
Abstract
Objective
To assess maxillary growth in subjects with an isolated cleft palate at 5 and 10 years of age.
Design
This was a retrospective study.
Setting
Subjects were treated at 2 hospitals within a cleft center in the United Kingdom.
Participants
The study involved consecutive subjects with an isolated cleft palate, with no associated syndrome. Subjects with Pierre Robin sequence were included in the study.
Interventions
Orthodontic study models were taken at 5 and 10 years of age, as part of a nationally agreed audit process.
Main Outcome Measures
The 5-Year Index and GOSLON Yardstick were used to assess dental arch relationships.
Results
Records were available for 124 subjects. There was no statistically significant difference between the 5-Year Index and GOSLON Index scores.
Conclusions
Our results show that for patients with an isolated cleft palate, study model scores to assess dental arch relationships and indicate maxillary growth, recorded at 5 years give a good reflection of the outcome at 10 years.
Introduction
Cleft palate is a congenital craniofacial anomaly resulting from the incomplete fusion of the palatal shelves during embryonic development, leading to a discontinuity in the hard and/or soft palate. This defect can occur in isolation or in conjunction with a cleft lip and is associated with functional impairments in feeding, speech, and maxillofacial growth. The etiology of cleft palate is multifactorial, involving genetic predisposition and environmental influences. Approximately 54.8% of cleft palate cases occur in isolation (nonsyndromic), while the remaining 45.2% are syndromic and associated with various genetic disorders, each presenting with additional craniofacial and systemic abnormalities. 1
Orofacial clefts represent a significant global health concern, with epidemiological data demonstrating consistent occurrence across diverse populations and geographic regions. Recent evidence from European and U.S. population-based studies reports an overall prevalence of cleft lip and/or palate of approximately 1.1 per 1000 births and 1 per 1050 births, respectively. While cleft palate alone occurs in 0.5 per 1000 births and 1 per 1600 births, respectively, slight variation exists between regions.2,3
Pierre Robin sequence (PRS) is defined by the association of glossoptosis, mandibular hypoplasia or retrognathia, and cleft palate. 4 The prevalence of CP in the PR population is about 90%. 5 There have been some previous studies which have looked at the cleft size in patients with an isolated cleft palate and those with PRS. 6 However, the authors are unaware of any published literature comparing how dental arch relationships may change and how growth progresses in subjects with an isolated cleft palate and PRS.
Standardized assessment of treatment outcomes is essential in cleft care to enable meaningful comparison between centers and to evaluate the effectiveness of different treatment protocols across healthcare systems. A range of methods are used to assess facial growth and dental arch relationships, typically including clinical photographs, dental study models and lateral cephalometric radiographs. These records provide important information on craniofacial development and are widely used to guide clinical decision-making and long-term treatment planning.
National and regional audit frameworks have been developed to facilitate systematic outcome monitoring. In the United Kingdom, the Clinical Standards Advisory Group highlighted inconsistencies in cleft care and emphasized the need for improved data collection, 7 which led to the development of a nationally coordinated audit process and the establishment of the Cleft Registry and Audit Network database to document and compare outcomes. As part of these protocols, recommendations were made for the collection of dental study models at key developmental time points, including 5, 10, 15 and 20 years of age. 8
While these initiatives have improved the availability of longitudinal outcome data and contributed to advances in patient care, they are also associated with increased clinical time, resource demands, and patient burden. This raises important questions regarding the necessity and clinical value of collecting comprehensive records at all time points for all cleft subtypes, particularly if certain assessments do not directly influence treatment decisions. In this context, understanding patterns of maxillary growth and the stability of early outcome measures becomes especially relevant in determining the optimal timing and value of such assessments.
The 5-Year Index 9 and GOSLON Yardstick 10 are applied to dental study models and are the most commonly used indices to give an indication of maxillary growth at ages 5 and 10, respectively. They were originally designed to be applied to subjects with a unilateral cleft lip and palate and provide a relatively simple and reproducible method of grading dental arch relationships. Dental study models are scored from categories 1 to 5, for both indices, with a score of 1 being a better arch relationship indicating good relative growth of the maxilla and 5 being a poorer arch relationship, indicating poor growth of the maxilla. The authors of this paper are unaware of any similar indices that have been designed for subjects with an isolated cleft palate.
Maxillary growth in patients with isolated cleft palate remains variable, the majority of published studies to date have assessed facial growth in patients with a complete unilateral cleft lip and palate. There are relatively few studies that have looked at maxillary growth in patients with an isolated cleft palate treated with the same surgical protocol, and none of those published includes subjects based in the United Kingdom. Parikakis et al (2020) have published a cephalometric study looking at growth in subjects in 10- and 16-year-olds with an isolated cleft palate, compared to a noncleft population. 11 They concluded that the treated group typically had a retrognathic, smaller and posteriorly inclined maxilla. The same group of authors also published another cephalometric study in 5- and 10-year-old subjects, comparing 2 types of surgical repair. 12 Study model analysis was published in the 5-years-old subjects in a separate paper, but this data was not compared to the study models taken at 10 years of age. 13
The aim of this study was to compare maxillary growth at 5 and 10 years in subjects with an isolated cleft palate, using the 5-Year Index and GOSLON Yardstick, respectively. The null hypothesis was that there is no difference in dental arch relationship scores indicating maxillary growth (5-Year Index vs GOSLON Yardstick) between ages 5 and 10 in subjects with isolated cleft palate. The outcome of this study will also reflect the need of new records (study models) at 10 years of age.
Methods
This longitudinal retrospective cohort study did not require any ethical approval as the data collection was part of a service evaluation audit. This study was carried out on subjects within the North Thames Cleft Service, United Kingdom, (Unit A) and (Unit B) Hospitals. The inclusion criteria were those subjects born with an isolated cleft palate between 1988 and 2002. Subjects were all operated on by one surgeon and had their initial cleft palate repair at 6 months of age using intravelar veloplasty with muscle repair (Sommerlad technique). 14 Subjects with PRS were included, but not those with any other associated syndrome. The identification of the subjects with PRS was in accordance with the medical records. The subjects with PRS were identified using the database kept by the department, having a micrognathia, glossoptosis and airway obstruction.
As part of a nationally agreed audit protocol, subjects were seen at 5 and 10 years of age. At both 5 and 10 years, dental impressions and wax bite occlusal registration were undertaken in accordance with a standardized procedure to construct orthodontically trimmed study models. Subjects had not undergone any orthodontic treatment. The subjects’ study models were nonidentifiable and examiners were blinded to the subject's diagnosis.
Study models at 5 years were scored using the 5-Year Index and the 10-year study models using the GOSLON Yardstick for each subject included in the study. Each subject was scored separately by 3 trained and calibrated operators. This was then repeated 1 month later. Where there was any lack of concordance in the score, this was discussed between the operators and a score was agreed upon. Interexaminer and intraexaminer reliability was assessed using weighted Kappa tests. 15
The dental overjet (to the nearest 0.5 mm) was measured, using a metal ruler, defined as the extent of horizontal (anterior–posterior) overlap of the maxillary central incisors over the mandibular central incisors. Each subject was scored separately by one trained and calibrated operator. This was then repeated 1 month later. Where subjects were either missing both central incisors at 5 years or 10 years these subjects were excluded from the analysis, as it was not possible to measure the overjet. Using the method described by Dahlberg (1940), the random method error was assessed to determine intraoperator reproducibility. 16 In addition, we wanted to measure the change in the overjet between the ages of 5 and 10.
A per-protocol analysis was performed. Statistical analysis was performed using SPSS (version 22.0; IBM Corp 2013). McNemar's Test was used to compare the 5-Year Index and GOSLON Yardstick scores on subjects’ study models taken at 5 and 10 years, where P < .05 was considered to be statistically significant. The overjet data was tested for normality using the Kolmogorov–Smirnoff test. The mean values for the overjet at 5 and 10 years were compared using a paired t-test, where P < .05 was considered to be statistically significant.
Results
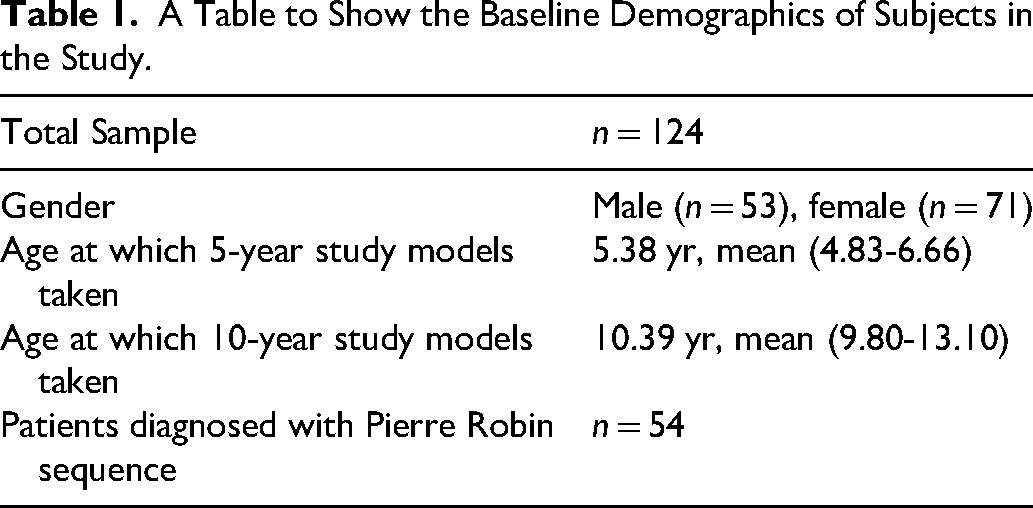
Database analysis highlighted 225 consecutive subjects that met the inclusion criteria. Dental study model records at both 5 and 10 years were available for 124 subjects (55%), including 53 males and 71 females. 54 of the 124 subjects were identified as having PRS, in accordance with their medical records. The baseline demographics of the subjects in the study are shown in Table 1.
A Table to Show the Baseline Demographics of Subjects in the Study.
The weighted Kappa scores for intraexaminer and interexaminer reliability with regard to the 5-Year Index and GOSLON Yardstick score are good to very good. 17
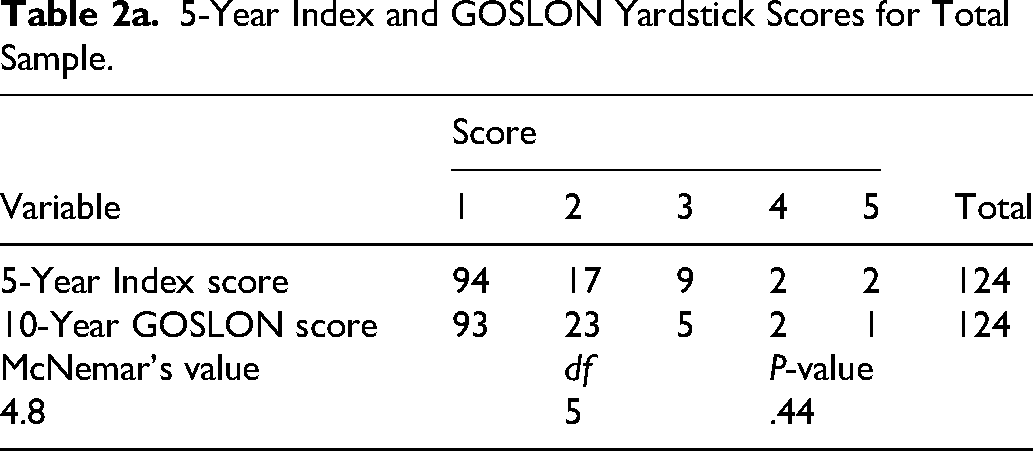
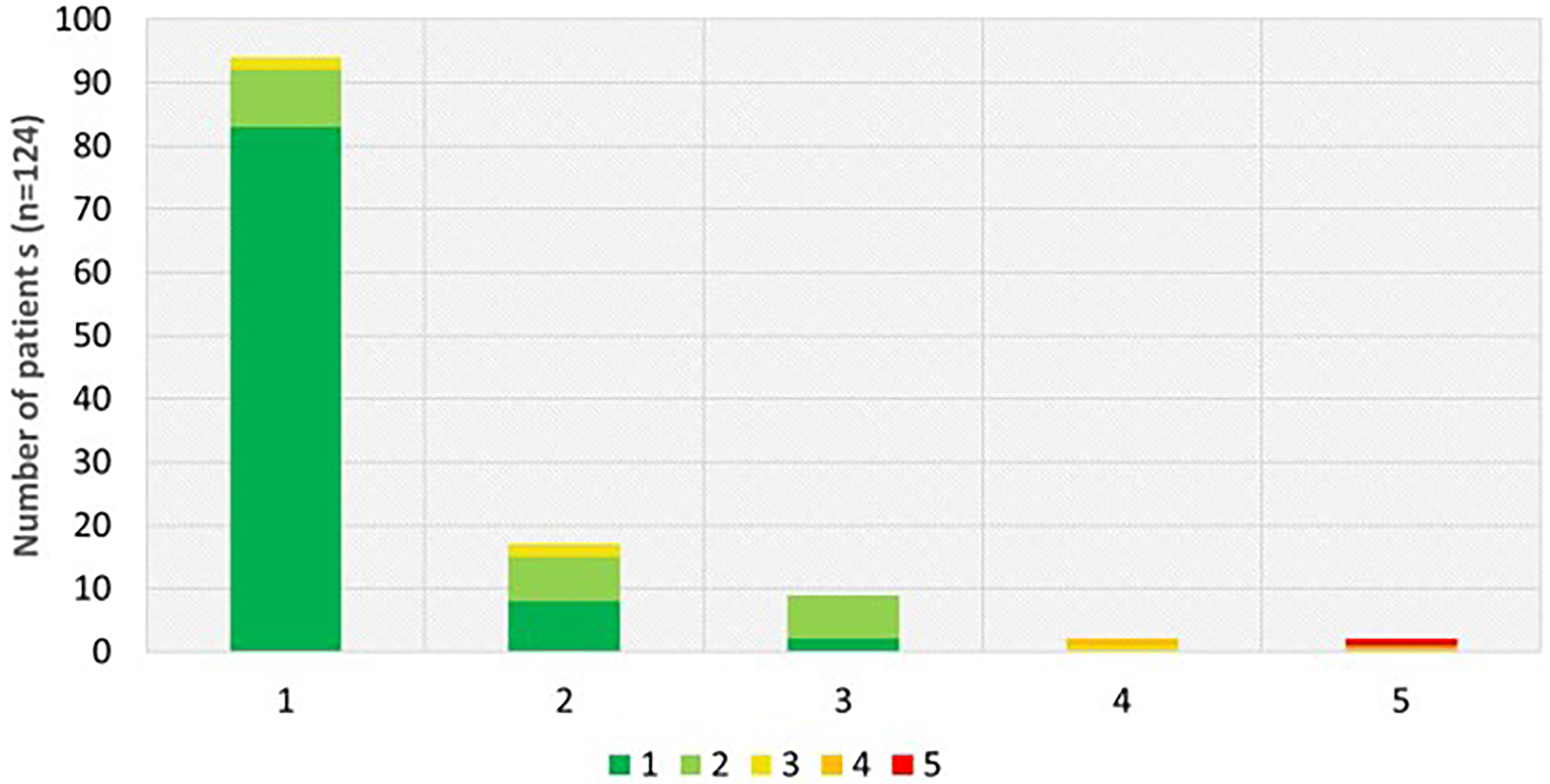
The 5-Year Index and GOSLON Yardstick scores for the 124 subjects in the study are shown in Table 2a. Figure 1a is a graph showing the distribution of the various scores for these subjects. Seventy-six percent of subjects had a 5-Year Index score of 1 and 75% of subjects had a GOSLON Yardstick score of 1. 14% of subjects had 5-Year Index score of 2 and 19% of subjects had a GOSLON Yardstick score of 2.
5-Year Index and GOSLON Yardstick Scores for Total Sample.

(a) The overall scores of the subjects’ 5-Year Index and GOSLON Yardstick scores. (b) The distribution of the various scores for PRS subjects’ 5-Year Index and GOSLON Yardstick scores.
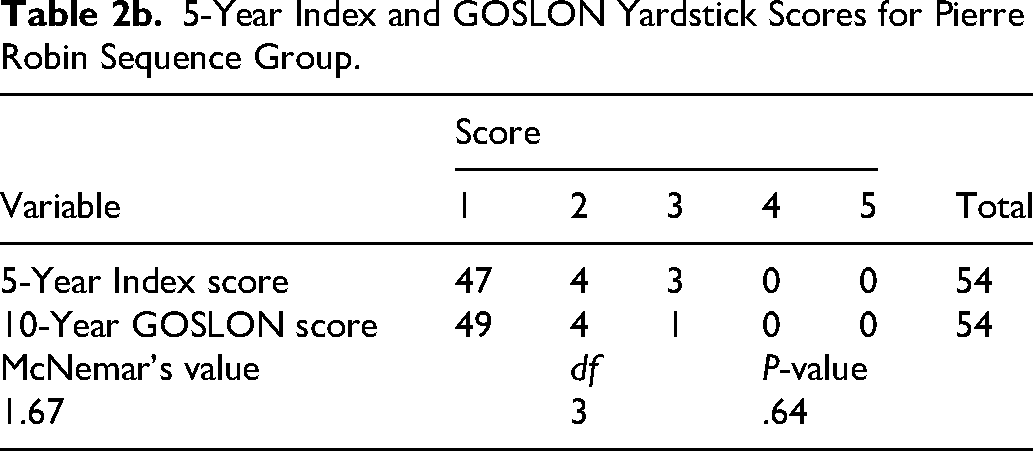
The scores for the 54 subjects with PRS are shown in Table 2b. Figure 1b is a graph showing the distribution of the various scores for these subjects with PRS. Eighty-seven percent of subjects with PRS had a 5-Year Index score of 1 and 91% of subjects with PRS had a GOSLON Yardstick score of 1. 7% of subjects with PRS had 5-Year Index score of 2 and 7% of subjects with PRS had a GOSLON Yardstick score of 2.
5-Year Index and GOSLON Yardstick Scores for Pierre Robin Sequence Group.
Both groups show no statistically significant difference at the 95% significance level between the 5-Year Index Score and the GOSLON Yardstick Score for subjects in this study (Table 3).
A Table to Show the Results of McNemar's Test Comparing the 5-Year Index Versus the GOSLON Yardstick Score.
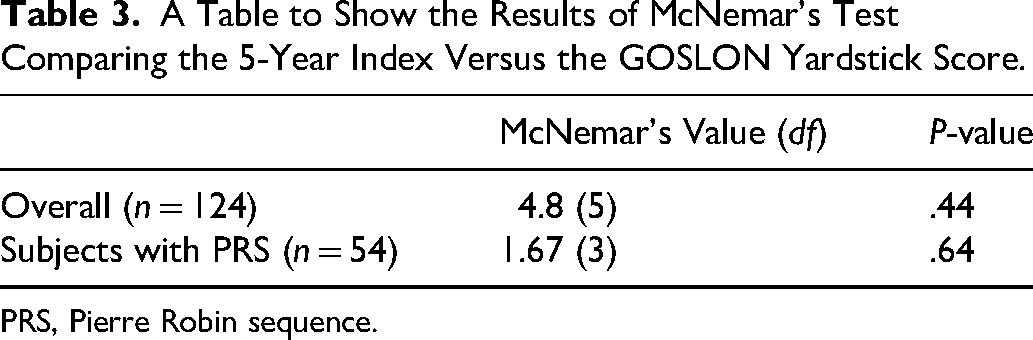
PRS, Pierre Robin sequence.
Figure 2 is a graph showing the overall and individual changes in the subjects’ 5-Year Index and GOSLON Yardstick scores. 75% of subjects had the same equivalent 5-Year Index and GOSLON Yardstick Score. The GOSLON Yardstick score had improved for 15% of subjects, compared to their score on the 5-Year Index. However, for 10% of subjects, their GOSLON Yardstick score was worse at 10 years of age, compared with the equivalent 5-Year Index score.
The overall and individual changes in the subjects’ 5-Year Index and GOSLON Yardstick scores.
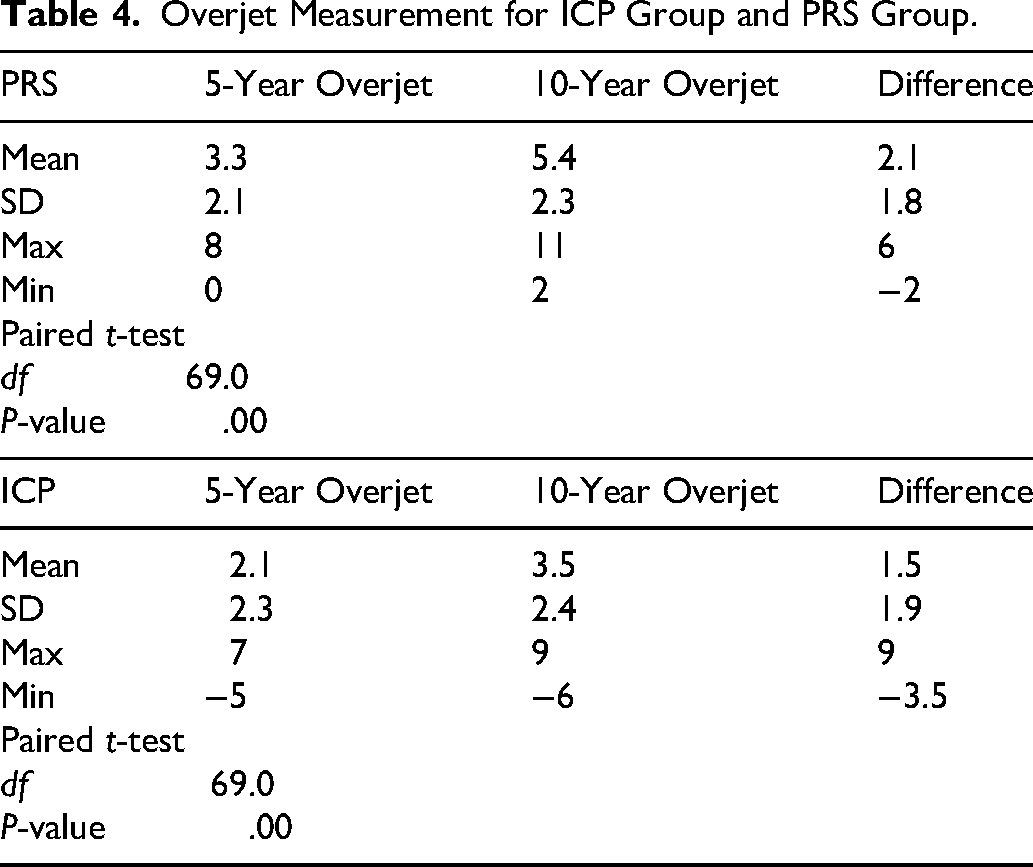
There were 118 subjects suitable for overjet analysis, of which 53 had PRS. The Dahlberg error value was 0.19 for the overjet measurement and thus within acceptable limits. The Kolmogorov–Smirnoff test showed the data to be normally distributed. Paired t-tests for the whole sample, those with an isolated cleft palate and no history of PRS and those with PRS, showed there is a significant difference in the overjet values at 5 and 10 years (Table 4). For subjects with an isolated cleft palate and no history of PRS, the mean overjet at 5 years of age was 2.1 mm, compared to 3.5 mm at 10 years of age. For subjects with a history of PRS, the mean overjet at 5 years was 3.4 mm, compared to 5.4 mm at 10 years of age (Table 4). The range of the overjet data and differences in overjet at 5 and 10 years are shown in Figure 3. However, there is no statistical significance between the 2 groups with P-value of .06.
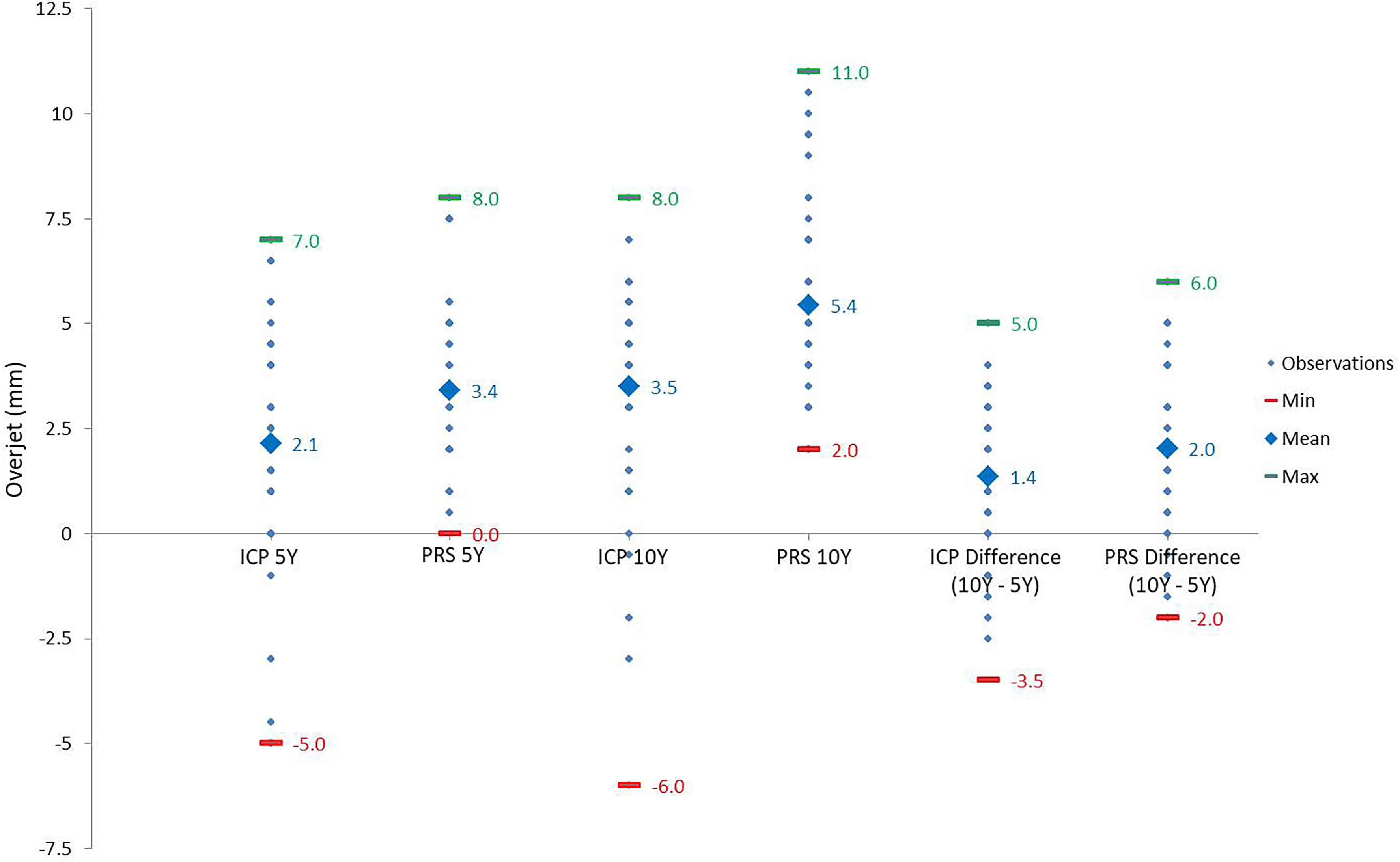
The range of the overjet data and differences in overjet at 5 and 10 years.
Overjet Measurement for ICP Group and PRS Group.
Discussion
The results of this study show that for the 124 subjects with an isolated cleft palate, the distribution of scores at 5 years and 10 years, on the 5-Year Index and GOSLON Yardstick, is relatively similar. This would indicate that in relation to maxillary growth, the outcome at 5 years of age is a good reflection of the outcome at 10 years of age. We have therefore confirmed the null hypothesis that there is no difference in maxillary growth at 5 and 10 years of age in subjects with an isolated cleft palate. The same was also true when the data for subjects with PRS was analyzed separately.
Although there was a statistically significant difference in the overjet measurements at 5 and 10 years in subjects with an isolated cleft palate and those with PRS, it is unlikely to be clinically significant. The mean change in overjet for the subjects with an isolated cleft palate being an increase by 1.4 mm and 2 mm in the PRS group fits in with the normal pattern of growth within this cohort. 18 The mean overjet values for the subjects with PRS were greater, which would be expected, as these subjects typically have a smaller mandible.
Previous longitudinal study in patients with unilateral cleft lip and palate have investigated the predictive value of early dental arch relationship indices. Mars et al (2006) reported poor agreement between 5-year and 10-year outcomes when comparing the 5-Year Index and GOSLON Yardstick in UCLP patients. In contrast, the present study demonstrated no statistically significant difference between assessments at 5 and 10 years in subjects with isolated cleft palate, suggesting potential differences in growth patterns and outcome stability between cleft subtypes. 19
In view of these results, in a climate where within the National Health Service in the United Kingdom, due to limited funds, there is a drastic need to prioritize resources. Therefore, the findings of this service evaluation may have direct implications for clinical record-taking when there is no other clinical indication to do so.
There are some limitations to the current study, which the authors wish to acknowledge. The number of participants lost to follow-up represented 55% of the total cohort. This was a result of nonattendance at our audit record collection appointment despite being invited on several occasions. The participants in this study were only 10 years of age, and maxillary growth will not be entirely complete by 10 years. However, since the majority of the sample had a favorable 5-Year Index and GOSLON Yardstick score, this is unlikely to become worse, in line with normal growth patterns within this cohort of patients. A further limitation is the use of a metal ruler for measurements. While this method demonstrated strong interexaminer and intraexaminer reliability within the present study, in retrospect, 3-dimensional digital scanning and software-based analysis methods could be used as a contemporary alternative, as these techniques can provide high levels of accuracy and reproducibility while also improving efficiency through reduced operator dependency, workload, and time requirements. This is consistent with findings from recent related studies which further support the use of 3-dimensional measuring tools can be a reliable and comparable method for patients with palatal clefts.20-22 However, in consideration of the available data resources and study design involving plaster dental study models, the use of a metal ruler remained an appropriate and robust method for the aims of this investigation.
The 5-Year Index and GOSLON Yardstick were designed for use in patients with a unilateral cleft lip and palate to assess dental arch relationships and thus provide an indication of maxillary growth. Although they are comparable, there are differences between the 5-Year Index and GOSLON Yardstick themselves. The patients in this study had an isolated cleft palate, but the authors are not aware of any widely used alternate growth indices for this group. Future studies could look at preorthodontic records and types of treatment provided in this cohort of patients. Comparison could also be made to growth in the wider population, without clefts and to directly compare outcomes with orthodontic baseline data.
Further work is required to develop and validate outcome measures specifically for patients with isolated cleft palate, as current indices may not fully reflect the unique growth patterns within this group. The development of more tailored assessment tools would enhance the accuracy of growth evaluation and improve the ability to compare outcomes across studies and clinical centers.
To our knowledge, there is no other similar relatively simple tool currently available to assess maxillary growth in patients with an isolated cleft palate. Future studies could potentially include measuring the width and length of the initial cleft. The height of the palatal vault could be measured longitudinally. Other aspects of the dental occlusion such as the presence of anterior and posterior cross-bites and the depth of the overbite, as well as measurements of maxillary dimensions on the subjects could also be recorded, to assess the effects of the initial surgery on maxillary growth. Although a significant advantage of the current study is that all operations were carried out by a single surgeon, the primary surgery was carried out over 14 years and the skill of the surgeon is likely to have improved over this time and therefore could affect the results observed. In this retrospective study only subjects’ dental study models, which were taken as part of a routine audit have been used to assess maxillary growth. It was not within the department's protocol to take lateral cephalograms on 5-year-old subjects, as clinically they would not be indicated, and radiation exposure could not be justified.
Conclusion
In this cohort, dental arch relationship scores at 5 years were consistent with those at 10 years, indicating that early assessment provides a useful reflection of later outcomes in patients with isolated cleft palate.
Footnotes
Acknowledgments
The authors would like to acknowledge the assistance of James Green, Laboratory Technician, Great Ormond Street Hospital, for his help in preparing the dental models for this study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.