
Abstract
Objective
To evaluate caregiver experiences with presurgical lip, alveolus, and nose approximation (PLANA) therapy, including adherence, burden, support, and perceived effectiveness in infants with cleft lip and/or palate.
Design
Cross-sectional survey study using an anonymous, voluntary questionnaire administered via Research Electronic Data Capture. Descriptive statistics were used to summarize responses, and qualitative responses were analyzed for common themes.
Setting
Single tertiary care academic institution.
Patients, Participants
Caregivers of infants with cleft lip and/or palate undergoing PLANA therapy were identified through institutional records. Of 48 eligible caregivers, 23 unique responses were included.
Interventions
PLANA therapy utilizing the NoseAlign device with concurrent lip taping, applied at home with periodic clinical follow-up.
Main Outcome Measure(s)
Caregiver-reported adherence, training satisfaction, infant tolerance, caregiver burden, perceived support, and perceived effectiveness.
Results
Caregivers reported high satisfaction with training (73.9% very satisfied) and high adherence, with 87.0% reporting consistent use and 100% reporting daily wear. Most reported no feeding interference (86.4%) and good infant tolerance (73.9% comfortable or very comfortable). Caregiver burden was low, with 60.9% reporting minimal impact on daily routines and 78.3% reporting confidence in application. Perceived support from the medical team was uniformly high (100%). Overall, 90.9% were satisfied with outcomes, and 95.7% would recommend PLANA therapy.
Conclusions
PLANA therapy demonstrates high caregiver satisfaction, strong adherence, and favorable perceived outcomes. Its simplified design may reduce caregiver burden while maintaining effectiveness. Further studies are needed to evaluate long-term outcomes and cost-effectiveness.
Keywords
Introduction
Cleft lip and palate (CLP), one of the most common congenital anomalies of the orofacial region, can have significant functional and psychosocial consequences for both affected children and their caregivers. 1 Patients may experience difficulties with feeding, growth, hearing, and speech, while caregivers often report emotional distress, including fear, grief, and guilt.1,2 As a result, comprehensive cleft care requires a multidisciplinary approach involving audiologists, orthodontists, nutritionists, speech-language pathologists, psychologists, social workers, and plastic surgeons, among others. 3
Presurgical infant orthopedics (PSIO) are commonly used to improve surgical outcomes of infant cleft lip and nasal repair.2,4,5 Available techniques include lip taping, nasal elevators, and nasoalveolar molding (NAM), the most widely utilized PSIO modality in North America. 4 Despite its benefits and widespread use, NAM can impose a substantial burden on caregivers due to the need for frequent in-person visits for device adjustments, as well as associated complications such as oral ulcers and candidiasis, contributing to reported discontinuation rates of up to 23.4%.5-8
Presurgical lip, alveolus, and nose approximation (PLANA) is a novel PSIO technique designed to achieve similar presurgical objectives while mitigating some of the limitations associated with NAM therapy. Traditional NAM therapy requires an initial dental impression and fabrication of a custom intraoral molding plate. The appliance undergoes weekly adjustments to guide approximation of the alveolar segments, and a nasal stent is typically added 6 to 8 weeks after treatment initiation with continued weekly modifications. Treatment generally extends over 3 to 4 months and requires approximately 12 to 16 clinic visits. In contrast, PLANA utilizes a prefabricated extraoral device without an intraoral molding plate and typically requires less frequent follow-up visits every 2 to 4 weeks. 9 PLANA utilizes the NoseAlign device in combination with medical adhesive taping to approximate and support the displaced nasolabial structures without the need for an intraoral plate. The silicone-based device consists of bilateral intranasal components connected by a columellar band, along with a curved external lip support secured with adhesive tapes, facilitating repositioning of the alar rim and cartilage, columella, nasal septum, and alar base. 10 While early studies suggest promising clinical and logistical advantages of PLANA, there remains limited data regarding caregiver experience, adherence, and perceived burden, which are critical to real-world implementation. 9
Methods
A cross-sectional survey study was conducted to evaluate PLANA therapy. Caregivers of infants with cleft lip and/or palate who underwent PLANA therapy at a single tertiary care institution were eligible for inclusion. Caregivers were identified through institutional records and contacted via telephone and/or email to invite participation.
An anonymous, voluntary survey was administered using Research Electronic Data Capture, a secure web-based application for data collection. The full survey instrument is provided in Supplemental Material S1. The survey consisted of multiple domains, including caregiver demographics, training and instruction, adherence to therapy, infant tolerance, caregiver burden, perceived support from the medical team, and perceived effectiveness of PLANA therapy. Responses were collected using a combination of Likert-scale, multiple-choice, and open-ended questions. Survey responses were collected over a 1-month study period.
Descriptive statistics were used to summarize survey responses. Categorical variables were reported as frequencies and percentages. Continuous variables were summarized using means and ranges. Qualitative responses were reviewed and analyzed to identify common themes related to caregiver experience, challenges, and suggestions for improvement. This study was deemed exempt by the institutional review board.
Results
Participant Characteristics
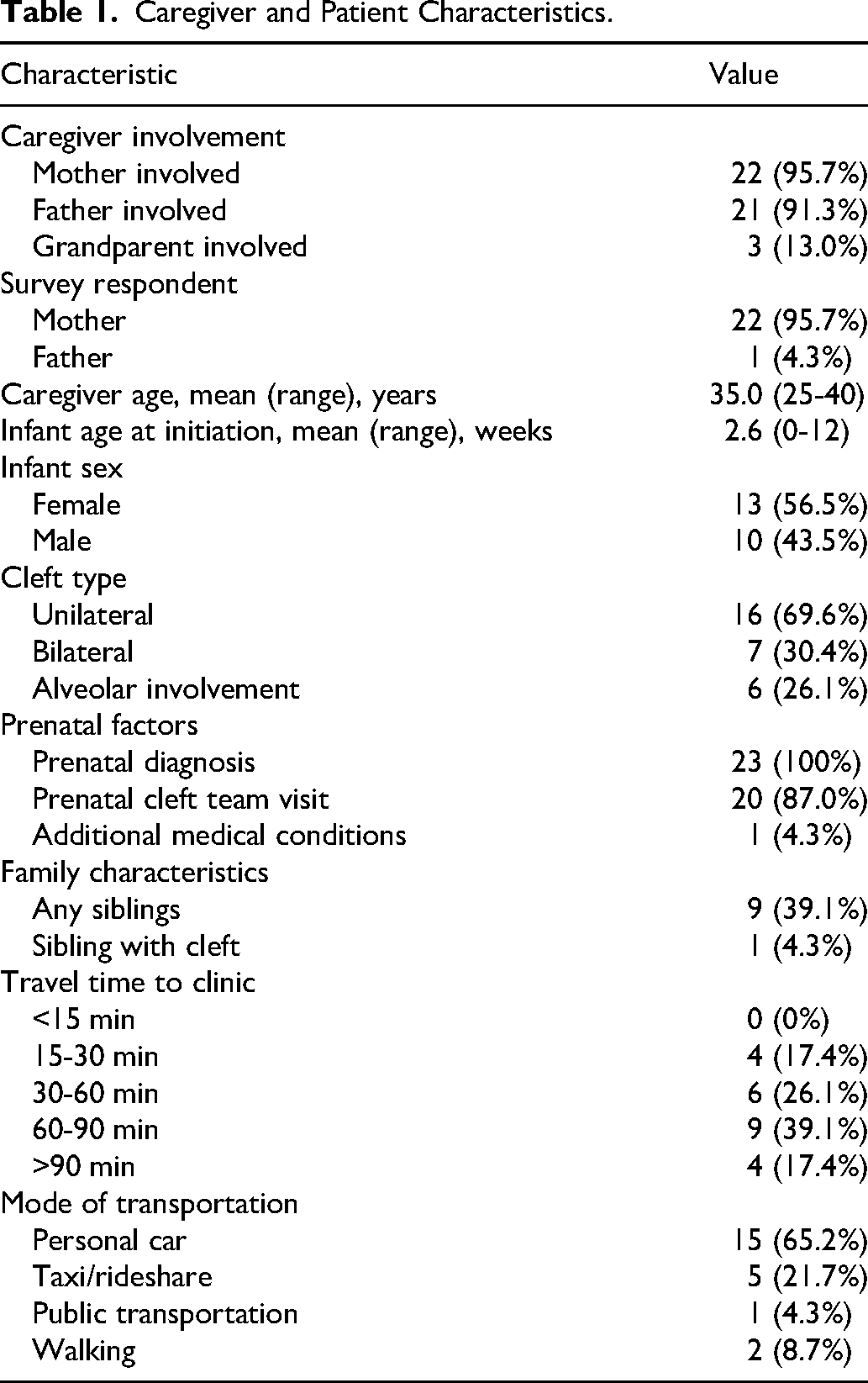
A total of 48 caregivers were eligible for participation, of which 23 completed the survey and were included in the analysis. In all but one case, mothers were involved in the child's PLANA therapy (22/23, 95.7%), and fathers were involved in 21 cases (21/23, 91.3%). Grandparent involvement was reported in 3 cases (3/23, 13.0%). The mother completed the survey in 22 cases (22/23, 95.7%), with one response completed by a father (1/23, 4.3%). The mean caregiver age was 35.0 years (range, 25-40 years). Nine infants had siblings (9/23, 39.1%), including one with a sibling also affected by a cleft (1/23, 4.3%).
Infants began PLANA therapy at a mean age of 2.6 weeks (range, 0-12 weeks). Thirteen infants were female (13/23, 56.5%) and 10 were male (10/23, 43.5%). Sixteen patients had a unilateral cleft (16/23, 69.6%), and 7 patients had a bilateral cleft (7/23, 30.4%). All patients were diagnosed prenatally (23/23, 100%), and 20 caregivers reported attending a prenatal cleft team visit (20/23, 87.0%). One caregiver reported additional medical conditions (1/23, 4.3%), which were not cleft-related.
Travel time to the clinic varied, with no caregivers reporting travel times less than 15 min. Four reported 15 to 30 min (17.4%), 6 reported 30 to 60 min (26.1%), 9 reported 60 to 90 min (39.1%), and 4 reported greater than 90 min (17.4%). The most common mode of transportation was personal automobile (15/23, 65.2%), followed by taxi or rideshare (5/23, 21.7%), walking (2/23, 8.7%), and public transportation (1/23, 4.3%) (Table 1).
Caregiver and Patient Characteristics.
Training and Instruction
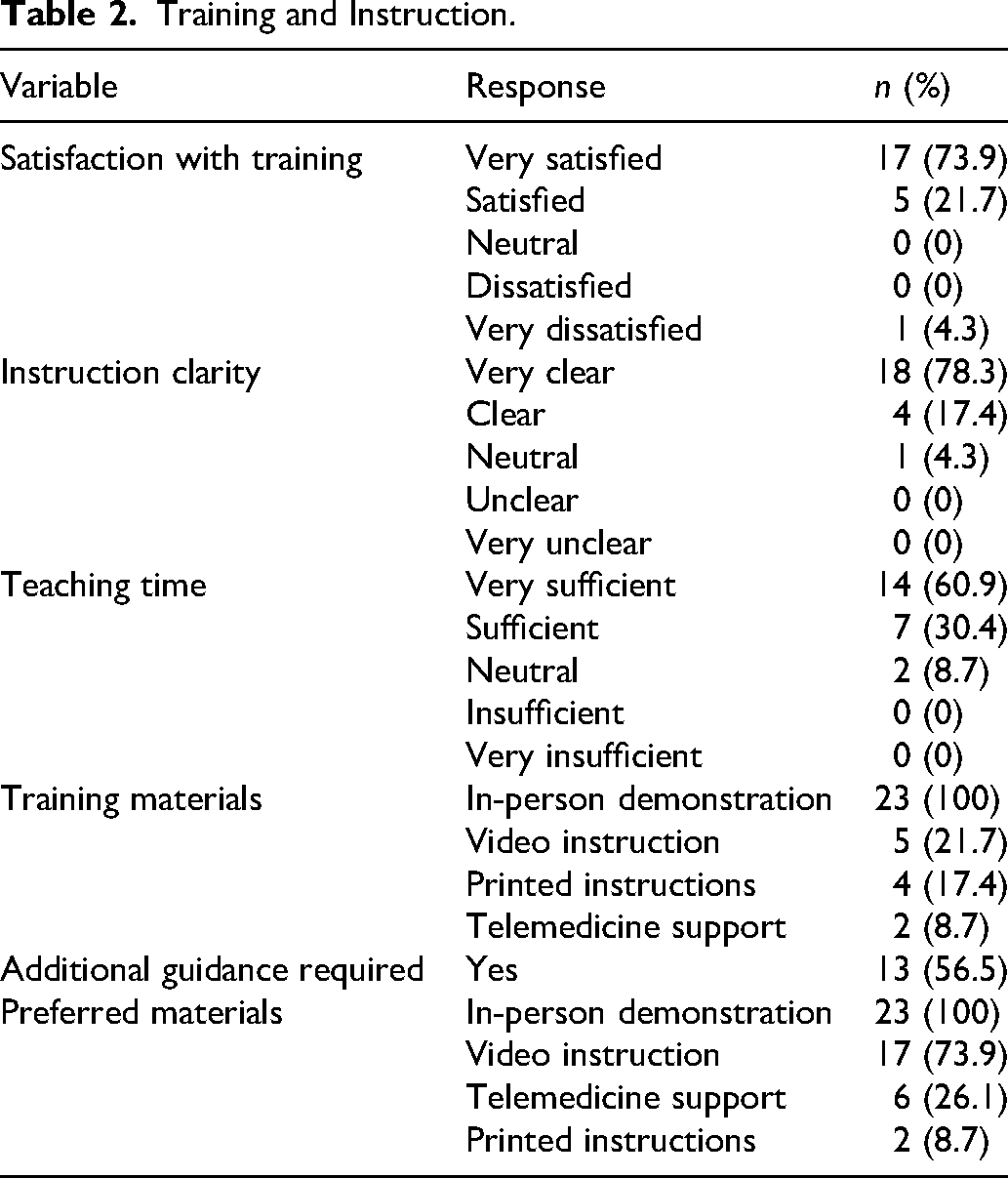
Caregivers reported high levels of satisfaction with training for PLANA therapy. Seventeen caregivers (17/23, 73.9%) reported being very satisfied, 5 (5/23, 21.7%) reported being satisfied, and one (1/23, 4.3%) reported being very dissatisfied. Instructional clarity remained high overall, with 18 caregivers (18/23, 78.3%) reporting that instructions were very clear, 4 (4/23, 17.4%) reporting that they were clear, and 1 (1/23, 4.3%) reporting a neutral response. Time spent on training was also viewed favorably, with 14 caregivers (14/23, 60.9%) reporting that teaching time was very sufficient, 7 (7/23, 30.4%) reporting it was sufficient, and 2 (2/23, 8.7%) reporting a neutral response. All caregivers (23/23, 100%) reported receiving in-person demonstration as part of training. Additional training materials included video instruction (5/23, 21.7%), printed instructions (4/23, 17.4%), and telemedicine support (2/23, 8.7%).
Despite overall high satisfaction with training, 13 caregivers (13/23, 56.5%) reported requiring additional guidance after initial instruction. When asked about preferred training modalities, all caregivers (23/23, 100%) selected in-person demonstration. Video instruction was the most commonly desired supplemental modality (17/23, 73.9%), followed by telemedicine support (6/23, 26.1%) and printed instructions (2/23, 8.7%) (Table 2).
Training and Instruction.
Adherence and Usage
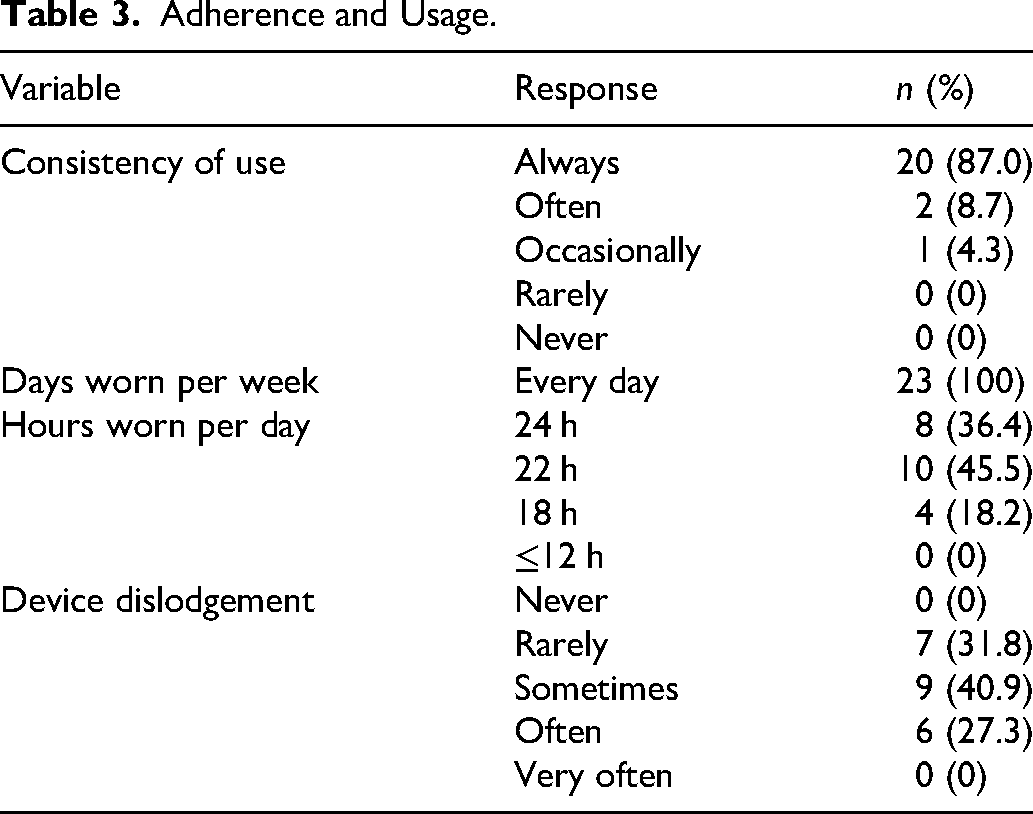
Adherence to PLANA therapy was high. Twenty caregivers (20/23, 87.0%) reported always applying the device as instructed, 2 (2/23, 8.7%) reported often, and 1 (1/23, 4.3%) reported occasional use. All caregivers (23/23, 100%) reported that their infant wore the device every day. With respect to daily duration of use, 8 caregivers (8/23, 34.8%) reported 24 h of use per day, eleven (11/23, 47.8%) reported 22 h per day, and 4 (4/23, 17.4%) reported approximately 18 h per day. No caregivers reported use of 12 h or less per day.
Device dislodgement or removal was reported with varying frequency. Eight caregivers (8/23, 34.8%) reported that this occurred rarely, 9 (9/23, 39.1%) reported sometimes, and 6 (6/23, 26.1%) reported often. No caregivers reported that dislodgement never occurred or occurred very often (Table 3).
Adherence and Usage.
Infant Comfort and Feeding
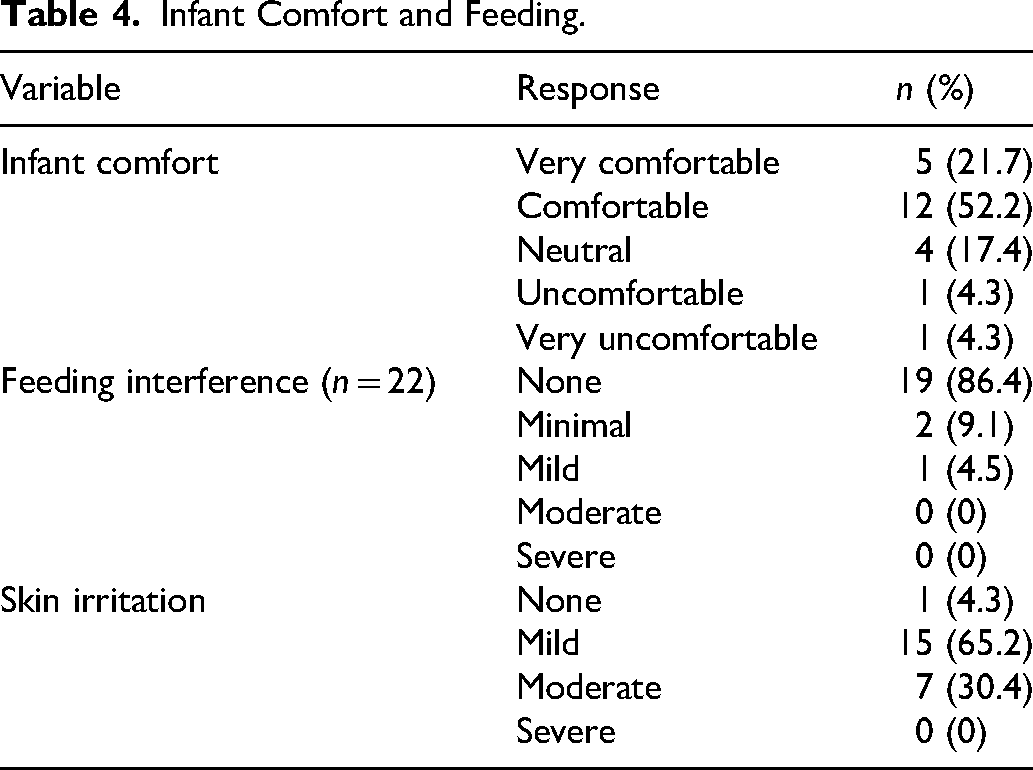
Caregivers generally reported that infants tolerated PLANA therapy well. Five caregivers (5/23, 21.7%) reported that their infant was very comfortable, and 12 (12/23, 52.2%) reported that their infant was comfortable, for a total of 73.9% reporting comfort. Four caregivers (4/23, 17.4%) reported neutral comfort, while one caregiver each reported that their infant was uncomfortable (1/23, 4.3%) or very uncomfortable (1/23, 4.3%).
PLANA therapy had minimal impact on feeding. Nineteen caregivers (19/22, 86.4%) reported no interference with feeding, 2 (2/22, 9.1%) reported minimal interference, and one (1/22, 4.5%) reported mild interference. One caregiver did not respond to this question.
Skin irritation related to the device or adhesive tape was commonly reported. Only one caregiver (1/23, 4.3%) reported no irritation, 15 (15/23, 65.2%) reported mild irritation, and 7 (7/23, 30.4%) reported moderate irritation. No caregivers reported severe irritation. Qualitative responses indicated that irritation was most often attributed to “the tape,” and was commonly described as redness or rash of the cheeks at the site of application. Some caregivers reported skin peeling or minor bleeding with tape removal, particularly as infants became more active. Several caregivers noted that irritation improved with careful removal techniques, including the use of ointments or oils, and was generally manageable. One caregiver specifically noted that irritation occurred early in therapy due to insufficient use of oil during tape removal and improved with more careful technique (Table 4).
Infant Comfort and Feeding.
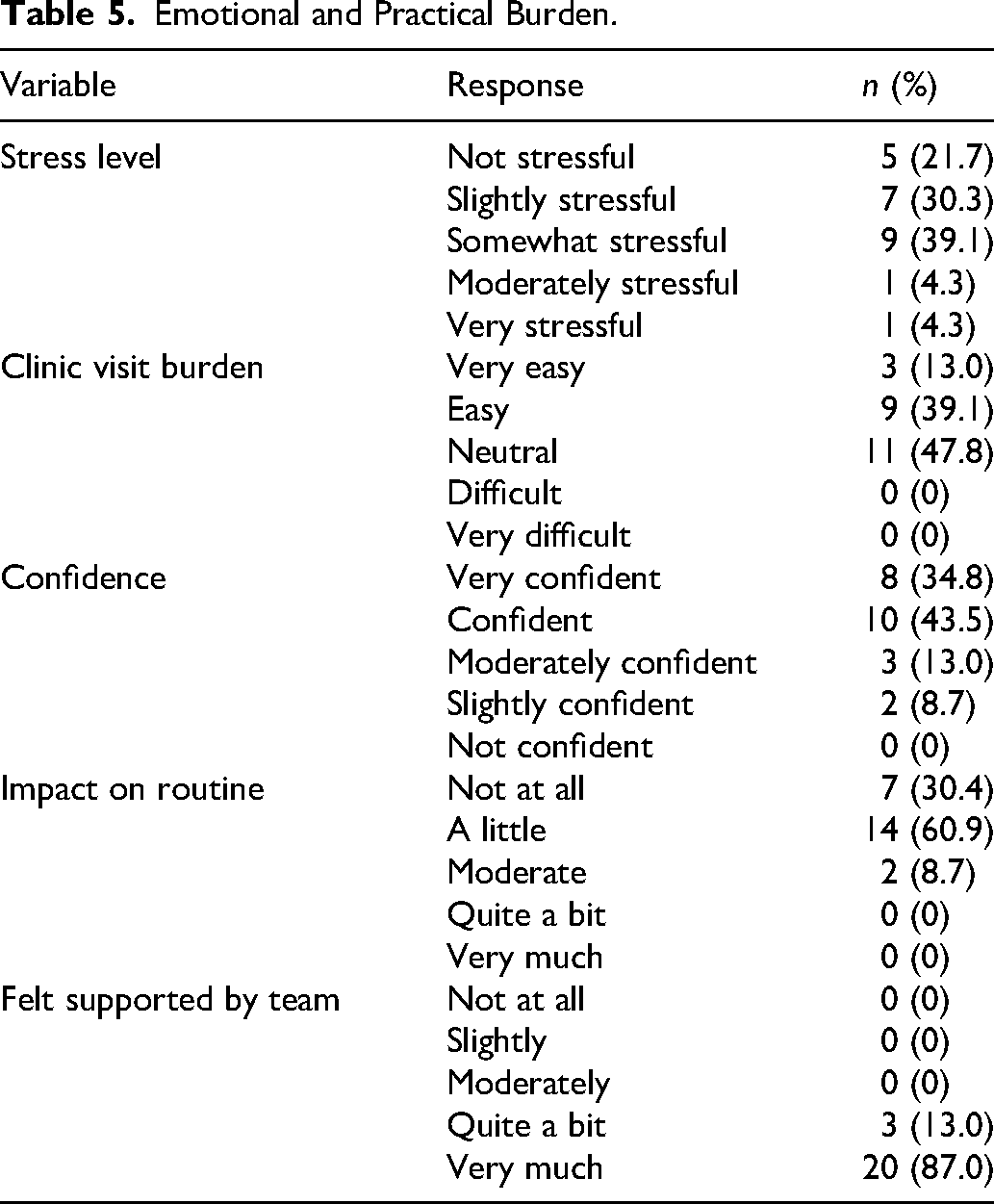
Emotional and Practical Burden
Caregivers reported variable levels of stress associated with managing PLANA therapy at home. Five caregivers (5/23, 21.7%) reported that it was not stressful, 7 (7/23, 30.4%) reported it was slightly stressful, 9 (9/23, 39.1%) reported it was somewhat stressful, one (1/23, 4.3%) reported it was moderately stressful, and one (1/23, 4.3%) reported it was very stressful.
Clinic visits were generally perceived as manageable. Three caregivers (3/23, 13.0%) reported that visits were very easy, 9 (9/23, 39.1%) reported they were easy, and 11 (11/23, 47.8%) reported a neutral experience. No caregivers reported that clinic visits were difficult or very difficult.
Caregiver confidence in applying PLANA therapy was high. Eight caregivers (8/23, 34.8%) reported being very confident, 10 (10/23, 43.5%) reported being confident, 3 (3/23, 13.0%) reported being moderately confident, and 2 (2/23, 8.7%) reported being slightly confident. No caregivers reported being not at all confident.
The impact of PLANA therapy on daily routines was generally minimal. Seven caregivers (7/23, 30.4%) reported no impact, 14 (14/23, 60.9%) reported a small impact, and 2 (2/23, 8.7%) reported a moderate impact. No caregivers reported a significant disruption to daily routines.
Perceived support from the medical team was uniformly high. Twenty caregivers (20/23, 87.0%) reported feeling very well supported, and 3 (3/23, 13.0%) reported feeling well supported. No caregivers reported inadequate support (Table 5).
Emotional and Practical Burden.
Social Media and Peer Support
A minority of caregivers reported using social media, online groups, or peer support during PLANA therapy (8/23, 34.8%). Among those who utilized these resources, Facebook groups were the most commonly used platform (7/8, 87.5%), followed by Instagram (1/8, 12.5%).
Among caregivers who reported using peer support, most found it to be helpful in maintaining adherence. One caregiver (1/8, 12.5%) reported it was very helpful, 3 (3/8, 37.5%) reported it was helpful, 1 (1/8, 12.5%) reported it was moderately helpful, 2 (2/8, 25.0%) reported it was slightly helpful, and 1 (1/8, 12.5%) reported it was not helpful at all.
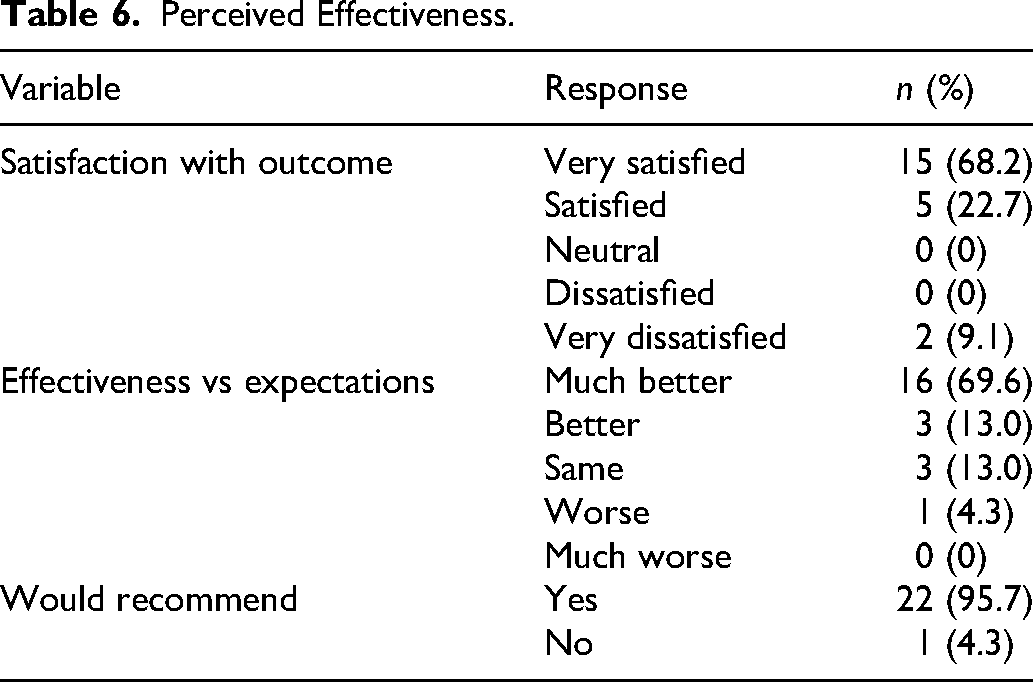
Perceived Effectiveness and Satisfaction
Caregivers reported high levels of satisfaction with the visual reduction in cleft severity prior to surgery. Fifteen caregivers (15/22, 68.2%) reported being very satisfied, and 5 (5/22, 22.7%) reported being satisfied. Two caregivers (2/22, 9.1%) reported being very dissatisfied, while no caregivers reported neutral or dissatisfied responses. One caregiver did not respond to this question.
When asked to compare outcomes to expectations, most caregivers reported that PLANA therapy exceeded expectations. Sixteen caregivers (16/23, 69.6%) reported that results were much better than expected, 3 (3/23, 13.0%) reported better than expected, 3 (3/23, 13.0%) reported outcomes were as expected, and 1 (1/23, 4.3%) reported worse than expected. The caregiver who reported lower perceived effectiveness also reported lower adherence to therapy. No caregivers reported outcomes that were much worse than expected.
Nearly all caregivers indicated that they would recommend PLANA therapy to others (22/23, 95.7%). One caregiver (1/23, 4.3%) reported that they would not recommend the therapy. This was the same caregiver who found that outcomes were worse than expected. In qualitative feedback, however, this caregiver noted that presurgical results were favorable, and dissatisfaction was due to postoperative nasal asymmetry not meeting expectations, specifically citing a smaller nostril on the affected side after discontinuation of therapy (Table 6).
Perceived Effectiveness.
Open-Ended Feedback
The survey included open-ended questions asking caregivers to describe the most challenging aspects of PLANA therapy, the most helpful or beneficial aspects, and suggestions for improving caregiver experience and adherence. These qualitative responses highlighted several common themes related to caregiver experience with PLANA therapy.
The most frequently reported challenges involved device application and maintenance, particularly placement of the nasal stent and lip taping. Caregivers described difficulty applying the device when infants were fussy and maintaining proper placement as infants became more active and began removing the device. Emotional stress related to application was also noted, with some caregivers describing distress associated with restraining their infant during device placement and observing infant discomfort or crying, particularly early in therapy. In some cases, differences in caregiver stress levels contributed to increased overall household stress. Skin irritation associated with adhesive tape was also commonly reported, particularly during removal. Several caregivers noted logistical challenges, including time commitment and travel to clinic visits, although these were generally considered manageable. Most caregivers reported minimal or no challenges and perceived PLANA to be easier to use than alternative therapies such as NAM. However, since most caregivers did not have direct experience with NAM, these perceptions were likely influenced by information obtained from other caregivers, social media platforms, online support groups, or discussions with members of the cleft care team.
The most commonly cited benefits included ease of use, minimal invasiveness, and lack of intraoral involvement, which caregivers perceived as beneficial for feeding. Many caregivers emphasized visible improvement in cleft appearance and nasal symmetry as a key motivating factor for continued adherence. Strong support from the care team was consistently identified as a major positive aspect, with caregivers highlighting accessibility, responsiveness, guidance, and reassurance throughout treatment. Some caregivers specifically noted rapid feedback from providers when sharing photos for review, which increased confidence in proper device application.
Suggestions for improvement centered on enhanced caregiver education and support tools. Many caregivers expressed a desire for clearer instructional resources, particularly video-based demonstrations and practical guidance on device application and tape removal. Additional suggestions included simplifying the taping process, providing pre-prepared taping materials (such as preassembled nasal stent tape constructs), and incorporating shared tips or guidance from other caregivers. Caregivers also emphasized the value of reinforcing communication pathways with the care team, including encouraging submission of photos for feedback. Overall, caregivers expressed high satisfaction with the therapy and appreciation for the care team, frequently noting that the benefits of PLANA outweighed the associated challenges.
Discussion
Families of children with CLP often experience significant financial, emotional, and psychosocial stress. While prior studies have largely focused on the impact of CLP on affected children, the burden on caregivers remains less well characterized. 1
PSIO, although associated with considerable long-term psychosocial benefits, can present a significant source of anxiety for caregivers of infants with a cleft. 11 Sarmadi et al observed that most parents of infants undergoing PSIO reported significant anxiety related to this component of their child's care, which was further heightened by the COVID-19 pandemic. 12 However, studies have also identified that despite an initial period of anxiety related to the increased responsibility associated with PSIO, caregivers develop important coping skills throughout the process.8,13 A study by Sischo et al observed that although caregivers of patients undergoing NAM express initial apprehension about the process, the component of active participation in the child's care can contribute to feelings of empowerment and increased self-esteem. 13 Separately, in a systematic review of the burden of care of NAM, Alfonso et al describe how engagement with the child through PSIO can be used as a coping strategy, which can ultimately contribute to improved caregiver-infant bonding. 8
Prenatal diagnosis and early coordination with a multidisciplinary cleft team can facilitate timely postpartum evaluation and early initiation of PSIO. 14 PSIO is ideally initiated within the first 1 to 2 weeks of life, to take advantage of increased cartilage plasticity associated with elevated maternal estrogen levels in the neonatal period. 15 NAM, the most commonly utilized PSIO modality, requires a maxillary impression obtained by a dental specialist and frequent clinic visits every 1 to 2 weeks for device adjustments as the infant grows. 16 In the present study, over half of caregivers (56.5%) reported travel times of one hour or more to the cleft center. This highlights a persistent disparity in geographic access to comprehensive cleft care. For example, a 2024 geospatial analysis demonstrated that Hidalgo County, Texas, the U.S. county with the highest demand for cleft care, was located 368.4 km from the nearest cleft center. This disparity is further compounded by social vulnerability, as the same county had a Social Vulnerability Index (SVI) of 0.99. 17 In the present cohort, most caregivers reported transportation by personal vehicle (68.2%), which may not be feasible in higher-SVI regions. The prefabricated and extraoral design of PLANA allows for less frequent in-person visits (every 2-4 weeks), with prior studies demonstrating a reduction in clinic visits of up to 61.2%. 9 This may substantially reduce the logistical burden of cleft care during infancy.
Caregivers in this study reported high satisfaction with PLANA training; however, 56.5% required additional guidance after the initial in-person instruction. Through both multiple-choice and open-ended feedback, caregivers expressed that additional educational resources, particularly video-based instruction, may further improve confidence and reduce reliance on in-person visits. PSIO therapies involving an intraoral molding plate, such as NAM, require specialized provider training and ongoing technical expertise, which may limit their availability and contribute to disparities in access.9,18 In contrast, PLANA requires less specialized provider training, which may allow a wider range of providers to be trained in its use, facilitating broader adoption across centers and improving access to presurgical therapy. 9
Adherence to PLANA therapy was high, with no reported interruptions in presurgical therapy. In contrast, nonadherence rates for NAM have been reported as high as 23.4%. 5 Barriers to NAM adherence include reversible side effects such as mucosal ulceration and candidiasis, as well as feeding difficulties associated with the intraoral appliance.5-8 A prior comparative study demonstrated a 72.19% reduction in transient side effects with PLANA compared to NAM, likely attributable to its extraoral design. 9 Additionally, patients undergoing PLANA have exhibited similar weight gain as patients receiving NAM, with significantly greater weight gain per day. 19 In the present study, 86.4% of caregivers reported no feeding interference, which likely contributed to the high adherence observed. Skin irritation was common in the present study, although all reported cases were mild or moderate in severity. Qualitative responses suggested that irritation was most often related to adhesive tape removal and generally improved with proper technique. Thorough caregiver education regarding tape application and removal, along with the use of skin barrier products, ointments, or oils when appropriate, may help reduce irritation and improve treatment tolerance.
Caregiver confidence is also an important component of presurgical cleft care. Prior studies have shown that although caregivers may initially experience apprehension, active participation in PSIO can improve feelings of empowerment and self-efficacy over time. 20 In the present study, 78.3% of caregivers reported feeling confident or very confident in applying PLANA therapy, suggesting that simplified treatment approaches may reduce caregiver burden and improve overall experience.
Visible improvement in cleft appearance and nasal symmetry was frequently cited as a motivating factor for continued adherence. Although PLANA is designed to facilitate approximation of the lip, alveolus, and nose, alveolar changes were not assessed in the present questionnaire-based study. A separate ongoing study is specifically evaluating alveolar outcomes associated with PLANA therapy. Compared to NAM, PLANA allows for earlier initiation of nasal molding, with prior studies reporting initiation of treatment at a mean age of 23.3 days, compared to 48.5 days for infants undergoing NAM. 9 In contrast, NAM typically delays nasal stent placement until partial alveolar approximation is achieved to avoid overexpansion of the nostrils. 9 A comparative study evaluating nasolabial morphology in infants with a unilateral cleft treated with PLANA and NAM found that surgeons rated overall outcomes as comparable or superior with PLANA, despite significantly few visits to the cleft center. 21 In the present study, 95.7% of caregivers responded that they would recommend PLANA to other caregivers, and affirmed that PLANA met or exceeded their expectations. Earlier visible changes in nasal morphology may therefore enhance caregiver motivation and contribute to improved adherence.
This study has several limitations, including a small sample size, single-institution design, and reliance on caregiver-reported outcomes. Although fathers participated in PLANA therapy in 91.3% of cases, only one father completed the survey. Consequently, the findings primarily reflect maternal perspectives and may be subject to response bias. Paternal experiences with treatment adherence, caregiver burden, stress, and perceptions of treatment effectiveness may differ from maternal experiences, limiting the generalizability of these findings to all caregivers. Although a robust list of survey questions was designed, background characteristics such as primary language, ethnicity, and additional socioeconomic factors were not captured and therefore their impact on caregiver experiences was not assessed. Because survey responses were collected anonymously, caregiver-reported outcomes could not be linked to individual medical records, preventing comparison of treatment continuity, visit frequency, treatment effectiveness, or other clinical variables. As a result, differences in caregiver burden, adherence, and satisfaction between the families who did and did not participate in the survey could not be evaluated. Within the study population, no significant differences were observed between caregivers of infants with a unilateral and a bilateral cleft in terms of adherence, perceived efficacy, and likelihood of recommending PLANA. Furthermore, caregiver-reported outcomes were highly skewed toward favorable responses, which limited variability in the study population and precluded robust analysis of predictors of treatment adherence and caregiver satisfaction. While this reflects a positive overall caregiver-reported experience with PLANA, larger-scale investigations are warranted to explore associations between instructional clarity, cleft team support, caregiver confidence with device application, and treatment success. Additionally, financial burden has been identified as a major contributor to caregiver stress in CLP care, likely related to the frequency of clinic visits and associated travel requirements. While this was outside of the scope of the current study, future studies should include cost analyses to compare the economic burden of PLANA and NAM, as well as larger, multicenter investigations to further evaluate caregiver experience and clinical outcomes.
Conclusion
PLANA therapy is associated with high caregiver satisfaction, strong adherence, and favorable perceived outcomes in infants with cleft lip and/or palate. The simplified, extraoral design of PLANA may reduce caregiver burden and improve accessibility compared to traditional PSIO techniques. Further studies are needed to evaluate long-term outcomes and cost-effectiveness.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656261464291 - Supplemental material for Caregiver Experiences With Infant PLANA Therapy for Cleft Lip and/or Palate: A Cross-Sectional Survey Study
Supplemental material, sj-docx-1-cpc-10.1177_10556656261464291 for Caregiver Experiences With Infant PLANA Therapy for Cleft Lip and/or Palate: A Cross-Sectional Survey Study by Chloe Ricke, Lucas R. Perez Rivera, David A. Staffenberg, Roberto L. Flores and Pradip R. Shetye in The Cleft Palate Craniofacial Journal
Footnotes
Ethical Considerations
This study was reviewed and deemed exempt by the NYU Grossman School of Medicine Institutional Review Board.
Consent to Participate
Informed consent was obtained electronically from all participants prior to survey completion.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Pradip R. Shetye has the following financial relationships to disclose: Founder/Scientific Advisor, Stockholder, Pending Patents, and Royalties: CleftAlign, Inc. NoseAlign®, Lip Align® and CleftAlign® are trademarks of CleftAlign, Inc. The NoseAlign device is patent pending. The other authors declare no conflicts of interest. There are no sources of funding to declare.
Data Availability
Data are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.