) and Pogonion (P = 0.020). The significance level was set at P < 0.05. In Group A, the average regression of Point B was 7.9 mm, and the average regression of Pogonion was 8.2 mm. Meanwhile, in Group B, the average regression of Point B was 6.2 mm, and the average regression of Pogonion was 6.5 mm.
A significant reduction in hypopharyngeal airway volume was observed postoperatively. Correlation analysis demonstrated a strong association between the magnitude of mandibular setback and hypopharyngeal airway reduction, particularly at skeletal landmarks B (r = 0.73) and Pog (r = 0.66).
Discussion
In recent years, the potential for airway narrowing after BSSO for mandible setback in the correction of skeletal Class III pattern has garnered significant attention. While most patients who undergo mandibular setbacks can successfully adapt to the new skeletal and muscular configuration, there are some individuals who may be at risk for developing OSA following the procedure. 11 According to previous research, 5 mandibular setback procedures can be the trigger for the onset of OSA. The mandible, hyoid bone, tongue base, and pharyngeal walls are interrelated through their muscles and ligaments, and a setback in the mandible can result in a narrowing of the hypopharyngeal airway. This narrowing leads to an increase in flow velocity and a reduction in intraluminal pressure, further narrowing the pharyngeal airway. Over time, this can lead to complete pharyngeal obstruction.
On the contrary, Saitoh et al 12 suggested that, although the pharyngeal airway morphology showed marked changes after BSSO, the pharyngeal airway morphology exhibited gradual physiologic readaptation. However, because the lower facial morphology after surgery was retained and stable for a long period, it was considered normal for the pharyngeal airway morphology to adapt after surgery to the improved hard tissue relationship.
Previous studies, such as one conducted using cephalometric analysis, 13 have shown that mandibular setback can lead to significant reductions in the oropharyngeal and hypopharyngeal airways over both the short and long term. Park et al 14 indicate that a significant decrease in pharyngeal depth and a significant posterior movement of the hyoid bone were noted after mandibular setback surgery using lateral cephalometry.
Volumetric analysis by CT showed that the oropharynx decreased after mandibular setback surgery. However, the volume and the axial section area of the airway in the CT images did not change significantly after mandibular setback surgery. Results of CT measurements differed from those of lateral cephalometric radiography, and this might be due to a different head posture while taking the image. Muto et al 15 reported a change of 10° in head posture resulting in a decrease of posterior airway space by up to 4 mm.
In our study, we further utilized 3D computer tomography to quantify the airway volume changes and provide more precise measurements. CT scans have numerous advantages over traditional plain radiographs, including improved visualization of soft tissue and air, which allows for more accurate airway morphology measurements. Compared with CBCT which is taken in standing posture, the medical CT was taken when the patient was in a supine position which is like sleeping.
Despite these findings, it is important to emphasize that the present study evaluates morphological airway changes rather than functional airway outcomes. Airway volume measurements obtained from supine CT imaging do not account for neuromuscular tone or dynamic airway behavior during sleep. Therefore, a reduction in airway volume should not be directly interpreted as airway obstruction or the presence of OSA.
Another important consideration is that total airway volume may not fully reflect airway patency. Previous studies have suggested that the minimum cross-sectional area, often referred to as the “chokepoint,” may have a stronger correlation with airway obstruction. As this parameter was not evaluated in the present study, the clinical implications of the observed airway volume changes should be interpreted with caution.
In addition, although occlusal plane modification, such as clockwise rotation, was part of the surgical planning, its independent effect on airway morphology was not quantitatively assessed. Given that occlusal plane changes may influence both skeletal repositioning and airway configuration, further investigation is warranted to clarify its role.
Table 1 provides important insights into the changes in hard tissue movement resulting from surgical intervention. The increases in the maxilla advancement indicate that the surgical intervention may have improved the position of the maxilla relative to the anterior cranial base. The advancement of the velum and velopharyngeal muscles caused by the Le Fort I osteotomy might be the reason for partly increasing the upper airway. 16 The amount of Point A advancement is more correspond to our surgery design compared with ANS, which is usually trimmed by the surgeon during Lefort I osteotomy for maxilla advancement to prevent and reduce the rotation of nasal tip in the upward direction.17,18 Similarly, the decreases in mandible setback suggest that the surgical intervention may have improved the position of the mandible relative to the anterior cranial base.
Table 2 provides important information on the impact of surgical intervention on the airway volume. The increases in the upper and oropharyngeal airway volumes suggest that the surgical intervention may have improved airway passage in these regions. In contrast, the decrease in hypopharyngeal airway volume may indicate that the surgical intervention had a negative effect on airway passage in this region.
Table 3 shows a decrease in the hypopharyngeal airway volume because of mandibular setback procedures, except for cases 26 and 27. Another study by Kawamata et al 19 used computed tomography to assess the morphological changes in the airway after mandibular setback surgery for prognathism. They found a downward and posterior displacement of the hyoid bone postoperatively and a positive correlation between the amount of mandibular setback and the reduction of the lateral width of the pharyngeal airway and the amount of hyoid bone displacement. In our study, we found a high positive correlation between the hypopharyngeal airway volume and the setback of Point B (r = 0.73), and a moderate positive correlation with the setback of Pogonion (r = 0.66). Cases 26 and 27 were exceptions, where the amount of maxilla advancement and mandible setback were almost the same, resulting in an increased hypopharyngeal airway volume postoperatively rather than a decreased volume.
As for oropharyngeal airway volume change in our study, the results were highly variable. Nevertheless, we found that patients with decreased oropharyngeal airway volume also had decreased total airway volume. To further analyze the effect of mandible setback on airway volume, the patients were divided into 2 groups (group A and group B) based on postsurgical airway volume change. Results from the statistical analysis showed a significant difference in the movement of Point B (P = 0.023) and Pogonion (P = 0.020), with a P-value of less than 0.05 being considered statistically significant. Our findings suggest that patients with a setback of more than 6 mm in Point B and Pogonion are more likely to experience decreased total airway volume. Demetriades et al 20 demonstrated a higher incidence of OSA related to mandibular setback surgery greater than or equal to 5 mm in the mandibular setback surgery (one jaw) group compared to 2-jaw surgery group; however, Uesugi et al 21 found no significant difference. Kamano et al 22 showed that a mandibular setback mean of 9.05 ± 0.17 mm had no correlation to decreased volumetric airway after 6 months. Hong et al 23 reported mandibular setback surgery in both 1 and 2 jaws resulting in decreased volumetric airway.
In addition, our findings indicated that mandible setback surgery can result in a reduction of the hypopharyngeal airway volume. This reduction is due to the backward displacement of the mandible and the subsequent narrowing of the hypopharynx. As the mandible, hyoid bone, tongue base, and pharyngeal walls are interrelated by their muscles and ligaments, mandibular setback can result in a reduction in the hypopharyngeal airway diameter. This reduction can increase the velocity of airflow and decrease intraluminal pressure, leading to further narrowing of the pharyngeal airway. In extreme cases, it can result in complete pharyngeal obstruction, which has been linked to an increased risk of OSA.
In the traditional surgical plan for orthognathic surgery, anterior-posterior discrepancies are corrected by advancement or setback of the jaw along the existing occlusal plane 24 This procedure, however, often fails to produce an ideal result of esthetics especially in Asians who have a preexisting dentoalveolar protrusion. Therefore, alternative treatment designs should be considered. Reyneke et al 25 suggested that an alteration of the occlusal plane could be an alternative. A change of the occlusal plane based on the clockwise rotation of the MMC could be a better solution to overcome the limits of simple advancement and setback of the jaw along the existing occlusal plane, which is like the surgery design in our study. Choi et al 26 indicated that the posterior pharyngeal airway space is decreased somewhat immediately after the orthognathic surgery of Class III patients, this loss could be restored as time passes after soft tissue adaptation and subsidence of swelling. In addition, because the preoperative airway space is enlarged in a class III dentofacial deformity, the posterior pharyngeal airway after a clockwise MMC rotation does not show a significant decrease compared with the normal airway space at the naso- and oropharynx level at 6 months post-operation.
Moreover, there are large individual differences in the airway volume. The average airway volume in our study was 16655.7 ± 5380.2 mm3. Saati et al 27 indicated that males have significantly larger pharyngeal volume. Buchanan et al 28 showed the volumetric airway of normal subjects (non-surgery) was 13,229.58 ± 4499.83 mm3 compared to 8977.43 ± 3360.29 mm3 in OSA patients. Shokri et al 29 reported that the average volumetric airway was 19,773.8 mm3, and different skeletal patterns even showed significantly different volumes. In our study, patients with larger initial airway tend to have a smaller decrease in airway volume after orthognathic surgery.
However, further studies are needed to verify this conclusion and to determine the optimal amount of maxilla advancement and mandible setback that would result in the best balance between correcting the skeletal Class III pattern and maintaining a patent airway. In addition, long-term follow-up is also important to evaluate the stability of the airway volume changes after surgery. The findings of our study provide valuable information for clinicians in considering the trade-offs between correcting the skeletal Class III pattern and maintaining a patent airway in patients undergoing mandible setback procedures.
The present study has several limitations. The sample size is relatively small, which may limit the generalizability of the findings. Furthermore, the absence of polysomnographic data precludes evaluation of functional airway outcomes. Future studies incorporating dynamic airway assessment and functional measurements are necessary to better understand the clinical relevance of these morphological changes.
Nevertheless, this study provides meaningful insight into the relationship between mandibular movement and regional airway changes. The strong correlation between mandibular setback and hypopharyngeal airway reduction highlights the importance of careful surgical planning, particularly in cases requiring large posterior mandibular repositioning.
Conclusion
Two-jaw orthognathic surgery in skeletal Class III patients results in region-specific airway changes, with a significant reduction observed in the hypopharyngeal airway. The magnitude of mandibular setback shows a strong correlation with hypopharyngeal airway volume reduction.
However, these findings should be interpreted as morphological changes rather than direct indicators of functional airway compromise. Further studies incorporating functional assessments, such as polysomnography and minimum cross-sectional airway analysis, are required to clarify the clinical significance of these changes.
Footnotes
Acknowledgements
The authors we would like to thank the Biostatistics Center, Kaohsiung Chang Gung Memorial Hospital for their assistance with all statistical analyses.
Ethical Approval
This study was approved by the Institutional Review Board of Kaohsiung Chang Gung Memorial Hospital(IRB No. 202101949B0C501).
Informed Consent
Written informed consent was obtained from all participants prior to inclusion.
Author Contributions
YJC contributed to conceptualization, study design, supervision, manuscript drafting, and critical revision. TCH contributed to data collection, imaging analysis, statistical analysis, and manuscript preparation. CHC contributed to data acquisition and validation. JPL contributed to surgical planning, operative management, and clinical interpretation. All authors approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Chang Gung Memorial Hospital Research Grant (CMRPG8M0781).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Clinical Trial Registration
IRB No: 202101949B0C501