
Abstract
Introduction
Orofacial clefts represent one of the most prevalent congenital malformations, manifesting either in isolation or as components of syndromic conditions. 1 Beyond its impact on facial esthetics, orofacial cleft also affects the jaw and development of the teeth, posing significant challenges to oral health.
Although the prevalence of dental caries has shown a declining trend among children in both developed and developing countries, a contrasting pattern is observed in individuals with clefts.2,3 This may be attributed to the difficulty in maintaining adequate oral hygiene, stemming from a combination of anatomical and dental anomalies, lack of awareness, repeated surgical interventions, and orthodontic treatments commonly associated with the condition. 4 These factors can disrupt the local microenvironment, alter the salivary properties and microbial balance, and promote colonization by atypical microbial strains thereby increasing the risk of dental caries and periodontal diseases compared to unaffected peers.5–7
Despite the significant oral health concerns associated with orofacial clefts, dental care is often overlooked by both patients and their parents, who tend to prioritize esthetics, surgical interventions, speech development, and psychological well-being.8–10 Ironically, maintaining good oral health is essential to the success of these very outcomes.
While the oral health of children in India has received some attention through various public health initiatives, large-scale epidemiologic studies focusing specifically on children with CLP are lacking. 11 Although similar efforts have been undertaken internationally, India still lacks comprehensive national data on the oral health needs of this vulnerable population.12–14 Recognizing this gap, the Cleft Care India Study (CCIS) adopted a comprehensive approach to evaluating the standard of care of individuals with non-syndromic UCLP at 5, 12, and 20 years old. While previous papers from CCIS focused on skeletal, dental, and nasolabial outcomes, the present work examines the oral health status of non-syndromic UCLP patients across the participating centers. 15
The objective of this study is to prospectively evaluate the oral health care needs of individuals with unilateral cleft lip and palate by documenting their past and present dental histories and current treatment status, thereby facilitating the development of tailored care strategies for this high-risk population.
Methods
This study was approved by the Jamia Millia Islamia University Research Ethics Committee (approval no. 18/3/ 279/JMI/IEC/2020) on March 18, 2020. All participants provided written informed consent prior to enrollment in the study. This research was conducted ethically in accordance with the Declaration of Helsinki.
Between December 2019 and June 2023, 14 centers from various regions of the country participated in the CCIS. Each center contributed data from consecutive non-syndromic UCLP patients aged 5, 12, and 20 years in the given time frame. Patients who had learning difficulties that prevent them from cooperating for data collection, and those who failed to provide consent, were excluded. Data were collected using a validated form and a uniform protocol and submitted through a dedicated web portal (www.ccis.org.in). The collected information included the patient's dental care history and oral health status. To ensure consistency, data collection was conducted by designated personnel who were trained for the indices and calibrated prior to collecting data. A pilot data collected by the data collection personnel from each center was evaluated by the Data Coordinating Centre (DCC) for quality assessment. Further details on the methodology are available in the first part of the paper.
The data collected included information on dental care history from parents in 5 and 12 year olds and both parents and patients in 20 year olds, such as attendance at the dentist, treatments received, dietary advice provided, and oral hygiene aids used. A clinical examination was conducted to assess oral health status, and all assessments were performed by a calibrated dentist to ensure consistency. Caries experience and treatment history were recorded using the Decayed, Missing, and Filled Teeth (dmft/DMFTindex), while developmental defects of enamel were assessed using the Developmental Defects of Enamel index. Oral hygiene status, assessed based on the amount of plaque on the labial and lingual aspect of lower incisors, was categorized as good (< no visible plaque), fair (visible plaque less than 1/3rd tooth surface), or poor (visible plaque more than 1/3rd tooth surface). As the lower incisors are easily accessible for standardized examination and are considered more representative of the general level of oral hygiene in patients with cleft lip and palate than upper incisors, they were taken as reference teeth for oral hygiene assessment. 13 Occlusal parameters were assessed during clinical examination, including the presence or absence of mandibular displacement on closure (forward or lateral). Data were reported descriptively as means and percentages. The CCIS data was collected using a standardized data collection protocol across all participating centers. Each center was assigned a unique center code, and none of the records included the names of the centers. Prior to initiation of data collection, designated clinicians from each center received training regarding the study methodology, diagnostic criteria, definitions of variables, and recording procedures in a workshop and as and when required. One experienced dental clinician from each center was trained to collect oral health data. Pilot data collected by each center were reviewed by the central coordinating team to assess adherence to the study protocol and ensure consistency in data recording. The details of the calibration process can be found in Part 1 of the series. 15 As this was a part of routine work for dentists, a formal reliability assessment was not performed.
Results
Oral health data were collected from n = 76 5 year olds, n = 154 12 year olds, and n = 66 20 year olds across the 14 participating centers.
Analysis of dental attendance revealed that 35% (n = 27) of 5 year olds and 41% (n = 63) of 12 year olds and 29% (n = 19) had never visited a dentist. Additionally, nearly 6% of 20 year olds were unsure whether they had ever visited a dentist. Across all age groups, secondary or tertiary care hospitals were the preferred providers for routine dental care, followed by primary care general dental practitioners. Despite 35% of 5 year olds reporting a history of tooth pain, 70% had never been seen by a pediatric dentist, and 20% were currently receiving some form of dental treatment. Moreover, more than half of the participants across all age groups had never received dietary counseling. The majority reported using a toothbrush and fluoridated toothpaste for daily oral hygiene. However, approximately 5% of 5 year olds did not use either a toothbrush or toothpaste (Table 1).
Dental Health History in Patients of Different Age Groups.
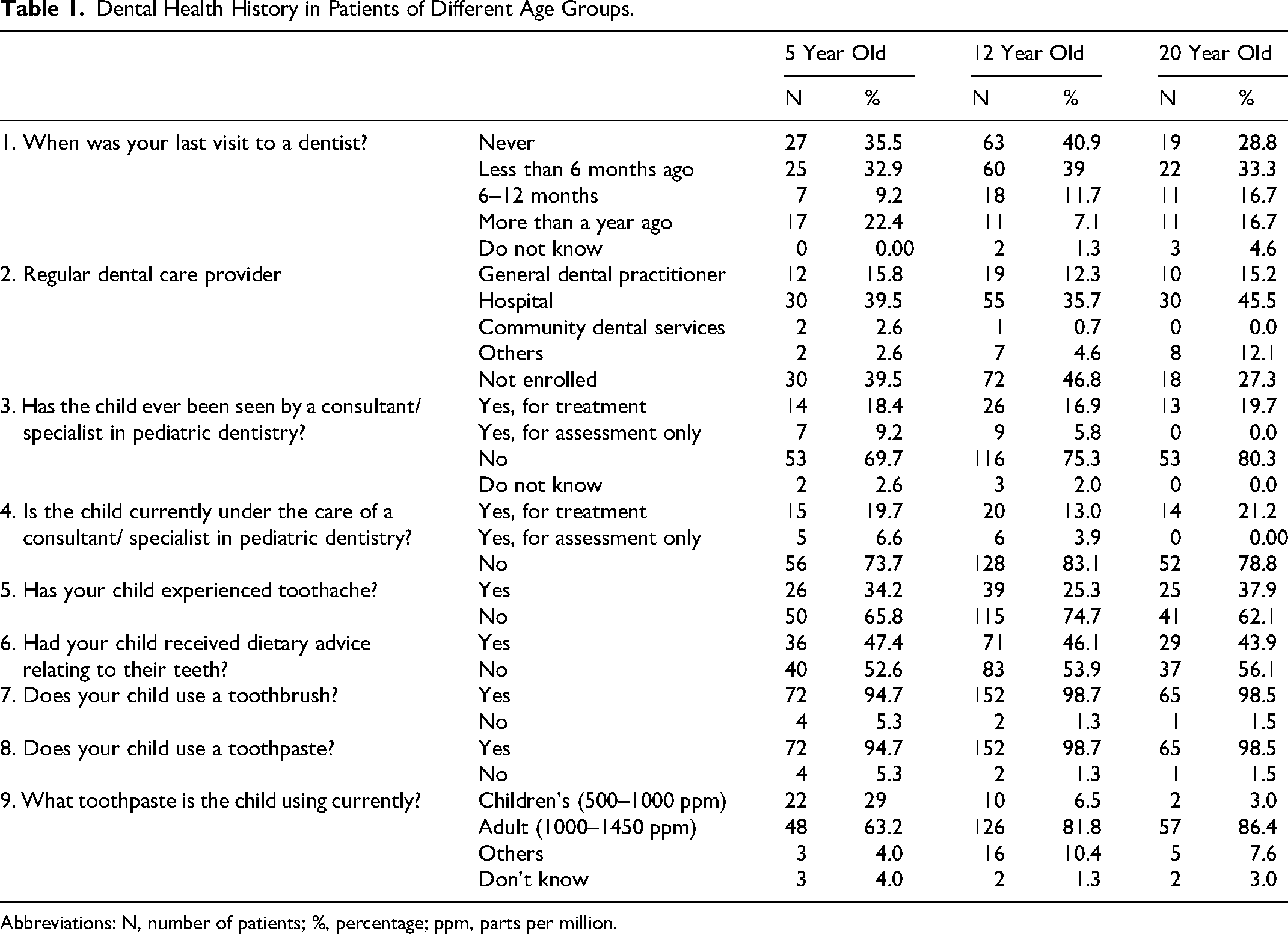
Abbreviations: N, number of patients; %, percentage; ppm, parts per million.
Most patients across all 3 age groups did not exhibit mandibular displacement on closure. However, 12.1-18.8% demonstrated either forward or lateral displacement on biting into intercuspation. Enamel hypoplasia was most prevalent among 5 year olds (31.6%; n = 33), followed by 20 year olds (27.3%; n = 24) and 12 year olds (21.4%; n = 18). Hypodontia was observed in over half of the 20 year olds (51.5%), in 39% of 12 year olds, and in 23.7% of 5 year olds. Additionally, between 40.9% and 50.0% of patients across all age groups required some form of dental treatment (Table 2).
Current Dental Status in Different Age Groups.
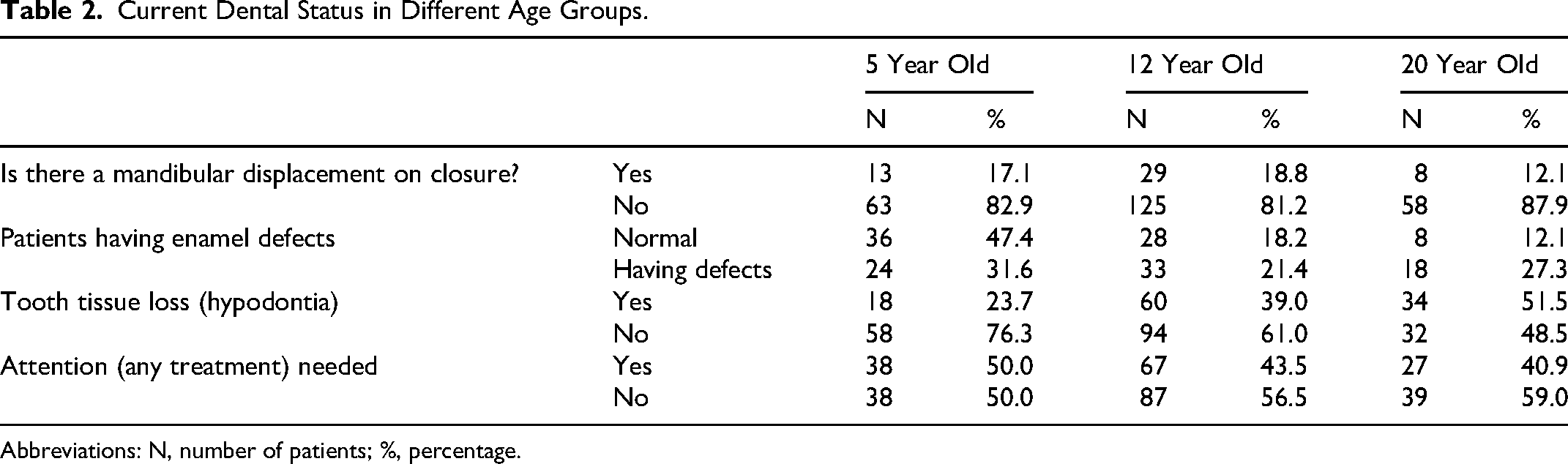
Abbreviations: N, number of patients; %, percentage.
There was considerable variation in caries experience across age groups, with 5 year olds showing the highest mean dmft/DMFT score (5.5 ± 14.9), followed by 12 year olds (3.4 ± 6.1) and 20 year olds (3.0 ± 3.9). More importantly, none of the participants was free of caries with a score 0 marked across all age groups. Regarding oral hygiene status, 47%, 60%, and 76% of 5, 12, and 20 year olds, respectively, had visible deposits on tooth surfaces (Table 3).
Comparison with Other Studies.
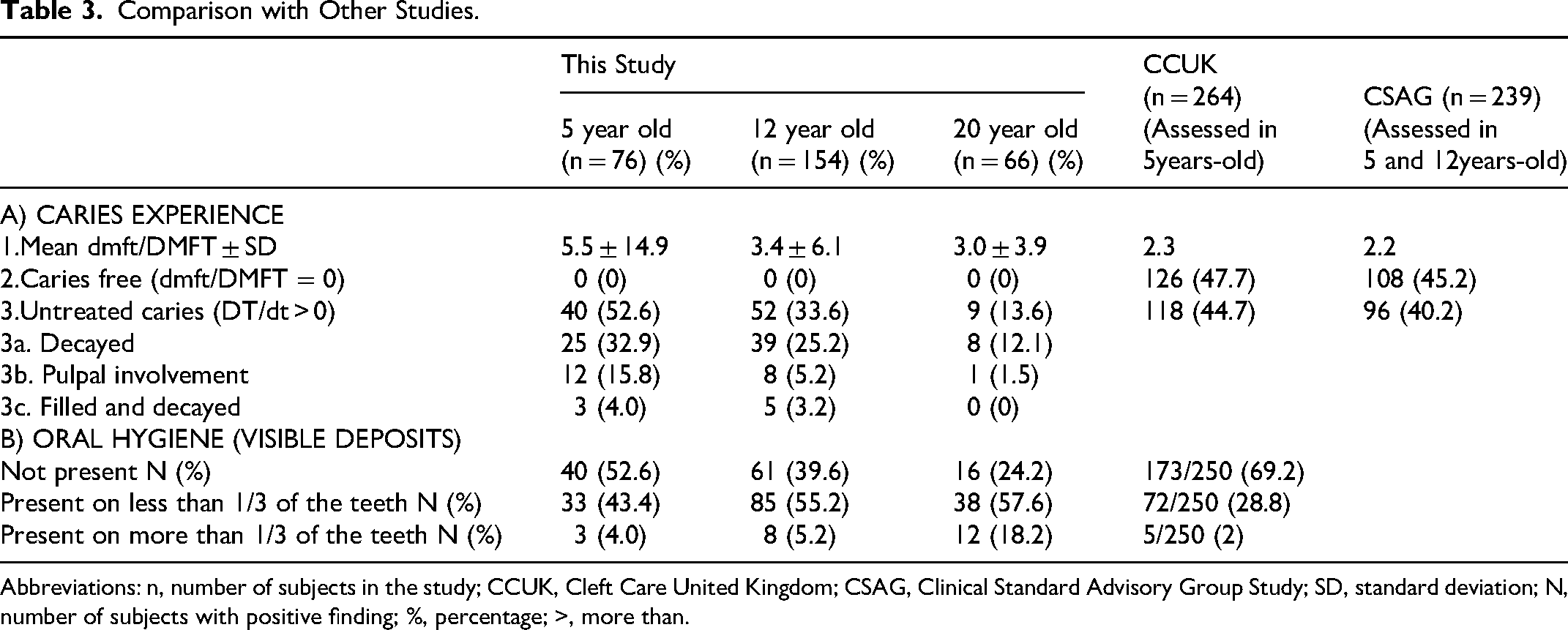
Abbreviations: n, number of subjects in the study; CCUK, Cleft Care United Kingdom; CSAG, Clinical Standard Advisory Group Study; SD, standard deviation; N, number of subjects with positive finding; %, percentage; >, more than.
Discussion
The results of the study showed that 35% (n = 27) of 5 year olds and 41% (n = 63) of 12 year olds and 29% (n = 19) had never visited a dentist. Between 70% and 80% of the population studied had never seen a pediatric dentist. While the majority of them use fluoridated tooth paste, 5% of 5 year olds do not use a tooth paste or a toothbrush. The dmft/DMFT scores were highest for 5 year olds (5.5 ± 14.9), followed by 12 year olds (3.4 ± 6.1) and 20 year olds (3.0 ± 3.9). More importantly, none of the participants was free of caries with a score 0 across all age groups. Around 47% of 5 year olds, 60% of 12 year olds, and 76% of 20 year olds had visible deposits on tooth surfaces.
Oral health remains an integral yet often under-addressed aspect of comprehensive cleft care. In individuals with UCLP, unique anatomical, developmental, and behavioral challenges, compounded by multiple surgical interventions, complicate both the maintenance and delivery of oral hygiene. 8 While surgical, orthodontic, and speech outcomes have long dominated the focus of cleft management, the present findings highlight the need to elevate oral health as a parallel priority. Interpreting these findings within the broader context of cleft care delivery offers an opportunity to identify the existing gaps and may guide improvements in clinical practice.
The high caries burden observed in this study, with mean dmft/DMFT scores exceeding 3 across all age groups, reflects the magnitude of unmet oral health needs in the CLP population. Although nearly one-third of patients across all age groups in this study had visited a dentist within the past 6 months, at least 40% still required dental treatment. Moreover, nearly 3-quarters of patients were either not receiving care, had never consulted a dentist, or were not enrolled with any regular dental care provider. Similar observations have been reported previously, where many cleft patients were found to be unregistered with dental practitioners or faced challenges in accessing dental services.10,14,16 These findings highlight the rapid progression of dental caries in this high-risk population, compounded by the lack of continuous care, and challenges in seeking these facilities. 5
While a high prevalence of dental caries in individuals with CLP has been consistently reported in the literature, the mean values observed in our study are notably higher than those previously documented. For example, the CCUK study showed a dmft score of 2 for 5 year olds and 48% of their children had a score of 0 for dmft. Although it can be argued that, these lower values in earlier studies may be partly due to the use of mean scores, which are susceptible to skew from extreme values and may not accurately capture the full range of caries experience, the difference from the present study is particularly worrying. Additional variations in reported prevalence could stem from differences in caries detection methods, the specific age groups studied, dietary patterns, and the impact of prior surgical or orthodontic interventions, which may confound the clinical presentation. 17 The present study attempted to use similar measurement tools used in the CCUK study to allow for comparison of the data.
The results of the present study are in contrast to the CCUK for caries prevalence.13,14,18,19 This may be attributed to differences in the availability and integration of pediatric dental services within cleft protocols. In the UK, such services are routinely incorporated into cleft care and supported by the national health infrastructure, facilitating early and consistent dental interventions, systems that remain unevenly implemented in India.20,21 However, the UK's cleft care model was fragmented and inconsistent prior to the Clinical Standards Advisory Group (CSAG) review. The CSAG report catalyzed a systemic transformation by recommending clinical audits, centralization of services to high-volume centers, structured training for cleft care providers, and the establishment of a national cleft registry. 22 These evidence-based reforms were supported by the government and ultimately led to the standardization and improved quality of cleft care, including dental services within the National Health Service. A similar national initiative in India, built around quality audits, registry development, and multidisciplinary training, could help bridge the current gaps in cleft care delivery. By conducting quality audits, improving data collection, investing in specialist training, and integrating pediatric dental care into multidisciplinary teams, India can work toward a more unified, accessible, and preventive-focused cleft care model.
Variations in health-seeking behavior, caregiver awareness, and the perceived importance of dental care may also influence the oral health outcomes. Geographic disparities, financial limitations, and the uneven distribution of comprehensive multidisciplinary cleft centers across India may further hinder timely access to dental services for many patients. While most patients reported using a toothbrush and fluoridated toothpaste, a small proportion continued to rely on less effective practices. This points to the need for ongoing emphasis on appropriate oral hygiene techniques, including consistent use of fluoridated toothpaste, supplementary hygiene aids, and specialized care tailored to this high-risk group. A child's oral hygiene habits are closely linked to parental education, particularly that of mothers, who typically serve as the primary caregivers. 9 Therefore, sustained efforts to counsel and educate parents, especially mothers about the importance of oral hygiene, are crucial, especially for children with CLP, to reinforce proper habits and address persistent misconceptions that may hinder oral health outcomes. 23
The results of this study underscore the pressing need to integrate pediatric dentistry into multidisciplinary cleft care teams. Only 1 of the 14 centers had specialist pediatric dentists within the unit; rest of the centers referred patients for further treatment. Additionally, at the time of data collection, none of the centers provided free care for patients requiring treatment from pediatric dentists. Integration of specialist care would help ensure that oral health needs are addressed systematically, even when families primarily seek care for surgical or orthodontic concerns and may inadvertently overlook other dental issues. Moreover, the involvement of a pediatric dentist as opposed to a general dental practitioner may increase parental willingness to engage with oral health services, as they may perceive the care to be more specialized and child centered.10,16 The present audit primarily represents centers supported by non-governmental organizations (13 of 14), including Smile Train, Akila Bharatha Mahila Seva Samaja (ABMSS), and Operation Smile, with 1 center supported by public funds (Government of India). This distribution reflects the pivotal role played by NGOs in delivering cleft care services across the country. Encouragingly, organizations such as Smile Train have recently recognized the importance of integrating specialist pediatric dental and oral health expertise into cleft care and have initiated pilot programs to incorporate oral health interventions within comprehensive care pathways in India. The findings of this audit underscore a clear and pressing need to expand and standardize these services across centers, highlighting oral health as an essential yet currently underdeveloped component of cleft care in India.
Although the demand for oral healthcare is high, financial barriers often deter families from seeking care. 24 The Smile Train Organisation's recent initiative the Smile Train Oral Health through Prevention program emphasizes prevention methods that are cost effective and practical in real-world setting.24,25 Furthermore, high-quality clinical practice guidelines should be framed that multidisciplinary healthcare providers can universally apply to improve oral health outcomes in children and adolescents with cleft conditions. 26 The findings of the present study further highlight the critical need for such initiatives, particularly in the Indian context, where the burden of oral disease remains disproportionately high amidst a severe shortage of trained dental professionals and specialist services. Strengthening specialist-driven, multidisciplinary oral health care, integrating pediatric dentistry, would help improve long-term outcomes and enhance the overall quality of life for affected individuals
The success of such interventions, however, is currently limited by the lack of comprehensive national data. The CCIS represents a critical step toward bridging this gap, and further multicentric, large-scale investigations are essential to develop evidence-based, preventive oral health protocols for cleft populations in India. Future efforts must continue to build on this foundation through collaborative, evidence-based strategies aimed at integrating pediatric dental care within the broader framework of cleft management.
Limitations of the Study
This study has certain limitations that should be considered while interpreting the findings. As a multicentric cross-sectional audit, the study did not include a formal a priori sample size calculation, and the sample consisted of a convenience sample of eligible patients from participating centers, which may limit the generalizability of the results. The participating centers were not uniformly comprehensive cleft care centers, and variations in infrastructure, expertise, and patient load across centers may have influenced the findings. Additionally, the cross-sectional design does not allow assessment of longitudinal changes or causal relationships. Although efforts were made to standardize data collection through training and calibration, inter-examiner variability cannot be completely excluded. Furthermore, oral hygiene assessment was based on a simplified clinical measure rather than full-mouth indices, which, while practical for large-scale studies, may not capture the complete oral hygiene status.
Conclusion
This study, as part of the CCIS, highlights the substantial and persistent burden of dental disease among individuals with non-syndromic unilateral cleft lip and palate across different age groups. The findings underscore significant gaps in access to dental care and preventive services in this high-risk population. There is a critical need to strengthen oral health awareness, improve access to pediatric dental services, and integrate preventive and therapeutic dental care within multidisciplinary cleft management protocols to enhance long-term outcomes.
Footnotes
Acknowledgements
We thank Smile Train India for their extensive support with the study. We thank Ms Mamta Carol for supporting us during the development stage. We would also like to thank Akila Bharatha Mahila Seva Samaja (ABMSS) for their support with the study. We are extremely thankful to the Government of India for their financial support.
ORCID iDs
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the Scheme for Promotion of Academic and Research Collaboration (SPARC), Government of India and UK India Education and Research Initiative (UKIERI), United Kingdom (grant No: P1025).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Grant Number
SPARC project No: P1025.