
Abstract
Objective
This investigation aimed to quantify the prevalence and associated risks of clinically significant ocular outcomes (refractive errors, strabismus, amblyopia, and papilledema) across 4 subtypes of nonsyndromic single suture craniosynostosis (NSCS) and compare these findings against those of matched controls.
Design
This investigation was executed as a large-scale, retrospective cohort study using deidentified electronic health record data, performed in compliance with STROBE guidelines.
Setting
This investigation used aggregated, geographically diverse U.S. patient data within the TriNetX Research Network.
Participants
The sample consisted of 5060 NSCS patients categorized by suture type (sagittal, metopic, unilateral coronal, lambdoid), inclusive of all surgical statuses (unstratified). Patients were matched 1:1 with a control patient using propensity scores from age (>5 years), sex, and race.
Interventions
Analysis identified differential rates of ocular abnormalities in patients with an NSCS diagnosis compared with nonaffected controls.
Main Outcome Measure
Risk ratios were calculated based on specific ICD-10-CM-coded ocular abnormalities.
Results
Unilateral coronal synostosis (UCS) demonstrated the highest risk for refractive disorders, strabismus, and amblyopia. Metopic synostosis (MCS) was also associated with an increased risk of refractive disorders and showed a significant association with congenital eyelid malformations. Sagittal synostosis (SCS) exhibited the lowest overall risk, though significant associations were observed for hyperopia and papilledema.
Conclusions
NSCS is associated with increased ocular morbidity with all suture patterns. UCS carries the highest burden, MCS is associated with refractive disorders and congenital eyelid malformations, and SCS shows increased risks of hyperopia and papilledema. These findings support early and continued ophthalmologic surveillance for all affected children.
Introduction
Craniosynostosis (CS) is the premature fusion of one or multiple cranial sutures in newborns and infants. CS has an estimated worldwide prevalence of 3.1 to 6.4 per 10 000 live births and is broadly classified as syndromic or nonsyndromic. Syndromic CS is characterized by a recognizable constellation of associated clinical features, often with an underlying genetic etiology, whereas nonsyndromic CS (NSCS) represents isolated premature suture fusion that may involve a single suture or multiple sutures. 1 NSCS is more prevalent and occurs in approximately 1 in 2000 to 2500 births. 2 This premature suture closure restricts normal growth of the skull, leading to characteristic cranial deformities, orbital malformations, and potential adverse effects on the central nervous system, including the visual pathway.2,3 Loss of vision in NSCS may result from multiple factors, such as optic neuropathy from chronically elevated intracranial pressure (ICP) or amblyopia due to untreated strabismus and refractive errors.2,3 Early diagnosis and intervention are essential to identify and manage elevated ICP, which may impact visual development as the critical period for development extends through 7 to 8 years of age.1,4
Prior literature demonstrates that morbidities vary between distinct patterns of craniofacial and orbital distortion, and that 4 common subtypes of NSCS, including sagittal synostosis (SCS), metopic synostosis (MCS), unicoronal synostosis (UCS), and lambdoid synostosis (LCS), are associated with distinct patterns of ocular disorders. 1 UCS, which causes anterior plagiocephaly, is consistently associated with the highest burden of ocular pathology among the NSCS subtypes.1,5 MCS, which causes trigonocephaly, is caused by premature metopic suture fusion, and traditionally leads to fewer ocular abnormalities than UCS due to a more symmetric pattern of skull deformation.1,6 However, prior literature also reports elevated rates of hyperopia, astigmatism, amblyopia, and strabismus in MCS, suggesting that symmetric skull deformations can nonetheless impact refractive development.6–8 SCS, which leads to scaphocephaly, is the most common subtype of NSCS and has also been regarded as less severe due to its effects lacking obvious orbital asymmetry, yet studies still highlight consequences including abnormal visual attention shift.3,7,9,10
Despite the clear risks and emerging findings on ocular involvement in NSCS, large-scale epidemiological studies that compare visual outcomes across all 4 major single-suture CS subtypes (UCS, MCS, LCS, SCS) against matched controls have not been conducted.11,12 Prior studies have often mixed syndromic and nonsyndromic cases and have also been limited by their small sample sizes, heterogeneous populations, and inconsistent follow-up, which has left a lack of a definitive understanding of the true subtype-specific risk profiles.1,13–15 To fill this critical research gap and to better inform clinical screening and NSCS management protocols, this study leverages a large, national administrative database to analyze and to compare the prevalence of clinically significant ocular disorders across all 4 major single-suture NSCS subtypes relative to a matched control from the general pediatric population.
Methods
Study Design and Data Source
A retrospective cohort study was conducted and reported in accordance with STROBE guidelines, utilizing information from the TriNetX Research Network from Cambridge, MA. TriNetX is a global health-research platform that aggregates deidentified electronic health-record data from over 160 million patients across multiple health-care organizations. Data extraction for this study was performed on May 12, 2025, and focused exclusively on patients from the United States. The study was approved as exempt from institutional review board approval, as it involved only deidentified data, without the requirement of subject consent.
Study Population
ICD-10-CM coding for suture-specific, NSCS was used to identify patients whose information would qualify for analysis. Patients were divided into cohorts based on NSCS subtype, including metopic (code: Q75.03), sagittal (code: Q75.01), unilateral coronal (code: Q75.021), and lambdoid (code: Q75.04) synostosis. We did not do an analysis for kids with bilateral coronal (code: Q75.02) since they are often associated with syndromic synostosis. Furthermore, to ensure the exclusion of syndromic cases, patients with a diagnosis of syndromic CS (codes: Q87.0, Q75.1, Q75.05, and Q75.4) were removed. An age-, sex-, and race-matched control group consisting of patients from the general population was also identified by selecting patients who had presented for an ambulatory visit for immunizations. Participants were not stratified according to the receipt, timing, or technique of surgical intervention. While surgical procedure codes exist within the network, the operative details or the exact age of the patient at intervention, could not be standardized across the diverse organizations contributing to the database. This study only included patients who were 5 years of age and older.
Outcomes
The primary outcome was the presence of various visual refractive errors, and this was defined using ICD-10-CM codes for myopia (code: H52.1), hyperopia (code: H52.0), astigmatism (code: H52.2), and anisometropia (code: H52.31). Aniseikonia (code: H52.32) was excluded. Collectively, these disorders were grouped under “disorders of refraction and accommodation” (code: H52).
Secondary outcomes evaluated included:
Orthoptic conditions, including esotropia (code: H50.0), exotropia (code: H50.1), heterotropia (codes: H50.3 and H50.4), vertical strabismus (code: H50.2), and paralytic strabismus (code: H49). Amblyopia (code: H53.0), categorized under “visual disturbances.” Structural abnormalities, including disorders of the orbit (code: H05), congenital malformations of the eyelid (code: Q10.3), papilledema (code: H47.10), and disorders of the lacrimal system (code: H04).
Statistical Analysis
One-to-one greedy nearest neighbor propensity score matching was employed to minimize selection bias and to control for confounding variables. A caliper of 0.1 pooled standard deviations of the logit propensity scores was used in the matching and included the following baseline variables that were defined by their ICD-10 CM codes: age at index, current age, sex, and race. Chi-square tests for categorical variables and t-tests for continuous variables were used to compare baseline variables, with the balance assessed using a standardized mean difference (SMD) threshold of <0.1.
Additionally, risk ratios (RRs) at 95% confidence intervals for the association between each CS subtype and the presence of ocular outcomes. Kaplan–Meier curves were constructed to visualize the cumulative incidence of the outcomes. Log-rank tests were used to compare differences between cohorts. Subanalyses were not performed. P-values less than .05 were considered statistically significant. All statistical analyses were performed using the online analytical platform from TriNetX.
Results
Participants and Descriptive Data
Electronic health record information from 5060 patients with CS were identified in the 4 subtypes NSCS using the TriNetX network. These cohorts consisted of MCS (n = 1651), UCS (n = 320) (Table 1), SCS (n = 2935) and LCS (n = 154) (Table 2).
Ocular Outcomes and Risk Ratios for Unilateral Coronal Synostosis (UCS) and Metopic Synostosis (MCS) Compared to Matched Controls.
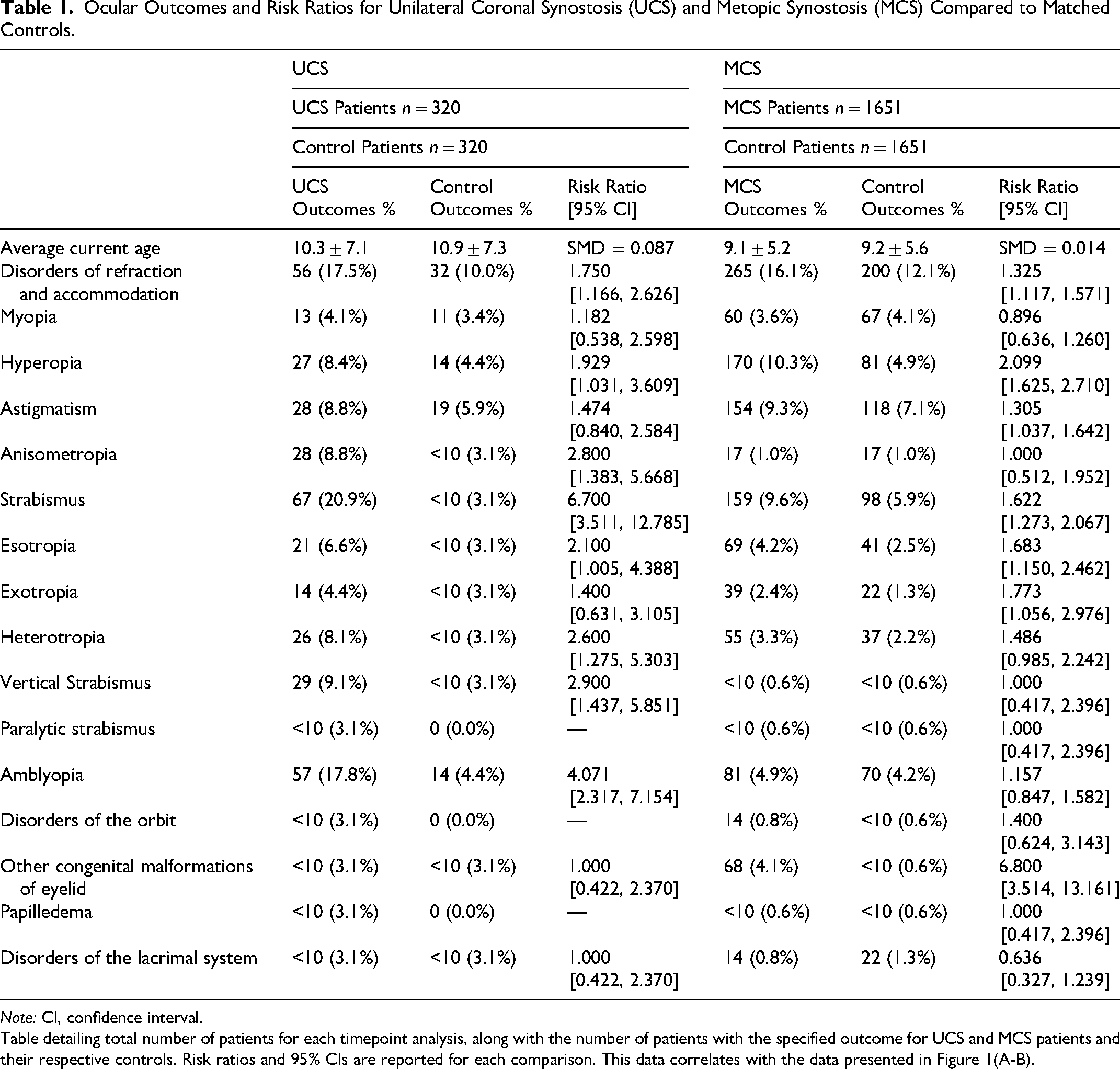
Note: CI, confidence interval.
Table detailing total number of patients for each timepoint analysis, along with the number of patients with the specified outcome for UCS and MCS patients and their respective controls. Risk ratios and 95% CIs are reported for each comparison. This data correlates with the data presented in Figure 1(A-B).
Ocular Outcomes and Risk Ratios for Lambdoid Synostosis (LCS) and Sagittal Synostosis (SCS) Compared to Matched Controls.
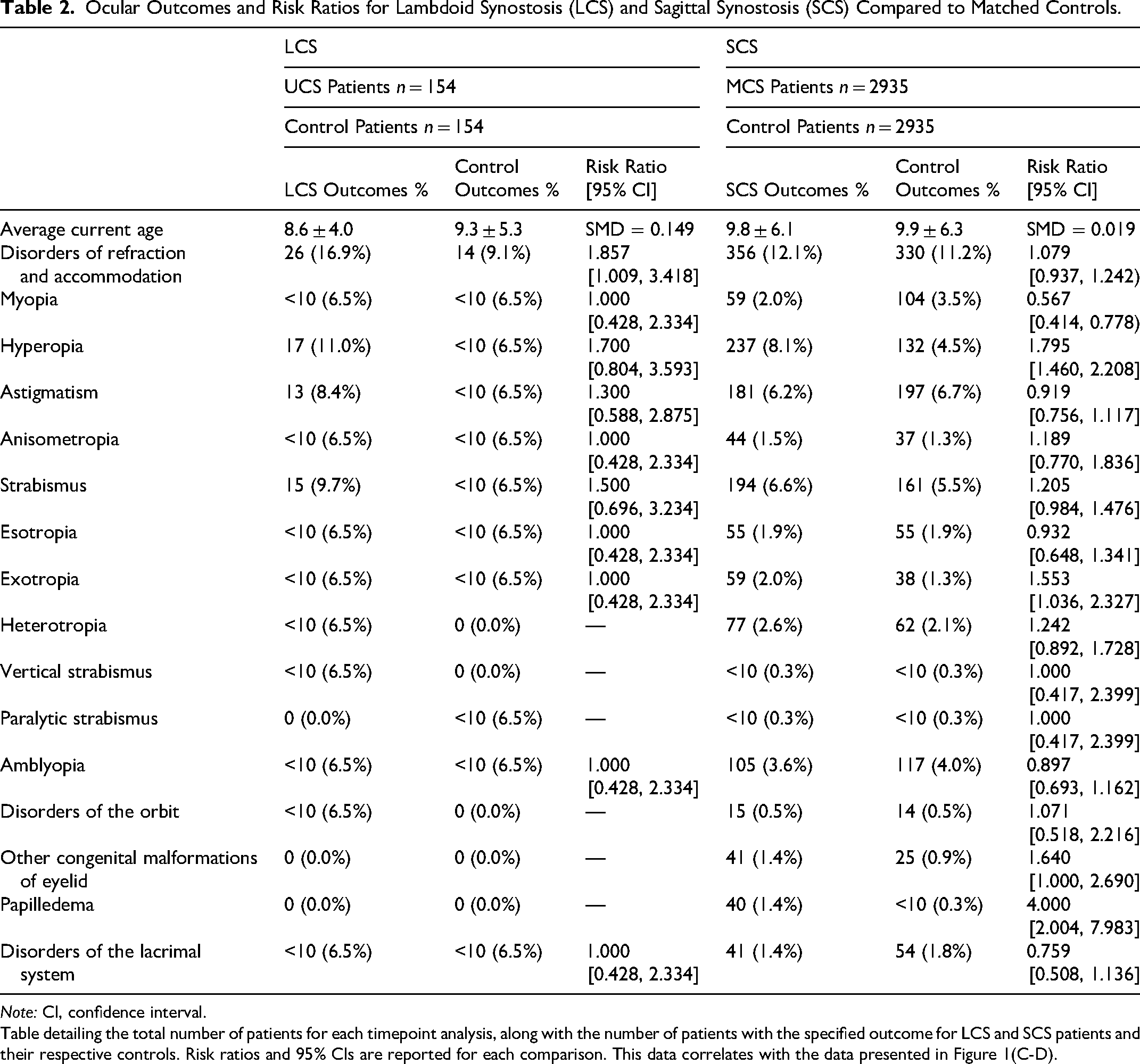
Note: CI, confidence interval.
Table detailing the total number of patients for each timepoint analysis, along with the number of patients with the specified outcome for LCS and SCS patients and their respective controls. Risk ratios and 95% CIs are reported for each comparison. This data correlates with the data presented in Figure 1(C-D).
Each CS subtype cohort was matched 1:1 with a control group from the general population using propensity score matching. This matching was based on demographics, that included age at diagnosis, current age, sex, and race. After matching, each cohort was well-balanced, with SMDs that were less than 0.1 for all covariates.
Descriptive data also revealed that patients with CS were largely male in the SCS (71.8%) and MCS subtypes (71.4%) and were largely female in the UCS subtype (65.0%). Racial compositions were comparable across all the matched groups. There were no missing data for key demographic or outcome variables in the matched cohorts.
Outcome Data
Across all subtypes of CS, the prevalence of disorders of refraction and accommodation ranged from 9.4% to 17.5% (Figure 1(A-D)). The highest prevalence of these disorders was observed in patients with UCS (17.5%) and LCS (16.9%). The prevalence of strabismus ranged widely from 6.6% (SCS) at the low end to 20.9% (UCS) at the high end. Amblyopia was also present in 3.6% to 17.8% of patients, with the highest rate of amblyopia seen in UCS. Papilledema was overall a rare visual finding but had significantly elevated rates in patients with SCS (1.4%) compared to their matched controls (0.3%). Full outcomes data for each cohort are presented in the respective results tables.
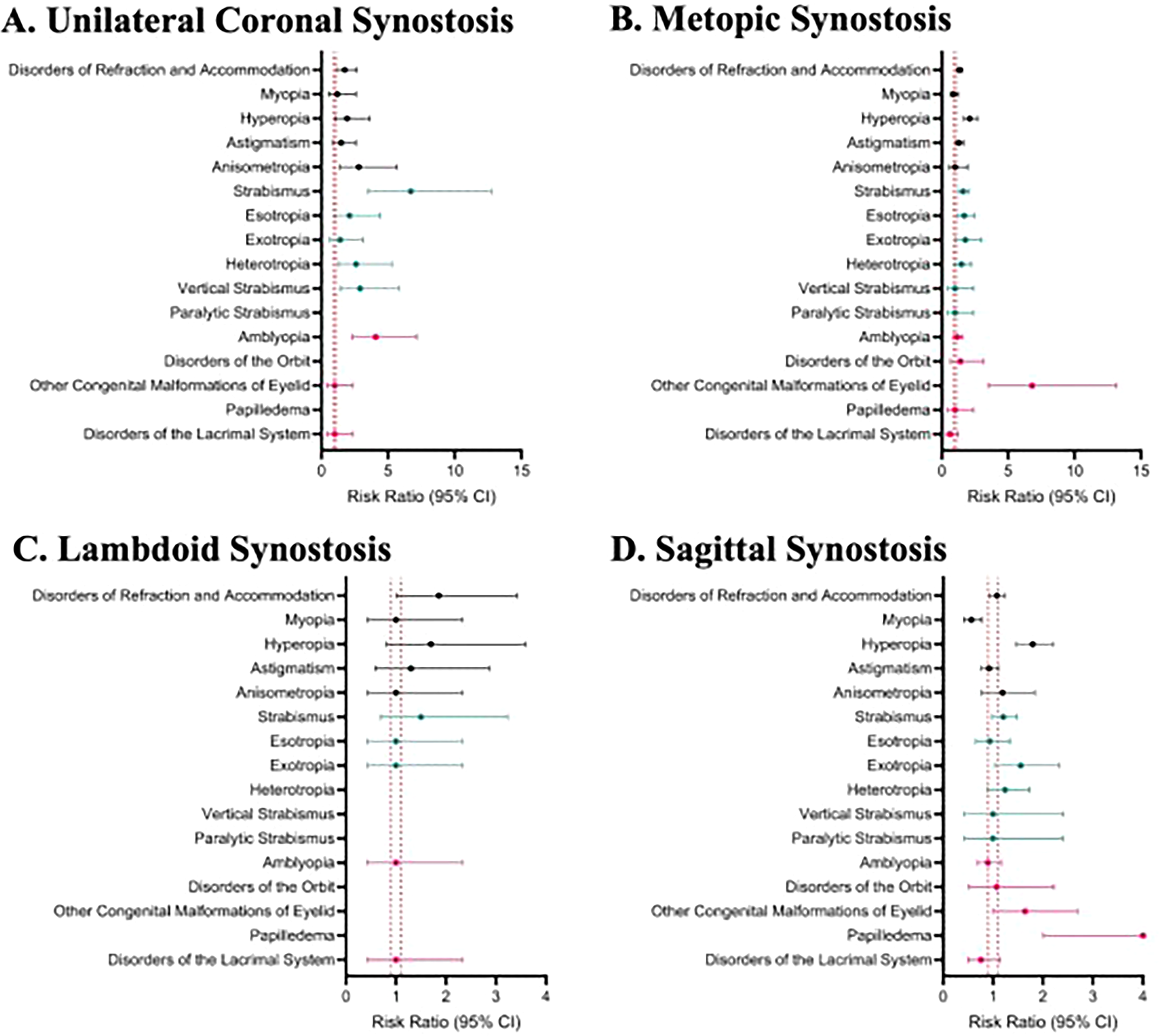
(A-D). Forest plot of risk ratios for ocular outcomes in unilateral coronal, metopic, lambdoid, and sagittal synostosis.
Main Results
Compared to the matched control group, patients with UCS had a significantly elevated risk for multiple ocular anomalies. For example, the risk of strabismus in UCS was almost 7 times higher than in their controls (RR 6.70, 95% CI 3.51 to 12.79), and the risk of amblyopia was over 4 times more likely (RR 4.07, 95% CI 2.32 to 7.15). MCS was also associated with elevated risks, specifically for strabismus (RR 1.62, 95% CI 1.27 to 2.07), hyperopia (RR 2.10, 95% CI 1.63 to 2.71), and eyelid malformations (RR 6.80, 95% CI 3.51 to 13.16). Findings for SCS showed a significantly elevated risk for hyperopia (RR 1.80, 95% CI 1.46 to 2.21). SCS also showed a substantially increased risk of papilledema (RR 4.00, 95% CI 2.00 to 7.98). The LCS cohort was the only group where most outcome trends were nonsignificant, though the risk of refraction disorders were higher than in controls (RR 1.86, 95% CI 1.01 to 3.42). These results are visualized in the forest plots below.
Other Analyses
No formal interaction testing was performed. However, sensitivity analysis, excluding rare outcomes like paralytic strabismus or papilledema, did not significantly alter estimates for the main effect. Additional analysis based on sex, race, or age was limited by sample size, and this was particularly evident in the UCS and LCS cohorts.
Discussion
This large, national, multicenter retrospective study comprehensively investigated the long-term ophthalmologic sequelae across 4 major subtypes of NSCS compared to patients from matched controls. The findings from this investigation confirm that there are substantial subtype-specific burdens on ocular pathology. The findings from UCS and MCS showed the greatest rates of ocular abnormalities. Furthermore, while SCS is generally associated with fewer ocular sequelae than other forms of NSCS, our findings of elevated papilledema in SCS reinforce the importance of monitoring SCS patients for intracranial hypertension, which is a known risk in scaphocephaly. These findings refine the perception of SCS as ophthalmologically benign by demonstrating a disproportionately elevated susceptibility to optic nerve pathology.1,2,10,14
Prior literature indicates that orbital asymmetry developing from UCS can lead to structural changes, such as the excyclorotation of the muscle cone, frequently results in strabismus (prevalence ranging from 19% to 71%) and refractive errors.1,16,17 This type of cranial distortion causes a characteristic excyclotorsion syndrome in the orbit contralateral to the prematurely fused suture, and presents with V-pattern strabismus, inferior oblique overaction, and high rates of aniso-astigmatism.16,18,19 This investigation confirmed that there is severe ocular morbidity associated with UCS, and this is consistent with findings from extensive prior literature.4,17 UCS is known to be associated with ipsilateral frontal retrusion, superolateral orbital rim elevation, and contralateral compensatory growth, resulting in marked craniofacial and orbital asymmetry.18,20 Within this context, we observed a nearly sevenfold increased risk of strabismus and over fourfold increased risk of amblyopia in patients with UCS. This outcome is significantly higher than those reported in the general population, where the prevalence of strabismus in a healthy pediatric population is between 1.9% and 3.2%.21–23 Conversely, studies on UCS consistently report the rate of strabismus as high as 50% to 71%.15,17 Specifically, these visual effects often manifest as pseudo-superior oblique palsy, V-pattern strabismus, and ocular torticollis, which are strongly associated with abnormal positioning of extraocular muscle insertions in a dysmorphic orbit.5,19 Furthermore, our findings reinforce prior observations that refractive errors, particularly astigmatism, preferentially affect the orbit contralateral to the fused suture, consistent with patterns reported in the literature.4,16,17
MCS produces a distinctive ocular risk profile in the cohort from our study and corroborates prior research that indicates elevated risks for refractive errors such as hyperopia, challenging the view that MCS is a comparatively mild craniofacial deformity.7,8 While UCS is characterized by asymmetry and unilateral deformity of the orbits, MCS is characterized by a symmetric, wedge-shaped narrowing of the frontal bones, including trigonocephaly and hypotelorism. 6 The consequence of these malformations is the reduction in volume and associated frontal narrowing which may restrict globe elongation, resulting in hyperopia, as observed in the data from this study. 24 Additionally, medial angulation of the orbit can affect the force vectors of extraocular muscles and lead to mechanical misalignments that contribute to the significantly increased risk of strabismus that we identified (Table 2).
Furthermore, congenital eyelid malformations were markedly more prevalent in children with MCS and demonstrated one of the largest effect sizes across CS subtypes. Eyelid malformations and malposition are recognized contributors to corneal exposure and ocular surface disease in CS, and in severe cases may necessitate protective interventions such as tarsorrhaphy to preserve corneal integrity. 25 The existing literature on eyelid malformation in patients with MCS is limited, with most prior studies focusing on bony orbital and cranial vault abnormalities rather than soft tissue development in periocular structures. Despite the high prevalence of risk factors associated with MCS, the rate of diagnosed amblyopia was not observed to have been elevated. This finding may reflect a potentially protective benefit of MCS as compared with other types of NSCS. Overall, visible trigonocephaly related to MCS should prompt early clinical recognition and specialist referral to facilitate appropriate ophthalmic surveillance and multidisciplinary evaluation, although the extent to which surgical intervention modifies visual outcomes in this population remains uncertain. 8
SCS has also been described as ophthalmological benign relative to other subtypes in prior literature, and this is primarily due to the absence of gross orbital deformities seen in SCS.2,3 However, data from the present study demonstrate a statistically significant increase in hyperopia, challenging the notion that posterior cranial deformities are uniformly ophthalmologically benign. Hyperopia was the only refractive or motility outcome to reach statistical significance in this cohort. Often frontal bossing can be observed in these patients secondary to compensatory growth of the anterior aspect of the cranium, 26 which may explain the findings seen here. Although scaphocephalic deformity is associated with compensatory elongation in the anterior–posterior axis, it is also characterized by restricted transverse growth and compensatory vertical growth. These malformations of the cranial vault have implications for the development of orbital dimensions and shape, resulting in a restrictive environment that inhibits normal development of the globe. The mechanisms of how these changes impact globe development are not completely understood, however, the ophthalmic consequences of SCS are likely not merely incidental and may be mechanically linked to altered vectors of cranial growth and ICP dynamics.9,10
In addition to these structural and refractive changes associated with SCS, the identification of papilledema in our SCS cohort underscores a critical finding indicative of intracranial hypertension. Unlike the structural orbit changes discussed above, papilledema likely results directly from a mismatch between increasing brain volume and restricted cranial vault growth, leading to elevated cerebral spinal fluid pressure that is transmitted along the sheath of the optic nerve. This finding is clinically important because while refractive errors can be managed with glasses, papilledema represents potential optic nerve atrophy and puts the patient at risk for permanent visual loss if the underlying increased ICP is not relieved.2,3,27 Therefore, the presence of papilledema in patients with SCS should not be viewed as a routine ophthalmic variance but rather as an indication for surgical urgency. Detection of papilledema should prompt urgent ophthalmic and neurosurgical evaluation for elevated ICP, with consideration of appropriate medical and or surgical management to reduce the risk of permanent visual impairment.
LCS is the rarest form of NSCS and typically accounts for less than 5% of all NSCS cases.11,12 As such, the rarity of LCS has contributed to a historic shortage of robust clinical data.11,12 Prior literature has also been limited to small case series or confounded by difficulty in diagnosing or distinguishing true synopsis from deformational posterior plagiocephaly, which is more prevalent.9,18 These limitations have led to mixed results and the frequent assumption that LCS is not commonly associated with ophthalmologic pathologies due to LCS's posterior location. Our study represents the largest LCS cohort published to date (n > 200) and challenges this view. The data from this study demonstrates a statistically significant increased risk for hyperopia and general refractive disorders in patients with LCS (Table 2). We hypothesize that the unique pathophysiology of LCS leads to the development of anterior visual sequelae. Specifically, the premature fusion of the lambdoid suture creates a rotational torque on the base of the skull, which can affect the petrous portion of the temporal bone. 5 This torsional force can transmit anteriorly to the orbits, altering the orbit dimensions and inhibiting axial elongation required for proper emmetropization. These findings might suggest that LCS is a complex cranial-based pathology with potential risks to visual development. This underscores the necessity for comprehensive ophthalmologic screening in patients with LCS.
Another important consideration is that patient cohorts were not stratified by surgical status. In the treatment of NSCS, both the timing of intervention and the specific surgical technique, such as endoscopic versus open cranial vault remodeling, can meaningfully influence outcomes. Because our database includes patients across various stages of care, our findings do not assess the efficacy of any single treatment paradigm. Rather, they capture the cross-sectional, real-world burden of ocular anomalies across single-suture NSCS under heterogeneous management conditions.
The results from this study underscore the necessity to implement comprehensive and universal ophthalmologic screenings for all children diagnosed with single-suture NSCS, irrespective of which suture is involved, following guidelines such as those published by the American Academy of Pediatrics. 28 Indeed, early detection and correction of embryogenic disorders and refractive errors like strabismus are crucial for achieving long-term visual function and minimizing the progression of ocular disorders associated with the synostosis. 29
Limitations and Future Directions
Because this was a large retrospective study that relied on administrative claims data, the findings of this study are constrained by the fidelity of the ICD-10 codes, which could potentially lead to a misclassification bias. The specific CS subtypes and the secondary visual outcomes are subject to undercoding, miscoding, or variations in institutional diagnostic standards. For example, asymptomatic refractive errors may be omitted from coding if they do not directly alter clinical or surgical management, leading to an underestimation of certain risks.
Furthermore, surveillance bias is a notable confounding variable in this database design, as children with CS receive care from specialized craniofacial teams, which may increase detection of subtle or asymptomatic conditions, such as mild astigmatism or early strabismus, relative to controls. As a result, observed differences between cohorts may partly reflect differential screening intensity rather than true differences in underlying incidence.
Moreover, a direct causal relationship between surgical intervention and the mitigation of ocular risks cannot be established because critical variables, such as the severity of cranial deformity, specific surgical techniques used, or timing of interventions were not uniformly available in the TriNetX database. As such, participants were not distinguished based on whether they had received medical or surgical intervention for their NSCS at the time by which they reported ocular comorbidities. There was also no direct correlation between structural orbital findings demonstrated in morphometric studies and clinical outcomes in our patient sample.
Future prospective studies that use advanced imaging, such as volumetric rendering CT or MRI, can correlate skull-based dysmorphology with objective measures of ocular outcomes, such as visual-evoked potentials, and these types of studies can help further explain the underlying biomechanical pathways responsible for varied risks of visual disorders in CS.2,5
Conclusion
Infants with nonsyndromic single-suture CS have a significantly increased risk of ophthalmologic morbidity compared to the general population. The risk profile is distinct for each subtype of CS, with unicoronal synostosis presenting the highest risk for strabismus and amblyopia, while MCS presenting an elevated risk for refractive errors of vision and congenital eyelid malformations. Most critically, the long-held perception that sagittal CS is ophthalmological benign is challenged by the findings from this study that show that there is a significantly increased risk for hyperopia and papilledema, which is a proxy for the serious finding of increased ICP. This investigation suggests that all types of suture fusions can carry subtle, vision-threatening risks. As such, these findings support continued early rigorous and universal ophthalmological surveillance for all children with CS, irrespective of which suture is fused. This will ensure timely diagnosis and treatment to prevent more severe or permanent visual impairment.
Footnotes
Acknowledgments
The authors would like to state that no external support or contributions from individuals outside of the authorship team were used during this research.
Ethical Statement
The authors have adhered to the highest standards of academic integrity and confirmed that this manuscript is original, not published elsewhere, and not under consideration by another journal. This research abided by all ethical guidelines for human subjects research, contains no plagiarized material or unauthorized content from third parties. All authors have reviewed the final version and agreed to its submission.
Author Contribution Statements
Eric Xu and John Ha led the project and conducted the majority of the data collection, first draft and editing for the manuscript. Charles Guo conducted data analysis, determined the results, and developed the figures and tables. Georgia Babb contributed to the writing and editing of the manuscript and the consolidation of references. Howard Wang and Krystal Tomei served as medical faculty advisors to the project and reviewed the manuscript for medical accuracy, writing style, and clinical relevance. All authors contributed to the production of this manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Clinical and Translational Science Collaborative of Northern Ohio, funded by the National Institutes of Health, National Center for Advancing Translational Sciences, Clinical and Translational Science Award grant (Grant No. UM1TR004528).
Declaration of Conflicting Interests
The authors do not have any financial disclosures. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.