
Abstract
Objective
We developed a hybrid technique, termed passive nasoalveolar molding (PNAM). The primary objective of this study is to compare the efficacy of PNAM to the established Grayson technique for nasoalveolar molding (NAM) in reducing the alveolar cleft in patients with clefts involving the lip and primary palate.
Design
This was a single-institution retrospective study.
Setting
One senior orthodontist performed traditional NAM, and another senior orthodontist performed PNAM.
Patients, Participants
All patients with cleft of the lip and primary palate who underwent these procedures between April 2019 and April 2022; n = 11 for NAM and n = 16 for PNAM.
Main Outcome Measures
For each patient, 3D digital models were analyzed at 2 time points: prior to treatment initiation and following primary palatal closure. Changes in interalveolar width, maxillary width, and canine position were compared using 2-tailed independent t-tests.
Results
There were no statistically significant differences between the PNAM and NAM groups. The mean reduction in interalveolar segment distance was 10.19 mm for the PNAM group and 8.32 mm for the NAM group (P = .258). Similarly, the mean change in canine distance was 2.89 mm and 1.74 mm, respectively (P = .410), and the mean change in maxillary width was 1.36 mm and 0.79 mm, respectively (P = .399).
Conclusion
PNAM achieves comparable alveolar treatment outcomes to traditional NAM while offering advantages in reduced cost and fewer required appointments. By reducing financial and logistical burdens, PNAM may improve access to care in the management of cleft lip and palate.
Introduction
Cleft lip and/or palate is one of the most common congenital anomalies, affecting approximately one in 700 births.1,2 This high prevalence has prompted physicians to establish numerous preoperative techniques aimed at improving outcomes of surgical repair. Neonates exhibit elevated levels of maternal estrogen for up to 6 months after birth, allowing for malleability of the affected tissues prior to surgical repair.3–5 Utilizing this inherent plasticity, Barry Grayson developed a technique for nasoalveolar molding (NAM). The process begins with presurgical orthopedics to mold the alveolus and minimize the cleft gap by weekly addition of acrylic to the alveolar mold to direct the cleft segments, followed by the addition of nasal stents to initiate nasal molding in preparation for subsequent cleft lip repair and primary nasal correction.6–9 Despite its potential to significantly improve surgical outcomes, NAM has limitations, including high costs, labor-intensive adjustments requiring precision dependent protocol responsibility of the caregiver, and the need for frequent (ie, weekly) patient visits.10,11
Various presurgical orthopedic techniques have emerged over the years. These techniques are classified as active and passive. Active techniques move the alveolar segments either by direct pull on the alveolar segments as done with the Latham device, or by directing the alveolar segments through weekly application of acrylic to the intraoral molding plate, as is done with classic NAM techniques developed by Grayson. Passive techniques seek to lessen the alveolar gap by applying traction to the lip segments by taping rather than actively molding the alveolar segments. Passive techniques include the Hotz appliance and other passive alveolar molding techniques.12–15 The appliance in our study is based on a design by Jacobson and Rosenstein. 16 This technique generally requires fewer follow-up appointments, resulting in a common criticism of passive methods for alveolar molding is lower efficacy compared to NAM.17,18
To address the limitations of traditional NAM, we have developed a hybrid technique, termed passive nasoalveolar molding (PNAM), which combines some active techniques utilized in NAM such as nasal stenting and taping, with a passive intraoral appliance that was designed in the 1960s. 16 The intraoral appliance is used to maintain palatal width and alveolar arch form without actively molding the alveolus. The primary objective of this study is to compare the efficacy of PNAM to the established Grayson NAM technique in reducing the alveolar cleft.
Methods
A single-institution retrospective chart review was conducted, encompassing all patients with cleft lip and cleft of the primary palate undergoing NAM or PNAM. All treatment was provided by 2 senior orthodontists, one of whom provided NAM treatment, and the other provided PNAM treatment. Families were given a choice of which treatment to pursue based on distance from the treating orthodontist, and frequency of orthodontic visits required, with NAM treatment requiring weekly visits and PNAM treatment requiring visits every 2-3 weeks. Patients who did not complete treatment, or were not consistently compliant, were excluded from the study. Only unilateral cleft deformities were considered. Age at treatment initiation and completion was the same for all patients, with the initial impression taken in the first month of life, cleft lip repair completed at age 3 to 5 months, and cleft palate repair completed at age 11 to 13 months. To control for interprovider variability, all NAM and PNAM treatments were each managed by a single, dedicated orthodontist. The protocol for surgical treatment was the same for both groups. For each patient, 3D digital models were analyzed at 2 time points: prior to treatment initiation (pretreatment) and following primary palatal closure (posttreatment). Pre- and posttreatment digital impressions of each patient's oral cavity were obtained using a 3Shape TRIOS Scanner (Copenhagen, Denmark).
Three-dimensional digital models of each patient's oral cavity were analyzed to record measurements for interalveolar width, maxillary width, and canine positions at both time points. Canine position was determined based on midline identification and appreciation of preerupted teeth and their effect on alveolar morphology. Treatment-related changes in these parameters were then calculated by subtracting the pretreatment measurements from the posttreatment measurements.
To compare treatment outcomes between the PNAM and NAM groups, 2-tailed independent t-tests were conducted for the changes in maxillary width, interalveolar width, and canine positions. The PNAM group included 16 patients, while the NAM group consisted of 11 patients. Statistical significance was determined a priori at P < .05. All statistical analyses were performed using RStudio version 2023.09.1 + 494 (Vienna, Austria).
NAM Methodology
Our technique for traditional NAM is very similar to that described by Grayson and utilized by numerous colleagues.6–9,15,19–22 Briefly, an oral plate is inserted within 3 weeks after birth (Figure 1a). Patients attend weekly dental appointments during which the device is adjusted by adding soft acrylic to the labial surface of the alveolar ridge near the leading edge of the greater segment on the NAM appliance (Figure 1b) as well as strategic reductions of hard acrylic to allow for alveolar directional movement, coupled with taping vectors to aid in retention and directional movement. A nasal stent is added to the oral plate once the alveolar gap is less than 5 mm (Figure 1c). On subsequent visits, soft acrylic is added to the existing acrylic bulb to continue to lift, shape, and project the nasal tip forward. The intraoral device is discontinued after cleft lip repair.
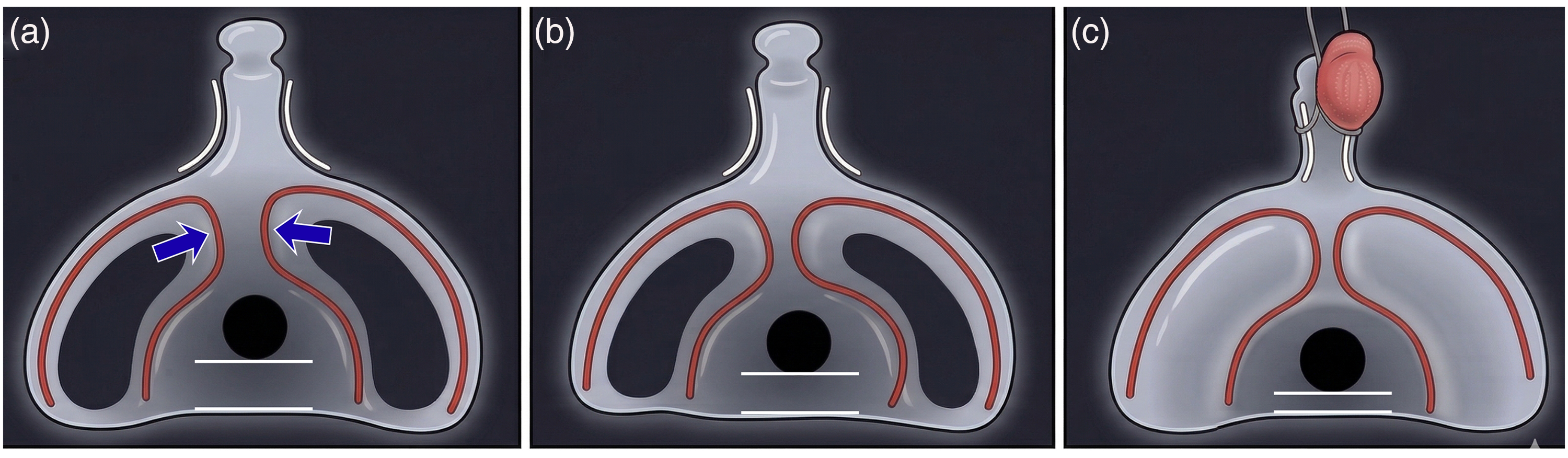
NAM technique. (a) Intraoral molding plate inserted for a right unilateral cleft lip and alveolus within 3 weeks after birth; arrows indicate direction of force applied by the molding plate. (b) Active movement of the alveolar ridge achieved by weekly addition of soft acrylic to the intraoral plate. (c) Nasal stent is added to the intraoral plate once the gap is <5 mm.
PNAM Methodology
Using the 3Shape TRIOS Scanner, initial patient assessment and digital impressions of the oral cavity are conducted between 1 and 3 weeks of age. A follow-up appointment is scheduled within a few days for appliance placement. The procedure begins with presurgical orthopedics, focused on alveolar alignment and maintaining palatal width (Figure 2a-c). The appliance is constructed with a layer of soft acrylic that flows into the undercuts of the cleft covered with a hard acrylic for strength. 16 When placed under warm water, the soft acrylic becomes more pliable which helps with insertion and retention of the appliance. Denture powder or paste can be used for additional retention. Extraoral tape is applied to provide gentle traction to the lip. Nasal stents are attached to an appliance with delivery but usually activated on the first adjustment to ensure the baby is used to the appliance before adding the nasal tip pressure.
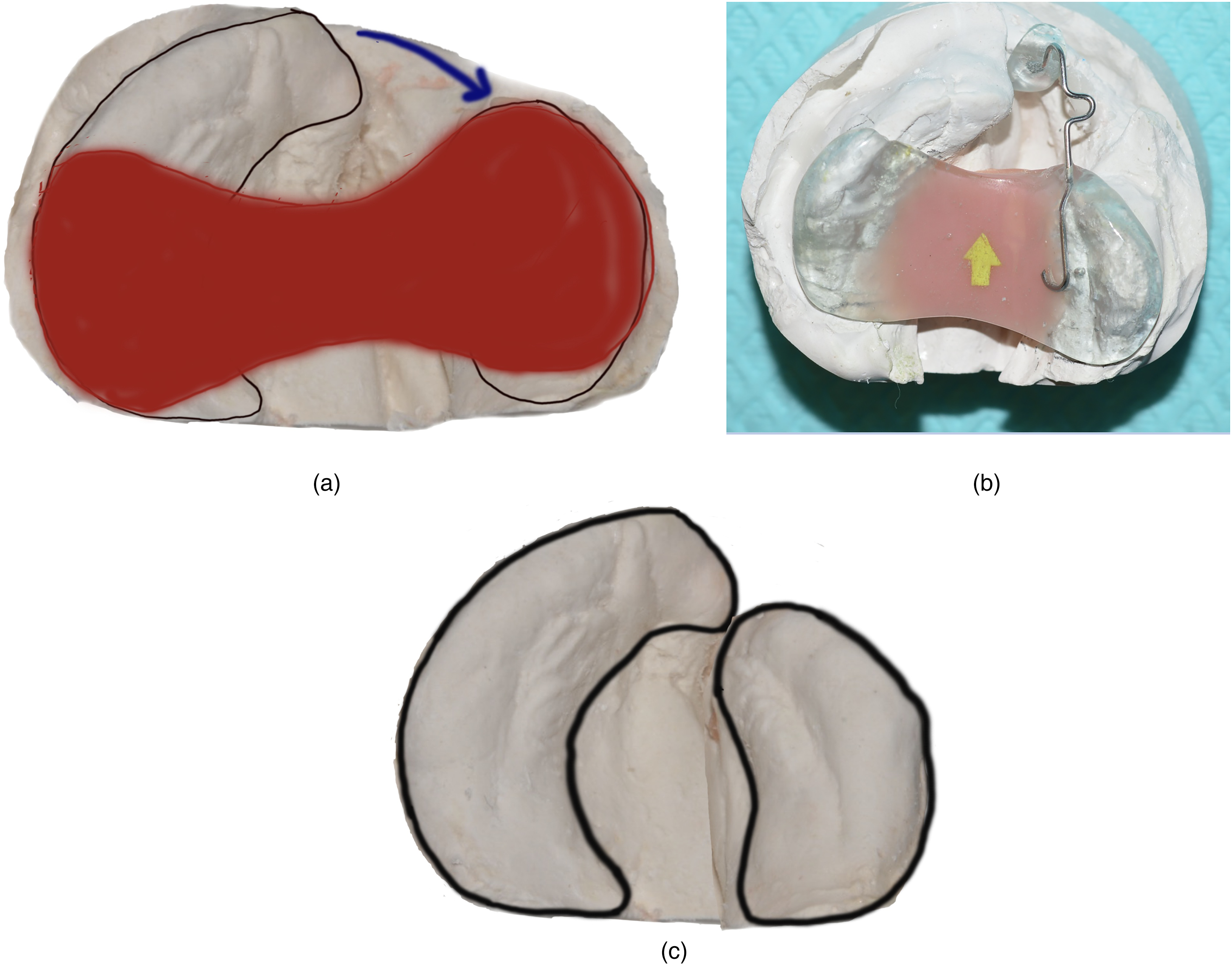
PNAM technique. (a) The intraoral plate placed on a study model, maintaining the transverse dimension of the alveolar arches; Alveolar ridge is outlined and the greater segment will be directed toward the lesser segment (arrow) by the tension from lip taping. (b) Nasal stent added to the intraoral appliance at the initial visit and activated on subsequent visits. (c) Alveolar segments approximated by the time of the palate repair while maintaining transverse palatal width.
Subsequent appointments for adjustments of the intraoral appliance and nasal stents are scheduled every 2 weeks and typically last 15 to 30 min. A few days prior to lip repair, the nasal stents are removed, and active molding with the appliance is discontinued. However, patients often choose to continue using the intraoral appliance as a feeding obturator until palatal closure. The appliance fits snugly into the gap in the palate due to the soft acrylic and only fits one way. Cost was not a factor if a family chose to continue with obturator use following lip repair, and this did not incur an additional charge by the supervising orthodontist. Following lip repair, patients are seen for 2 short visits, 8 weeks apart, to check that the appliance is fitting well and there are no areas of mucosal irritation. During this time, caregivers are easily able to keep the appliance in the cleft gap due to the snug fit offered by the soft acrylic.
Parent compliance with NAM and PNAM was excellent, there were no cases that dropped out of the sample. Any case that didn’t comply fully with the technique was excluded from the study.
Results
There were no statistically significant differences between the PNAM and NAM groups in alveolar width prior to treatment. Prior to treatment the interalveolar width was 11.71 mm ± 3.03 for the PNAM group and 10.04 mm ± 3.95 for the NAM group (P = .2250). The mean reduction in interalveolar segment distance was 10.19 mm for the PNAM group and 8.32 mm for the NAM group (P = .258). Similarly, the mean change in canine distance was 2.89 mm and 1.74 mm, respectively (P = .410), and the mean change in maxillary width was 1.36 mm and 0.79 mm, respectively (P = .399) (Table 1, Figure 3).
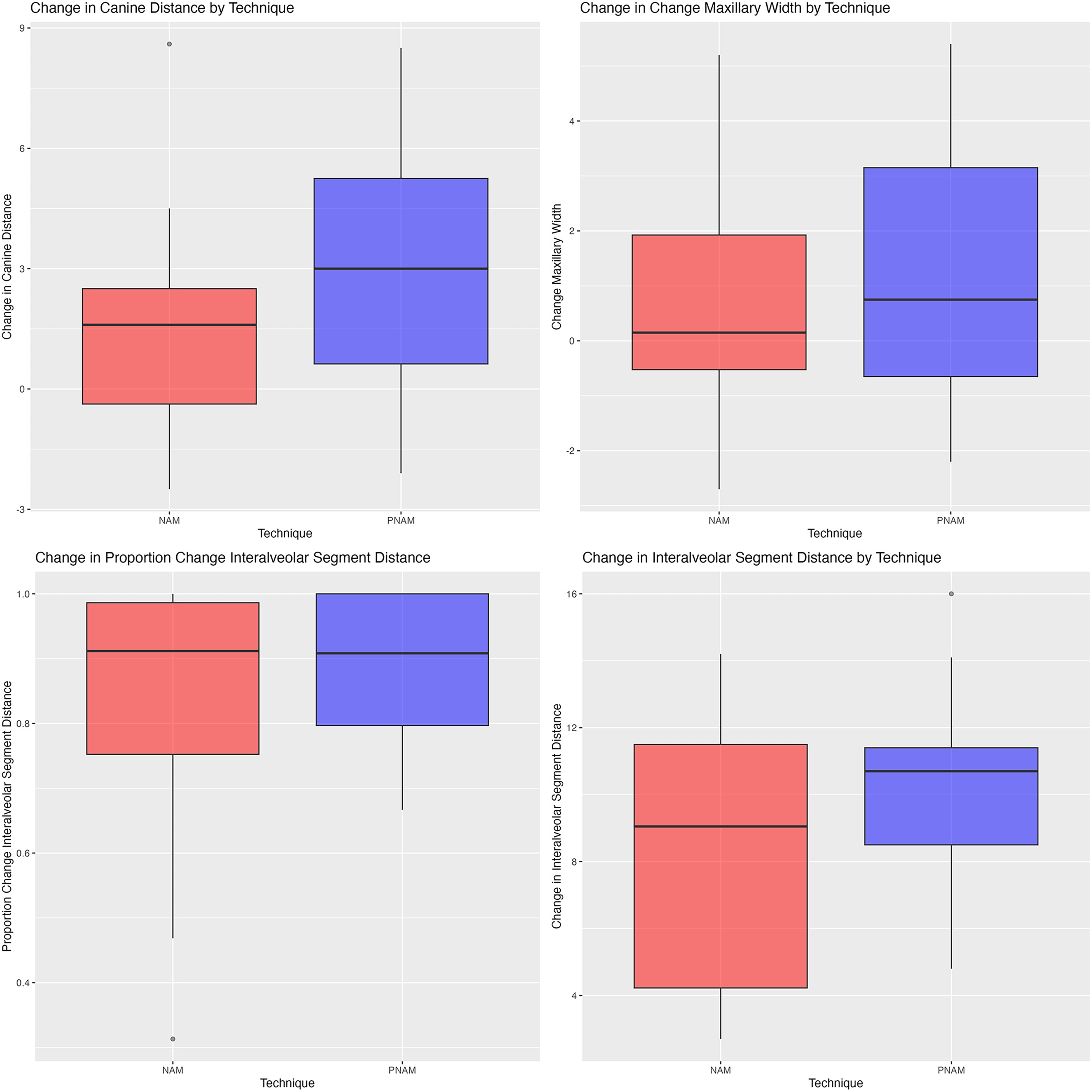
NAM versus PNAM measurement boxplots. No significant differences were observed between NAM and PNAM techniques.
NAM Versus PNAM Measurements.

Abbreviations: NAM: nasoalveolar molding; PNAM: passive nasoalveolar molding.
No significant differences in canine distance, interalveolar segment distance, or maxillary width were observed between NAM and PNAM techniques.
Discussion
The principal finding of this study is that our PNAM technique achieved comparable alveolar gap reduction to the traditional active Nasoalveolar (NAM) technique. Despite its reduced treatment burden, PNAM demonstrated no significant differences in changes to interalveolar distance, canine distance, or maxillary width. While previous research has indicated that passive techniques may be more cost and time-efficient than NAM,15,16 concerns have been raised regarding their potentially lower efficacy.17,18 Notably, the PNAM technique described in this paper appears to achieve similar results to NAM, while potentially retaining the advantages of passive approaches, a promising finding for lowering the costs and barriers to care in implementing techniques for presurgical orthopedics in cleft children.
Whereas both PNAM and traditional NAM utilize comparable biomechanical principles to guide craniofacial growth, traditional NAM incorporates an active component: an intraoral appliance that is adjusted in 0.5 to 1 mm increments weekly through the addition of soft acrylic to the labial segment of the appliance, thereby progressively repositioning the alveolar segments.5,9,19,23 In contrast, PNAM typically employs a passive intraoral appliance that is premolded to guide alveolar segments without the need for weekly adjustments.9,10 By combining elements of both approaches, PNAM may offer a balance between active and passive forces, potentially optimizing treatment outcomes while minimizing the need for frequent adjustments.
A key point of contention surrounding NAM is centered on its management.18,24–26 Aside from complications resulting from NAM, 21 its successful implementation can place a substantial burden on providers and patients’ families. This burden is multifaceted, encompassing financial costs, logistical challenges, and the potential for noncompliance.22,27 Past studies have reported average NAM-associated expenses of approximately $8739 ± $113.44, 28 which aligns with the approximately $ 10 000 charged at our institution. In contrast, the cost of PNAM at our institution is significantly lower, at approximately $3000.
The high frequency of appointments not only increases the financial burden on families but also contributes to a higher rate of missed appointments, which represents a substantial financial cost for healthcare institutions. 29 By achieving similar outcomes with fewer appointments and lower costs, PNAM may increase the overall utilization of presurgical orthopedic techniques in cleft patients, offering a compelling alternative for centers that find the traditional NAM protocol prohibitive. By minimizing the number of visits, PNAM may mitigate cumbersome barriers by reducing costs for families and providers, decreasing travel burdens, and improving compliance.
A common criticism leveled against passive presurgical infant orthopedic techniques is their purportedly lower efficacy compared to NAM.17,18 However, our findings challenge this notion. Our analysis revealed no statistically significant differences in outcomes between NAM and PNAM when measured at the time of palate repair. These results are particularly encouraging for clinicians who are interested in implementing presurgical orthopedic techniques but find the NAM protocol to be excessively demanding on both providers and patients.
Anecdotally, another benefit of the PNAM design we employed is that many families feel that the device improves comfort during feeding. Because the appliance uses soft acrylic to go into the cleft areas, the appliance is very stable and the retention is excellent. This creates an obturator effect that allows the tongue to control the milk/formula flow through the nipple and assist with feeding. The classic NAM appliance designed by Grayson 7 is designed to be free floating and inherently less stable during feeding. The intraoral device used with NAM is removed after cleft lip repair. In contrast, the intraoral device used in our PNAM method can be utilized until cleft palate closure to assist with feeding. In our experience, families appreciate using the intraoral appliance as a palatal obturator after lip closure.
The primary limitations of this study are its retrospective design and small sample size. Unfortunately, we are unable to extend the NAM sample size as the orthodontist performing this technique is no longer in practice and adding the outcomes of another orthodontist would introduce a confounding variable. However, we had the unique opportunity to compare outcomes between 2 senior orthodontists who practiced concurrently on a similar patient population, which is not easily reproduced. Furthermore, conducting robust retrospective chart reviews for presurgical orthopedic techniques in infants is inherently challenging due to the variability in treatment protocols and data collection methods.10,20,30 This did not allow us to analyze complications such as sore spots or mucosal irritation. Another limitation of our study is that the final measurements were obtained at the time of palatal closure, rather than at lip closure. Consequently, the precise position of the alveolar segments at the time of lip repair remains unknown. Of note, a central objective of NAM is nasal correction, a variable we were unable to evaluate in this study. This is an important area for future investigation. Future studies with larger sample sizes, prospective data collection, standardized protocols, and nasal morphology are needed to confirm our findings and further evaluate the long-term efficacy of PNAM.
Conclusions
This study demonstrates that PNAM achieves comparable alveolar treatment outcomes to NAM, as evidenced by similar changes in interalveolar segment distance, canine distance, and maxillary width. Moreover, PNAM offers several advantages over NAM, including reduced cost, decreased chair time for providers, and fewer follow-up appointments. While further investigation is warranted to assess long-term outcomes, these findings suggest that PNAM has the potential to increase access to presurgical infant orthopedics. By potentially reducing financial and logistical burdens, PNAM may improve access to care and promote greater health equity in the management of patients with clefts involving the lip and primary palate.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.