
Abstract
Objectives
This study examined the association between maternal pharmacological exposures and nonsyndromic craniosynostosis (NSC).
Design and Methods
In this retrospective database study, all pregnancies affected by NSC were identified in the Epic Cosmos database and matched 1:1 to control pregnancies for case-control analysis. In hypothesis-driven analysis, associations between NSC and first- or second-trimester medication exposures with prior evidence of association were estimated. In exploratory analysis, all first- and second-trimester medication exposures were compared, and those that remained significant after correction for multiple comparisons with an odds ratio >2 were retained. All significant exposures were reevaluated in sibling-controlled models to isolate within-family risk.
Patients
10,470 pregnancies affected by NSC and 10,470 control pregnancies.
Main Outcome Measure
Adjusted odds ratios (aORs) estimating the association between candidate medication exposures and NSC in case-control analysis; within-family risk of NSC in sibling-controlled analysis.
Results
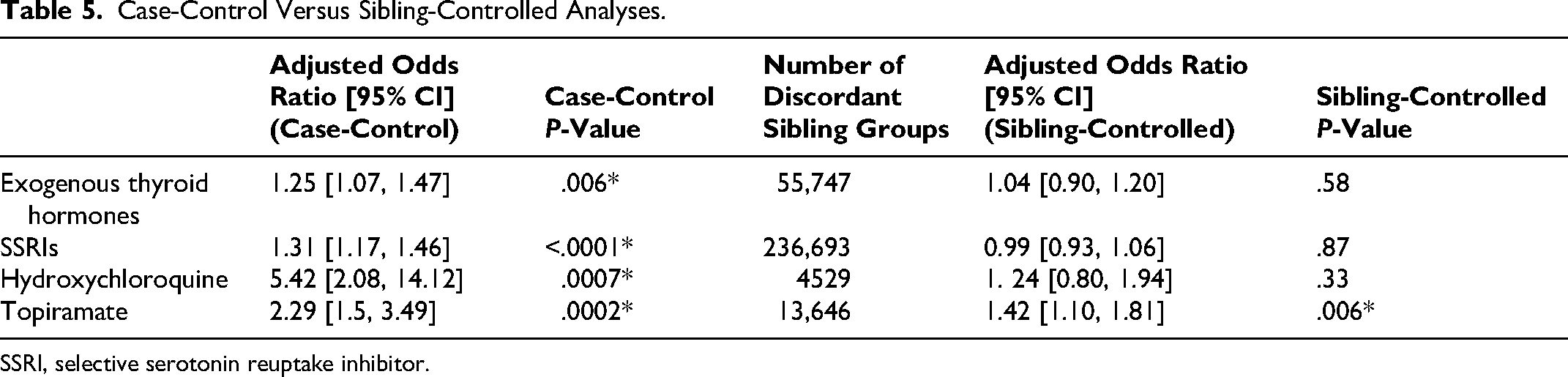
Among medications with prior evidence, exogenous thyroid hormones (aOR: 1.25 [95% CI: 1.07, 1.47]) and selective serotonin reuptake inhibitors (SSRIs) (aOR: 1.31 [95% CI: 1.17, 1.46]) were significantly associated with NSC. Exploratory analysis revealed topiramate (aOR: 2.29 [95% CI: 1.50, 3.49]) and hydroxychloroquine (aOR: 5.42 [95% CI: 2.08, 14.12]) as significant. However, in sibling-controlled analysis, only topiramate remained significantly associated with NSC (aOR: 1.42 [95% CI: 1.10, 1.81]).
Conclusions
Our findings identify topiramate as a potential teratogen for craniosynostosis. The modest association and null sibling effect for SSRIs do not support discontinuation during pregnancy. Associations with thyroid hormones suggest a complex interplay between thyroid function and suture development.
Keywords
Introduction:
Nonsyndromic craniosynostosis (NSC) involves the premature fusion of usually a single cranial suture without extracranial anomalies or syndromic features, resulting in a characteristic abnormal head shape and potential restriction of brain growth.1–3 NSC has a complex etiology involving both genetic and environmental factors, including maternal comorbidities, intrauterine constraint, and gestational exposures.4–8 In particular, maternal teratogenic exposures may precipitate craniosynostosis by disrupting suture stem cell populations and osteogenic signaling during early cranial suture formation in the first trimester.9–16 Teratogenic risk may also extend into the second trimester, with potential effects on suture homeostasis and bone development.17–19
Pharmacologic exposures are among the most actionable risk factors. Prior studies have linked sodium valproate, exogenous thyroid hormones, certain nitrosatable drugs, methotrexate, selective serotonin reuptake inhibitors (SSRIs), and clomiphene citrate to NSC.9–18,20–28 However, these studies have been limited by small sample sizes, lack of rigorously matched controls, and the assessment of individual exposures in isolation.9,11–13,17 Furthermore, no prior studies have used sibling-controlled analyses to account for shared maternal or genetic factors, which may confound observed teratogenic associations.
We therefore leveraged a large, nationally representative database to achieve the following aims: (1) reevaluate previously implicated drug exposures, (2) identify novel candidate medications associated with NSC, and (3) validate findings within sibling-controlled models to distinguish true teratogenic effects from familial or maternal confounding.
Methods
Study Design and Data Source
A retrospective, case-control study was performed utilizing the Epic Cosmos database (Verona, Wisconsin), 29 a nationwide electronic health record repository with over 300 million patients across 1800 participating hospitals in the United States. This Health Insurance Portability and Accountability Act-defined limited dataset includes demographic information, ICD-10 codes, CPT codes, and medication prescription records. This study was exempt from institutional review board approval as all data were deidentified.
Patient Selection
All pregnancies resulting in a child diagnosed with isolated, single-suture craniosynostosis (ICD-10 codes Q75.01, Q75.021, Q75.03, Q75.041) between 2015 and 2024 were extracted. Exclusion criteria included missing maternal data, patients who had a concurrent diagnosis of a genetic syndrome, or concurrent billing codes for two or more involved sutures (Figure 1). Single-suture cases without concurrent diagnosis of a genetic syndrome were considered to be nonsyndromic. Mother–child linkages were established using unique identifiers within Cosmos. Analyses were conducted at the pregnancy level, defined by the mother's unique patient identifier and the child's date of birth. Multiple gestations were included. Data collected included demographic data such as social vulnerability index (SVI), diagnosis codes for the mother and child, and medication administration history.
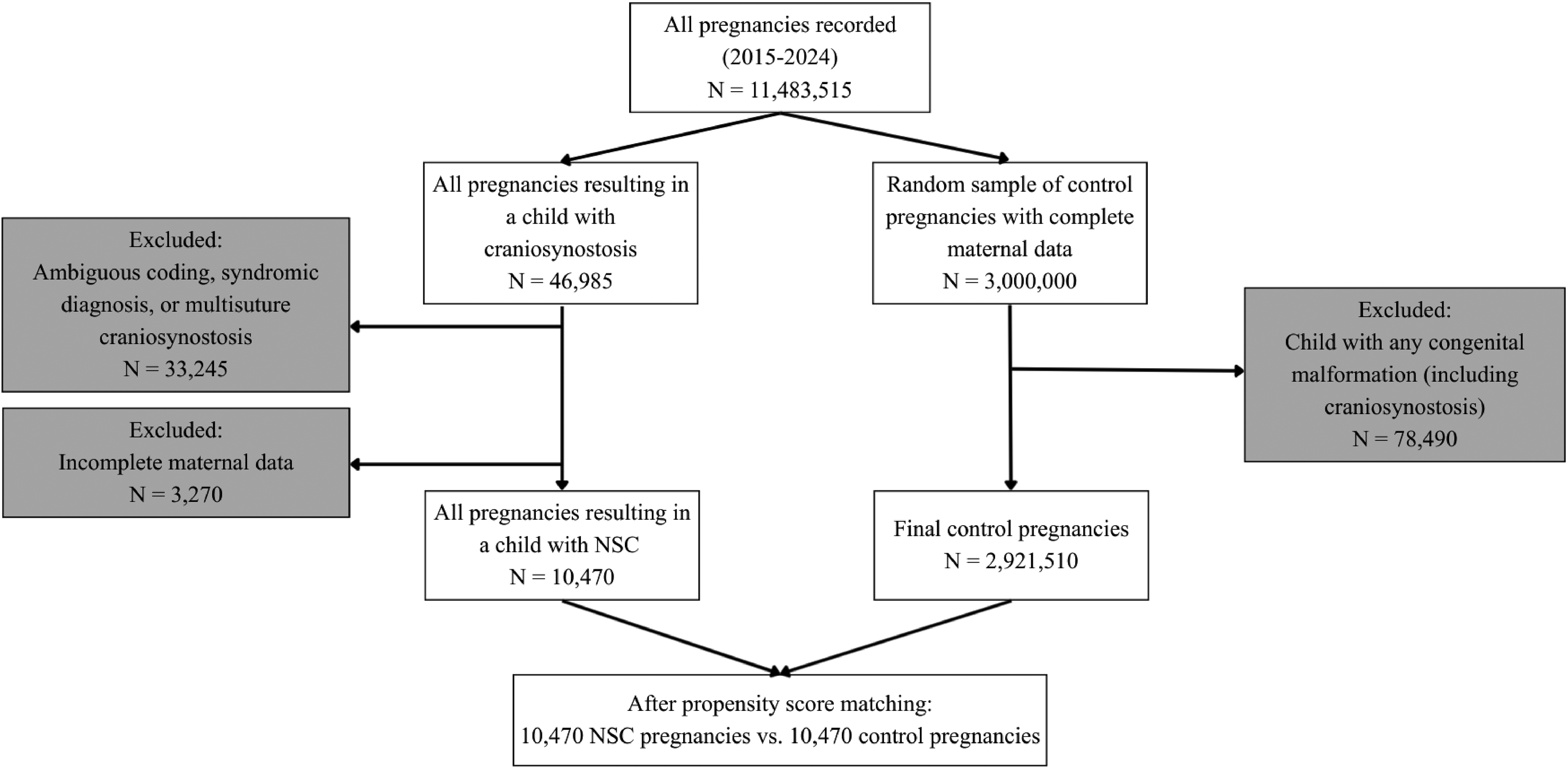
Flow chart of cases and controls.
Control Cohort
A random sample of 3 million control pregnancies was extracted from the database to use for propensity score matching. Pregnancies resulting in a child with any congenital malformation were excluded (Figure 1).
Propensity Score Matching
All affected pregnancies were matched 1:1 to a control pregnancy using propensity score nearest-neighbor matching without replacement. Controls were matched based on maternal age at birth, SVI, preexisting maternal diabetes, preexisting maternal hypertension, and plurality (singleton vs. multiple gestation). All propensity score matching was performed in R (v 4.1.2). Covariate balance between groups was confirmed by a standardized mean difference (SMD) < 0.1 for all variables.
Identification of Pharmacological Agents for Hypothesis-Driven Analysis
Pharmacological agents previously associated with craniosynostosis were identified through a nonsystematic review of PubMed and Embase using the search terms “pregnancy,” “exposed” or “exposure*,” and “craniosynostosis.” Additional human and animal studies were identified for each exposure using the name of the medication and “craniosynostosis” as search terms. Any prescription drug exposures that had a reported association with craniosynostosis in human or animal studies were included regardless of study design or strength of evidence (Table 1).
Pharmacological Exposures Previously Linked to Craniosynostosis.
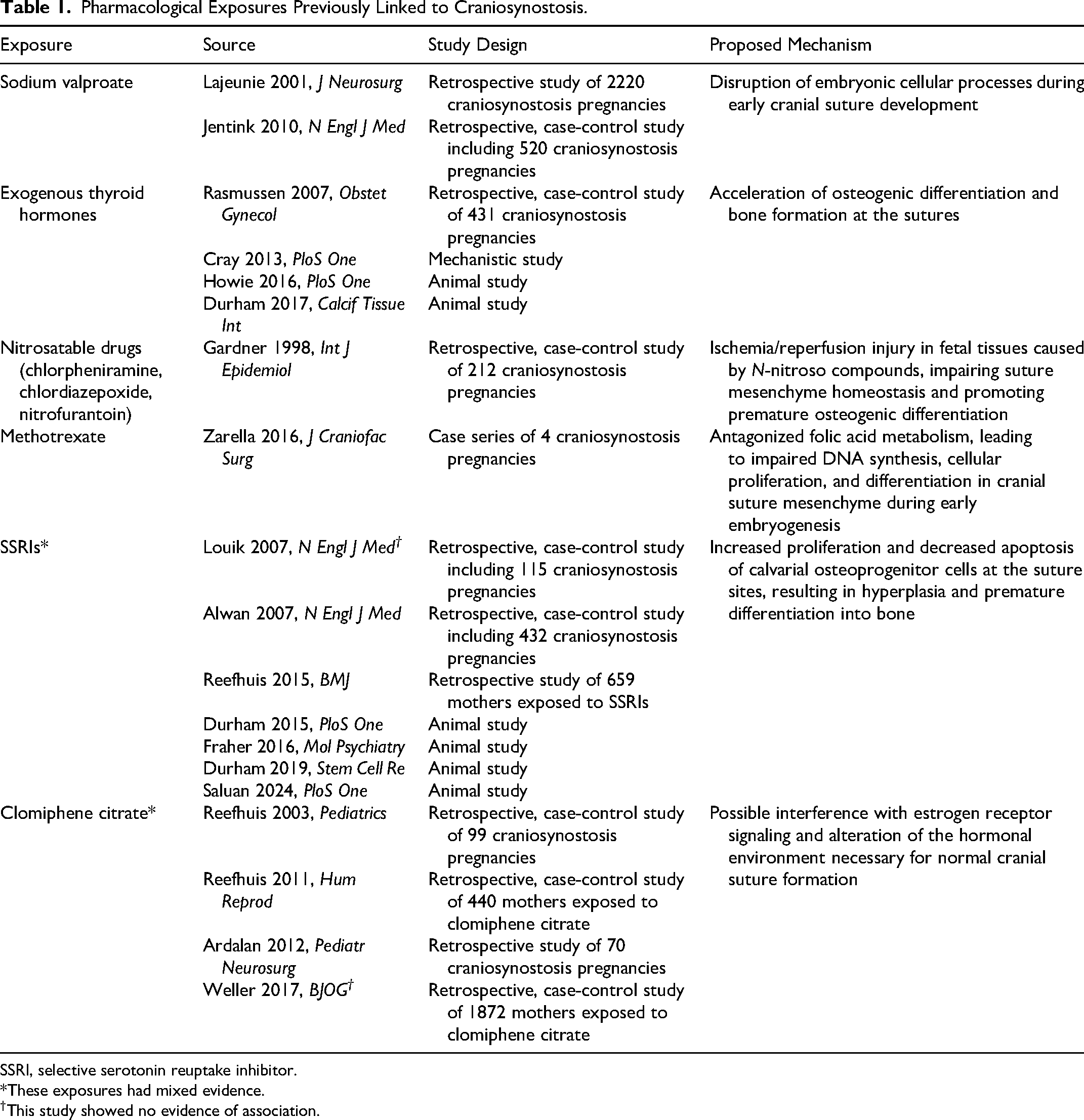
SSRI, selective serotonin reuptake inhibitor.
*These exposures had mixed evidence.
†This study showed no evidence of association.
Hypothesis-Driven Analysis
All pharmacological agents identified in the literature as previously linked to craniosynostosis were included. Rates of exposure were compared between the craniosynostosis and control cohorts. Although the timing of craniosynostosis development is complex, with hypothesized contributing processes extending from preimplantation through the postnatal period,9,30–32 most proposed teratogenic mechanisms for pharmacologic exposures involve processes occurring during the first 2 trimesters (Table 1). Thus, medication exposure was defined as the presence of a prescription that overlapped any portion of the first or second trimester, as teratogenic effects during the third trimester are minimal.33,34 For fertility medications, the exposure window was expanded to 2 months prior to conception, consistent with their proposed teratogenic mechanism. 16 Medication exposures were identified using Cosmos-specific medication groups (eg, SSRIs) and keyword searches within prescription names.
Exposure rates were compared using chi-squared tests, with Benjamini–Hochberg (BH) correction for multiple comparisons. Adjusted odds ratios (aORs) for craniosynostosis were estimated using multiple logistic regression controlling for concurrent exposure to all other included medications (craniosynostosis ∼ medication 1 + medication 2 + …). Analysis was performed in R (v 4.1.2).
Exploratory Analysis
An exploratory analysis was performed including all medications prescribed to >10 mothers in the craniosynostosis group with prescriptions spanning the first two trimesters. Exposure rates were compared using chi-squared tests, with multiple comparisons corrected for using the BH method. Only medications with a significant chi-squared test after BH correction and with an unadjusted odds ratio >2 (a common threshold for potential teratogenicity)35,36 were retained for further evaluation.
Sibling-Controlled Analysis
For each medication identified as significant in either the hypothesis-driven or exploratory analyses, sibling groups discordant for in-utero exposure were ascertained by first identifying all pregnancies in the database positive for an exposure and then identifying their sibling pregnancies. Discordant sibling groups were defined as any family group of 2 or more siblings in which at least one sibling was exposed in utero and at least one was not. Among the discordant sibling groups, those affected by craniosynostosis were then identified by ICD-10 codes. The conditional ORs for craniosynostosis within discordant sibling groups were estimated using conditional logistic regression for all significant medications, providing an estimate of the within-family difference in risk (craniosynostosis ∼ medication1 + medication2 + … + strata(family)). Analysis was performed in R (v 4.1.2).
Results
Identification of Pharmacological Agents for Hypothesis-Driven Analysis
Six medications and 2 medication groups were identified as having prior evidence of an association between in utero exposure and craniosynostosis: sodium valproate, chlorpheniramine, chlordiazepoxide, nitrofurantoin, methotrexate, clomiphene citrate, exogenous thyroid hormones, and SSRIs. Two exposures, SSRIs and clomiphene citrate, demonstrated mixed evidence in prior studies, with some studies reporting no association with craniosynostosis (Table 1).
Cohort Selection and Baseline Characteristics
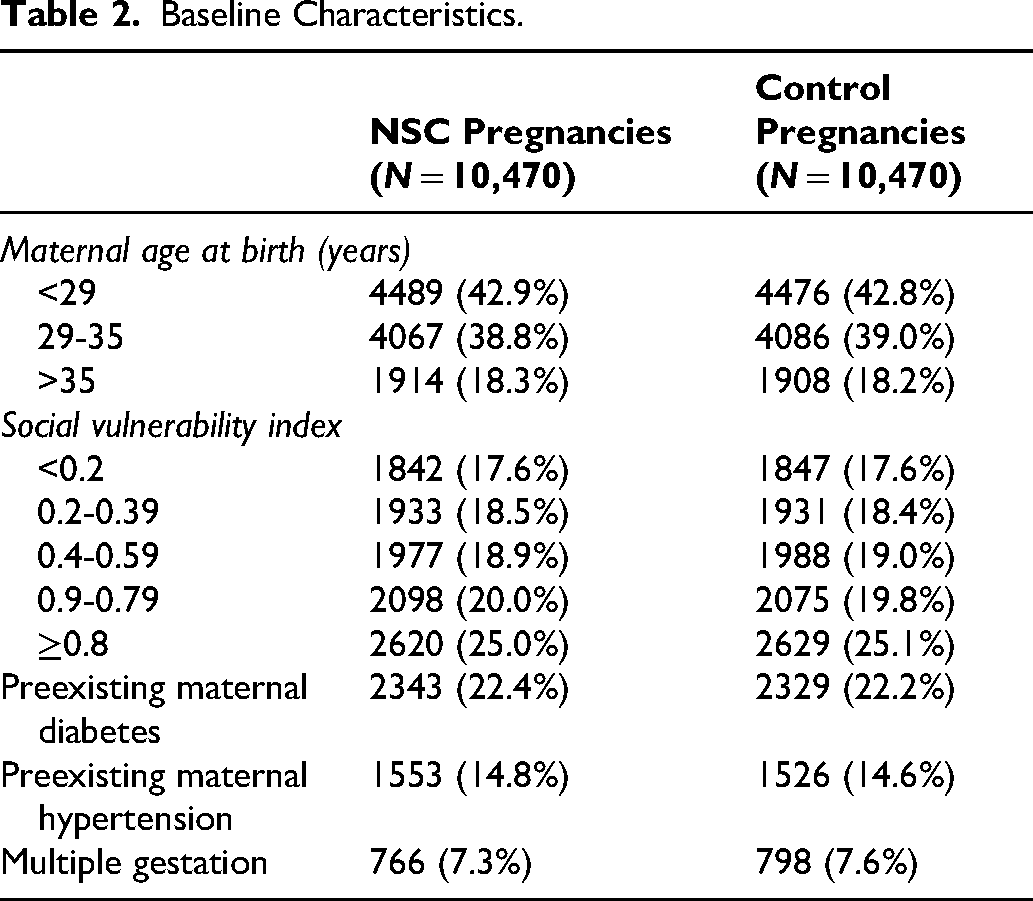
A total of 10,470 pregnancies resulting in a child with NSC were identified, with a total of 10,470 matched control pregnancies. Rates of maternal diabetes, hypertension, and multiple gestation in the craniosynostosis cohort were 22.4%, 14.8%, and 7.3%, respectively. The cohorts were well balanced across all matching covariates. After propensity score matching, all variables achieved an SMD of <0.1 (Table 2; Figure 1). The average age of the initial craniosynostosis diagnosis was 7.08 months (standard deviation: 10.08 months).
Baseline Characteristics.
Hypothesis-Driven Analysis
Among previously implicated medications, exposure to exogenous thyroid hormones and SSRIs was significantly more frequent in the craniosynostosis cohort. In multivariable regression, the aOR was 1.25 [95% CI: 1.07, 1.47] (P = .006) for exogenous thyroid hormones and 1.31 [95% CI: 1.17, 1.46] (P < .0001) for SSRIs (Table 3). Sertraline, escitalopram, fluoxetine, and citalopram accounted for >98% of SSRI prescriptions in both groups, with similar distributions between cases and controls.
Results of Hypothesis-Driven Analysis (Rates of Exposure and Adjusted Odds Ratios).
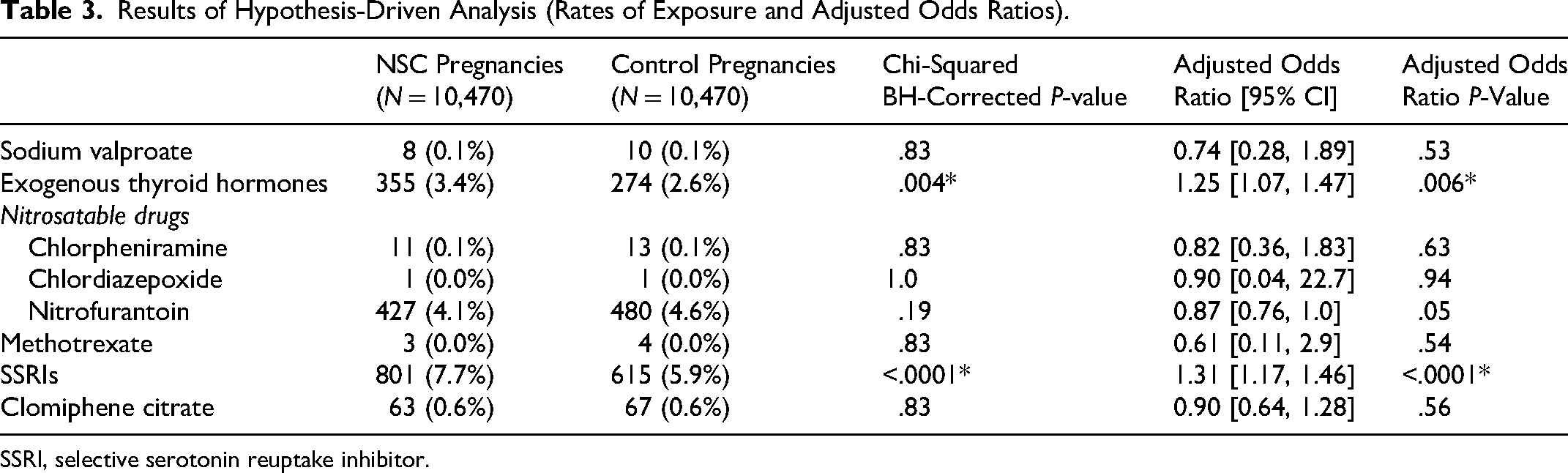
SSRI, selective serotonin reuptake inhibitor.
Exploratory Analysis
In an exploratory analysis comparing all first and second trimester exposures, hydroxychloroquine and topiramate demonstrated significantly higher rates of exposure in the craniosynostosis group. The unadjusted odds ratio was 5.41 [95% CI: 2.08, 14.06] (P = .0001) for hydroxychloroquine and 2.23 [95% CI: 1.47, 3.38] (P = .0001) for topiramate (Table 4).
Results of Exploratory Analysis (Rates of Exposure and Odds Ratios).

Sibling-Controlled Analysis
All medications that were significant in case-control analysis (both hypothesis-driven and exploratory) were included in sibling-controlled analysis. There were 55,747 discordant sibling groups for exogenous thyroid hormones, 236,693 for SSRIs, 4529 for hydroxychloroquine, and 13,646 for topiramate. Only topiramate remained significant in sibling-controlled analysis (aOR 1.42 [95% CI: 1.10, 1.81], P = .006) (Table 5).
Case-Control Versus Sibling-Controlled Analyses.
SSRI, selective serotonin reuptake inhibitor.
Discussion
We present a large national, multiinstitutional study examining maternal prescription drug exposures associated with NSC, from which we identify topiramate as a previously unrecognized potential teratogen for craniosynostosis. Among previously implicated medications, SSRIs and exogenous thyroid hormones demonstrated significant associations in case-control analysis, though these associations were not observed in sibling-controlled models. Overall, our findings support limiting topiramate use during pregnancy when clinically feasible, while providing no evidence to warrant restriction of SSRIs. Additionally, these results underscore the complex interplay between maternal thyroid disease, thyroid hormone supplementation, and craniosynostosis risk.
Topiramate, used primarily for epilepsy and migraine prophylaxis, demonstrated a significant association with NSC that persisted in sibling-controlled analysis. Although previously associated with orofacial clefts, 37 topiramate has not been linked to craniosynostosis before. Mechanistic studies show that topiramate upregulates TGF-β1 and SOX9, key regulators of craniofacial morphogenesis. 38 TGF-β1 plays a pivotal role in cranial suture formation and fusion, with upregulation correlating with suture closure and craniosynostosis.39–42 Thus, these molecular pathways offer a plausible mechanism for our findings. Taken together, these findings suggest that topiramate may be associated with multiple adverse craniofacial developmental outcomes, including an increased likelihood of craniosynostosis in addition to its established association with cleft palate. Accordingly, topiramate should be prescribed during pregnancy only when the potential maternal benefit outweighs fetal risk, and patients should receive appropriate counseling.
In case-control analysis, SSRIs showed a significant but small association with craniosynostosis (aOR: 1.31 [95% CI: 1.17, 1.46]), but this association did not remain significant in sibling-controlled analysis. Prior animal studies have shown that SSRIs can induce premature suture fusion and deplete calvarial stem cells in murine models.17,23 Earlier epidemiological studies also reported an elevated risk for NSC (odds ratios ranged from 1.9–2.5) with maternal exposure to SSRIs, but these studies were limited by small sample sizes and did not control for maternal hypothyroidism, a known risk factor for craniosynostosis which is also associated with depression.14,15,43 After adjustment for hypothyroidism (using exogenous thyroid hormone supplementation as a proxy) and other covariates, the association between SSRI exposure and NSC remained significant but attenuated (aOR < 2). This suggests that confounding factors may have led to an overestimation of earlier risk assessment, although an independent effect of SSRIs cannot be excluded. In general, an odds ratio exceeding 2 is regarded as a common threshold suggestive of a significant teratogenic effect,35,44–46 and our observed association does not meet this criterion. Moreover, our null findings in sibling-controlled analysis suggest that a portion of the observed risk may stem from unmeasured maternal-level confounders. Taken together, our results do not support a major teratogenic effect of SSRIs on craniosynostosis and require further confirmation by other studies.
Exogenous thyroid hormones showed a modest association with craniosynostosis (aOR: 1.25 [95% CI: 1.07, 1.47]) in case-control analysis, which was not significant in sibling-controlled analysis. Animal studies demonstrate that excess thyroid hormones accelerate osteogenic differentiation and suture closure, supporting a potential biological mechanism.20,23,47 Additionally, transcriptomic and gene expression data from human osteoblast-like cells suggest a link between thyroid hormone signaling and growth factor pathways.48,49 Prior epidemiological studies have also linked maternal thyroid disease and thyroid hormone replacement therapy to craniosynostosis, but did not distinguish between hyperthyroidism and hypothyroidism treated with replacement hormones. Our study specifically examined exogenous thyroid hormones used for hypothyroidism. Overtreatment of hypothyroidism, occurring in up to 30% of cases,50,51 may contribute to the modest risk we observed in case-control analysis. The null result in sibling-controlled analysis further suggests potential confounding by maternal-level factors. Overall, our findings indicate a nuanced interplay between maternal thyroid function, treatment, and craniosynostosis risk. Prospective studies incorporating serum thyroid indices will be essential to determine whether risk stems from hormonal excess, genetic predisposition, autoimmune milieu, or the connection between maternal thyroid abnormalities and fetal thyroid abnormalities (such as the association between fetal hyperthyroidism and maternal hypothyroidism). 52 Furthermore, future studies should investigate differences in risk associated with maternal hypothyroidism treated with replacement hormone, maternal hyperthyroidism, and neonatal hyperthyroidism.
Several medications previously associated with craniosynostosis were not significant in our analyses. Clomiphene citrate is particularly notable given extensive prior investigation.9,10,16,26–28 Prior evidence linking clomiphene citrate to craniosynostosis is mixed: earlier studies report an association, whereas later studies do not. Earlier studies were limited by small sample sizes and lacked control for confounding factors such as twin pregnancy, which is associated with induced ovulation and also separately increases craniosynostosis risk.16,26,27,53–55 Our findings align with later studies showing no evidence of association. 28 Additionally, several medications in this study such as sodium valproate and methotrexate had exposure rates of <0.1%, precluding meaningful inference about their relationship to craniosynostosis. Since medications like sodium valproate and methotrexate are well-established teratogens for a broad range of birth defects,10,56 these limited data likely reflect contemporary prescribing patterns that limit the use of these medications during pregnancy. 57
This study's strengths include its cohort size, stringent propensity-matched controls, and use of sibling comparisons, which at least partially account for potential unmeasured maternal and familial confounders. The primary limitation is reliance on prescription records which provide only an approximation of actual medication use during pregnancy, as adherence to prescribed medications can vary widely and dose information is not available. Additionally, use of ICD-10 codes to identify single-suture cases may misclassify some syndromic patients as nonsyndromic, as complex syndromes can present with isolated, single-suture craniosynostosis. For example, approximately 10 to 17% of unicoronal craniosynostosis cases are attributable to Muenke syndrome (caused by a mutation in FGFR3 P250R). 58 Additionally, sibling-controlled analyses are inherently biased toward the null hypothesis when assessing associations between maternal exposures and offspring outcomes, largely due to their greater susceptibility to measurement error. Random misclassification of exposure status disproportionately affects sibling comparisons, which depend on exposure discordance between siblings.59–61 Consequently, positive findings in case-control analyses accompanied by null findings in sibling-controlled analyses should be interpreted as potentially reflecting confounding by maternal-level factors, rather than definitive evidence of no independent risk. Additionally, large databases are susceptible to systematic bias. The higher incidence of craniosynostosis observed in this study relative to population-level estimates 62 may reflect informative presence bias, in which individuals with symptoms or risk factors are more likely to seek care and be captured in healthcare databases.63,64 This discrepancy may also reflect admission-rate bias, in which databases including hospitals overrepresent patients with more severe disease or comorbidities. 65 However, because controls were selected using stringent exclusion criteria, these biases are unlikely to meaningfully influence case-control comparisons, which form the basis of this study. Finally, this analysis did not stratify results by suture due to power limitations in the context of modest effect sizes and rarity of exposures. Suture-specific analysis represents an important direction for future research given that premature fusion of different sutures may involve distinct signaling pathways and cellular mechanisms.66,67
This study examined maternal pharmacological exposures associated with craniosynostosis, incorporating both case-control and sibling-controlled analyses. We observed moderate associations for exogenous thyroid hormones and SSRIs in case-control analyses, but neither remained significant after within-family adjustment, suggesting potential confounding by shared maternal or familial factors. These findings do not support a major teratogenic effect of either SSRIs or exogenous thyroid hormones on craniosynostosis. In contrast, topiramate exposure remained significantly associated with craniosynostosis across analytic frameworks, identifying a novel pharmacologic signal with biologic plausibility. While causality cannot be established due to retrospective design, the consistency and magnitude of the topiramate association warrant further mechanistic and prospective investigation. Furthermore, it reinforces the need for careful risk–benefit counseling when prescribing this medication during pregnancy.
Footnotes
Ethical Statement
All study analyses were conducted in accordance with the ethical standards of the institutional and national research committees. This study utilized deidentified data and as such was exempt by the institutional review board (IRB). The authors affirm that this work is original and has not been previously published or submitted elsewhere. The authors confirm that all data are accurate, original, and have not been manipulated. Any potential conflicts of interest or funding sources have been fully disclosed. Authorship accurately reflects all individuals who contributed to the study, and all authors have reviewed and approved the final manuscript.
Consent to Participate
This is an IRB-exempt retrospective study utilizing only de-identified data and patient consent was not required.
Consent for Publication
Not applicable. No identifiable individual data, images, or videos are included in this manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.