
Abstract
Craniometaphyseal dysplasia (CMD) is a rare disorder that causes hyperostosis of craniofacial and long bones. Radiographic findings can show narrowing of the foramen magnum due to bony overgrowth. Orthognathic surgery, orthodontics and implant placement in these patients have been rarely reported and can pose significant challenges due to bony sclerosis. We present a male patient with CMD with class III incisors on a skeletal III base, with obstructive and central sleep apnea. Our patient successfully underwent orthodontic treatment, a Le Fort 1 osteotomy with refashioning of the nasal passages, and subsequent implant placement at the age of 16 due to psychosocial pressures. The surgical results have remained stable at 5-year review.
Introduction
Craniometaphyseal dysplasia (CMD) is a rare hereditary bone disorder occurring in both an autosomal dominant and an autosomal recessive pattern. It falls under the category of disorders known as craniotubular bone dysplasia, which are characterized by abnormal skeletal development and remodeling. 1 Its characteristic features are typical and include hyperostosis of craniofacial bones, and an abnormal development of the metaphysis of long bones. 2
While the exact pathogenesis remains unclear, mutations in the ANKH gene are known to contribute. This gene encodes the progressive ankylosis protein (ANK), which is responsible for transporting inorganic pyrophosphate (PPi) across cell membranes.3-5 PPi extracellularly acts as an inhibitor of bone mineralization; therefore, ANK's function plays a critical role in normal bone remodeling. 6 In CMD individuals, mutations in ANKH disrupt the normal transport mechanism, resulting in decreased levels of PPi levels in the extracellular matrix. This causes increased density and progressive thickening of cranial bones, which is a key feature of CMD.2,4
The craniofacial hyperostosis causes protrusion of the frontal and paranasal region, flattened nasal bridge, hypertelorism, and obliteration of paranasal sinuses and mastoid. 7 Additionally, hyperostosis may also cause compression of cranial nerves, resulting in complications such as visual and hearing impairments and facial paralysis. 3
From a dental perspective, dental eruption is frequently impaired due to increased bone sclerosis. Deciduous teeth are often retained longer than usual, and eruption of the permanent teeth is typically delayed by around 2 years. 3 The literature also indicates that these patients may have bucco-lingual expansion of the maxilla and mandible, with this being more prominent in the mandible. 8 Affected individuals often present with a prognathic mandible and delayed eruption of permanent teeth, which may necessitate orthodontic and orthognathic interventions.8-10
Clinically, the autosomal dominant form is more common and tends to have a milder presentation, with affected individuals having a normal life-expectancy despite the characteristic clinical features. Whereas those with the rarer autosomal recessive form tend to experience a more severe form of the disease due to extensive hyperostosis and cranial nerve compression.9,11
Radiographic findings can often show narrowing of the foramen magnum caused by hyperostosis of the skull. In severe autosomal recessive cases, quadriparesis or death can occur due to narrowing of the foramen magnum with the compression of the medulla.12,13
Although CMD presents with distinctive clinical features, genetic testing is essential in reaching an accurate diagnosis. Due to similar physical and radiographic features, conditions such as craniodiaphyseal dysplasia, frontometaphyseal dysplasia, and Pyle disease have been misdiagnosed as CMD. 14
Case Report
We present a case report of a male patient with CMD who was initially referred to the maxillofacial dental department at Great Ormond Street Hospital in 2013. In this report, we discuss our experience of managing our patient through his orthodontic treatment, orthognathic surgery, restorative dental care, and post-surgical review. Written informed consent was obtained from the patient for publication of health information and images.
At 17 months of age, the patient was referred for genetic testing by both the Ear, Nose and Throat (ENT) specialists and pediatricians, following the observation of distinctive clinical features, including a broad nasal bridge, hypertelorism, hearing impairment, and cranial size outside of the normal centiles. Interestingly, clinicians observed strong physical similarities between the patient and his mother, who exhibited comparable clinical features and hearing impairment. While these features in the mother had been previously been attributed to birth trauma, the treating pediatrician suspected an underlying inherited condition.
At the age of 2 years, genetic testing confirmed a diagnosis of autosomal dominant CMD, with the condition identified as having been inherited from the patient's mother. This genetic diagnosis was further confirmed by several specialties including ENT, Pediatrics, Neurology, and Endocrinology, all of whom independently documented clinical features of CMD.
Early clinical presentations included hearing impairment requiring hearing aids by the ENT team at age 18 months, with ongoing delay in speech and language development. Further investigations determined that the hearing impairment was caused by a number of factors including: otitis media with effusion, restricted ossicular mobility, and stenosis of internal acoustic meatus, affecting the eighth cranial nerve function. The ongoing nasal obstruction was due to bony thickening of the nasal cavities, a characteristic feature of CMD.
A computed tomography (CT) brain and CT skull scan taken of our patient at age 5 (Figure 1), reported by a neuroradiologist, demonstrated significant hyperostosis of craniofacial bones, particularly affecting the petrous bones, with suspected compression of adjacent nerves and the auditory system. The frontal bone measured 14 mm in thickness. There was a lack of pneumatization in the bilateral maxillary sinuses and mastoid air cells, while the ethmoid air cells appeared hypoplastic. The skull base and foramen magnum were also found to be small. Additionally, the middle ear clefts were reduced in size and partially opacified. The reporting neuroradiologist concluded that appearances were consistent with features of CMD.
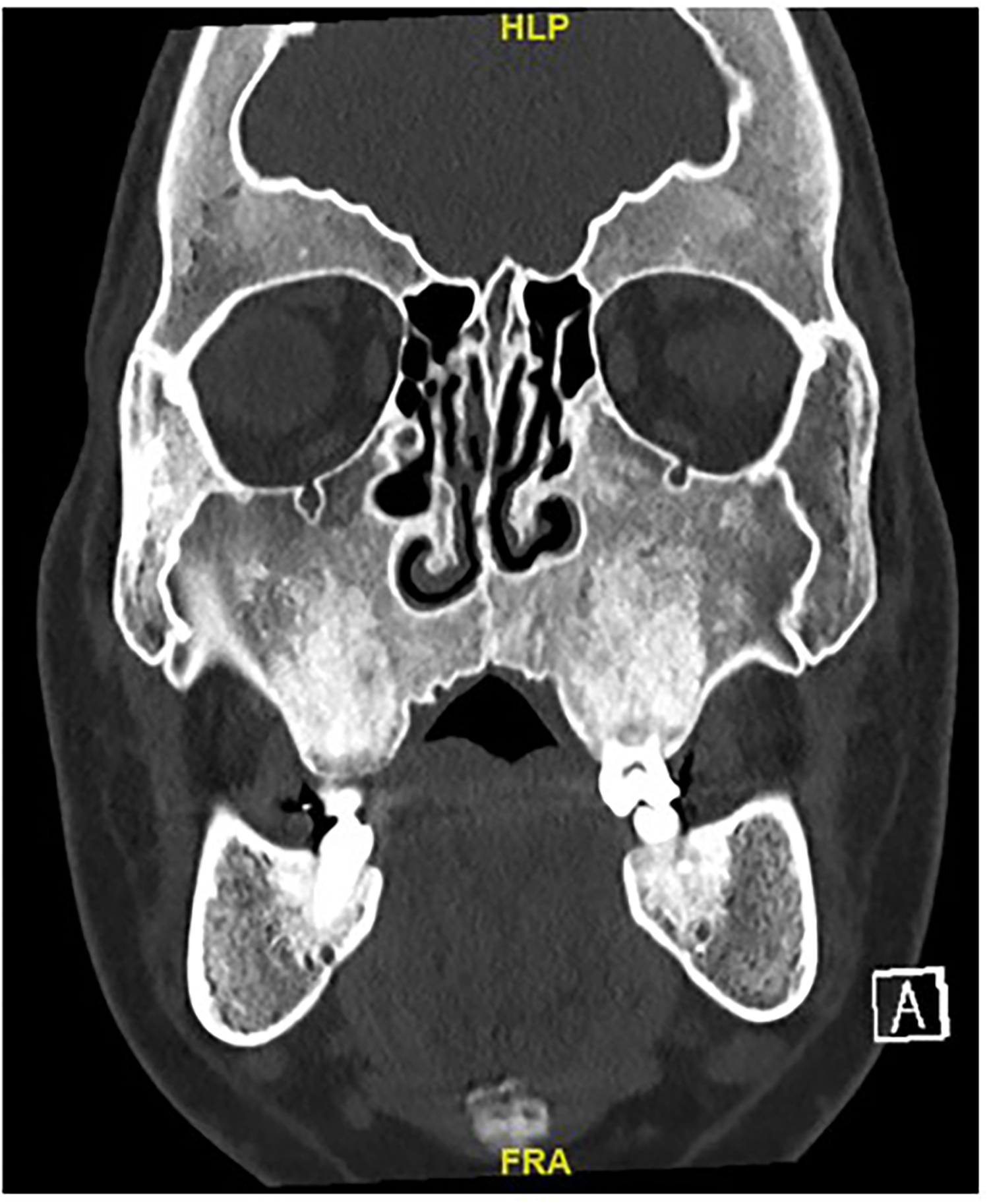
CT showing total obliteration of the sinus. Key CMD-related findings not shown in this slice: obliteration of CSF space at foramen magnum, cerebella tonsillar descent to the level C2. CMD, craniometaphyseal dysplasia.
A review with the ophthalmology team revealed no significant ocular abnormalities beyond the previously documented hypertelorism.
At age 10, our patient was assessed by our orthodontic team, when he was in the mixed dentition with the upper left central and lateral incisor in palatal cross bite. A course of upper removable appliance therapy was provided to correct this.
At age 13, our patient was reviewed by our orthodontic team, who noted several unerupted permanent teeth (Figure 2). To facilitate the eruption of these permanent teeth before bone sclerosis occurred, all remaining deciduous teeth were extracted, and a surgical exposure and bond procedure for UR5, UL4, UL5, LL4, and LR4 was performed under general anesthesia. These teeth were subsequently aligned with fixed appliances. Orthodontic tooth movement and alignment of the impacted teeth was slow, which is likely to be related to the increased bone density.
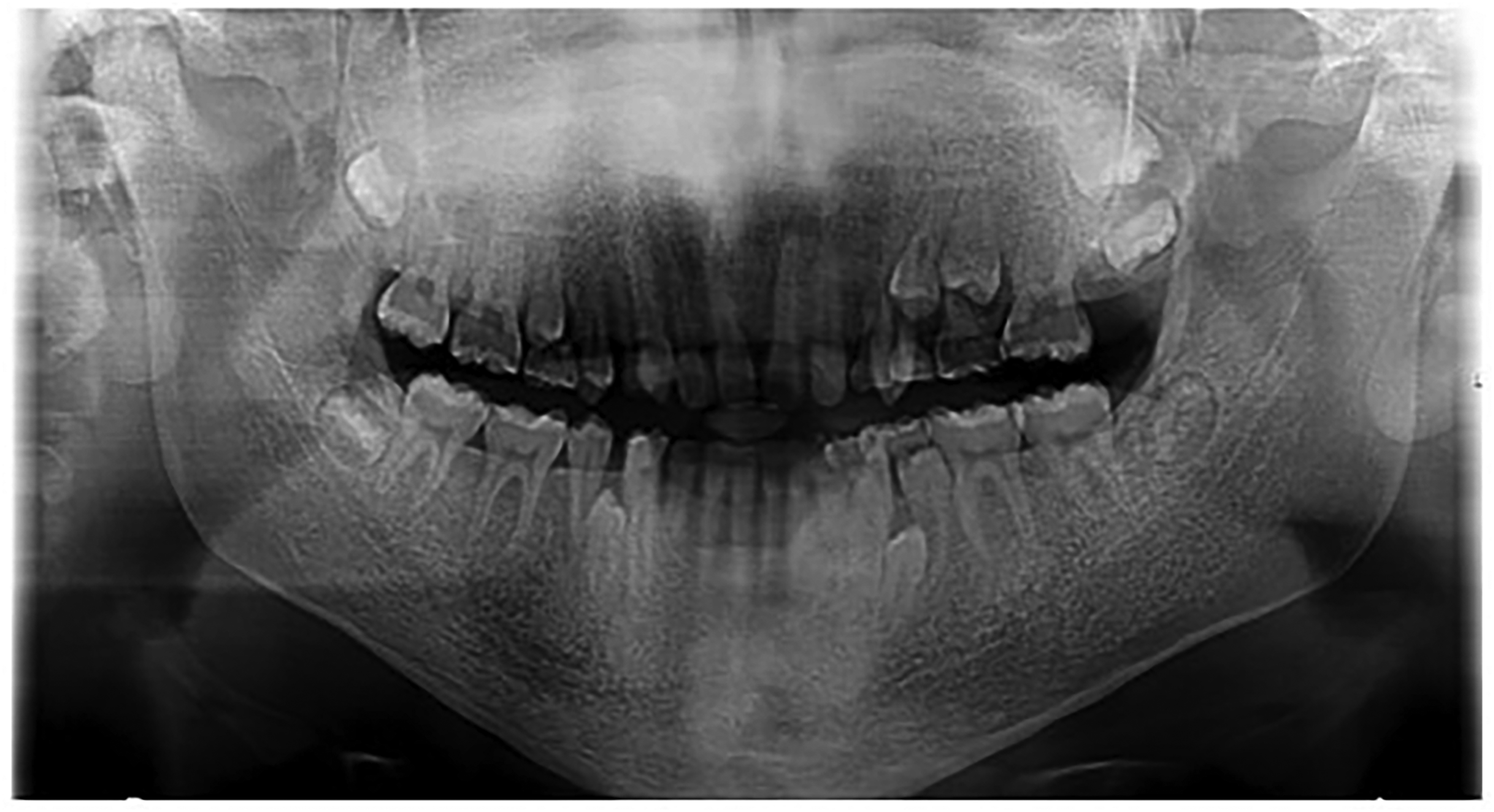
Orthopantomogram taken at age 13.5 years demonstrating the unerupted UR5, UL4, UL5, LR4, LL4, LL5.
The patient had significant spacing in the upper arch and together with restorative and maxillofacial teams, it was decided that it would be better to avoid extended time in orthodontics and prosthetically place an extra unit in the upper right and left quadrants.
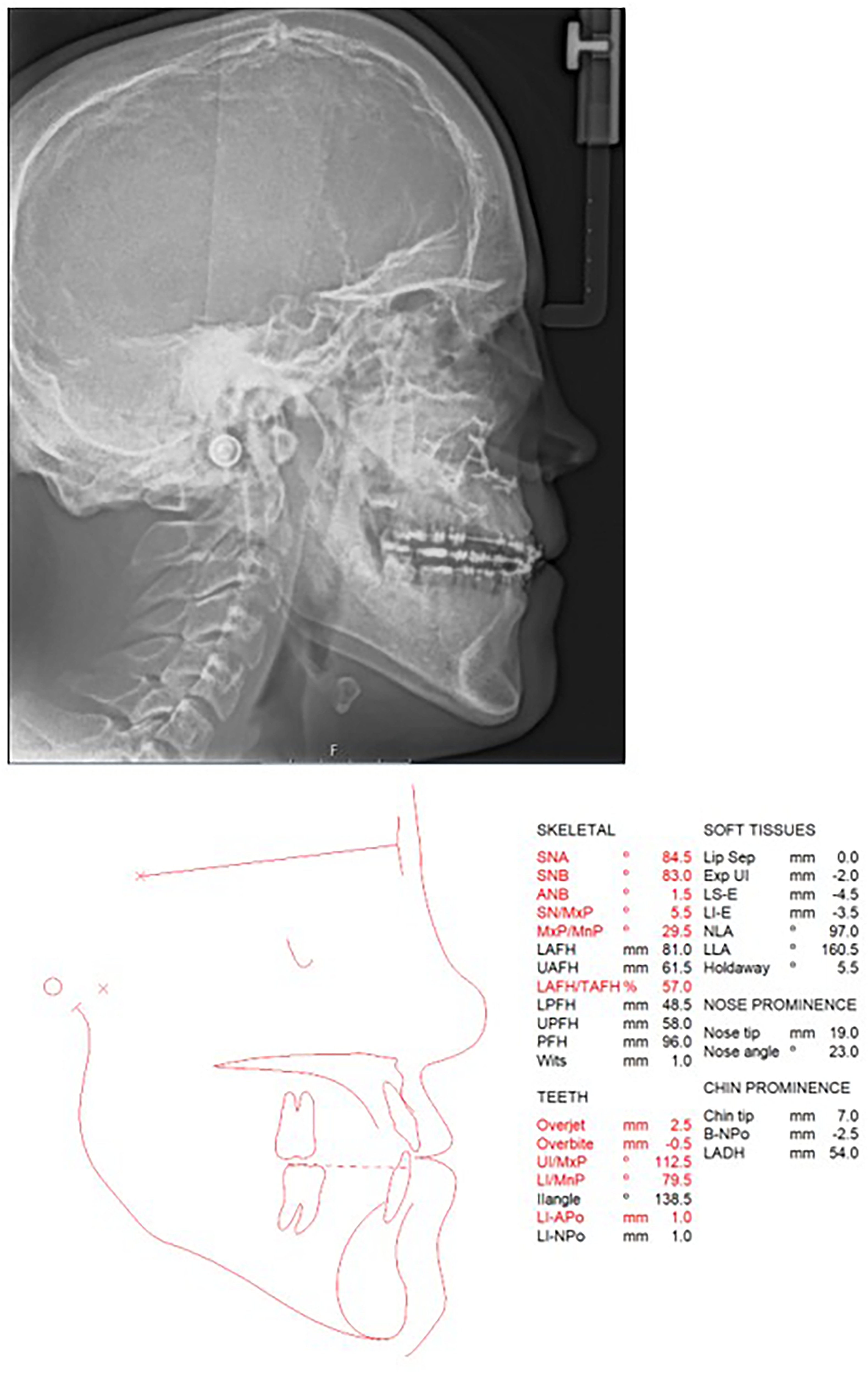
At age 14, during his orthodontic treatment, our patient expressed significant concerns about his facial appearance, difficulty eating, and reported experiences of being bullied at school. Clinical assessment revealed a class III incisor relationship on a skeletal III base, with increased vertical proportions (Figure 3). Following joint review with the maxillofacial team, it was established that the extent of the skeletal discrepancy meant that orthodontic camouflage would not address the patients’ concerns and orthognathic surgery would be required to achieve optimal functional and esthetic outcomes (Figure 4). Our patient was also referred for psychological assessment, to further explore his motivations for orthognathic surgery and to provide psychological support. This identified three primary motivations for the patient's desire to undergo orthognathic surgery.
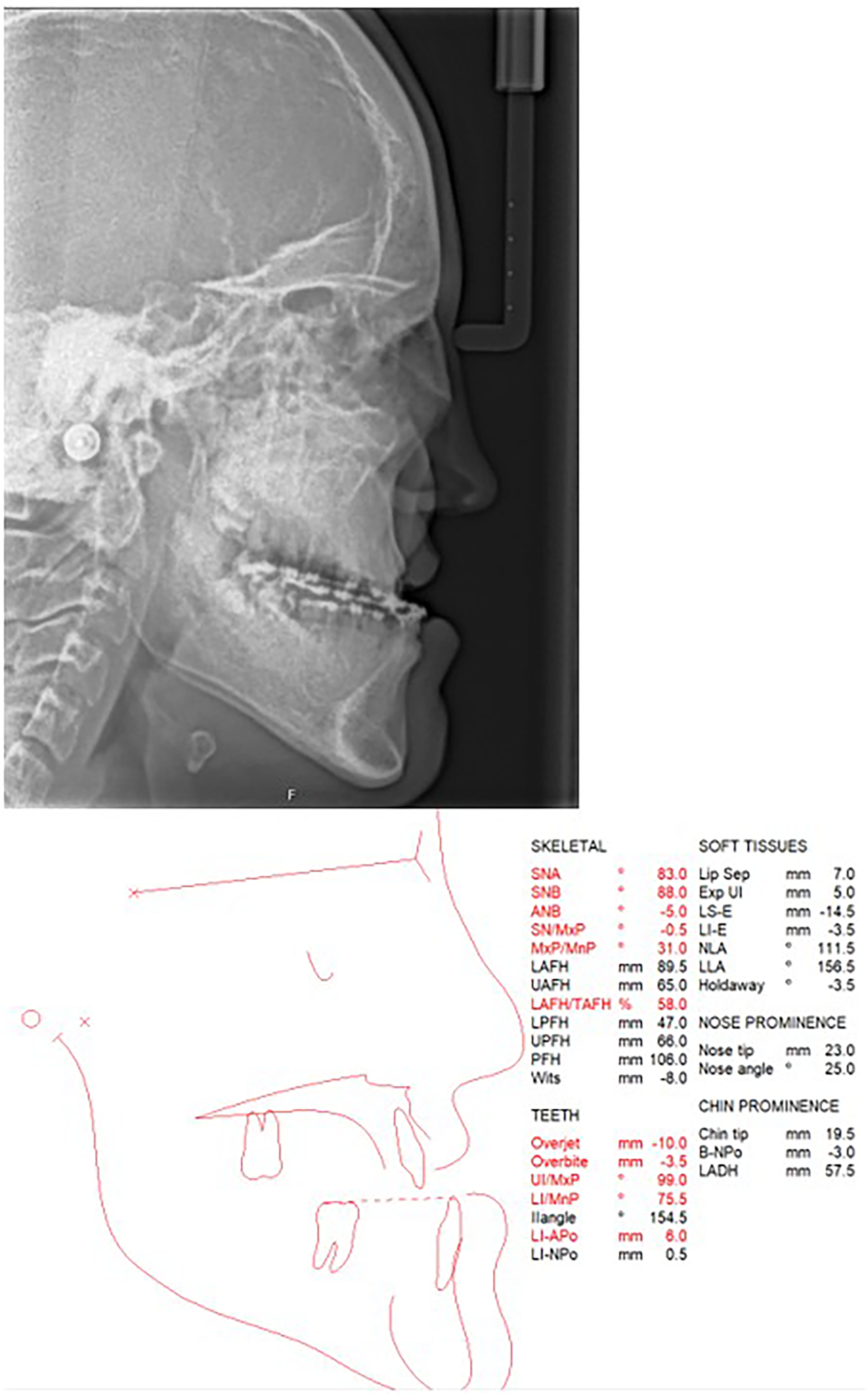
Pre-surgical lateral cephalogram and tracing demonstrating Class III malocclusion and skeletal III pattern.

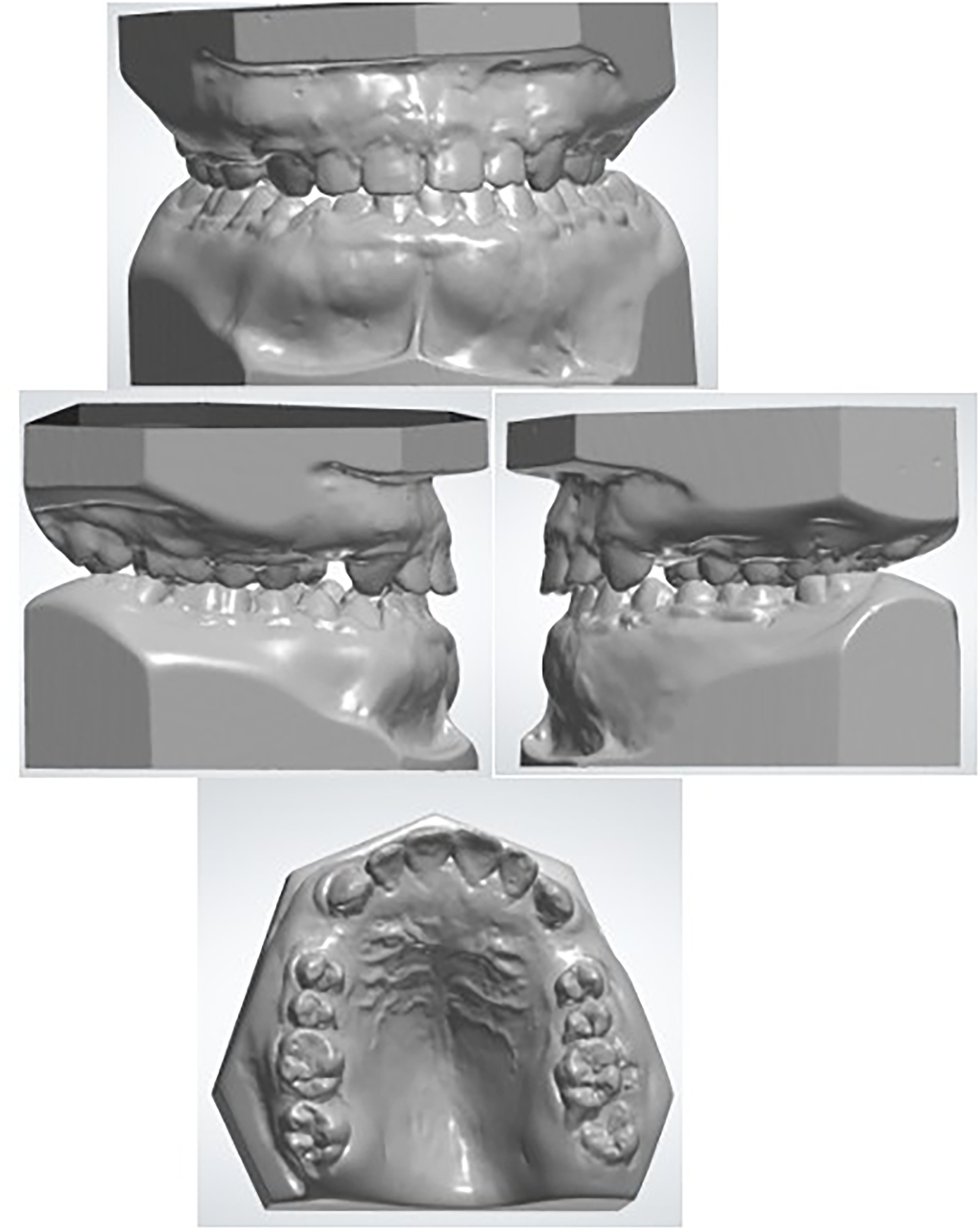
Pre-surgical orthodontic records demonstrating skeletal Class III malocclusion prior to orthognathic surgery. (A) Intraoral clinical photographs demonstrating class III incisor relationship during pre-surgical orthodontics. (B) Extra-oral clinical photographs demonstrating skeletal class III facial profile. (C) Orthodontic study models.
A sleep study at age 15 confirmed mixed sleep disordered breathing, with both severe obstructive and central sleep apnea. After careful consideration and discussion with the surgery psychologists, the patient's family and our maxillofacial team decided to proceed with early orthognathic surgery prior to completion of pre-surgical orthodontic treatment. This decision was influenced by numerous reasons: the anticipated prolonged duration of orthodontic treatment due to the underlying diagnosis of CMD, as well as the significant psychosocial impact on the patient's wellbeing caused by bullying at school. The family and patient were counseled regarding the potential for further growth and relapse of the malocclusion. The patient was also aware of the need for long-term retention and was provided with removable retainers.
Surgical Procedure
The planned surgical procedure included Le Fort 1 osteotomy with maxillary advancement and impaction. Although our patient had an element of mandibular prognathism, a mandibular setback procedure was not a viable option due to his obstructive sleep apnea. The risks and benefits of the proposed orthognathic surgery were thoroughly discussed with the patient as well as the specific risks in connection to CMD, notably the challenges of making surgical cuts and disimpacting the maxilla due to bony sclerosis, the risk of an unfavorable osteotomy split and the need to abort the procedure intraoperatively. The risk of maxillary necrosis due to poor blood supply post-operatively was also discussed. The pre-operative CT scan revealed narrowed anterior nasal passages caused by maxillary thickening with potential nasal intubation issues. The maxillofacial team explained that this could potentially be improved by carrying out refashioning of the nasal passages during maxillary osteotomy. The patient was advised a submental intubation would be required to allow both access to the nasal passages and predictable intubation.
Our patient underwent a Le Fort I maxillary advancement at age 16 to improve his symptoms, skeletal relationship and facial profile. In addition to standard dexamethasone and co-amoxiclav antibiotics, tranexamic acid was administered at induction. To aid soft tissue dissection 20mls of tumescent solution (containing hyaluronidase, triamcinolone and local anesthetic mixed with Hartman's solution) was infiltrated into the tissues. A submental incision with tunneling to the floor of the mouth lateral to the submandibular duct was undertaken to facilitate submental intubation with endotracheal tube passage. A layered maxillary sulcus incision was undertaken with the initial incision from upper right first canine to upper left canine to preserve a wide soft tissue cuff blood supply followed by a periosteal incision from first molar to first molar allowing wide posterior access in anticipation of any excessive bleeding.
In contrast to our standard practice, pterygoid dysjunction was performed next. A right-angle saw was utilized to form a small groove, and then pterygoid chisels were employed to complete the procedure. The rationale for early dysjunction was based on the possibility of excessive bleeding or difficulty in achieving a dysjunction. In both situations, the procedure could have been abandoned prior to more extensive surgery. Standard cuts were undertaken with numerous saw blade changes required due to the very thick and sclerotic consistency of the bone and a lack of any maxillary sinuses. Small volume persistent bleeding was noted, and copious irrigation was required to prevent bone heating. Entry to the lateral nasal wall and nasal floor was difficult due to bone thickening with some tears of the nasal mucosa.
In addition to the thickened bone, posteriorly unerupted wisdom teeth encased within the bone required to be sectioned within the planned osteotomy line. Final downfracture of the maxilla required the use of serial osteotomes angled along the osteotomy line and then posteriorly along the lateral maxilla toward the pterygoid plates. The density of the bone did not allow for tone change to guide the procedure such that once a wide enough gap was created, surgical spreader instruments were used to hinge the maxilla down anteriorly allowing for the final fracture under direct vision. Mobilization of the maxilla was achieved without difficulty, but bony interferences required diligent removal with burs to allow a 7 mm advancement, advancement, with differential impaction of 4 mm anteriorly and 2 mm posteriorly, and a 2 mm correction of the dental center-line to the patient's left (Figure 5).
Model surgery planning demonstrating the planned maxillary repositioning, including 7mm advancement, differential impaction of 4mm anteriorly and 2mm posteriorly, and a 2mm correction of dental center-line to the patient's left.
Refashioning of the nasal passages was undertaken via bone removal and required rotary drills to complete. The bony nasal septum was reduced initially followed by the development of bilateral nasal grooves. The grooves were deemed of adequate depth once a size 6 endotracheal tube could be passed along the groove floor with the maxilla handheld upward. Further cartilaginous nasal septum trimming was undertaken to ensure the septum was not buckled and then secured via polydioxanone suturing to the residual anterior nasal spine.
Maxillary fixation was achieved without issue using the KLS Martin 2.0 system with 4 L-shaped plates utilizing 7 mm titanium screws. Intraoral incisions were closed with 3.0 Vicryl Rapide sutures. The procedure concluded with closure of the submental lesion with 5.0 Ethilon sutures. Post-operative care included a 5-day course of co-amoxiclav, pain management, a soft diet, and the use of 0.2% chlorhexidine mouthwash for 14 days. Surgical blood loss was estimated to be 1100mls and predominately related to persistent low-flow bleeding from the bony tissues. No transfusion was required, but a further tranexamic acid dose was administered.
Implant Placement
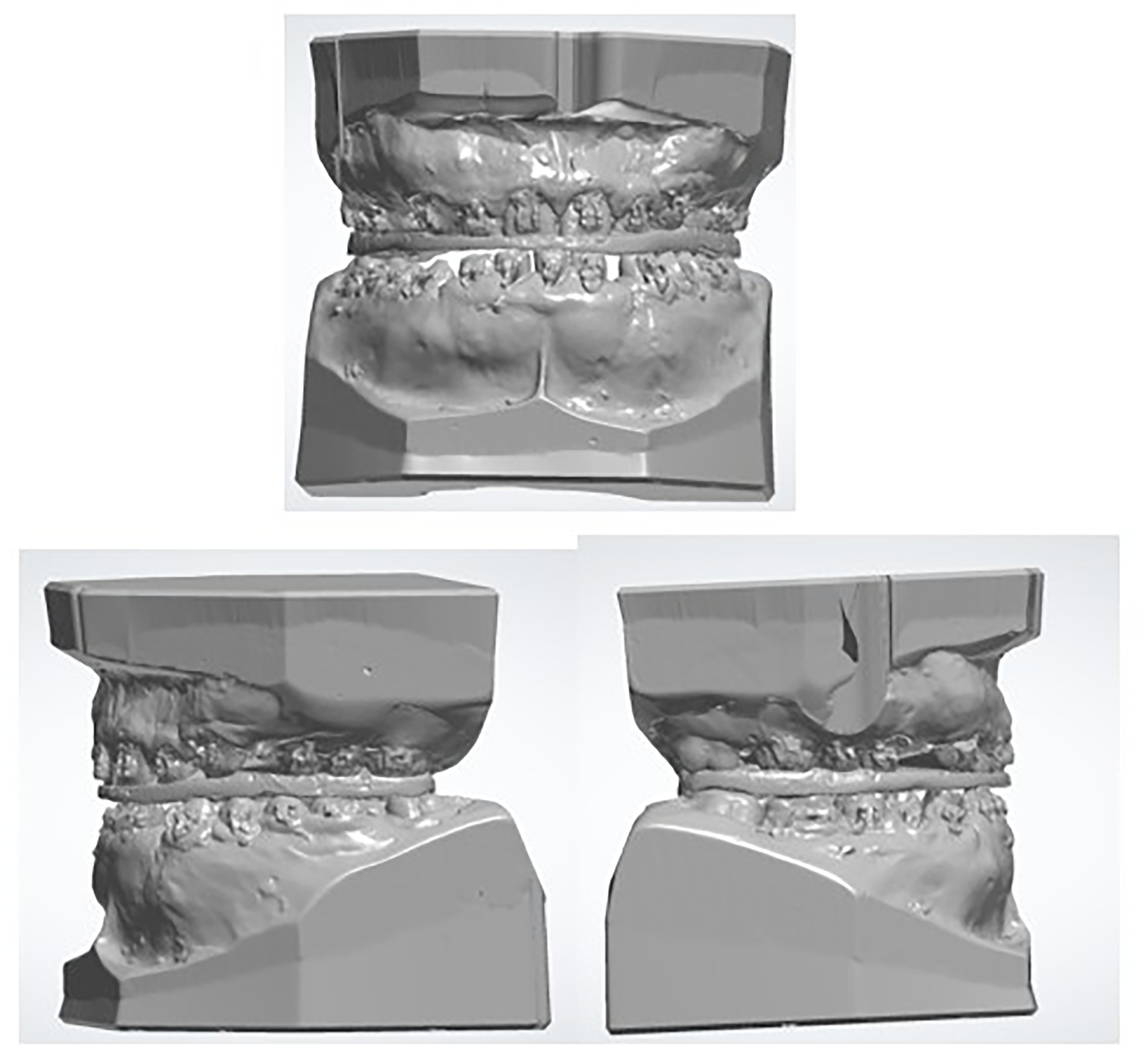
The patient completed fixed orthodontic treatment in mid-2021, at 18 years of age and was subsequently referred to the restorative department for placement of 2 Straumann dental implants adjacent to UR3 and UR4, and UL3 and UL4 due to the presence of residual space (Figure 6). The implant on the upper right was successful; however, the initial upper left implant exfoliated and was re-attempted after 8 weeks. At the 3-month follow-up, it was found that the upper left implant had failed for a second time. The repeated implant failure is likely to be related to the bone biology associated with CMD. Given the potential of another unsuccessful outcome, it was agreed with the patient that a further implant would not be attempted, and a resin-bonded bridge was used to replace the space between UL3 and UL4 instead. The implant on the upper right was restored with a screw-retained zirconia crown.
Post-orthodontic study models obtained at completion of fixed appliance treatment, demonstrating residual spacing in the upper arch prior to restorative treatment with dental implants.
Results
The patient recovered well from the Le Fort I osteotomy and reported satisfaction with his function and facial profile. At 5-year follow-up, his occlusion remained relatively stable with no signs of abnormal bone regrowth (Figures 7 and 8). He reported improved breathing, eating, and confidence. He noted a particular improvement in breathing through his right nostril following the surgery.

Five-year post-operative clinical and orthodontic outcomes following Le Fort I osteotomy in a patient with CMD. (A) Extra-oral clinical photographs showing frontal view at rest, smiling view, and lateral facial profiles. (B) Intraoral photographs demonstrating buccal views, anterior views, maxillary arch and mandibular arch relationships at follow-up. (C) Orthodontic study models obtained at 5-year follow-up demonstrating stable occlusion with no evidence of relapse. CMD, craniometaphyseal dysplasia.
Post-surgical lateral cephalogram and tracing.
Discussion
Surgical management of CMD presents unique challenges due to the abnormal physiology of the craniofacial bone. Hyperostotic craniofacial bones are denser, more brittle and poorly vascularized than normal bone, thereby increasing the risk of post-operative complications, impaired healing and unpredictable surgical outcomes.
In our case, detailed imaging including CT and MRI scans was crucial in evaluating the extent of hyperostosis and nasal passage narrowing. Although there is no definitive cure for CMD, both surgical and medical interventions can help manage and reduce some of its physical manifestations. Medical treatments such as low-calcium diets and calcitriol have been used to modulate bone remodeling but often yield variable and limited results. 14
Although complex, surgical intervention can offer functional and psychological benefits, as seen in our patient. The quality of life can be enhanced by improving occlusion, breathing, and facial profile. In this case, the functional and psychological burden justified early surgical intervention prior to completion of orthodontic treatment. It was also recognized that the rate of orthodontic tooth movement was going to be slower due to the increased bone density, prolonging the course of treatment. 15
Reports of orthognathic surgery in patients with CMD are exceedingly limited, largely due to the rarity of the condition and the significant surgical challenges posed by the abnormal bone physiology.
One of the few reported cases of orthognathic surgery in CMD is described by Chan et al, 16 who reported simultaneous Le Fort I and Le Fort III osteotomies in a 19-year-old patient with severe midface hypoplasia and obstructive sleep apnea. In that case, surgery was performed in a skeletally mature patient to address “facial deformity” and improve airway function. Due to the increased bone density and sinus obliteration, the authors noted the technical challenges associated with marked craniofacial sclerosis, including the need for repeated intraoperative changes of ultrasonic osteotomy tips to make the necessary osteotomy cuts.
In contrast, our case demonstrates earlier multidisciplinary escalation during adolescence, with surgical timing influenced not just by skeletal discrepancy but also by progressive functional impairment, including mixed obstructive and central sleep apnea, and psychosocial distress. Additionally, orthodontics tooth movement in sclerotic bone was markedly reduced, which further influenced treatment planning and duration. The functional and psychosocial intervention expands on the management described by Chan et al, demonstrating that orthognathic intervention in CMD may be considered prior to skeletal maturity in carefully selected cases. This case therefore adds to the limited literature by highlighting the role of earlier, function-driver intervention in CMD.
Reports of orthognathic surgery in CMD patients remain exceedingly rare due to the complexities of craniofacial sclerosis and surgical risk. This case report represents one of the few documented instances of successful orthognathic surgery in CMD, with a 5-year follow-up demonstrating stable occlusion and sustained functional improvement. In addition to this, there are no studies reporting placement of dental implants in these patients, likely due to the anatomical challenges involved, making implant placement unpredictable.
The high osteogenic potential of the bone complicates the surgical management of CMD. Previous reports have highlighted the rapid regrowth of bone following surgical intervention. In one case, facial recontouring resulted in significant bony regrowth within just 6 weeks post-operatively, to the extent that it was speculated the surgical procedure may have inadvertently stimulated new bone formation. 15 In contrast, our case did not demonstrate such early post-operative regrowth, possibly due to differences in surgical timing, the nature of the osteotomy, or pre-operative planning. This highlights the importance of tailored, multidisciplinary planning in mitigating such complications.
Other literature further highlights the risks associated with craniofacial surgeries. One report described surgical interventions in a 20-month-old which included bifrontal craniectomy with orbital roof resection and cranial nerve decompression. The patient required repeated surgery due to restenosis at age 5 and by age 8, the symptoms worsened resulting in foramen magnum compression, hearing, and visual impairments. 17 This case highlights the risk of progressive bone regrowth, a hallmark of CMD's active bone turnover.
Similarly, in another case report, authors reported post-operative blindness following optic nerve decompression, potentially due to compromised vascular supply to the optic nerve from the surrounding hyperostotic bone. 18
This case, together with that reported by Chan et al, demonstrates that orthognathic procedures can be successfully undertaken in patients with CMD, when supported by careful multidisciplinary planning and appropriate intraoperative adaption to sclerotic bone. In our case, standard orthognathic procedures were possible despite the increased bone density. Although intraoperative blood loss was significantly more than usually expected, this was effectively managed with local hemostatic measures and tranexamic acid, without the need for blood transfusion. There were no post-operative complications such as wound infections, bone necrosis, or evidence of pathological bone regrowth during follow-up. Intraoperatively, copious irrigation was considered essential to reduce the risk of bone overheating during orthognathic surgery.
From an orthodontic perspective, time in fixed appliances was extensive, and treatment took close to 5 years. The authors acknowledge that the occlusion is not perfect, with a small center-line discrepancy and posterio unilateral crossbite, with no associated displacement. However, a stable and functional occlusion was achieved, with our patient being pleased and satisfied with the overall treatment outcomes.
There is a wide variability in the presentation of patients with CMD, their functional impairments and timing of interventions across reported cases. This highlights the need for further research on the surgical management of these patients to better define optimal intervention timing and management strategies in CMD.
Conclusion
The presented case report describes a multidisciplinary approach to treating a young patient with CMD with a focus on orthognathic management. We have demonstrated that orthodontics and orthognathic surgery can be safely provided for this cohort of patients with careful multidisciplinary team planning. In addition, the results of the surgical intervention have continued to be stable after 5 years.
Footnotes
Ethical Statement
Our institution does not require ethical approval by a research ethics committee for reporting individual cases.
Informed Consent / Patient Consent
Written informed consent was gained from the patient for publication of information and images.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.