
Abstract
Objective
To determine the prevalence and anatomical distribution of work-related musculoskeletal disorders (WRMDs) among cleft surgeons and evaluate associations with ergonomic practices, training exposure, and physical activity patterns.
Design
Cross-sectional survey study.
Setting
An International Craniofacial Cleft Workshop.
Participants
Cleft surgeons attending the workshop either in person or virtually.
Interventions
None. A 25-item anonymous questionnaire assessing musculoskeletal symptoms, ergonomic behaviors, and physical activity habits was administered.
Main Outcome Measures
Prevalence and anatomical distribution of self-reported musculoskeletal discomfort among participating cleft surgeons across predefined anatomical regions. Extensive musculoskeletal involvement was defined as symptoms affecting three or more anatomical regions. Associations between ergonomic behaviors, prior ergonomic training, physical activity patterns, and musculoskeletal burden were analyzed to identify potential contributing and protective factors.
Results
A total of 108 surgeons responded to the survey. Musculoskeletal discomfort was highly prevalent, most commonly affecting the neck (68.5%), lower back (38.9%), and upper back (34.3%). Many respondents reported that symptoms interfered with leisure activities, concentration, or surgical performance. Although most surgeons indicated familiarity with surgical ergonomics, only 18.5% had received formal ergonomic training. Preventive intraoperative behaviors such as posture monitoring and micro-breaks were inconsistently practiced. Strength training was independently associated with lower odds of extensive musculoskeletal involvement (Odds ratio 0.61; 95% confidence interval 0.15-0.99).
Conclusions
WRMDs are common among cleft surgeons, and ergonomic awareness does not consistently translate into preventive behaviors. Incorporating structured ergonomics education into surgical training and implementing standardized intraoperative preventive strategies may promote long-term musculoskeletal health and career sustainability in cleft practice.
Keywords
Introduction / Background
Surgical practice is widely recognized as a high-risk profession with respect to work-related musculoskeletal disorders (WRMDs), a major concern within occupational health. The prevalence and severity of ergonomic injuries vary substantially across surgical subspecialties, reflecting differences in operative techniques, posture, and procedural duration. Surgeons involved in cleft lip and palate repair represent a particularly vulnerable population, as their work frequently requires the maintenance of ergonomically unfavorable postures and the performance of meticulous, microsurgical tasks over prolonged periods. These challenges are further compounded by insufficient ergonomic awareness, limited formal training, a paucity of targeted interventions, and the absence of standardized ergonomic monitoring and reporting systems in many surgical institutions. 1
Recent evidence highlights the magnitude of this burden among cleft care providers. A systematic review by Garcia et al reported WRMD prevalence rates ranging from 47.5% to 97% in at least one anatomical region among cleft surgeons, with the neck, shoulders, and lower back identified as the most commonly affected areas. 2 The consequences of WRMDs extend beyond physical discomfort, with potential ramifications for surgeons’ operative efficiency, work absenteeism, career longevity, and decisions to change specialties or retire early. Moreover, these disorders can significantly impair quality of life, sleep patterns, and social functioning. 3
Despite the growing body of literature addressing WRMDs in surgery at large, studies focusing specifically on the unique ergonomic demands of cleft surgery, and on the preventive or therapeutic strategies adopted by cleft surgeons, remain limited. A comprehensive understanding of the musculoskeletal challenges faced by cleft care providers is therefore essential to guide the development of targeted ergonomic interventions, structured training programs, and evidence-based preventive strategies aimed at reducing the risk of injury and improving surgeons’ well-being.
The present study aimed to characterize WRMDs among cleft surgeons through a 25-item survey administered to all surgeons attending an international craniofacial cleft workshop. The objectives of this survey were to assess the prevalence and anatomical distribution of WRMDs, as well as to evaluate symptom management strategies, ergonomic practices, levels of ergonomic knowledge and awareness, attitudes toward ergonomics, and physical activity habits among cleft surgeons. Additionally, the study sought to explore potential correlations between the presence and severity of WRMDs and these ergonomic, behavioral, and lifestyle-related factors.
Methodology
Study Design and Setting
This study employed a cross-sectional survey design and was distributed to all surgeons who attended an international craniofacial cleft workshop held in Latin America, either in person or virtually. Because the workshop location may have influenced respondent geographic distribution, this was considered when interpreting regional representation and generalizability. The workshop was attended by a diverse group of healthcare professionals from multiple countries, including surgeons as well as anesthesiologists, dentists, speech-language pathologists, psychosocial specialists, and other allied healthcare providers involved in comprehensive cleft care. Survey participation was voluntary.
Participants and Eligibility Criteria
The target population comprised cleft surgeons across various surgical subspecialties. Inclusion criteria consisted of physical or virtual attendance at the workshop and active involvement in surgical cleft care. Exclusion criteria included non-surgeon attendees and incomplete survey responses.
Survey Instrument
A 25-item Google Forms questionnaire was developed based on a PubMed literature search regarding surgeons’ ergonomic practices and musculoskeletal disorders. The drafting process utilized AI assistance, followed by expert review and refinement by an experienced cleft surgeon.
The survey covered key domains including respondent demographics, surgical practice characteristics (eg, years in practice and average number of cleft procedures performed per week), prevalence and anatomical distribution of musculoskeletal symptoms, symptom management strategies, frequency and type of physical activity, knowledge and awareness of ergonomics, and ergonomic practices in the operating room.
Weekly physical activity duration was assessed using predefined response categories: no regular physical activity, 1-2 h, 3-5 h, 6-9 h, and ≥10 h per week. These categories were used descriptively and were not intended to represent validated low-, moderate-, or high-intensity physical activity classifications.
Within the survey instrument, the item “appropriate loupes” was intended to refer to surgical loupes selected and adjusted to optimize ergonomic posture and visualization, including consideration of working distance, declination angle, magnification, and individualized fit. Furthermore, within the survey instrument, the item “lightweight headlights” was intended to refer to surgical headlight systems perceived to reduce head-borne weight compared with conventional headlight systems, with the goal of improving ergonomic comfort and minimizing cervical strain. No specific weight-based threshold was provided to respondents.
Data Collection
The electronic survey was distributed via a QR code to all participating surgeons during the workshop, with reminder notifications sent over the subsequent month to optimize response rates. Responses were collected anonymously, and no personally identifiable information was obtained. The study protocol was reviewed by the organization's Ethical Review Board (ERB), which classified the project as exempt minimal-risk research involving an anonymous survey of adult professionals. Participation was voluntary, and completion of the survey constituted implied informed consent.
Outcome Measures
The primary outcome of this study was the prevalence and anatomical distribution of self-reported work-related musculoskeletal discomfort among cleft surgeons. Secondary outcomes included associations between musculoskeletal symptom burden and ergonomic behaviors, physical activity patterns, prior ergonomic training, and practice-related characteristics.
Statistical Analysis
Survey responses were exported into Microsoft Excel (Microsoft Corp., Redmond, WA) and underwent a structured data-cleaning process prior to analysis. Descriptive statistics were generated to summarize the data, including frequencies, percentages, and means with corresponding standard deviations. Extensive musculoskeletal involvement was operationally defined as self-reported discomfort affecting three or more anatomical regions, based on cumulative symptom reporting across survey items. This threshold was selected to represent multi-site involvement indicative of broader musculoskeletal burden. Inferential statistical analyses were conducted using the Statistical Package for the Social Sciences (SPSS; IBM Corp., Armonk, NY). Spearman correlation analyses were performed to examine associations between ergonomic behaviors, physical activity patterns, training exposure, and musculoskeletal outcomes. Univariate binary logistic regression analyses were conducted to identify factors independently associated with extensive musculoskeletal involvement. Odds ratios (ORs) with corresponding 95% confidence intervals (CIs) were calculated. Statistical significance was defined as a P-value of less than 0.05.
Results
Respondent Demographics and Practice Profile
Of the 210 surgeons who attended the workshop, a total of 108 surgeons responded to the survey. This resulted in a 51% response rate, with a predominance of male participants (56.5%) and the majority aged between 30 and 49 years (66.7%). Respondents were geographically diverse, most commonly practicing in Latin America (56.5%). Plastic surgery (51.9%) and oral and maxillofacial surgery (35.2%) were the most represented specialties. Over half of participants had fewer than 10 years of surgical experience (54.7%) and primarily worked in hospital-based (54.6%) and/or academic settings (42.6%), most often within medium-resource environments (59.3%). Most respondents reported a low cleft surgery volume, performing two or fewer procedures per week (76.9%).
When asked about their country of surgical training, respondents reported a wide geographic distribution, with the highest proportions trained in Colombia (14.8%), Ecuador (9.3%), and the United States (8.3%). Similarly, current surgical practice demonstrated a diverse geographic pattern, with most respondents practicing in Colombia (16.7%) and Ecuador (10.2%), followed by the United States (7.4%) and Malaysia (6.5%). Figure 1 presents a geographic map illustrating the distribution of participants according to their country of practice. The demographical characteristics of participating surgeons are summarized in Table 1.
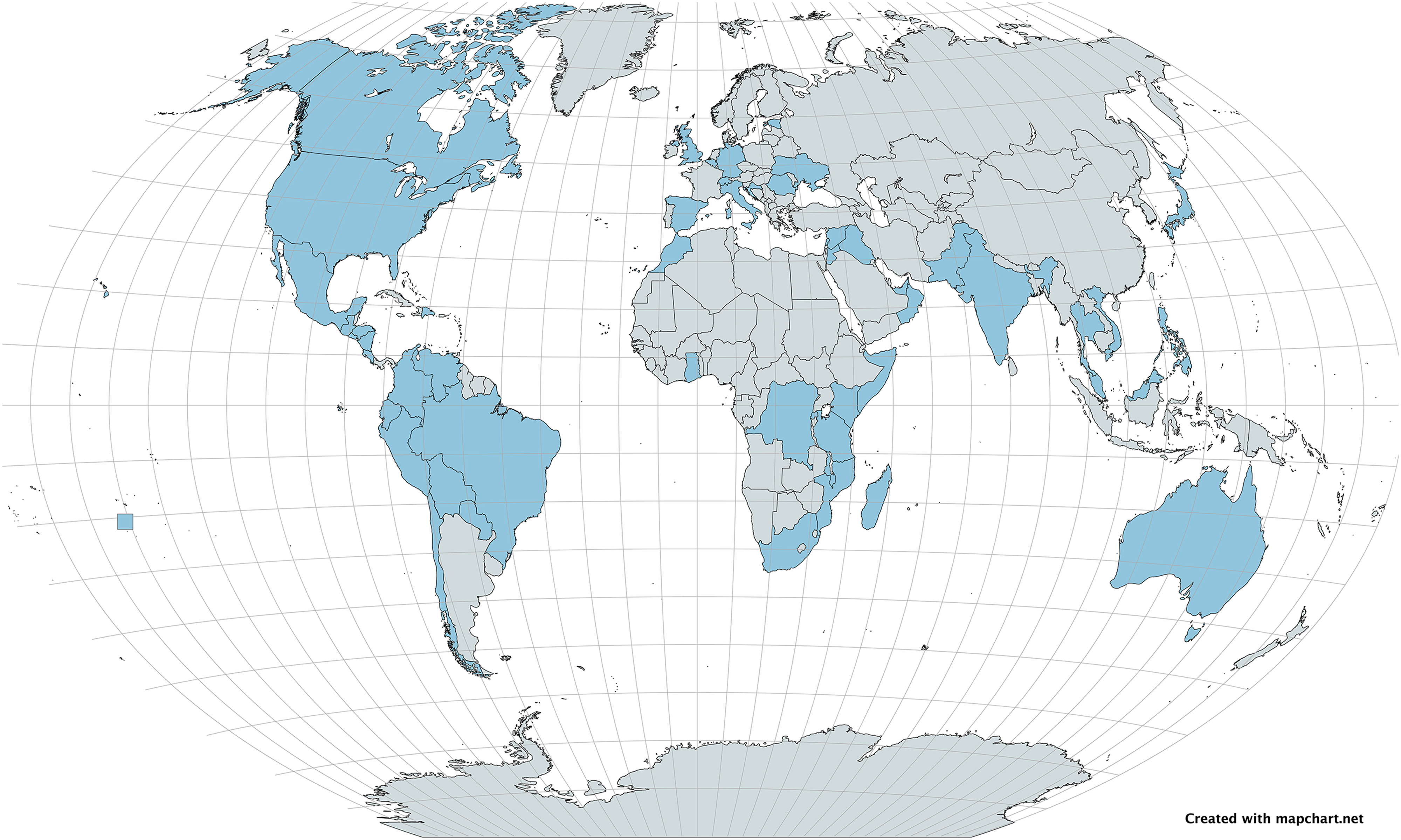
Geographic distribution of participants by country.
Demographic and Professional Characteristics of Participating Surgeons (N = 108).
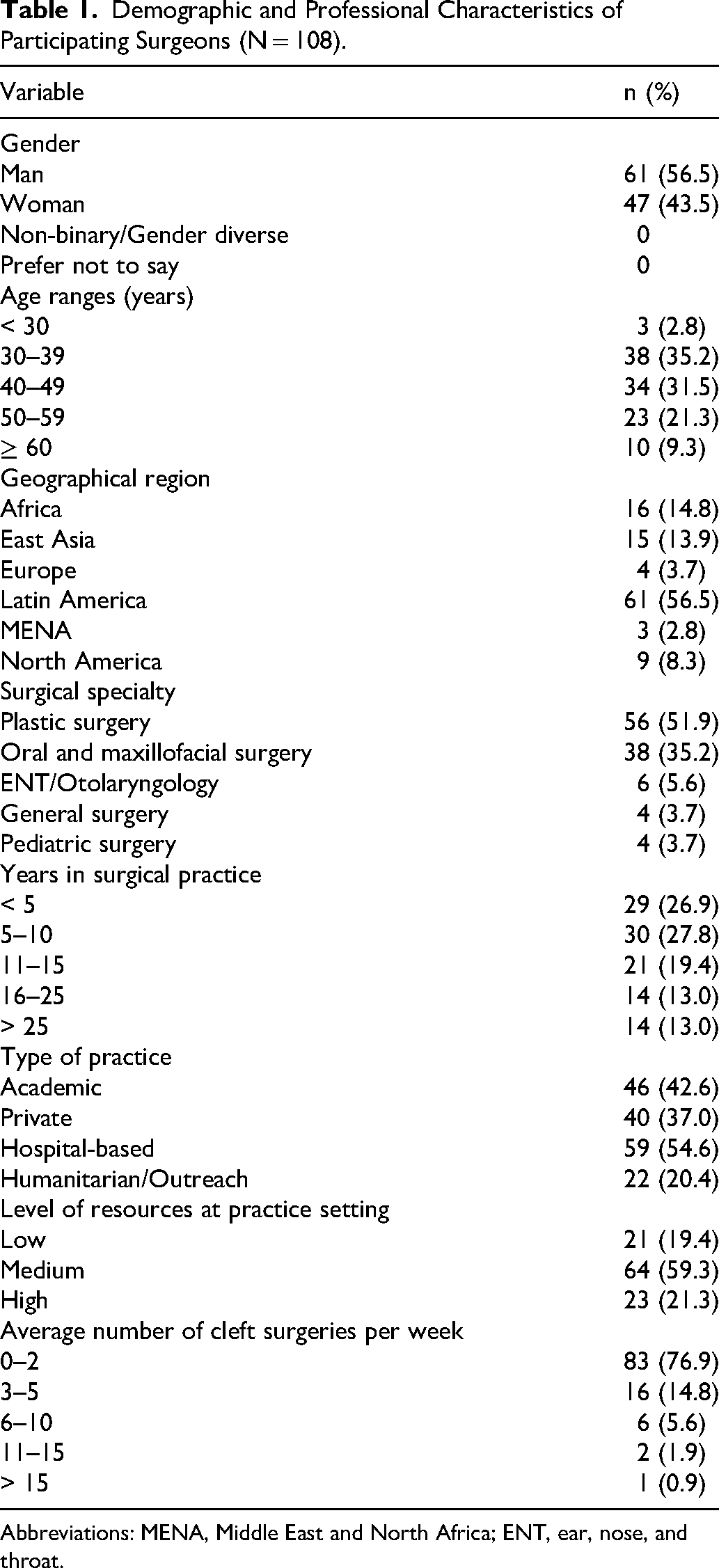
Abbreviations: MENA, Middle East and North Africa; ENT, ear, nose, and throat.
Physical Activity Profile
Of the surgeons who completed the survey, 79.4% engaged in some form of physical activity. Cardiovascular exercise was the most common modality (70.6%), followed by strength training (37.6%) and stretching (31.8%). Mindfulness or meditation practices (22.4%) and yoga or Pilates (16.5%) were less frequently practiced, while 20.6% of respondents indicated no regular physical activity.
Among participants who responded to the question on weekly exercise duration (89.8%), 42.3% reported exercising 1-2 h per week and 39.2% reported exercising 3-5 h weekly. Smaller proportions exercised 6-9 h (14.4%) or ≥10 h (4.1%) weekly, while 10.2% engaged in no regular physical activity.
Musculoskeletal Symptom Burden, Management, and Medical Consultation
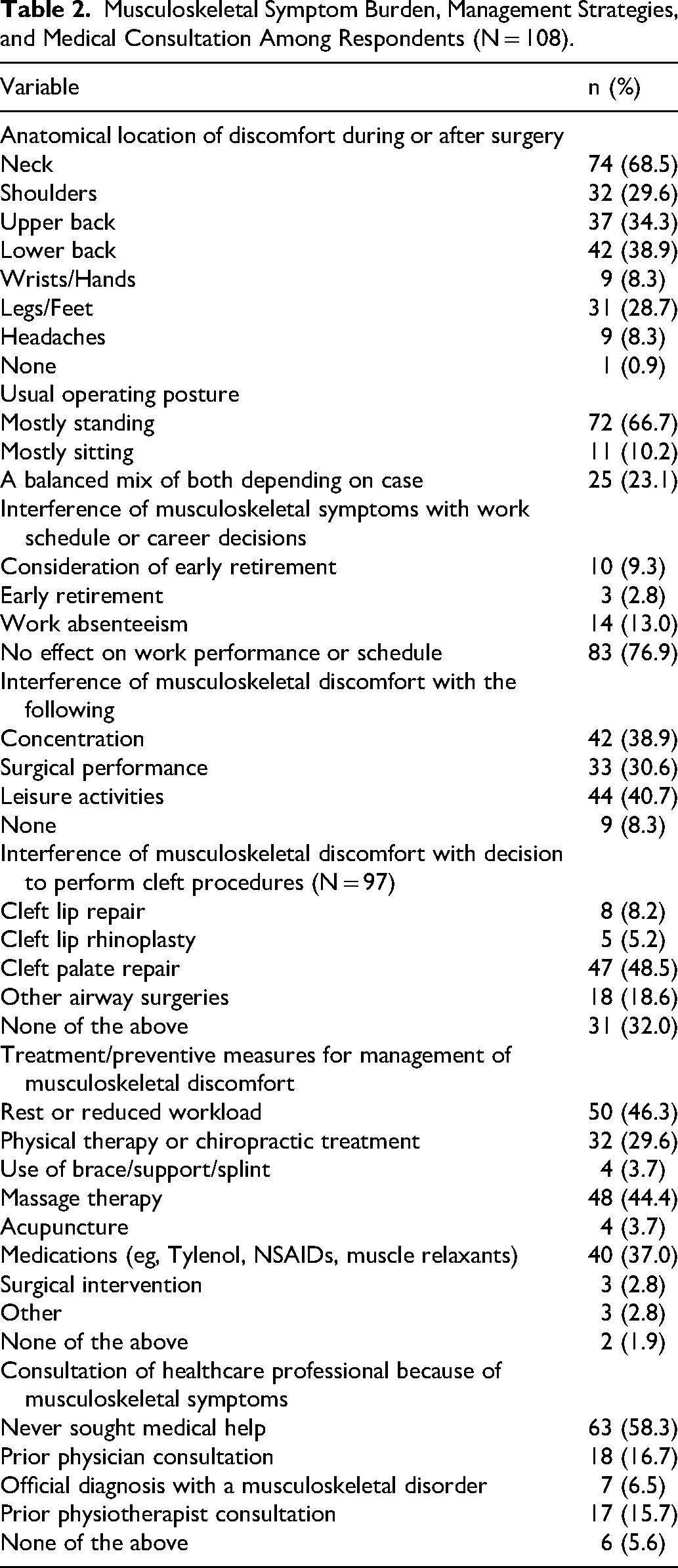
Table 2 summarizes musculoskeletal symptom burden, management strategies, and medical consultation among respondents. Musculoskeletal discomfort during or after surgery was highly prevalent, most commonly involving the neck (68.5%), lower back (38.9%), and upper back (34.3%). Most respondents operated primarily in a standing position (66.7%), while 10.2% worked mostly seated and 23.1% used a balanced mix of both positions depending on the case. Although the majority indicated no effect on work performance or scheduling (76.9%), a substantial proportion reported interference with leisure activities (40.7%), concentration (38.9%), and surgical performance (30.6%), with some reporting work absenteeism (13.0%) or consideration of early retirement (9.3%). Nearly half of respondents (48.5%) reported that musculoskeletal discomfort led them to forgo performing cleft palate repair procedures. Common management strategies included rest or workload reduction (46.3%), massage therapy (44.4%), medications (37.0%), and physical therapy or chiropractic care (29.6%); however, most respondents had never sought formal medical consultation for their symptoms (58.3%).
Musculoskeletal Symptom Burden, Management Strategies, and Medical Consultation Among Respondents (N = 108).
Ergonomic Attitudes and Practices
Figure 2 illustrates self-reported familiarity with the concept of surgical ergonomics and prior participation in formal ergonomic training or workshops. While a majority of respondents reported being familiar with surgical ergonomics (63.0%), fewer had previously participated in formal ergonomics training or workshops (18.5%).
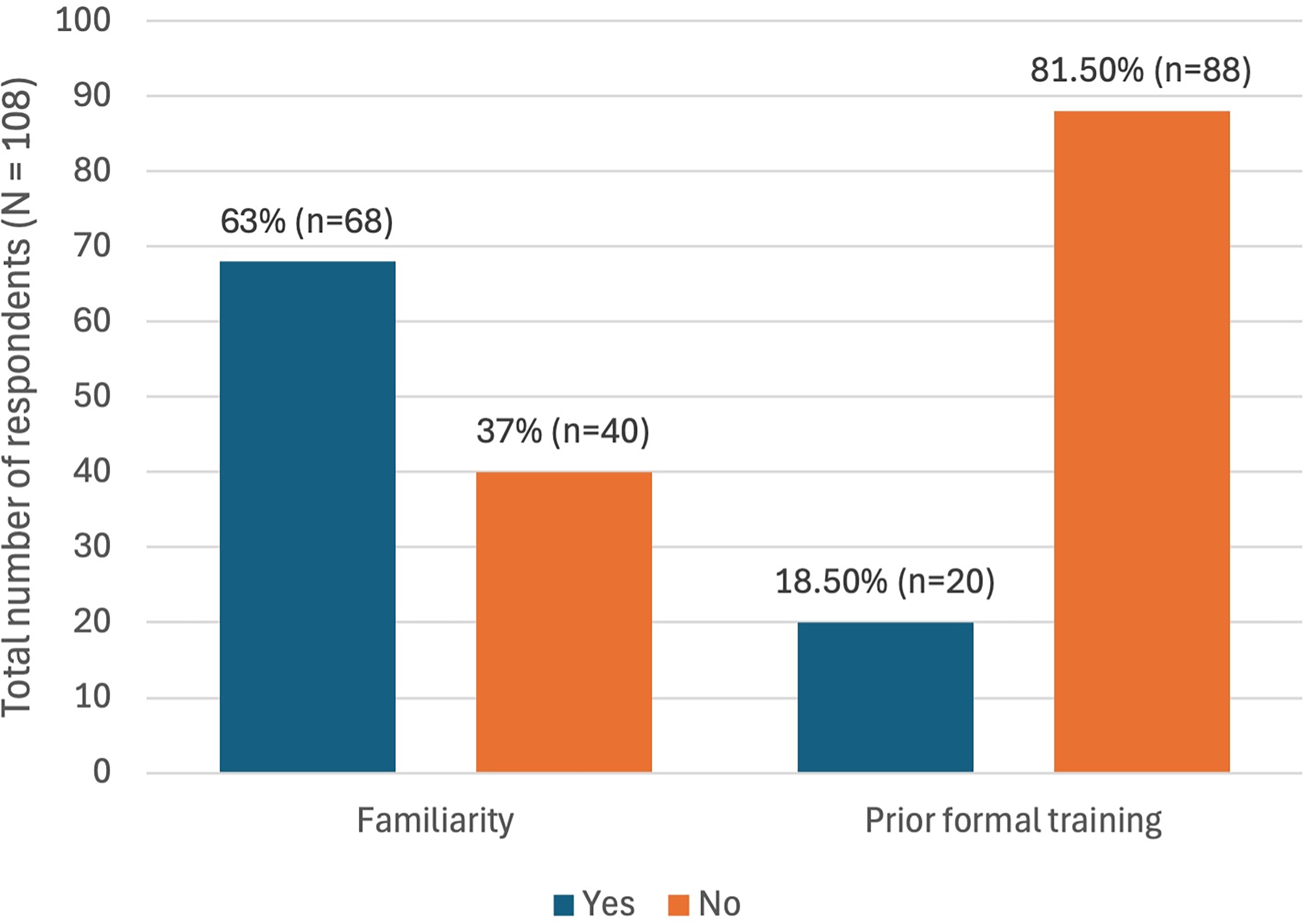
Familiarity with surgical ergonomics and prior ergonomic training among respondents.
Perceived importance of ergonomic awareness for career longevity was high, with 70 respondents (64.8%) rating its importance as 5 on a 5-point Likert scale and 27 (25.0%) rating it as 4. Lower or neutral importance ratings were less frequent, with 7 respondents (6.5%) assigning a rating of 3, 1 (0.9%) a rating of 2, and 3 (2.8%) a rating of 1.
Conscious monitoring of operative posture was variably reported, with most respondents indicating that they monitored posture sometimes (44.4%), while fewer reported doing so often (11.1%) or always (6.5%). In contrast, micro-breaks or stretching during long procedures were infrequently practiced, with the majority reporting never (20.4%) or rarely (43.5%) engaging in these behaviors, and only a small proportion reporting regular implementation (8.3%).
Adjustable operating chairs or tables were the most commonly used ergonomic aids (51.9%), while 36.1% of participants reported utilizing appropriate surgical loupes. Use of other ergonomic equipment was uncommon, including magnetic pads (1.9%) and other specialized tools (0.9%), while 12.0% of respondents reported using none of the listed ergonomic aids (Figure 3).
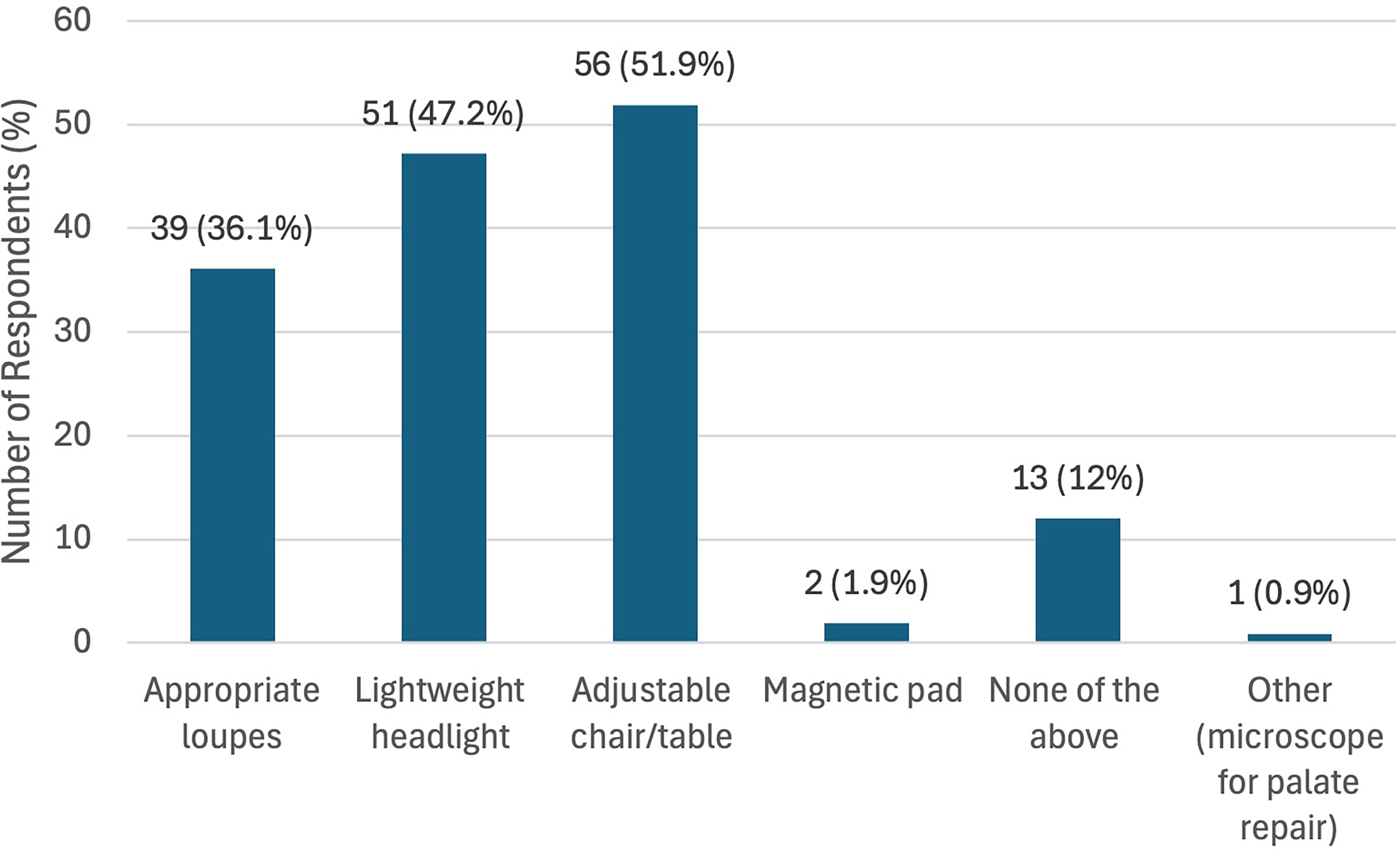
Use of ergonomically optimized equipment in the operating room among survey participants.
Ratings of the perceived impact of ergonomic and physical wellness habits on work-related outcomes were generally favorable across all assessed domains. High levels of perceived improvement (ratings 4-5) were reported by 57 respondents (52.8%) for physical function and mobility, 55 (50.9%) for fatigue and stress reduction, 60 (55.6%) for mental focus and team communication, 58 (53.7%) for surgical performance and efficiency, and 53 (49.1%) for error reduction or accuracy. Mean Likert scores across domains were consistently above the midpoint of the scale, ranging from 3.39 ± 1.22 for error reduction or accuracy to 3.52 ± 1.18 for mental focus and team communication (Figure 4).
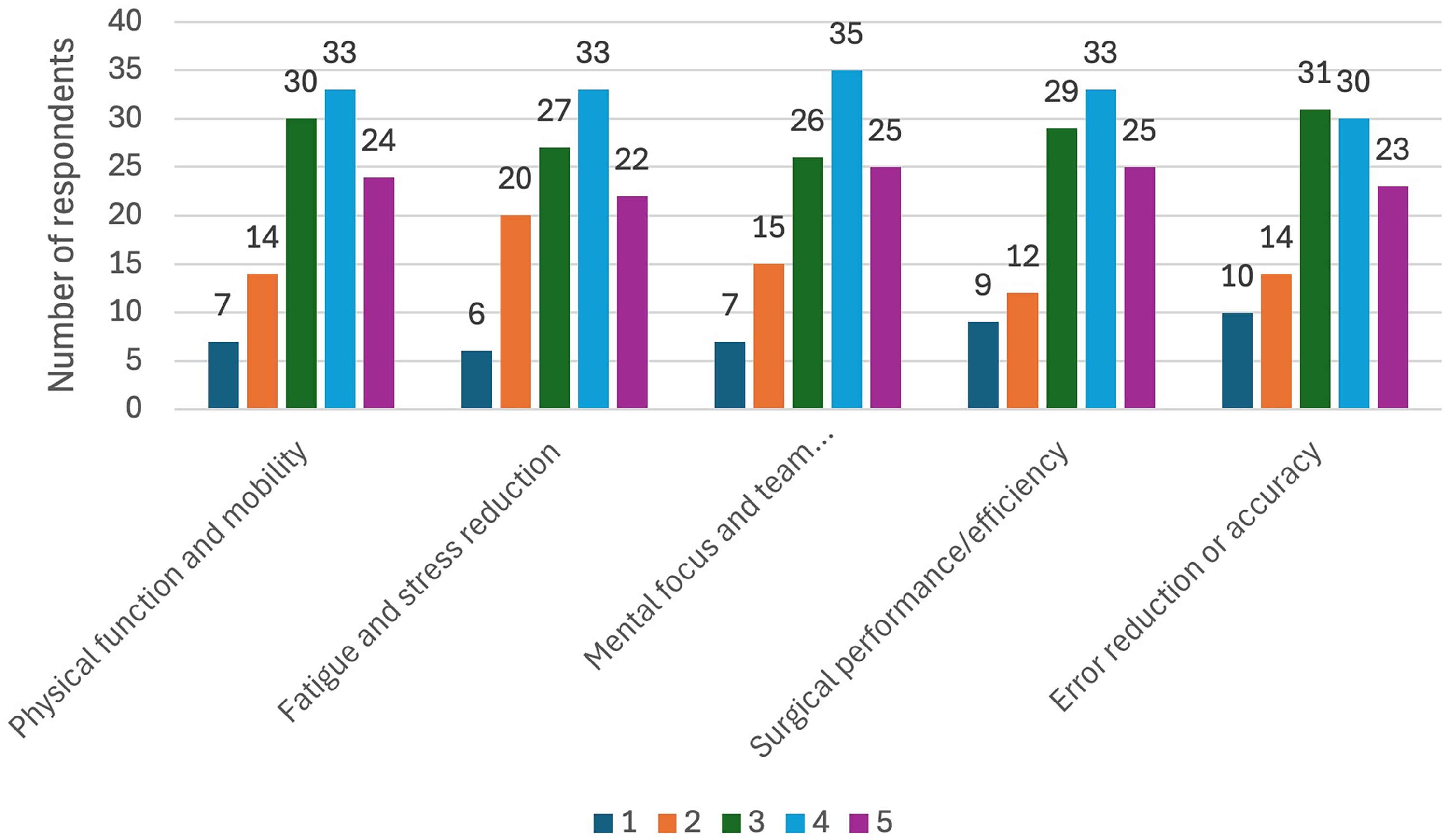
Perceived impact of ergonomic and physical wellness habits on work-related outcomes among respondents.
Discussion
Our survey aimed to assess the prevalence and anatomical distribution of WRMDs among cleft surgeons attending an international craniofacial cleft workshop, while also providing insight into their knowledge, attitudes, and operating room ergonomic practices, as well as strategies for symptom management and mitigation. Our findings demonstrate that increasing years in surgical practice are associated with a greater perceived importance of musculoskeletal health and operating room ergonomics. Nevertheless, despite this heightened awareness, and even among surgeons reporting prior formal ergonomics training, the actual implementation of ergonomic guidelines and preventive practices remained substantially lower than expected. This highlights a persistent and clinically relevant gap between ergonomic awareness and real-world behavioral adoption.
Anatomical Locations
Our results align closely with existing literature regarding the most commonly affected anatomical regions, with the neck, lower back, and upper back emerging as the top three sites of discomfort. Similar distributions have been reported by Rodman et al and Shah et al, who likewise identified the shoulders, neck, and lower back as the most frequently involved regions among craniofacial surgeons.4,5 These consistent findings reinforce the notion that sustained static postures, prolonged cervical flexion, and cumulative truncal loading remain central ergonomic challenges in cleft and craniofacial surgery, regardless of surgeon experience or geographic setting.
Physical Activity and work-Related Musculoskeletal Disorders
Most respondents (79.4%) engaged in some form of physical activity, with an estimated mean weekly exercise duration of approximately 3.3 h, closely mirroring values reported in comparable surgical populations. 6 Consistent with prior findings by Lobo et al, no association was observed between time spent exercising per week and the absence of WRMDs. 6 This may reflect the high overall prevalence of musculoskeletal symptoms in our cohort or the non-specific nature of exercise routines, which may fail to adequately target vulnerable muscle groups or, in some cases, exacerbate symptoms. These findings suggest that exercise quality and specificity may be more important than duration alone.
Binary logistic regression analyses were conducted to identify potential contributing and mitigating factors involved in extensive musculoskeletal involvement, defined as pain affecting three or more anatomical regions. Strength training, among the various forms of physical activity assessed, emerged as a statistically significant protective factor (OR 0.61 95% CI 0.15-0.99). Strength-based exercise has been consistently shown to confer both preventive and therapeutic benefits in the management of musculoskeletal disorders across multiple occupational and clinical populations.7,8 Hamdan et al emphasize strength training as a core component of musculoskeletal longevity in cleft providers, alongside stretching, posture optimization, and aerobic conditioning within a structured ergonomics curriculum. They specifically advocate for regular core and targeted resistance training to enhance spinal stability, preserve stamina, and mitigate neck, back, and shoulder pain associated with prolonged operative postures. 7 Andersen et al demonstrated in their randomized controlled trial, that targeted resistance training of the neck and shoulder musculature, even when performed for very short daily durations, resulted in significant reductions in pain intensity and muscular tenderness compared with control interventions. These benefits were accompanied by modest but meaningful improvements in regional muscle strength, supporting strength training as an effective strategy for both symptomatic relief and functional enhancement. 9 This finding supports the inclusion of strength training in surgeon-specific wellness programs.
Musculoskeletal Health and Operating Room Ergonomics
Findings from this survey showed that surgeons sometimes or only rarely consciously monitor their posture intraoperatively, supporting prior observations by Tandon et al, who suggested that deep cognitive immersion during surgery may limit real-time postural awareness. 10 A similar pattern was observed for the practice of micro-breaks, which were infrequently performed in the cohort despite robust evidence demonstrating their role in reducing musculoskeletal discomfort and improving physical function and performance. Together, these findings underscore the difficulty of maintaining consistent ergonomic behaviors during demanding surgical procedures.
In fact, data from this survey revealed a positive association between conscious posture monitoring and the performance of intraoperative micro-breaks (ρ = 0.439; P < 0.001), as well as between posture monitoring and time spent exercising per week (ρ = 0.276; P = 0.004). These relationships likely reflect a shared preventive ergonomic mindset. Surgeons who consciously monitor their posture may exhibit heightened bodily awareness and self-regulatory capacity, facilitating both immediate corrective behaviors in the operating room and sustained engagement in health-promoting activities outside the surgical environment. Preventive behaviors also tend to cluster and may be reinforced by prior ergonomic education, institutional culture, and a proactive focus on musculoskeletal sustainability rather than symptom-driven responses. This suggests that surgeons who adopt one ergonomically favorable behavior are more likely to engage in others as part of a broader preventive strategy.
Among the physical activity modalities assessed, stretching was the only activity positively associated with posture monitoring (ρ = 0.298; P = 0.002). The association between stretching and reduced musculoskeletal symptoms is likely explained by its direct effect on posture-related muscle tension and proprioceptive awareness. Given its practicality and routine inclusion in ergonomic education, stretching has been consistently highlighted by Shah et al and Hamdan et al as a fundamental preventive strategy against WRMDs.5,7 Hamdan et al proposed the triple A framework, Avoid, Adopt, and Advance, as a practical approach to ergonomic sustainability in surgical practice. Surgeons should Avoid back-breaking and static positions, Adopt neutral posture, micro-breaks, and targeted strength and stretching strategies, and Advance time utilization to integrate these behaviors into routine operative workflows. Overall, the observed association underscores stretching as a posture-centric behavior that likely enhances intraoperative postural awareness, reinforcing its role as a practical and immediately applicable strategy for promoting conscious posture monitoring during surgery.
The absence of a significant association between intraoperative posture monitoring and number of painful regions (ρ = -0.078; P = 0.425), or similarly micro-break frequency and number of painful regions (ρ = -0.130; P = 0.179) likely reflects the multifactorial and cumulative nature of musculoskeletal symptoms in surgeons. Self-reported ergonomic behaviors may not translate into consistent, sustained, or biomechanically effective exposure reduction, particularly in the context of operative constraints, prolonged case duration, and equipment-dependent positioning. Additionally, surgeons already experiencing pain may be more inclined to adopt posture monitoring or micro-break strategies, introducing the possibility of reverse association. The subjective and non-standardized nature of these measures, along with unmeasured confounders such as case complexity and operative time, may have further attenuated detectable associations. These findings emphasize the complexity of linking isolated ergonomic behaviors to cumulative pain outcomes. 11
The use of ergonomically optimized intraoperative visualization systems is another important strategy for reducing musculoskeletal strain during surgery. Surgical loupes, which are ubiquitously used in cleft surgery, are a key factor influencing surgeons’ musculoskeletal health and have repeatedly been associated with cervical loading and subsequent degenerative spinal disease.12,13 Hamdan et al emphasized that properly selected loupes may improve ergonomic posture during prolonged procedures. 7 Specifically, they recommended the use of front-mounted loupes with 2.5×, 3.5×, or 4.5× magnification, steep declination angles, clear lenses, and low-set frames. Fan et al highlighted several perceived benefits of prismatic, or deflection, loupes during simulated surgical tasks. Surgeons reported lower neck discomfort when using both low-tilt and high-tilt prismatic loupes compared with their traditional loupes, and many described the devices as improving comfort, visual function, and neck posture. Notably, most participants preferred the low-tilt prismatic loupes, citing better fit, lighter weight, image brightness, and overall usability. 14 Similarly, a controlled comparative study evaluating prismatic glasses among oral and maxillofacial surgeons reported reduced neck and back discomfort, with maintenance of the neck in a more neutral position. 15 Beyond loupe optimization, the use of the intraoperative microscope has gained increasing attention over the past several decades. 16 In palatoplasty, intraoperative microscope use has demonstrated multiple advantages, including improved surgical field visualization, as well as enhanced surgeon posture through maintenance of the neck in a neutral position, ultimately translating into improved surgical ergonomics.17,18
Ergonomic Knowledge, Training, and Resource Setting
Most respondents reported good knowledge of surgical ergonomics and recognized its value for career longevity and overall health, consistent with prior studies. 19 Despite this, fewer than one-fifth of surgeons reported prior participation in formal ergonomics training, reflecting the well-documented scarcity of structured ergonomic education within surgical curricula. Importantly, we identified a significant inverse association between prior ergonomic training and the presence of musculoskeletal pain or discomfort (ρ = -0.203; P = 0.035), aligning with findings by Cerier et al, who demonstrated meaningful reductions in pain severity among surgical residents following a dedicated ergonomics workshop. 20 Collectively, these data support the protective role of formal ergonomic education in long-term surgeon well-being and occupational sustainability.
A positive association was observed between higher resource practice settings and receipt of ergonomic training (ρ = 0.248; P = 0.010), highlighting disparities in access to educational resources. This underscores the need for targeted implementation of ergonomics training programs in resource-limited environments to ensure equitable improvements in surgeon health worldwide.
Experience and Healthcare-Seeking Behavior
As mentioned above, greater years in practice were associated with increased perceived importance of ergonomics as both a preventive and therapeutic tool; however, no association was observed between years in practice and the presence of musculoskeletal discomfort. This likely reflects the multifactorial etiology of WRMDs, involving cumulative exposure, general health status, lifestyle factors, and occupational risk behaviors.6,21 Similarly, no relationship was identified between surgical experience and prior medical consultation or formal diagnosis of a musculoskeletal disorder (ρ = 0.075; P = 0.441), consistent with prior reports suggesting that surgeons often favor self-management over professional care due to time constraints and cultural norms within demanding specialties.5,22,23 Our findings support this pattern, with high reliance on rest, massage, and over-the-counter analgesics for symptom relief, pointing toward substantial underdiagnosis of WRMDs among cleft surgeons.
Notably, among all reported anatomical pain sites, lower back pain was the only symptom consistently prompting our surgeons to seek medical consultation or formal diagnosis. Howarth et al similarly reported that craniomaxillofacial surgeons who sought medical care were more likely to report chronic or persistent lower back WRMDs, compared with other musculoskeletal complaints. 24 This suggests that lower back pain may represent a threshold symptom that overcomes prevailing barriers to healthcare-seeking behavior among surgeons.
From Awareness to Adoption: Practical Ergonomic Interventions
The above findings highlight the urgent need for prompt action to address two major gaps: persistently inadequate ergonomic awareness and the even greater disconnect between awareness and sustainable behavioral change.
To address the first gap, efforts should focus on continuing medical education and the systematic integration of ergonomics into surgical training through residency curricula, simulation-based education, and procedure-specific workshops. 20 These initiatives should train surgeons to recognize high-risk postures and understand their long-term consequences for musculoskeletal health, while also teaching preventive ergonomic strategies before, during, and after surgery, including proper equipment optimization and setup.
To address the second gap, awareness must be paired with practical implementation strategies that support the adoption of ergonomic behaviors during routine operative care. These strategies may include standardized institutional policies that establish surgeon musculoskeletal health as a core component of surgical safety culture; scheduled intraoperative micro-breaks supported by timers, alarms, or wearable reminder systems; posture self-monitoring facilitated by visual cues, peer feedback, or digital prompts; and preoperative verification of ergonomic setup, including loupe fit, monitor position, working distance, and instrument arrangement. 7 Core and cervical strengthening programs may also help support long-term prevention. Another valuable approach would be to organize regular group discussions in which senior surgeons share personal experiences with WRMDs, such as cervical or lumbar disc disease, that developed over the course of prolonged surgical careers. These discussions could also address how affected surgeons managed these conditions, including whether they required physical therapy, activity modification, procedural adjustments, or surgical intervention, particularly when these outcomes were linked to limited ergonomic education or difficulty maintaining ergonomic practices. Such peer-led reflection may help younger surgeons better appreciate the long-term consequences of inadequate ergonomic training and inconsistent adoption of preventive practices.
Ultimately, it is essential to bridge knowledge dissemination with both sustainable individual behavioral change and institutional support systems that facilitate consistent adoption of preventive practices.
Study Limitations and Future Directions
Respondents represented a select group of participants attending a single international craniofacial cleft workshop that was held in a single geographic region, which contributes to regional selection bias and limits the generalizability of the results to the broader population of cleft and craniofacial care providers. Second, the geographic distribution of respondents was skewed, potentially introducing regional bias. Additionally, most participants were affiliated with academic institutions or private practice, suggesting relatively greater access to resources and ergonomically friendly equipment; as such, the burden of ergonomic requirements may be underestimated in lower resource settings. Although all respondents had a surgical background, the overall sample size was insufficient to allow meaningful subgroup analyses by sub-specialty or other demographic variables of interest. Furthermore, two survey items addressing ergonomic visualization aids, “lightweight headlights” and “appropriate loupes,” were not accompanied by formal standardized definitions at the time of survey administration. Specifically, no weight-based threshold was provided for “lightweight headlights,” and “appropriate loupes” was intended to refer broadly to ergonomically optimized loupes, including consideration of working distance, declination angle, magnification, and individualized fit; however, the survey did not separately categorize traditional loupes, ergonomic/deflection loupes, or other loupe designs. As a result, respondents may have interpreted these items variably based on their individual experience with surgical lighting and loupe systems, potentially limiting the consistency and interpretability of responses related to these variables. Finally, medication use was assessed as a general symptom management strategy and was not further categorized by medication type, dose, frequency, or prescription status.
Collectively, these limitations underscore the need for future studies with larger, more diverse, and multidisciplinary samples across multiple geographic regions, as well as more procedure-specific workload metrics, and granular data on intraoperative ergonomic equipment use, to better characterize ergonomic challenges in cleft care. Future surveys should also assess whether surgeons use timers, reminders, peer feedback, or other cueing strategies to support posture monitoring and micro-break adherence during surgery.
Conclusion
WRMDs are highly prevalent among cleft surgeons and predominantly affect the neck and back, reflecting the sustained postural and biomechanical demands of cleft and craniofacial surgery. Although greater surgical experience is associated with increased awareness of ergonomics and more frequent use of ergonomic equipment, this awareness does not consistently translate into preventive behaviors or a reduced burden of symptoms. Our findings highlight a persistent gap between ergonomic knowledge and real-world implementation, underscoring the multifactorial and cumulative nature of WRMDs. Collectively, these results support the need for structured, accessible ergonomics education and targeted preventive strategies at both the individual and institutional levels, particularly in resource-limited settings, to promote long-term musculoskeletal health and career sustainability among cleft surgeons.
Footnotes
Ethical Considerations/ Consent to Participate
This study was conducted in accordance with established ethical research principles. Data were collected through an anonymous electronic survey of cleft surgeons, and no personally identifiable information was recorded. Participation was entirely voluntary, with participants verbally informed about the purpose of the study and their right to decline participation. The study protocol was reviewed by the Ethical Review Board of Global Smile Foundation and was classified as exempt minimal-risk research involving an anonymous survey of adult professionals. Completion and submission of the survey constituted implied informed consent to participate in the study.
ORCID iDs
Consent for Publication
Not Applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.