
Abstract
Objective
Cleft lip and palate is the most common craniofacial birth defect. Timely primary cleft surgery is important to achieve good esthetic and speech outcomes and to prevent complications. The aim of this study was to compare outcomes between patients undergoing surgery at a comprehensive cleft center (CCC) and non-CCCs.
Design
Retrospective comparative study.
Settings
One CCC and non-CCCs in 5 cities.
Patients and Intervention
The study included 300 children who underwent primary cleft surgery at the participating centers between 2020 and 2024.
Main Outcome Measures
The age at primary cleft surgery, length of hospital stay (LoS), and complications.
Results
Primary cleft-lip and cleft-palate surgery was delayed in >50% and >60% of patients in the non-CCC group, respectively, which was significantly different compared to the rates in the CCC group. LoS was significantly shorter in the non-CCC group (P = .001). Complications such as bleeding, dehiscence, and return to the operating room after primary cleft surgery were significantly more common in the non-CCC group (P < .01)
Conclusion
This study offers an insight into the timing of cleft lip and palate surgery, epidemiology, complication rates, and LoS in CCC and non-CCC settings in Indonesia. The frequency of delayed primary cleft lip and palate surgery and complication rates were significantly higher in non-CCC than in CCC settings. Therefore, strengthening cleft-care infrastructure in remote regions through multidisciplinary training, standardized operative protocols, and improved logistical support is essential to reduce disparities and ensure sustainability.
Introduction
Cleft lip and palate is the most common craniofacial birth defect. The World Health Organization reported that the global incidence of cleft lip ranges from 3.4 to 22.9 per 1000 births, whereas that of isolated cleft palate ranges from 1.3 to 25.3 per 1000 births.1–3 However, the incidence varies between countries owing to variations in genetic, nutritional, and environmental factors.
Treatment of cleft lip and palate aims to restore the normal anatomical structure, speech, and occlusion and minimize psychological problems in the patients and family.4,5 However, for optimal results, an interdisciplinary approach and accurate treatment timing are required.6,7 Delayed primary cleft lip surgery negatively affects physical appearance, speech, feeding, and psychosocial outcomes. Furthermore, delayed primary cleft palate surgery is associated with poorer speech outcomes, often requiring prolonged speech therapy and additional surgical intervention due to velopharyngeal insufficiency, as well as an increased risk of ear infections.8–10 Therefore, early surgical repair is advisable. However, surgical procedures should be meticulously planned to ensure safety and adequate repair, avoid complications, and reduce exposure to anesthesia during multiple surgeries.
National guidelines, namely those of the American Cleft Palate Craniofacial Association (APCA) and the Cleft Lip and Palate Association (CLAPA) of the United Kingdom recommend that primary cleft-lip repair should be performed before 6 months of age. The recommended age for primary repair of cleft palate is 12 months (UK; CLAPA) or 18 months (USA; ACPA).8,9 In our institution, we follow the guidelines of the ACPA for cleft palate surgery.
Smile Train is the world's largest charity organization that provides funding for the treatment of children with clefts. Ideally, the treatment must be performed by a comprehensive cleft-care team; however, in some countries this is not always possible, owing to a lack of specialists and hospitals and difficulties in transportation.3,6,11,12 Our institution has partnered with Smile Train to provide surgery for children not only in our comprehensive cleft center (CCC) but also in non-CCC settings in remote areas where getting proper care is difficult owing to a lack of specialists and facilities.
A CCC is a single-center, hospital-based facility that provides comprehensive cleft management through a coordinated multidisciplinary team approach. The team typically consists of cleft surgeons, pediatricians, anesthesiologists, obstetricians and gynecologists, speech therapists, general dentists, pediatric dentists, orthodontists, pediatric nurses, and social workers. In contrast, non-CCC settings are typically located in smaller cities and remote areas, where access to a comprehensive multidisciplinary cleft team is limited or unavailable; therefore, cleft care services are often delivered through periodic visits by external cleft teams that usually consist of cleft surgeon, anesthesiologist and pediatric nurse.
Non-CCC facilities are often located several hundred kilometers away from established CCCs. Patients presenting to non-CCC settings frequently travel long distances, ranging from tens to hundreds of kilometers, to access available cleft care services. In terms of infrastructure, both types of cleft treatment centers are required to meet basic requirements for cleft care delivery, including the availability of an operating theater, neonatal intensive care unit, pediatric ward, resuscitation room, laboratory services, and radiological facilities such as chest X-ray.
In the study area, postoperative care protocols in both CCC and non-CCC settings were found to be comparable, with standardized guidelines for diet, oral hygiene, and wound care implemented across both settings. Elbow restraints were not utilized in either center. However, differences were observed in postoperative follow-up. In non-CCC settings, patients typically remained near the facility for only 2 to 3 days postoperatively before returning home, after which wound care and follow-up were continued at the nearest local healthcare facility. In contrast, patients treated at CCC underwent regular and structured follow-up visits.
Currently, birth defects, including cleft lip and palate are not uniformly registered by the national health institution body in our country. Moreover, to the best of our knowledge, few studies have reported the trends and patterns in age at primary surgery and complications between patients treated in CCC and non-CCC settings. Therefore, the aim of the present study was to compare the trends and patterns in age at primary surgery, complications, and length of hospital stay (LoS) between patients undergoing cleft surgery at CCC and non-CCC group.
Materials and Methods
This retrospective comparative study included 300 nonsyndromic patients who underwent primary cleft surgery funded by Smile Train between 2020 and 2024. All surgeries were performed by the same cleft team at either the CCC or non-CCC settings at charity missions in 5 cities in Indonesia. Three cleft surgeons were involved in this study. All surgeons routinely practiced and operated at CCC, resulting in comparable surgical training and clinical experience in cleft surgery. Data were extracted from the Smile Train Express (STX) database, an online electronic medical record developed as a control tool for all partner institutions of Smile Train. The database classifies cleft conditions into several categories: cleft lip (noncleft, complete, or incomplete; further categorized as unilateral or bilateral), cleft palate (noncleft, complete, incomplete, or submucous), and hard palate involvement (unilateral or bilateral).
All adult patients and parents of children who underwent cleft surgery provided written informed consent for surgery and for the use of their data for research purposes. All data were anonymized before we had access.
Variables
The primary outcome measure was delayed primary surgery (age at surgery ≥12 months for primary cleft-lip surgery and ≥18 months for primary cleft-palate surgery). Independent variables were date of birth or age, sex, type of cleft, type of surgery, date of surgery, complications, and LoS. Complications were defined as postoperative bleeding, return to the operating room, wound dehiscence, and wound infection.
Statistical Analysis
Data were analyzed using SPSS software (version 29.0; IBM Corp., Armonk, NY, USA). Categorical variables were analyzed using the chi-square test with continuity correction and Fisher's exact test when expected cell counts were <5. Continuous variables were analyzed using the independent t-test for normally distributed data with equal variances, and the Mann–Whitney U-test for nonnormally distributed data. Statistical significance was set at P < .05.
Results
Primary Cleft-Palate Repair
Demographic and Clinical Characteristics
A total of 205 primary cleft-palate surgeries were performed during the 5-year study period (2020-2024). The demographic and clinical characteristics of the patients are listed in Table 1. The male:female ratio was 66:34.
Demographic and Clinical Characteristics of the Patients.
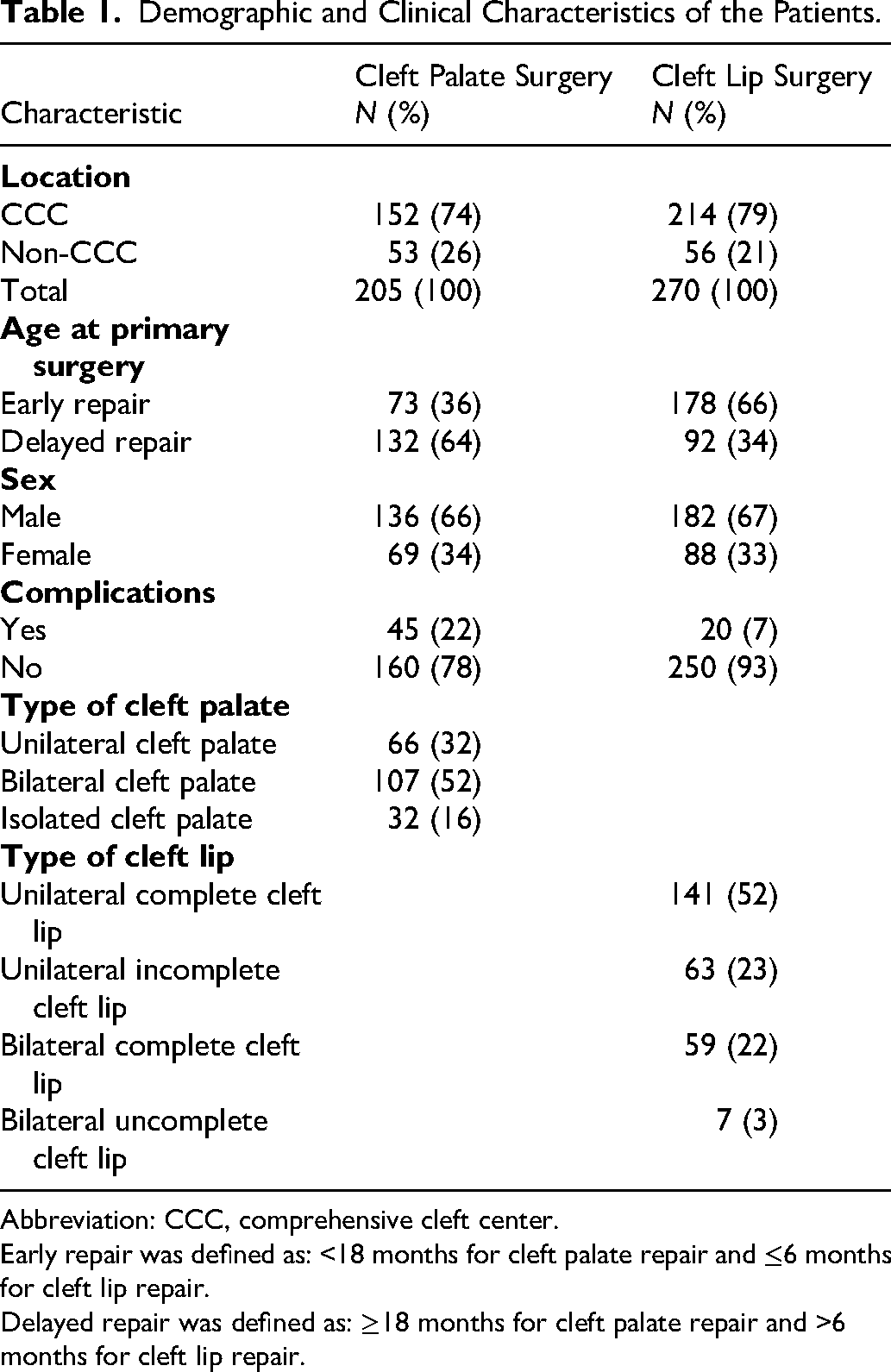
Abbreviation: CCC, comprehensive cleft center.
Early repair was defined as: <18 months for cleft palate repair and ≤6 months for cleft lip repair.
Delayed repair was defined as: ≥18 months for cleft palate repair and >6 months for cleft lip repair.
The majority of patients who underwent primary cleft-palate surgery were male, either in the CCC group (n = 102 [67.1%]) or the non-CCC group (n = 34 [64.2%]; odds ratio [OR] < −0.877. Sex distribution was not significantly different between the 2 groups (P > .05) (Table 2).
Gender Distribution Between CCC and Non-CCC Groups.
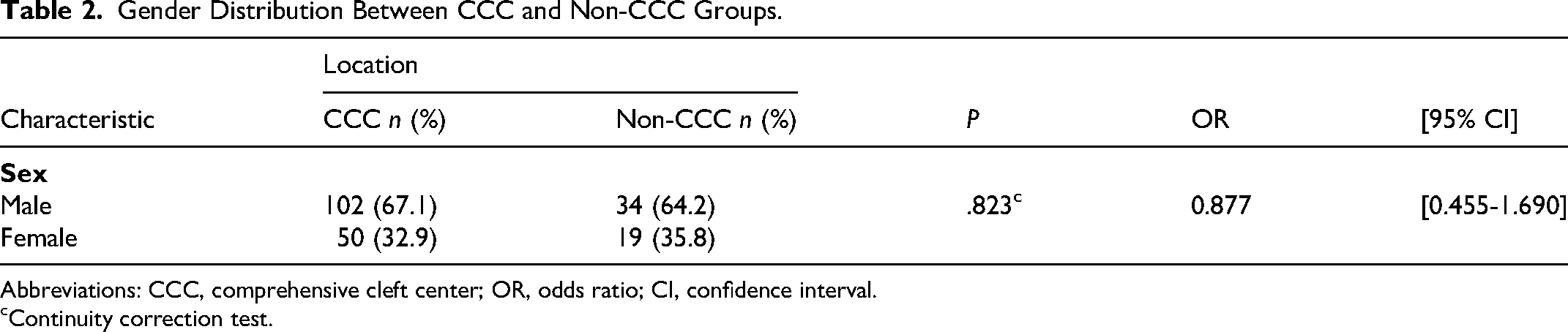
Abbreviations: CCC, comprehensive cleft center; OR, odds ratio; CI, confidence interval.
Continuity correction test.
The incidence of bilateral cleft palate (n = 107 [62%]) was higher than that of unilateral cleft palate (n = 66 [38%]). In all cases, cleft-palate repair was performed using the modified 2-flap technique with radial muscle dissection under 4.5× magnification using loupes. The majority of primary cleft-palate surgeries were performed at the CCC (n = 152 [74%]), and only 53 patients (26%) were treated in non-CCCs. Most patients underwent complete cleft palate repair (n = 188 [94%]).
Association of Demographic and Clinical Characteristics With Age at Primary Surgery
Most patients who underwent primary cleft-palate surgery were aged >18 months (n = 132 [64%]). However, the proportion of children aged <18 months was higher in the CCC group (n = 62 [40.8%]) than in the non-CCC group (n = 11 [20.8%]); (P = .014; OR = 0.380; Table 3). Age at primary cleft-palate surgery was significantly associated with the type of center. Specifically, cleft-palate surgery tended to be performed later in non-CCCs than at the CCC (Figure 1).
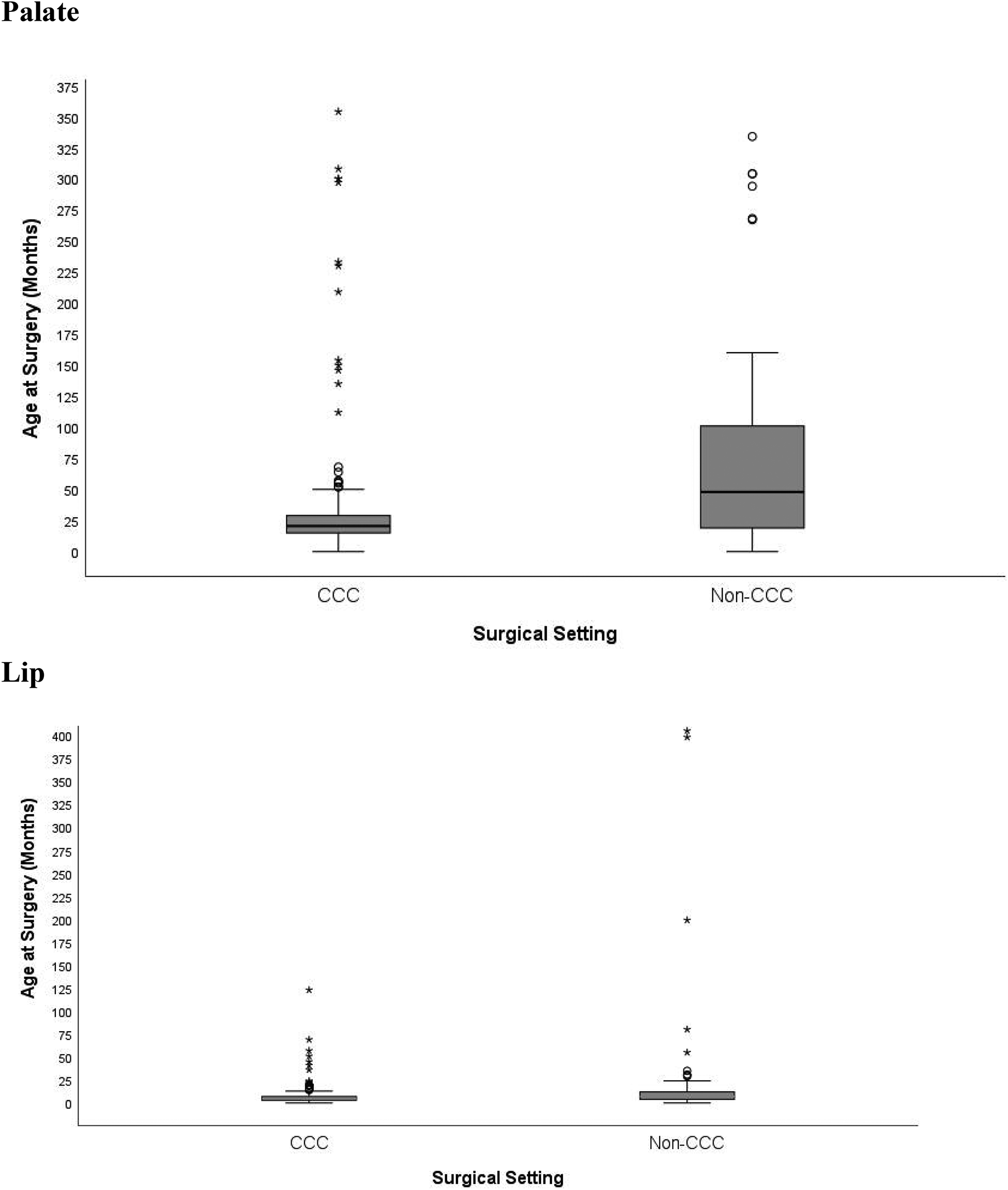
Age of primary cleft lip and cleft palate surgery.
Age at Primary Cleft Palate Repair.
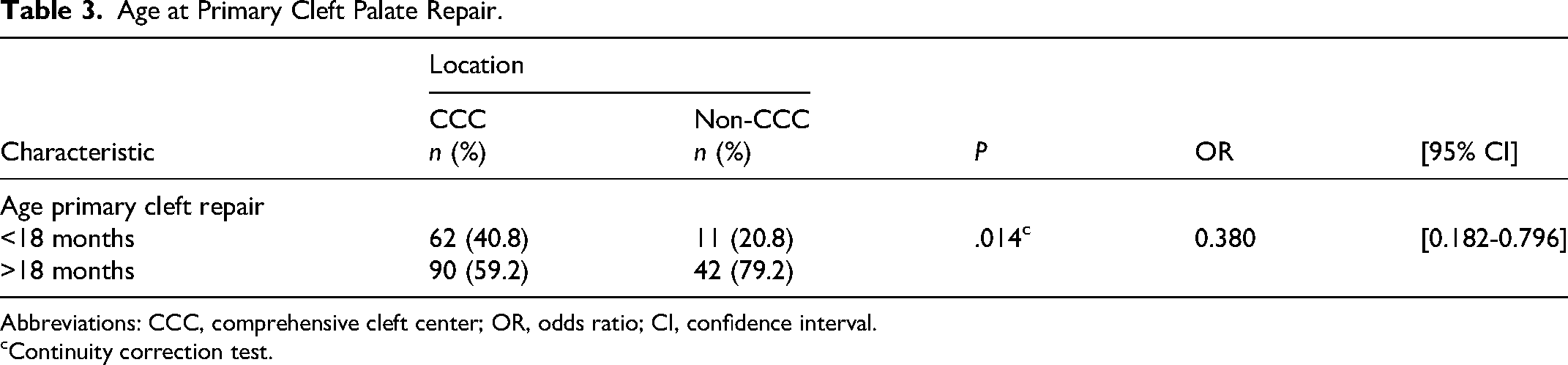
Abbreviations: CCC, comprehensive cleft center; OR, odds ratio; CI, confidence interval.
Continuity correction test.
Both unilateral and bilateral cleft palate repair were more frequent in the CCC group (n = 53 [40.5%] and n = 78 [59.5%], respectively) than in the non-CCC group (n = 13 [31%] and n = 29 [69%], respectively). However, the distribution of bilateral clefts was not significantly different between the groups (P = .357).
Complete soft-palate cleft was more frequent in the CCC group (n = 146 [98.6%]) than in the non-CCC group (n = 42 [82.4%]). However, incomplete soft-palate cleft, including submucous cleft palate, was more frequent in the non-CCC group (n = 9 [17.6%]) than in the CCC group (n = 2 [1.4%]), and the difference was statistically significant (P < .001).
Association of Demographic Data and LoS for Primary Palate Surgery
The mean LoS was 2.22 days (SD, 0.596) in the CCC group and 1.74 days (SD, 0.524) in the non-CCC group. The difference was not statistically significant (P = .071, Table 4).
Length of Stay (LoS) After Primary Cleft Palate Repair.
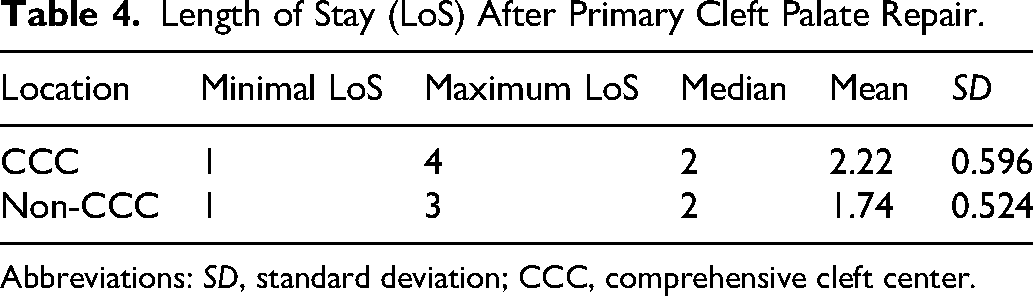
Abbreviations: SD, standard deviation; CCC, comprehensive cleft center.
Complications of Primary Cleft-Palate Surgery
As shown in Table 5, complications such as bleeding, dehiscence, and return to the operating room were significantly more frequent in the non-CCC group than in the CCC group (n = 32, 60.4% vs. n = 13, 8.6%; P < .01). This indicates a higher tendency for complications of primary cleft-palate surgery in non-CCC settings.
Complication After Primary Cleft Palate Repair.

Abbreviations: CCC, comprehensive cleft center; OR, odds ratio; CI, confidence interval.
Continuity correction test.
Primary Cleft-Lip Repair
Demographical and Clinical Characteristics
During the study period (2000-2024), 270 patients underwent primary cleft-lip surgery. The demographic and clinical characteristics of the patients are listed in Table 6. The male:female ratio was 66:34. The majority of patients (n = 204 [75%]) presented with unilateral cleft lip.
Demographic and Clinical Characteristics of Patients Between CCC and Non-CCC.
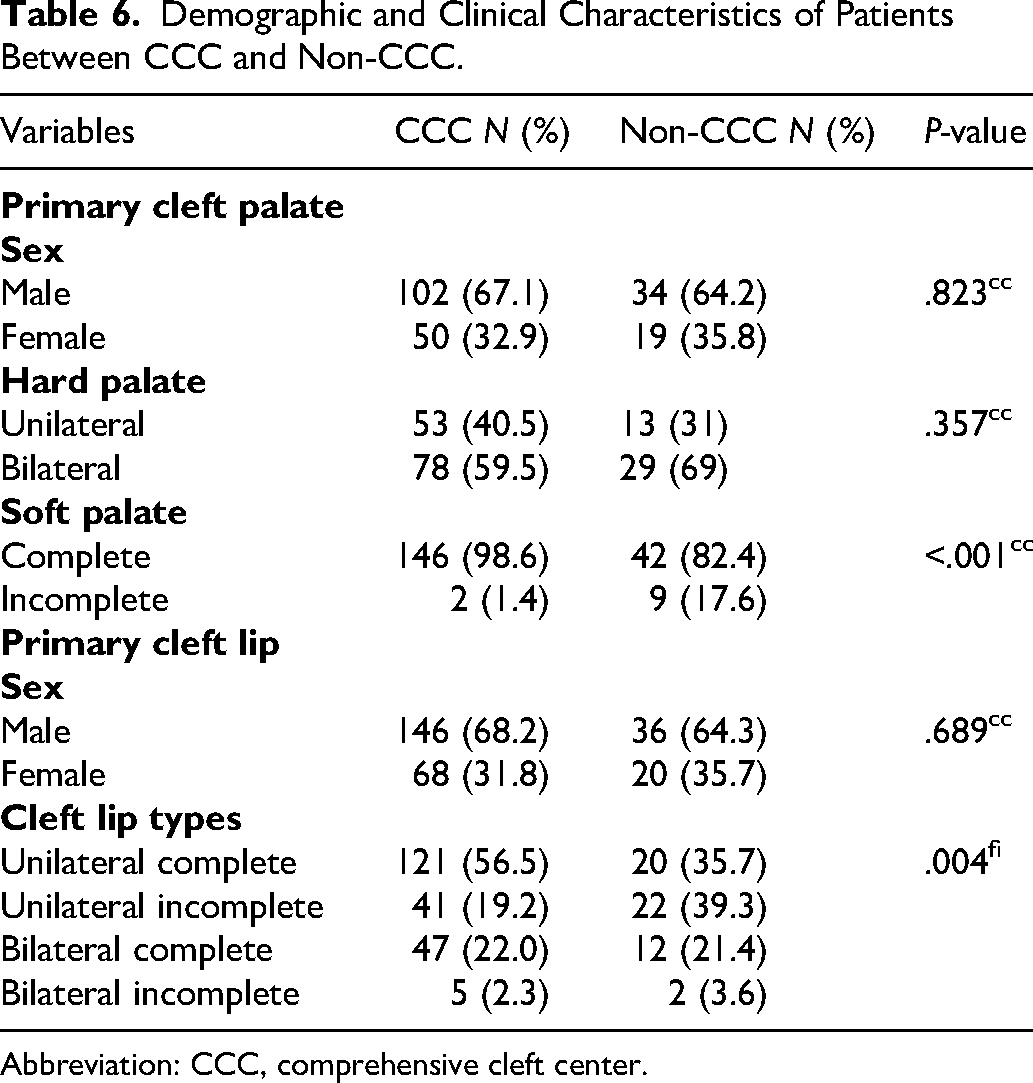
Abbreviation: CCC, comprehensive cleft center.
Age at Primary Cleft Lip Surgery.
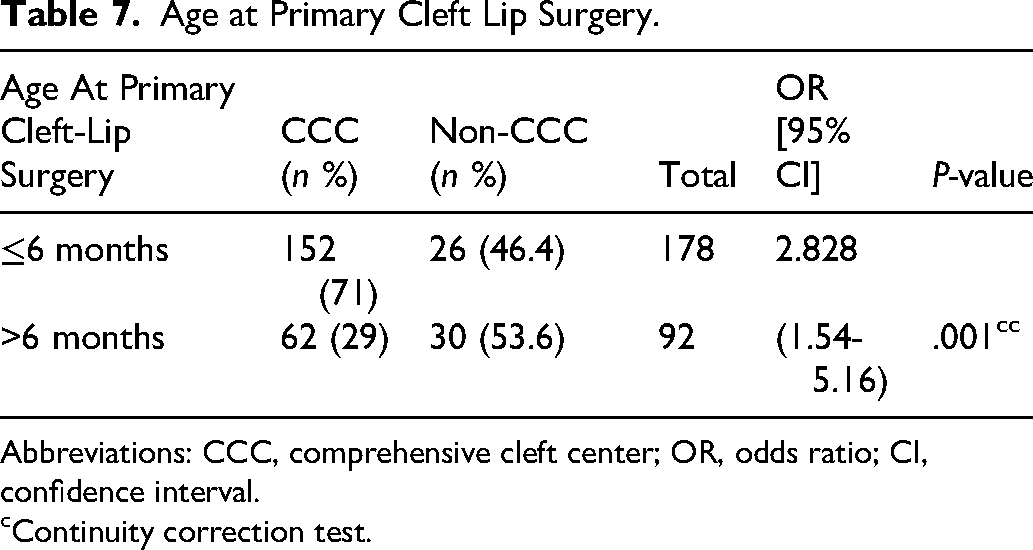
Abbreviations: CCC, comprehensive cleft center; OR, odds ratio; CI, confidence interval.
Continuity correction test.
Complication After Primary Cleft Lip Repair.

Abbreviations: CCC, comprehensive cleft center; OR, odds ratio; CI, confidence interval.
Continuity correction test.
In both groups, the majority of patients were male (CCC group, n = 145 [68.2%]; non-CCC group, n = 36 [64.3%]). Sex distribution was not significantly different between the groups (P = .823). Modified Millard techniques were used for cleft-lip repair in all patients, and the majority of surgeries were performed at the CCC (n = 214 [79%]).
In both groups, unilateral primary cleft-lip repair was more frequent than bilateral primary cleft-lip repair (CCC group, n = 162 [75.7%] vs. n = 52 [24.3%]; non-CCC group, n = 44 [75%] vs. n = 14 [25%]). Distribution of cleft type was not significantly different between the 2 groups (P > .05).
Association of Demographic and Clinical Characteristics With Age at Primary Cleft-Lip Surgery
In the CCC group, most children underwent primary cleft-lip repair at age ≤6 months (n = 152 [71%]). In contrast, in the non-CCC group, the proportion of children with cleft-lip surgery at age ≥6 months was higher (n = 30 [53.6%]) (Table 7). Thus, the type of center was significantly associated with age at primary cleft-lip surgery (P = .001). This indicates a higher tendency for delayed primary cleft lip-surgery in non-CCC settings.
Logistic regression analysis to determine the correlation between cleft-lip type and age at primary cleft-lip surgery revealed that complete unilateral cleft lip was significantly associated with delayed surgery (OR, 2.33; 95% confidence interval [CI], 1.24-4.35; P = .008). In contrast, no significant associations were observed for incomplete bilateral cleft lip (OR, 1.01; 95% CI, 0.497-2.07; P = .967) and complete bilateral cleft lip (OR, 2.00; 95% CI, 0.36-11.09; P = .438)
Association Between Demographic Characteristics and LoS for Primary Lip Surgery
The mean LoS in the CCC was 2.25 days (SD, 0.63) and non-CCC group was 1.54 days (SD, 0.60). The difference was statistically significant (P < .01).
Complications of Primary Cleft-Lip Surgery
Complications such as bleeding, dehiscence, and return to the operating room were more frequent in the non-CCC group (n = 17) than in the CCC group (n = 3) (Table 8), and the difference was statistically significant (P < .01). This indicates a higher tendency for complications of primary cleft-lip surgery in non-CCC settings.
Discussion
The results of our analysis highlight important disparities in cleft-care delivery between CCC and non-CCC settings. Although cleft lip and palate are not life-threatening conditions that require emergency surgery, timely cleft surgery is essential for optimizing feeding, appearance, speech, hearing, and psychosocial outcomes. According to the APCA guidelines adopted at our center, primary cleft-lip surgery should be performed before 6 months of age and primary cleft-palate surgery before 18 months of age.8,9
In this study, primary cleft-lip surgery was delayed in >50% of patients in the non-CCC group and primary cleft-palate surgery was delayed in >60% of patients in this group; the proportion of cases of delayed surgery in the 2 groups (CCC and non-CCC) was significantly different. Delayed cleft-palate repair can impact speech development that is very difficult to manage later. The data on the considerable delay in primary cleft repair highlights the challenges in accessing cleft care services in this country. These findings are comparable to those in a Nigerian study, in which it was reported that primary cleft-lip surgery was delayed in 39.7% and primary cleft-palate surgery in 67.1% of patients. 13 The data from this study present opportunities for improvement for the cleft care system nationwide.
The survival rate of individuals with unrepaired cleft is low, and <25% survive beyond the age of 5 years. In contrast, patients who receive timely surgical care have survival rates similar to those of unaffected children.1,14
In lower- and middle-income countries, the national income is correlated with delayed primary cleft surgery. The likelihood of late surgery increases by 70% for every $1000 decrease in gross domestic product per capita.15,16 In the present study, surgery was delayed despite the availability of free cleft surgery. This could be attributed to factors such as lack of awareness, travel cost, lack of trust in healthcare providers, lack of trained doctors, and stigma associated with the condition. 16 Regression analysis based on the severity of cleft showed a tendency for delayed surgery in all complex cleft types (OR >1). However, a statistically significant delay was observed only in unilateral complete cleft lip and palate (P = .008). This is comparable to the finding of Michaels et al that patients with more complex cleft (bilateral CL/P vs. unilateral CL/P) types tend to undergo surgery early. 9
Interestingly, we found that LoS was significantly shorter in the non-CCC group than in the CCC group (1-3 vs. 1-7 days; P = .001). However, the shorter LoS in the non-CCC group reflects the need for early discharge rather than enhanced efficiency and safety. Non-CCC hospitals usually have limited facilities and access, and because patients mostly come from other cities, they cannot stay for extended periods. The advantage of shorter LoS is the reduced cost; however, it is associated with a risk of unmonitored complications such as bleeding and dehiscence, which can cause difficulties in feeding postoperatively. Indeed, incidents of postoperative bleeding, dehiscence, and return to the operating room were significantly more common in the non-CCC group (P < .01). This is consistent with the findings in a previous study that the palatal fistula rate after cleft palate repair at the Guwahati Cleft Care Center was higher in surgeries performed by visiting doctors.17,18 In a study in China, the authors reported that the incidence of palatal fistula was higher among surgeries performed by an international team (34.4%) compared to surgeries performed by local doctors (12.8%). 19 Similarly, in a Peruvian study, an outreach surgical cleft surgery program by the same team resulted in significantly higher rates of wound dehiscence (22.9% vs. 9.8%) and palatal fistula (25% vs. 3.8%). 20 These results highlight the importance of preoperative patient preparation, including presurgical infant orthopedic and nutritional status assessment; surgeons’ expertise; availability of equipment; standardization of sterilization protocols and facilities; experienced local nursing; and postoperative monitoring for 7 to 10 days. Particularly, the patient's diet, wound hygiene and dressing, and identification of early signs of infection are important. Therefore, in non-CCC settings, changes should be made to prioritize quality perioperative care rather than the total number of surgeries performed.
Hackenberg et al, in their comparison of the outcomes from 2 different settings of cleft treatment, showed that surgery at CCC was more cost-effective than that at non-CCC (USD 190 vs. 466). 21 Moreover, the cost per procedure was lower at the CCC (USD 400 vs. 677). 22 Furthermore, optimal cost-effectiveness of cleft surgery was achieved when the procedure was performed by local teams in government-managed hospitals.
Although differences in operative setting and perioperative support may have influenced complication rates between centers, surgeon-related variability was likely minimized because the same experienced cleft surgeons performed procedures in both CCC and non-CCC groups.
Limitations
The data used in this study were extracted from the online STX database. Thus, information regarding variables such as economic status, parents’ education level, and host hospital condition was limited. In the future, multicenter studies that include these variables are warranted.
Conclusion
This study offers an insight into the timing, epidemiology, and complication rates of cleft lip and palate surgery and LoS in CCC and non-CCC settings in Indonesia. The frequency of delayed primary cleft lip and palate surgery and complication rates were significantly higher in non-CCCs than in CCCs. Therefore, strengthening cleft-care infrastructure in remote regions through multidisciplinary training, standardized operative protocols, and improved logistical support is essential to reduce disparities and ensure sustainability.
Barriers to timely primary cleft surgery, such as socioeconomic and financial factors, geographic barriers, inequities in access to care, lack of awareness, cultural beliefs, and social stigma need to be overcome to give children a chance to survive, grow normally, and develop to their full potential. Although surgery in non-CCCs remains vital, developing sustainable and well-equipped regional cleft centers is crucial to ensuring safe, timely, and equitable cleft care throughout the country.
Footnotes
Acknowledgments
The authors thank Smile Train for their support and contribution to patient care and data collection.
ORCID iDs
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.