
Abstract
This clinical report describes the prosthetic rehabilitation of a completely edentulous 12-year-old girl with AEC syndrome (ankyloblepharon–ectodermal dysplasia–cleft lip and/or palate), also known as Hay–Wells syndrome, a rare disorder frequently associated with craniofacial and oro-dental anomalies. The patient presented with severe masticatory dysfunction and esthetic concerns. Considering ongoing craniofacial growth and clinical limitations related to cleft palate repair, implant therapy was not indicated. A complete removable denture was fabricated for both arches. The patient adapted well to the prostheses, with improvement in mastication, speech, facial esthetics, and social confidence, supporting removable prosthetic rehabilitation as a suitable option in growing patients.
Introduction
Hay–Wells syndrome (HWS), also known as ankyloblepharon–ectodermal dysplasia–cleft lip and/or palate (AEC) syndrome, is a rare ectodermal disorder inherited in an autosomal dominant pattern and caused by heterozygous pathogenic variants in the TP63 gene. This gene plays a pivotal role in the development and maintenance of ectoderm-derived structures. Clinically, HWS is characterized by a constellation of ectodermal abnormalities affecting the skin, hair, nails, and teeth, in association with ankyloblepharon and cleft lip and/or palate.1,2 Approximately 30% of patients have an affected parent, while 70% have a de novo TP63 pathogenetic variant. 3 TP63 mutations have also been implicated in several other autosomal dominant developmental disorders, including Rapp–Hodgkin syndrome, ectrodactyly–ectodermal dysplasia–cleft lip/palate syndrome, acro-dermato-ungual-lacrimal-tooth syndrome, limb-mammary syndrome, and split hand/foot malformation syndrome. 4 The considerable clinical and molecular overlap among these conditions supports the concept of a phenotypic continuum within the spectrum of TP63-related disorders. This variability is attributed to distinct gain- or loss-of-function mutations affecting different TP63 isoforms, as the gene encodes multiple proteins with diverse and context-dependent biological functions. 5 AEC syndrome exhibits a broad and heterogeneous clinical presentation, including ankyloblepharon, neonatal erythroderma, erosive scalp dermatitis, limb malformations, hypohidrosis, nail dystrophy, sparse hair, and cleft lip and/or palate. 6 Ankyloblepharon filiforme adnatum, characterized by partial fusion of the eyelids, represents a distinctive and diagnostically significant feature, reported in ∼70% of affected newborns. 7
Oral and dental manifestations are prominent and clinically significant in HWS. Common findings include hypodontia or oligodontia, conical-shaped teeth, delayed eruption, and maxillary hypoplasia. Previous reports have described a markedly reduced number of permanent teeth in affected adults, with an average of fewer than 5 teeth. 8 Interestingly, the presence of impacted teeth has rarely been described in association with AEC syndrome. In the present case, radiographic examination revealed impacted mandibular teeth, an unusual finding that may further complicate prosthetic management.
Cleft lip and/or palate constitutes one of the principal craniofacial manifestations of the syndrome and is frequently accompanied by additional oral anomalies. Congenital alveolar synechiae, defined as adhesions between the maxillary and mandibular alveolar ridges, may also occur.7,9 Furthermore, patients often present with dental conditions commonly associated with cleft-related anomalies, including dental agenesis, tooth malposition, structural defects, and periodontal compromise, all of which may increase the risk of premature tooth loss. Collectively, these abnormalities frequently lead to early tooth loss and may progress to partial or complete edentulism. The resulting functional impairment, altered craniofacial development, aesthetic concerns, and psychosocial distress highlight the need for comprehensive, individualized, and multidisciplinary management.
From a prosthodontic standpoint, the odontostomatologic management of patients with HWS is particularly challenging, especially during adolescence. Ongoing craniofacial growth, oral tissue fragility, maxillary hypoplasia, cicatricial bands, compromised tissue quality within the cleft region, and the psychosocial impact of facial and dental anomalies complicate prosthetic treatment planning. In addition, the presence of impacted teeth, when present, may further complicate treatment planning by limiting available prosthetic space and altering the underlying alveolar anatomy. Although implant-supported rehabilitation may be considered in adulthood, it is generally contraindicated or deferred in growing patients because of skeletal immaturity and frequently unfavorable anatomical conditions. Consequently, removable prosthetic rehabilitation often represents the most conservative, adaptable, and clinically appropriate treatment option during this transitional phase.
Despite these challenges, the literature addressing prosthetic rehabilitation in adolescents with HWS remains scarce. Most published studies focus on clinical characterization or early surgical or dermatological management, with limited data on long-term prosthetic outcomes, particularly concerning complete removable dental prostheses in young patients. Furthermore, no standardized clinical guidelines are currently available to support prosthodontic decision-making in this specific population, highlighting the need for further clinical documentation and long-term follow-up studies.
We present the case of a 12-year-old female with HWS, emphasizing the orofacial involvement and the specific challenges related to removable prosthetic management during adolescence.
Case Report
A 12-year-old girl, the youngest of 3 siblings, was referred to our department for prosthetic rehabilitation; her chief complaint was aesthetic concerns related to her complete edentulism and considerable impairment of masticatory function.
The pregnancy proceeded without incident and was carried to term. The patient was delivered vaginally, weighing 2.5 kg, with no signs of neonatal distress. The family history revealed no congenital disorders, including any hereditary or acquired skin conditions.
At birth, the patient presented with filiform ankyloblepharon, ectodermal dysplasia, and a cleft palate, which are the characteristic signs associated with HWS. The diagnosis was confirmed by molecular analysis identifying a heterozygous missense mutation in exon 14 of the TP63 gene, which was absent in both parents.
The patient underwent surgical repair of bilateral filiform ankyloblepharon with eyelid separation under general anaesthesia at one month of age. Subsequently, 3 surgical procedures were performed during early childhood to obtain definitive closure of the cleft palate.
According to the patient's mother, she presented with oligodontia associated with small tooth size, increased dental fragility and wide diastemas, along with early tooth loss at around the age of 8.
Clinical examination revealed mild hypohidrosis, sparse, dry, and fine hair, absence of eyelashes, sparse eyebrows, thin and xerotic skin, and nail dystrophy (Figure 1).

Clinical photograph of the hands showing nail dystrophy, a characteristic manifestation of ankyloblepharon–ectodermal dysplasia–cleft lip and/or palate (AEC) syndrome.
Extraoral examination revealed a characteristic facial profile, including mild frontal bossing, a depressed nasal bridge, maxillary hypoplasia, a thin and dry upper lip with reduced lip support, and a prognathic mandibular profile (Figure 2). A mild reduction in lower facial height was also observed, consistent with a decreased occlusal vertical dimension secondary to complete edentulism.

Lateral facial photograph showing characteristic craniofacial features, including maxillary hypoplasia, a thin upper lip with reduced lip support, and a clinically apparent Class III facial profile.
Psychomotor development and growth were within normal limits, with no limb abnormalities identified. Cognitive development was age-appropriate, with good academic performance.
The intraoral examination revealed complete edentulism of both the maxillary and mandibular arches, with poorly developed ridges exhibiting marked volume deficiency, resembling Atwood Class V morphology in the maxilla and Atwood Class VI morphology in the mandible. The maxillomandibular relationship was suggestive of a class III pattern. The palatal vault is flat. The cleft palate had closed, with persistent fibrous, deformable scar tissue in the area previously repaired surgically. The clinical examination revealed a reduction in vestibular depth as well as a limitation of the usable palatal surface in the anteroposterior direction, related to impaired tissue quality in the cleft region. The soft palate appeared shortened and contractile. Prominent, hard fibrous scar bands extending between the posterior areas of the 2 maxillary and mandibular ridges were also noted (Figure 3). The buccal mucosa was thin and fragile. Indeed, these anatomical and tissue constraints were likely to compromise prosthetic support, retention, and stability, thereby complicating removable prosthetic rehabilitation.
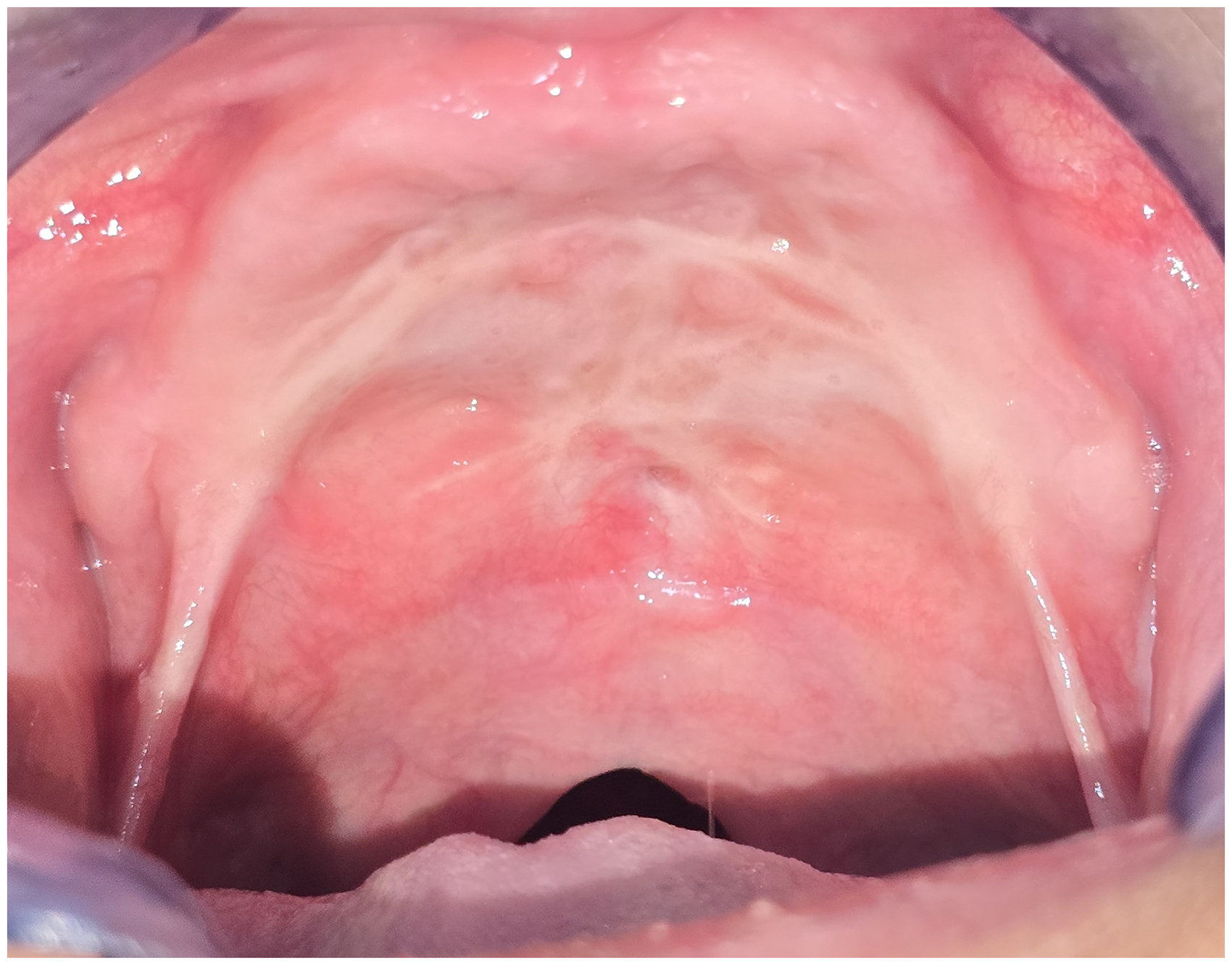
Intraoral photograph showing a repaired palatal cleft, complete edentulism, and maxillomandibular scar bands. Note the reduced denture-bearing surfaces and tissue alterations resulting from previous surgical repair.
According to the patient's medical history, premature tooth loss had occurred during childhood. Panoramic radiograph (Figure 4) revealed maxillary hypoplasia, marked resorption of the mandibular alveolar ridge, and 3 impacted permanent teeth, located ectopically within the body of the mandible. The patient had never undergone prosthetic rehabilitation. The functional assessment revealed hypernasal speech and a considerable impairment of mastication related to complete edentulism.
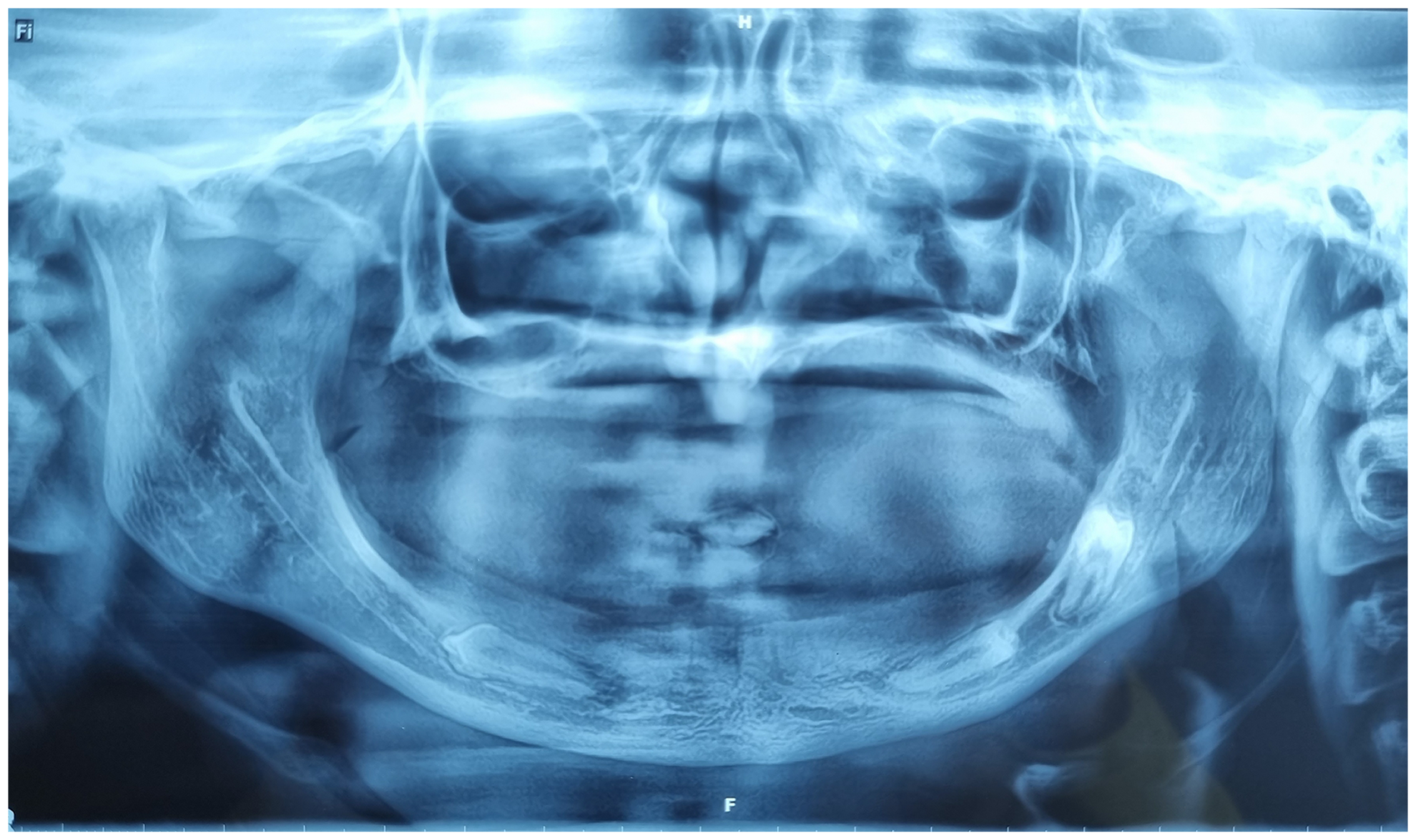
Orthopantomogram revealing the presence of 3 impacted permanent teeth in the mandible.
From a psychosocial perspective, the patient reported significant aesthetic concerns associated with edentulism, which constituted a significant functional and social handicap, leading to reduced self-esteem and a marked negative impact on her academic performance and overall quality of life.
Prosthetic rehabilitation was complicated by the sequelae of cleft palate reconstructive surgery, including fragile mucosa, poor tissue quality, and a reduced prosthetic support surface, particularly in the posterior region. Other limiting factors included maxillary hypoplasia and thick, retractile intermaxillary scar bands, which significantly compromised prosthetic stability. Complete bimaxillary edentulism, the patient's young age and the psychological distress arising from a complex medical and surgical history further increased the complexity of the rehabilitation.
Two treatment options were considered: implant-supported prostheses and conventional removable complete dentures. The first option was deemed unsuitable due to the patient's ongoing craniofacial growth, financial constraints, and the patient and her family's psychological opposition to any further surgical intervention, given her previous surgical history. Furthermore, several local anatomic factors also limited the feasibility of implant placement, namely maxillary hypoplasia, pronounced resorption of the mandibular alveolar ridge, and the presence of asymptomatic impacted teeth in the mandibular body, which we discovered incidentally on Panoramic radiography. These conditions may compromise both the surgical approach and the long-term predictability of implant-supported rehabilitation. Consequently, complete dentures were fabricated for both arches, covering the palatal scar resulting from the surgically repaired cleft palate, replacing the missing teeth, and providing good support for the peri-prosthetic tissues via the denture base, whilst taking into account the patient's specific anatomical and functional constraints (Figure 5).
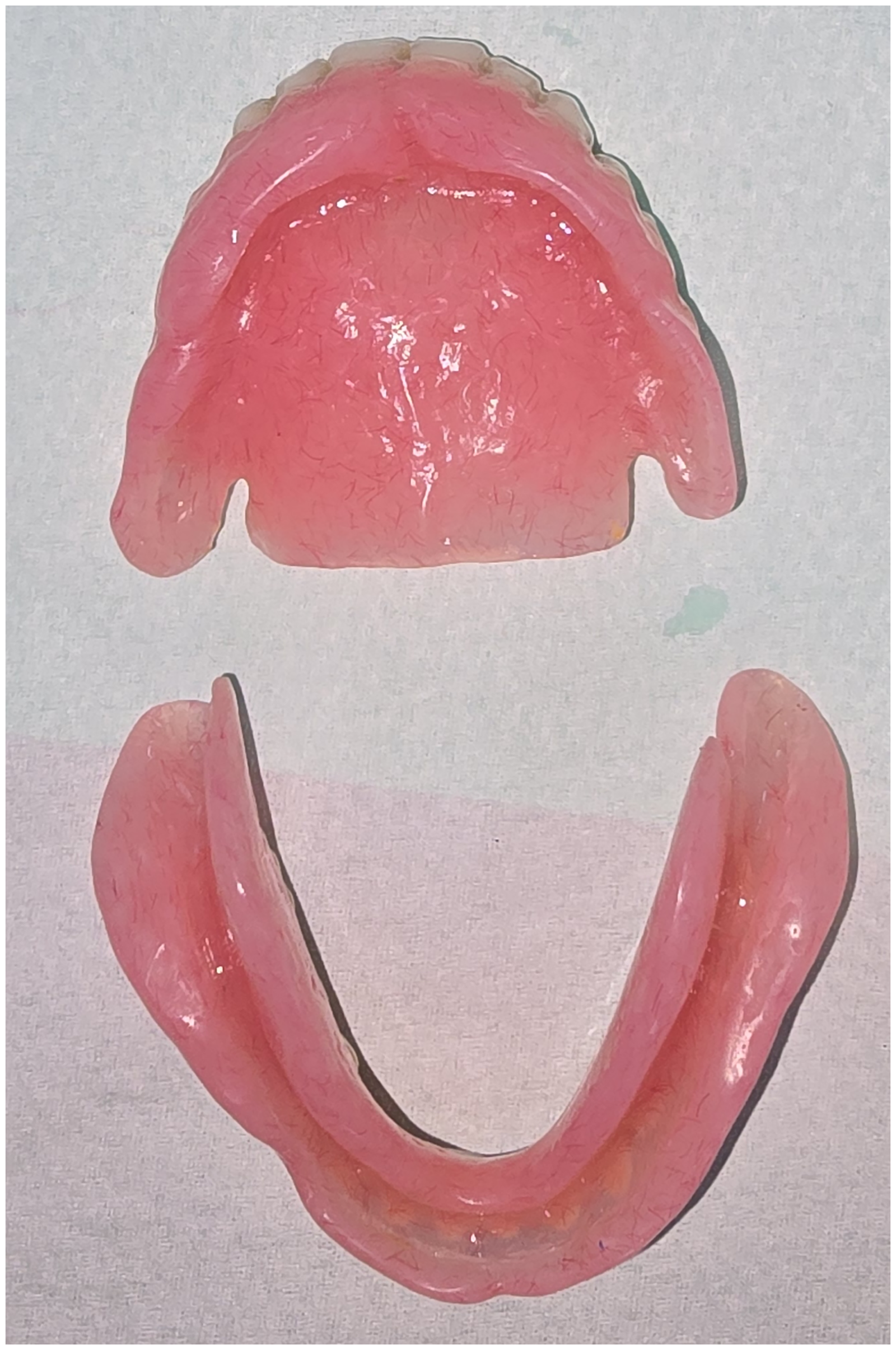
Complete removable dentures demonstrating adequate relief in the areas corresponding to the maxillomandibular scar bands to minimize tissue irritation and enhance prosthesis stability.
Preliminary impressions were made to obtain diagnostic casts. The posterior palatal seal was clinically determined using anatomical landmarks and a functional assessment, and subsequently transferred to the casts. Custom trays were fabricated from self-curing acrylic resin and adjusted to minimize tissue compression and peripheral overextension. A minimally compressive impression technique was adopted, with selective spacing provided over mobile and fibrous tissues to reduce tissue displacement. Particular attention was paid to the maxillomandibular scar bands to prevent prosthetic destabilization. Border molding was performed using impression compound, followed by a final impression with a low-viscosity silicone material. Given the presence of fragile mucosal tissues and scar bands, particular care was taken throughout the impression procedures to accommodate anatomical irregularities and minimize pressure on sensitive tissues. The potential use of soft liners and tissue conditioners was considered during treatment planning, and reserved for possible future use in the event of compromised retention, instability, or mucosal intolerance.
The occlusal vertical dimension was re-established taking into account facial aesthetics, phonetic evaluation, interocclusal rest space, and the assessment of lower facial height. Following determination of the occlusal vertical dimension and recording of centric relation, the secondary models were mounted on a semi-adjustable articulator.
The resin teeth were mounted according to a bilaterally balanced occlusal scheme to enhance denture stability during functional mandibular movements and minimize destabilizing forces acting on the supporting tissues. Given the significant deficiency of the residual ridges and the compromised oral conditions associated with AEC syndrome, this occlusal concept was considered appropriate to improve prosthesis retention and stability. Tooth arrangement was guided by both aesthetic and functional considerations, including phonetic assessment, and optimized to restore adequate lip support and harmonious facial proportion in both frontal and profile views, thus improving overall facial aesthetics.
A wax try-in was performed and approved by the patient. The final prostheses were then fabricated from heat-cured acrylic resin and polished. At insertion, the prosthetic base was carefully adapted, and occlusal adjustments were made to achieve balanced bilateral occlusion, while preserving tooth morphology and optimizing masticatory efficiency. Oral and prosthetic hygiene instructions were provided.
The prostheses were delivered, and maintenance appointments were scheduled at 1-week, 2-week, 1-month, and then monthly intervals. At insertion, the prosthesis exhibited satisfactory retention and stability despite the limited denture-bearing surfaces and the presence of scarred tissues. Clinical phonetic assessment revealed satisfactory speech intelligibility, with appropriate pronunciation following a short adaptation period. The patient adapted remarkably well to her prostheses, experiencing substantial improvements in chewing efficiency, speech, facial appearance, and social interactions. These functional and aesthetic gains were accompanied by a marked improvement in self-confidence and overall well-being. Throughout the 2-year follow-up period, no significant adjustments to the prostheses were required, and no biological or mechanical complications, such as mucosal ulceration, prosthesis fracture, or denture intolerance, were observed. Satisfactory retention, stability, and patient comfort were maintained throughout follow-up; consequently, the use of tissue conditioners or resilient denture liners was not required. At the 2-year follow-up, the patient remained satisfied with her prosthesis, reporting sustained functional and aesthetic benefits (Figure 6). The patient will continue to be monitored regularly, with definitive treatment planned upon completion of craniofacial growth.

Facial photograph obtained at the 2-year follow-up visit, showing satisfactory facial esthetics and lip support with the prostheses in place.
Discussion
AEC syndrome, also known as Hay–Wells syndrome (HWS), falls within the broad spectrum of ectodermal dysplasias (ED). 10 To date, nearly 200 distinct subtypes of ED have been identified, reflecting marked genetic and phenotypic heterogeneity. 11 ED comprise a group of conditions characterised by abnormal development of one or more structures derived from the ectoderm, including notably hair, nails, and sweat glands, as well as oral ectodermal tissues, particularly the dentition. 12
Around a hundred cases of AEC syndrome have been reported in the literature, with an equal distribution between the sexes (female-to-male ratio of 1:1). Nevertheless, the actual prevalence of this condition remains unknown. 13
In terms of oral health, clinical manifestations may include quantitative dental anomalies, such as hypodontia or even anodontia, morphological anomalies, notably conical teeth, as well as structural alterations, particularly enamel hypoplasia with dentine exposure, reflecting severe damage to hard dental tissues. Other, more rarely reported anomalies, such as taurodontism of the first molars, have also been described. 14
In the present case, the patient had 3 impacted permanent teeth, located ectopically within the mandibular body. To our knowledge, such an association has not previously been reported in the literature in patients with HWS.
Other craniofacial abnormalities may be observed, including maxillary hypoplasia, mandibular micrognathia, a broad nasal bridge, cup-shaped ears, external auditory canal atresia, a short philtrum, microstomia, and hypoplasia of the midface. A cleft palate, with or without a cleft lip, may also be present. 15
From an oral perspective, patients frequently present with early, partial, or total tooth loss. This dental condition is likely to result in significant functional and aesthetic consequences, including impaired mastication, speech disorders, altered facial appearance, as well as an impact on craniofacial development and overall quality of life.
Prosthetic rehabilitation in adolescents with AEC syndrome presents a major challenge, due to the complex interaction between craniofacial malformations, postsurgical scarring, and ongoing craniofacial growth. In this case, the presence of extensive palatal scarring, reduced prosthetic support surfaces, and the existence of retractile intermaxillary bands made it difficult to achieve retention and prosthetic stability. These constraints necessitated a rigorous and personalized adaptation of conventional prosthetic principles.
Implant-supported rehabilitation in growing patients remains a subject of controversy. Indeed, ongoing maxillomandibular development can lead to progressive imbalances between osseointegrated implants and adjacent structures, thereby compromising occlusion, facial aesthetics and long-term functional stability. Furthermore, the optimal timing of implant placement, the choice of implant site, and the predictability of long-term outcomes remain widely debated. 16
In addition, surgical morbidity may be increased in these patients, particularly in the presence of fragile soft tissues and unfavorable anatomical conditions, making implant treatment more complex and less predictable.
For these reasons, removable prosthetic rehabilitation is often considered the most appropriate treatment option during adolescence. 17 Removable dentures offer a reversible and adaptable solution that can be periodically relined, modified, or remade to accommodate growth-related changes. When implant treatment is considered, it should be limited to carefully selected cases as part of a multidisciplinary approach and regarded as a temporary rather than a permanent solution, requiring rigorous long-term follow-up. 11
In the present case, implant therapy was not considered appropriate because of the patient's age, severe maxillary hypoplasia with limited bone volume, the presence of impacted permanent teeth in the mandible, and socioeconomic considerations.
The treatment led to a significant improvement in the patient's self-esteem and psychosocial well-being, largely due to the restoration of a harmonious smile. Nevertheless, regular clinical follow-up remains essential until craniofacial growth is complete, with a view to considering definitive rehabilitation in adulthood, provided that favorable anatomical conditions prevail.
Removable prostheses offer several major advantages, notably their minimally invasive nature, reduced morbidity compared to surgical alternatives, and their ability to adapt to growth-related changes. However, the sustainability of long-term results remains closely dependent on the patient's adherence to treatment and follow-up.
Whilst the fundamental principles of complete dentures remain broadly comparable to those applied in patients without the syndrome, their implementation is frequently complicated by several specific factors, notably the fragility of the mucosa, maxillary hypoplasia, scarring associated with cleft lip and palate repair resulting in the formation of dense fibrous bands, and the difficulty in achieving effective posterior palatal sealing.
All these constraints compromise prosthetic stability, increase the risk of discomfort, and make the clinical stages particularly technically demanding. Consequently, rigorous treatment planning, combined with the adoption of specific clinical precautions, is essential to optimize functional outcomes and patient comfort. In this context, precise control of impression-taking procedures is essential to ensure accurate registration of the supporting tissues whilst avoiding interference with mobile anatomical structures, particularly bands of fibrous scar tissue that may compromise prosthetic stability. Anatomical retention factors, notably undercuts at the tuberosity and along the residual ridges, must be utilized appropriately to improve peripheral seal without compromising tissue health. Recording the maxillomandibular relationship is a key step in the fabrication of the prosthesis, as it determines both functional performance and long-term biomechanical stability. Establishing an appropriate vertical dimension of occlusion (VDO) is essential for achieving neuromuscular balance and facial aesthetic harmony. Restoring the VDO helps to improve masticatory efficiency, restore facial height, optimize the facial profile, and normalize phonetic function.
The arrangement of prosthetic teeth is a key determinant of treatment success, due to its direct influence on the stability of the prosthesis, occlusal dynamics, and the support of the peri-oral soft tissues. In patients with an unfavorable facial profile, characterized by insufficient support of the upper lip and a deficient interarch relationship, the arrangement of the teeth must strike a balance between biomechanical requirements and aesthetic imperatives. In this case, the interarch disharmony was corrected by a controlled proclination of the maxillary anterior teeth, combined with a lingualized positioning of the mandibular dentition, thereby achieving a functional and aesthetic balance in accordance with the principles of bilaterally balanced occlusion. Furthermore, the anterior prosthetic flange played a decisive role in optimizing the aesthetic result by improving maxillary labial support and contributing to the restoration of a harmonious soft tissue profile.
This case highlights the potential value of complete removable prosthetic rehabilitation in a growing patient with AEC syndrome. In the present case, this approach provided satisfactory functional and esthetic outcomes and was associated with a high level of patient satisfaction over a 2-year follow-up period. Nevertheless, the findings should be interpreted with caution given the limitations inherent to a single case report, and further longitudinal studies are needed to confirm these observations.
Conclusion
Complete removable dentures may represent a reversible, accessible, and adaptable treatment option for young patients with HWS. This case underscores the importance of individualized, patient-centered prosthetic management in special care dentistry, particularly for patients with complex craniofacial anomalies. Regular clinical follow-up remains essential to monitor craniofacial growth and, when appropriate, to plan for definitive rehabilitation in adulthood. Furthermore, early dental care appears essential to prevent premature tooth loss and limit its long-term functional and esthetic consequences.
Footnotes
Informed Consent
Written informed consent was obtained from the patient's legal guardian for participation in this case report and for publication of the clinical data and accompanying images. The patient and her legal guardian were informed about the nature and purpose of the publication, including its potential dissemination in an open-access format accessible via the internet. All identifying information has been removed to ensure patient anonymity.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.