
Abstract
Objective
To compare maxillary bone structure between right- and left-sided unilateral cleft lip and palate (UCLP), quantify cleft vs. non-cleft asymmetry, and determine whether the non-cleft side differs from healthy controls.
Design
Retrospective cross-sectional cohort study.
Setting
University hospital, Department of Oral and Dentomaxillofacial Radiology.
Patients, Participants
Fifty UCLP (25 right, 25 left; mean age 14.8 ± 5.1 years) and 50 controls (16.5 ± 4.6 years). Power calculation indicated n = 28/group sufficient.
Interventions
Cortical thickness measured on CBCT at 4-12 mm depth across 6 interradicular regions. Trabecular architecture assessed by fractal dimension (FD) (BoneJ/Fiji).
Main Outcome Measures
Cortical thickness and FD differences between right-/left-UCLP, cleft vs. non-cleft sides, non-cleft vs. controls.
Results
No differences between right- and left-UCLP cleft sides (P > 0.05). Cleft side thickness was 0.05-0.07 mm less than non-cleft side in anterior regions (P < 0.001, d = 0.30-0.38). Non-cleft side was thinner than controls by 0.12-0.18 mm (P < 0.001), representing 86-92% of control thickness. FD showed similar patterns. Asymmetry increased from posterior to anterior.
Conclusions
UCLP is associated with bilateral maxillary bone deficits; the non-cleft side also shows significant deviations from controls. Side-specific assessment is essential. These differences may warrant caution in treatment planning, but prospective outcome studies are needed.
Keywords
Introduction
Unilateral cleft lip and palate (UCLP) is a common craniofacial anomaly that significantly affects maxillary development, leading to characteristic bone deficits primarily localized to the cleft region.1–4 Previous studies have consistently demonstrated reduced alveolar bone height, decreased bone density, and altered cortical thickness in UCLP patients compared to non-cleft controls.5–7 However, these investigations have typically treated UCLP as a homogeneous condition, grouping right-sided and left-sided clefts together for analysis.
While these studies have provided valuable insights into specific aspects of maxillary morphology in cleft patients, a comprehensive understanding of side-specific bone structure across the entire maxilla remains unexplored. The maxilla is a complex structure with varying bone thickness at different depths from the alveolar crest, and both cortical and trabecular components contribute to its overall structural integrity. Cortical bone provides primary mechanical support and is critical for orthodontic anchorage and implant stability, while trabecular bone architecture reflects the metabolic activity and bone quality.8–11
This approach raises fundamental questions: Is the pattern of bone deficits symmetrical between right- and left-sided clefts, or does the side of the cleft influence the distribution of bone abnormalities? Furthermore, while it is well-established that the cleft side is compromised, the status of the non-cleft side remains unknown. Is the non-cleft side truly “normal,” or does it exhibit subclinical deficits that may affect treatment outcomes?
These questions have significant clinical implications. Orthodontic treatment planning, temporary anchorage device placement, and surgical interventions such as alveolar bone grafting all depend on accurate assessment of bone availability on both sides of the maxilla. If the non-cleft side is compromised, even unilateral cleft patients may require bilateral treatment considerations.12–15
Fractal dimension (FD) analysis has emerged as a valuable tool for quantifying trabecular bone architecture, providing insights into bone quality that complement conventional thickness measurements.11,16–18 Lower FD values indicate simplified, less complex trabecular architecture, which has been associated with compromised bone quality in various pathological conditions. Applying this methodology to side-specific analysis may reveal subtle differences in trabecular architecture that are not apparent on standard radiographic assessment.19–21
The depth from the alveolar crest is a critical consideration in treatment planning.22,23 At shallow depths (4-6 mm), bone quality affects orthodontic tooth movement and the risk of fenestrations or dehiscences. At intermediate depths (8 mm), it influences temporary anchorage device placement. At deeper levels (10-12 mm), it impacts surgical procedures and implant placement near vital structures. Characterizing bone structure at these multiple depths provides a 3-dimensional understanding that is essential for individualized treatment planning. 24
Recent evidence suggests that the developmental disturbance in UCLP may involve bilateral maxillary fields, not simply the focal cleft site. 4 Additionally, the side of the cleft has been associated with patterns of congenitally missing teeth, suggesting a broader developmental influence. 25 Therefore, this study was designed to: (1) compare cortical bone thickness and trabecular architecture between right-sided UCLP (R-UCLP) and left-sided UCLP (L-UCLP) patients; (2) quantify the asymmetry between cleft and non-cleft sides within individual patients; (3) determine whether the non-cleft side differs from healthy controls; and (4) identify region-specific patterns of side-to-side variation to inform clinical decision-making.
Materials and Methods
Study Design and Sample
This retrospective CBCT study was approved by the Istanbul University Faculty of Dentistry Clinical Ethics Research Board (Protocol No: 2018/81, Decision No: 324). The study utilized anonymized data, and written informed consent for the use of diagnostic records for research purposes had been obtained from all participants at the time of scan acquisition. All procedures were performed in accordance with the ethical standards of the institutional research committee and with the principles of the 1964 Declaration of Helsinki and its later amendments.
The study sample consisted of 50 patients with unilateral cleft lip and palate and 50 age- and gender-matched controls. A priori power calculation (G*Power 3.1.9.7) assuming a clinically meaningful difference in cortical thickness of 0.3 mm (SD 0.4 mm) based on pilot data (n = 5 per group) indicated that a sample size of 28 per group was required to achieve 80% power at α=0.05. Our sample of 50 per group exceeded this requirement. UCLP patients were further subdivided based on cleft side: 25 patients with R-UCLP and 25 patients with L-UCLP. All UCLP patients had received standardized treatment at our university hospital, including cheiloplasty, palatoplasty, and secondary alveolar bone grafting with autologous iliac crest bone graft, followed by comprehensive orthodontic treatment as needed. Patients with known syndromes, craniofacial anomalies other than UCLP, or history of orthognathic surgery were excluded.
No significant difference in age was observed between UCLP and control groups (P = 0.082, independent t-test). Skeletal maturity (eg, cervical vertebral maturation) was not assessed due to the retrospective design; this is acknowledged as a limitation.
CBCT Acquisition and Parameters
All CBCT scans were acquired using a standardized protocol on a Sorodex Scanora 3Dx CBCT Unit (Sorodex, Tusula, Finland). Acquisition parameters were as follows: 90 kVp, 5 mA, voxel size 0.1-0.3 mm, field of view minimum 8 × 16 cm. Only scans with voxel size ≤0.3 mm and no motion artifact were included. Given the sensitivity of FD analysis to spatial resolution, we performed a secondary sensitivity analysis restricting the sample to scans with voxel size ≤0.2 mm (n = 34 UCLP, 36 controls) to assess robustness of findings (see Results). Image analysis was performed using OnDemand 3D Project Viewer Imaging Software (Cybermed, California, USA). During acquisition, the patient's head was oriented using the device's red guiding lights and scout images to align the Frankfort horizontal plane parallel to the floor. No reorientation software other than image analysis software was used.
Measurement Protocol
Cortical Bone Thickness Measurements
Measurements were performed by a single calibrated observer who consulted with an experienced orthodontist for advice on measurement protocol and landmark identification; agreement on the approach was reached through discussion. The coronal slice through the center of the cleft (for UCLP patients) or through the ipsilateral lateral incisor (for controls) was selected as the reference image. All measurements were performed 5 mm above the alveolar crest on that slice. The alveolar crest was defined as the most coronal point of the interradicular bone septum. Cortical bone thickness was measured perpendicular to the cortical plate at depths of 4 mm, 6 mm, and 8 mm from the alveolar crest for buccal regions, and at 4 mm, 6 mm, 8 mm, 10 mm, and 12 mm for palatal regions. Measurements were obtained at 6 interradicular sites as previously described. For UCLP patients, measurements were recorded separately for the cleft side and the non-cleft side. For control subjects, right and left sides were measured separately (not averaged) to allow side-specific comparisons; however, no significant side-to-side differences were found in controls (P > 0.05), so data from both sides were combined for the main analysis.
Fractal Dimension Analysis
FD analysis was performed using the BoneJ plugin for Fiji (ImageJ Version 1.54p). Square regions of interest of 50 × 50 pixels were placed in the trabecular bone area at each depth level, avoiding cortical bone, tooth roots, and artifacts. The box-counting method was applied to calculate FD, with higher values indicating more complex trabecular architecture. Images were processed using a standardized protocol as previously described.
Reliability Assessment
Intra-observer reliability was assessed by the primary observer re-measuring 25 randomly selected scans (20% of sample) after a 2-week interval. The intraclass correlation coefficient (ICC, 2-way random effects, absolute agreement) was calculated for cortical thickness and FD measurements. The ICC for cortical thickness ranged from 0.91 to 0.95 (95% CI 0.87-0.97), and for FD from 0.89 to 0.93 (95% CI 0.84-0.96), indicating excellent reliability. Inter-observer reliability was not assessed because all measurements were performed by a single calibrated examiner; this is acknowledged as a limitation.
Statistical Analysis
Statistical analyses were performed using Python (Version 3.9) with SciPy (Version 1.9.0) and StatsModels (Version 0.13.0) libraries. Descriptive statistics (mean, standard deviation) were calculated for all measurements. Normality was assessed using the Shapiro-Wilk test.
Group comparisons were performed as follows:
For the primary comparisons between UCLP patients and controls, ANCOVA was used to adjust for the small but non-significant age difference (UCLP mean 14.8 vs control 16.5 years). The adjusted mean differences and P-values are reported.
Effect sizes were calculated using Cohen's d, with values of 0.2, 0.5, and 0.8 considered small, medium, and large, respectively. Confidence intervals (95%) were calculated for all mean differences. Bonferroni correction was applied to control the family-wise error rate across the 15 primary comparisons (3 regions × 5 parameters). The corrected significance threshold was set at P = 0.0033 (0.05/15). Statistical significance was set at P < 0.05 after correction where indicated.
Post hoc power analysis was conducted using G*Power software (Version 3.1.9.7) to confirm adequate sample size for side-specific comparisons.
Missing data and confounders: Data on missing lateral incisors adjacent to the cleft site, previous maxillary expansion, and detailed surgical histories were not available due to the retrospective design. These limitations are addressed in the section discussion.
Results
Reliability
Intra-observer ICC values were excellent: cortical thickness ICC = 0.93 (95% CI 0.89-0.96); FD ICC = 0.91 (95% CI 0.86-0.95).
Comparison of Right- UCLP vs Left- UCLP Groups
No statistically significant differences were observed between R-UCLP and L-UCLP groups when comparing cleft sides (P > 0.05 for all comparisons, simplified Table 1; full data in Supplementary Table S1). This indicates that the overall severity of bone deficits is similar regardless of cleft side, confirming a mirror-image pattern with deficits consistently localized to the cleft side.
Comparison of Cortical Bone Thickness: R-UCLP vs L-UCLP (Cleft Sides—Anterior Regions Combined).

Note: No statistically significant differences were observed for any region (all P > 0.05). Full depth-specific data are presented in Supplementary Table S1.
Asymmetry Between Cleft and Non- Cleft Sides Within Patients
When analyzed by side within patients, significant asymmetry was observed (simplified Table 2; full data in Supplementary Table S2). The most pronounced asymmetries were observed in anterior regions (canine-lateral, lateral-central, and centrals), with mean differences ranging from 0.05 to 0.07 mm (P < 0.001, d = 0.30-0.38). Posterior regions showed minimal asymmetry (0.01-0.02 mm), with only isolated depths reaching statistical significance.
Cortical Bone Thickness: Cleft Side vs Non-Cleft Side (All UCLP Patients—Anterior Regions).

Note: aBonferroni-corrected significance threshold P < 0.0033. Full depth-specific data are presented in Supplementary Table S2.
Mirror- Image Pattern: R- UCLP vs L- UCLP Analyzed Separately
Table 3 (simplified) demonstrates the mirror-image pattern.
Mirror-Image Asymmetry: R-UCLP vs L-UCLP (Anterior Regions Combined).
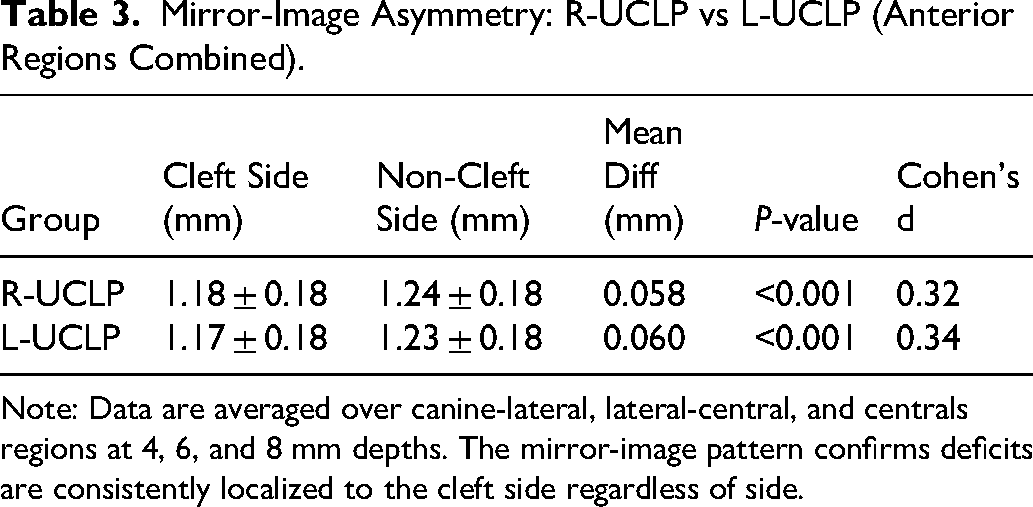
Note: Data are averaged over canine-lateral, lateral-central, and centrals regions at 4, 6, and 8 mm depths. The mirror-image pattern confirms deficits are consistently localized to the cleft side regardless of side.
Non- Cleft Side vs Controls (ANCOVA with Age Covariate)
After adjusting for age using ANCOVA, the non-cleft side exhibited cortical thickness values ranging from 86 to 92% of control values, with deficits of 0.12-0.18 mm that remained highly statistically significant (adjusted P < 0.001) (simplified Table 4; full data in Supplementary Table S3). The age covariate was not significant in the model (P = 0.21), indicating that the small age difference did not drive the findings. This indicates that the non-cleft side demonstrates significant structural deviations from age-matched healthy controls.
Non-Cleft Side vs Control Group (Anterior Regions).

Note: The non-cleft side exhibits only 86-92% of control cortical thickness. Full depth-specific data are presented in Supplementary Table S4.
Voxel Size Sensitivity Analysis
To assess whether voxel size variation (0.1-0.3 mm) influenced results, we repeated the primary comparisons (non-cleft vs control, anterior regions) restricting the sample to scans with voxel size ≤0.2 mm (n = 34 UCLP, 36 controls). The direction and significance of all findings were unchanged: mean differences ranged from 0.11 to 0.16 mm (adjusted P < 0.001). Effect sizes were slightly larger in the higher-resolution subgroup (Cohen's d range 0.72-1.04 vs. 0.65-1.17 in the full sample), suggesting that voxel variation may have slightly attenuated the true differences. Therefore, our main findings are robust to voxel size variation.
Fractal Dimension: Side- Specific Analysis
FD analysis revealed patterns consistent with cortical thickness findings (simplified Table 5; full data in Supplementary Table S4). Control FD ranged from 1.67 to 1.76 depending on depth and region; cleft side FD ranged from 1.54 to 1.62; non-cleft side FD ranged from 1.61 to 1.67. All comparisons were significant after Bonferroni correction (P < 0.001).
Fractal Dimension: Side-Specific Analysis (Anterior Regions).

Note: Bonferroni-corrected significance threshold P < 0.0033.
Cleft side vs control; bNon-cleft side vs control. Full depth-specific data are presented in Supplementary Table S5.
Regional Gradient of Asymmetry
Table 6 illustrates the gradient of asymmetry from posterior to anterior. Asymmetry increased progressively from posterior to anterior, with the largest differences in the central region.
Regional Gradient of Asymmetry (Mean Cleft—Non-Cleft Difference).
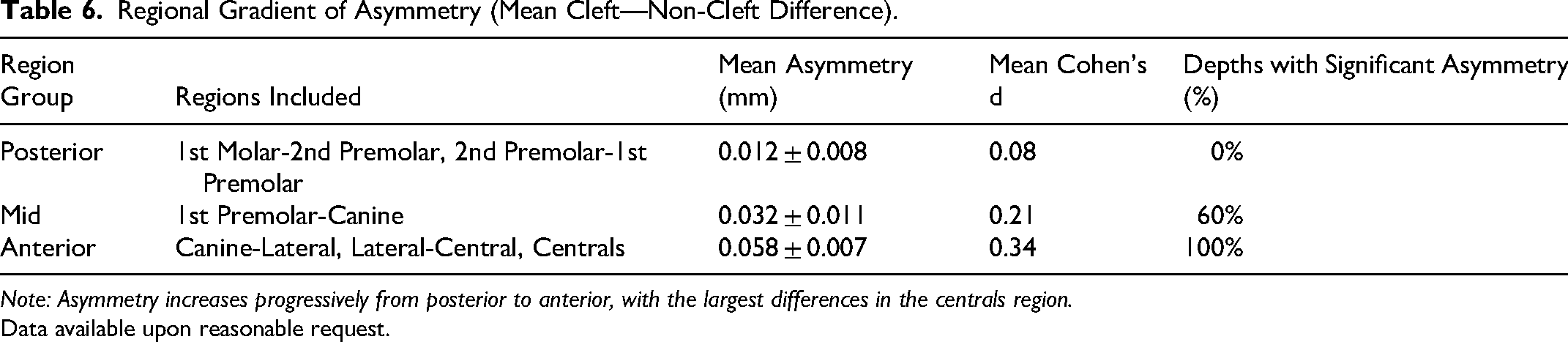
Note: Asymmetry increases progressively from posterior to anterior, with the largest differences in the centrals region.
Data available upon reasonable request.
Power Analysis
Post hoc power analysis confirmed that the study was adequately powered for side-specific comparisons. For anterior region comparisons (effect sizes d = 0.30-0.38, n = 50 per group), achieved power exceeded 0.85. For non-cleft side versus controls (effect sizes d = 0.65-1.17), power exceeded 0.99.
Discussion
This study provides the first comprehensive side-specific analysis of maxillary bone structure in patients with unilateral cleft lip and palate, comparing right-sided and left-sided clefts and evaluating the status of the non-cleft side relative to healthy controls. Our findings reveal 3 major insights.
Mirror- Image Symmetry of Deficits
The comparison between R-UCLP and L-UCLP groups revealed a striking mirror-image pattern. When groups were compared without accounting for side, no differences were observed. However, when analyzed with respect to cleft side, both groups showed identical patterns: the cleft side was consistently and significantly compromised, while the non-cleft side was relatively but not completely spared. This mirror-image symmetry confirms that the developmental disturbance in UCLP is consistently localized to the cleft side, and that the magnitude of deficit is independent of whether the cleft occurs on the right or left. This finding validates the common practice of grouping right- and left-sided clefts together for analysis, while emphasizing the importance of side-specific measurement in individual patient assessment.
The Non- Cleft Side is Not Normal
Perhaps the most clinically significant finding of this study is that the non-cleft side, while significantly better than the cleft side, remains compromised compared to healthy controls. After adjusting for age, cortical thickness on the non-cleft side was 86-92% of control values, with deficits of 0.12-0.18 mm that were highly statistically significant (adjusted P < 0.001). FD analysis confirmed that bone quality on the non-cleft side was also intermediate between cleft side and controls.
This finding challenges the common assumption that unilateral cleft patients have at least 1 “normal” side. The cleft affects both sides of the maxilla, though the contralateral side is less severely involved. This bilateral involvement suggests that the developmental disturbance in UCLP is not strictly confined to the cleft site but affects the entire maxillary complex, likely due to altered growth patterns, functional adaptations, and possibly genetic factors that influence both sides. Consistent with this, a previous study reported that cleft sidedness is associated with patterns of congenitally missing teeth, supporting a broader developmental field defect. 25
The clinical implications are that when planning treatment on the non-cleft side, clinicians should not assume bone quality and quantity are equivalent to those in non-cleft patients. These structural differences may warrant caution during orthodontic or surgical procedures, but prospective clinical studies are needed to determine whether they translate into higher complication rates.
Regional Gradient of Asymmetry
The degree of asymmetry between cleft and non-cleft sides varied markedly by region. Posterior regions showed minimal side-to-side differences, indicating relative symmetry. In contrast, anterior regions demonstrated pronounced asymmetry, with differences of 0.05-0.07 mm. This gradient mirrors the distance from the cleft site, suggesting that the impact of the cleft is most severe in adjacent areas and diminishes with increasing distance.
For procedures involving posterior regions, bilateral symmetry may be reasonably assumed. However, for anterior procedures, significant side-to-side differences should be anticipated and incorporated into treatment planning.
Fractal Dimension: Bone Quality Follows Bone Quantity
FD analysis confirmed that trabecular bone architecture follows the same side-specific pattern as cortical thickness. The cleft side showed significantly lower FD values, indicating less complex trabecular architecture, while the non-cleft side showed intermediate values between the cleft side and controls. This concordance between bone quantity and bone quality suggests that the developmental disturbance in UCLP affects both components of bone structure proportionally.
Comparison with Previous Studies
Our findings are consistent with previous studies reporting reduced bone dimensions in UCLP patients.3,4,7 However, this study extends prior work by providing detailed side-specific analysis and quantifying the status of the non-cleft side. The gradient of asymmetry we observed parallels the findings of Çelikoğlu et al 6 and Björk and Skieller, 26 who reported significant reductions in intercanine alveolar widths in cleft patients, with the most pronounced effects anteriorly.
The FD values obtained in this study are within ranges reported in the literature and demonstrate the expected gradient of bone quality. 7
Consistent with this, family history studies have identified genetic and environmental risk factors that may influence maxillary development bilaterally.27,28
Clinical Considerations
Our findings support side-specific CBCT assessment in UCLP patients, as averaging may obscure clinically significant asymmetry. However, specific numerical thresholds for clinical decision-making (eg, recommended force levels or TAD protocols) cannot be derived from this cross-sectional study. Future prospective studies correlating bone measurements with clinical outcomes (eg, orthodontic root resorption, TAD failure rates, graft success) are needed to establish evidence-based guidelines. 29
Biological Mechanisms and Iatrogenic Effects
The bilateral involvement observed in our study suggests that the developmental disturbance in UCLP is not strictly confined to the cleft site 30 . We acknowledge that the observed asymmetry may arise from a combination of innate deficiency and iatrogenic effects of surgery and orthodontics 31 . However, detailed individual surgical histories were not available in this retrospective cohort. Future prospective studies should standardize and record surgical variables.
Limitations
This study has several limitations. First, the cross-sectional design precludes causal inference. Second, we did not assess skeletal maturity (eg, cervical vertebral maturation); adjustment for chronological age may not fully account for differences in developmental stage. Third, detailed individual surgical histories and data on secondary alveolar bone grafting timing/success were not available; therefore, we cannot separate innate from iatrogenic effects. Fourth, data on missing lateral incisors adjacent to the cleft site and prior maxillary expansion were also unavailable, and these factors may influence alveolar bone morphology. Fifth, all scans were acquired on a single CBCT device with minor voxel size variability (0.1-0.3 mm); however, a sensitivity analysis restricted to high-resolution scans confirmed the main findings. Sixth, we did not correlate radiographic findings with clinical outcomes. Seventh, inter-observer reliability was not assessed because all measurements were performed by a single calibrated examiner. Eighth, the subgroup size of 25 per cleft side may have limited power to detect very subtle differences between right- and left-sided clefts. Ninth, despite using ANCOVA with age as a covariate, residual confounding from growth and developmental stage cannot be completely excluded.
Conclusion
This side-specific analysis of maxillary bone structure in unilateral cleft lip and palate patients reveals several findings. Right- and left-sided clefts show mirror-image patterns of bone deficits. The non-cleft side demonstrates significant structural deviations from age-matched healthy controls, exhibiting cortical thickness 86-92% of control values and reduced FD. Asymmetry follows a clear regional gradient, with anterior regions showing the greatest differences. These findings highlight the importance of side-specific assessment in UCLP treatment planning. These structural differences may warrant caution during orthodontic or surgical planning, but prospective clinical outcome studies are needed to determine their practical significance.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656261465481 - Supplemental material for Asymmetry of Maxillary Bone Structure in Unilateral Cleft Lip and Palate: A Cone Beam Computed Tomography Study
Supplemental material, sj-docx-1-cpc-10.1177_10556656261465481 for Asymmetry of Maxillary Bone Structure in Unilateral Cleft Lip and Palate: A Cone Beam Computed Tomography Study by Murat Mert Atapek in The Cleft Palate Craniofacial Journal
Footnotes
Ethical Approval
This study was approved by the Istanbul University Faculty of Dentistry Clinical Ethics Research Board (Protocol No: 2018/81, Decision No: 324). Written informed consent was obtained from all patients or their legal guardians at the time of CBCT scanning as part of routine clinical assessment. All procedures were performed in accordance with the Declaration of Helsinki.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.