
Abstract
Newly arrived immigrant and refugee children are faced with significant physical and mental health issues and often rely on school nurses for care and connection to healthcare. The purpose of this qualitative phenomenological study was to explore urban public school nurses’ experiences caring for newly arrived children. Data were collected through one-time in-depth semistructured interviews with school nurses (n = 20). Three relational themes were identified: (1) Trials and Triumphs: Telling Stories About Newly Arrived Children; (2) Walk a Mile in My Shoes; and, (3) Being a Trusted Health Navigator. The Role of School Nurses in the Context of Trauma emerged as the constitutive pattern. The current study enhances our understanding of the unique role played by school nurses as they address the profound needs of newly arrived children and their families, many of whom have survived trauma and face a number of barriers to accessing care.
Introduction
In the United States, approximately 132,300 school nurses (SNs) are caring for nearly 77 million school-age children in prekindergarten through grade 12, or about 25% of the total population (United States Census Bureau, 2019; Willgerodt et al., 2018). Additionally, the school population cared for by SNs is rapidly changing with an unprecedented influx of immigrants. Ninety million immigrants and their U.S.-born children account for approximately 28% of the total U.S. population (Batalova et al., 2020). According to the Pew Research Center, immigrants and refugees are regarded as newly arrived (henceforth “newly arrived children”) if their entrance into the United States occurred in the previous 5 years (Radford & Krogstad, 2019).
School nursing is a specialized practice of professional nursing that promotes individual and population health; and advances lifelong well-being and academic achievement for students (American Nurses Association [ANA] & National Association of School Nurses (NASN), 2017). In the context of discrimination and lack of access to formal healthcare and other social services, SNs serve a critical role oftentimes acting as the only source of healthcare for many newly arrived children (Hilfinger Messias et al., 2015). Yet there is limited research on experiences of SNs and how their schools may offer safe harbors and empathetic ports or promote healthy development and deliver services to children in immigrant communities (Capps et al., 2015; McNeely et al., 2017). This may be due in part to some of the feasibility challenges to conducting school-based research related to newly arrived children, such as language barriers and access to undocumented parents who may be hesitant to participate due to justifiable concerns of discovery (Gulb & Zayas, 2017). SNs have comparatively higher access to this population and are bolstered by an established trust with their parents. Given the existing knowledge gap related to the stressors affecting newly arrived children, we targeted SNs and formulated the following research question: What are the lived experiences of SNs in caring for newly arrived immigrant and refugee children in urban public schools in grades K-8? and deemed a qualitative phenomenological study to be the most appropriate study design.
Methods
Study Design
Study procedures were approved by the Office of Human Subject Research Protection at Northeastern University. The study utilized a qualitative approach guided by hermeneutic interpretive phenomenology based on Heideggerian philosophy (Crist & Tanner, 2003; Heidegger, 1962; Ironside, 2006). In phenomenology, qualitative researchers explore the personal meaning, composition, and core of the lived experience of specific phenomena (Edmonds & Kennedy, 2017). Interpretations of lived experiences allows contexts that might otherwise be taken for granted or overlooked to be explored deeply from the perspective of the expert, or those with the lived experience (Husserl & Ideas, 1931; Underhill et al., 2012). Approaching the proposed research question through a phenomenological lens allows insight into the SNs meaning and experience. Therefore, offering an opportunity to identify areas to address and improve in future policy, practice, and research initiatives that will be relevant specifically to SNs caring for children in this context.
Sample and Setting
A purposive sample of SNs was recruited by email and telephone through the Massachusetts Department of Public Health School Health Services and Massachusetts School Nurse Organization listservs from February 2019 through June 2019. Participants were considered eligible if they: (a) were full-time public SNs (including district public charter schools) who work in the Massachusetts cities with a population of at least 80,000 residents; (b) had at least 15% enrollment of English Language Learners in their school/district; (c) were certified through the Massachusetts Department of Elementary and Secondary Education; and (d) in the past year had worked with at least five newly arrived children in a Kindergarten - 8th grade urban school setting. Written and verbal consent were obtained.
Data Collection
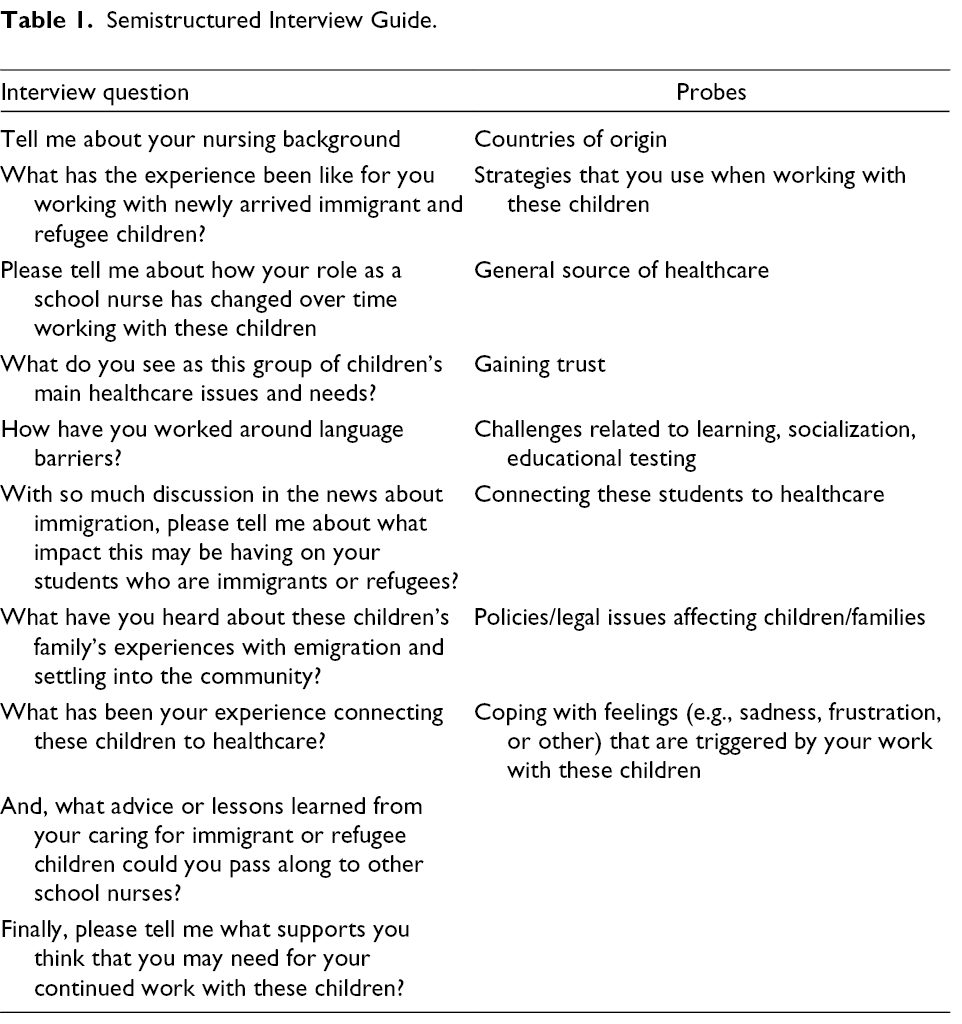
The first author conducted all interviews and wrote field notes (i.e., physical expressions, gestures and intonations) of the interview context directly after each encounter (Crist & Tanner, 2003; Underhill et al., 2012). Data were collected through one-time in-depth in-person (n = 16) or telephone (n = 4) interviews framed by a semistructured interview guide (Table 1). Data were collected until redundancy in data, or when common stories were being shared and no new themes emerged.
Semistructured Interview Guide.
Interpretation Procedures (Data Analysis)
All interviews were audio recorded, de-identified, and transcribed verbatim for analysis in a qualitative analysis software NVivo (NVivo, 2018). Pseudonyms were assigned to the participants to ensure privacy and to protect their confidentiality. Analysis was implemented with a team approach of committee members using a five phase hermeneutic interpretation process as described by Crist and Tanner (2003). In Phase One, hermeneutic interpretation began with examining the first few transcripts to gain an overall understanding and discuss the interpretive process. The early focus resulted in a refined semistructured interview guide in the hope of generating a thicker, richer description of narratives for future interviews. In Phase Two, each interpretive team member (JB, MUB, PB & CL), wrote one-to-three-page summaries of central concerns (i.e., important meanings or themes) and salient excerpts from each early participant’s story. The naming and coding of central concerns was an iterative process that acted as a vehicle for discussion. In Phase Three, team members discussed categories and themes across stories and agreed on a constitutive pattern (i.e., a thread that ties all of the themes together) considered the highest level of analysis (Diekelmann, 1993). A descriptive passage was chosen for the constitutive pattern to establish the essence of the study (Creswell & Poth, 2018; Crist & Tanner, 2003). In Phase Four, the team discussed final interpretations and attended to pending lines of inquiry (Crist & Tanner, 2003). In Phase Five, the manuscript underwent a final review by the entire five-member dissertation committee with emphasis placed on the discussion of the findings, recommendations for school nursing practice and implications for health policy regarding newly arrived children.
Results
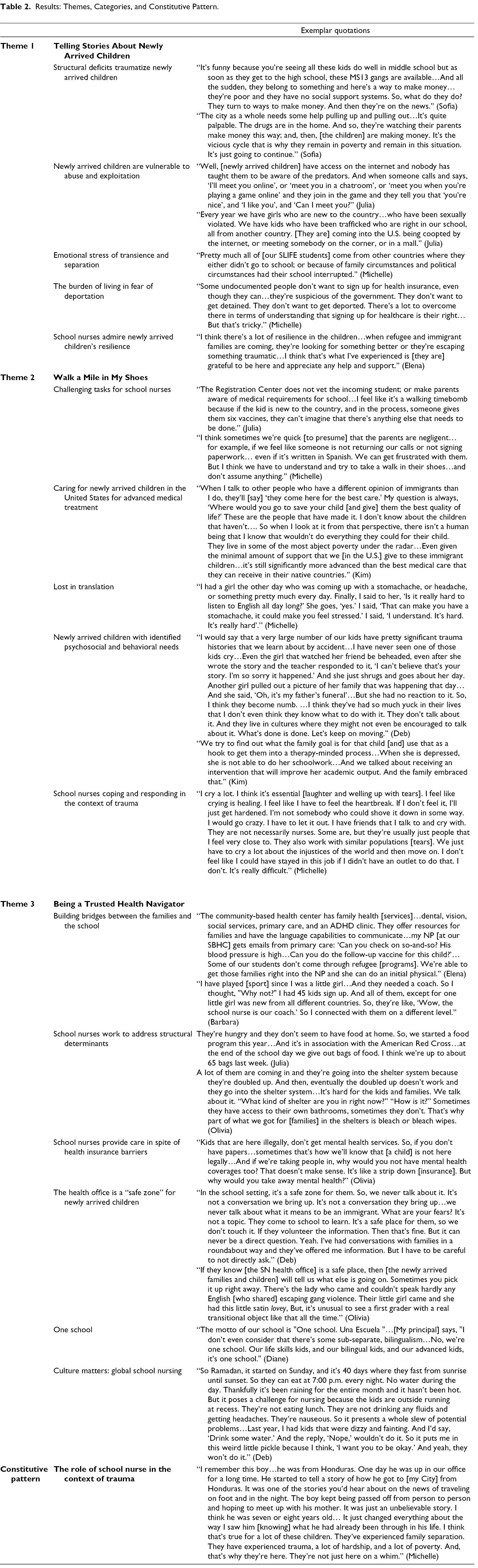
A total of 20 female participants consented to study participation with a median age of 57 years (range 25–71). Participants self-identified as Non-Hispanic. Most of the participants (n = 17) self-identified as White, while the remaining participants self-identified as African American (n = 1), Native American/African European (n = 1), or White/Mixed (n = 1). SNs worked within nine of the eleven cities in Massachusetts that met study eligibility criteria. All of the SNs were registered nurses (RNs) with a bachelor’s degree, 12 had a master’s degree, and two had a doctoral degree (n = 1 PhD; n = 1 DNP). The sample included participants with two to 43 years’ experience practicing as a RN (median 24.5 years); and one to 23 years practicing as a SN (median 13 years). English was the primary language for all 20 participants. Some participants reported speaking Spanish (n = 6), French (n = 1), or sign language (n = 1). Coding yielded a total of sixteen Categories, three main Themes, and one Constitutive Pattern (Table 2).
Results: Themes, Categories, and Constitutive Pattern.
Theme One: Trials and Triumphs—Telling Stories About Newly Arrived Children
The SNs illuminated the study phenomenon by sharing human experiences and in-depth perspectives in the context of being with the newly arrived children and their families. SNs described the significant structural deficits encountered by the children and their families along with the risks for exploitation, traumatic stress, and fear of deportation. In recounting their stories, the SNs voiced concerns about the effects on the children’s mental and physical health, shared frustrations with the challenges and barriers to healthcare delivery. The SNs also volunteered admiration for the resilience observed in these vulnerable children. Theme One features the following five Categories.
Structural Deficits Traumatize Newly Arrived Children
The SNs described structural deficits (i.e., lack of food, stable housing, parental supervision, healthcare access) as affecting mental and physical health and educational achievement of newly arrived children. Newly arrived children and their families were also dealing with housing instability (i.e., living in shelters and unsafe housing projects.) Olivia shared that one of the newly arrived children that she cared for “saw somebody get shot when he was getting off the bus.” Stephanie told the story of a 22-year-old immigrant single mother who had fled domestic violence; currently she earns minimum wage and lives in a shelter with her 8-year-old son who requires a one-to-one nurse in school. Stephanie was aware that sending the child to the hospital for medical reasons (e.g., high fever or respiratory crisis) deepens the financial crisis at home, because “for him to go home, [Mom] loses a day’s pay…so, a day’s pay for her is one less step towards getting out of this shelter.” Michelle shared, “There’s a [newly arrived] mom who has escaped domestic violence [with] a couple of kids…she is isolated and has to work all of the time…I just can’t imagine how hard that must be.”
Newly Arrived Children Are Vulnerable to Abuse and Exploitation
Several SNs described situations of predators online, bullying, social media, and sexual exploitation (i.e., sex/human trafficking). Julia explained that newly arrived children “are being caught up” with predators because the culture is so new to them here in the United States. Julia strongly believed that newly arrived children are much more at risk than U.S.- born peers for exploitation, adding: “We don’t have enough support systems in place to help kids and parents to understand the fear and the reality that their children are ‘ready targets’ for sexual predators.” Lisa described the problem of social media, teasing and online bullying in her middle school: “So, this social media stuff now is outrageous. I think it has exposed [newly arrived] kids to a lot of things they’re not ready to be exposed to.”
Ava shared, “[Newly arrived] parents work two and three jobs and the oldest child [may] take care of the younger kids.” Several SNs expressed concern over the predicament faced by parents who needed to work multiple low-paying jobs to make ends meet and thus had to rely on the older children to supervise their younger siblings for extended periods of time.
Emotional Stress of Transience and Separation
The SNs described situations where newly arrived children have experienced transience, separation from families, or both, “which is very traumatic, especially for young kids.” Beth recalled a fourth-grade Asian boy who had not met his parents until he immigrated to the United States at 5 years of age: “He has had issues from day one…behavioral issues, emotional issues…I can see that he is stressed a lot of the time.” Moreover, some newly arrived children are multiple years behind their peers, thus significantly older and placed in Students with Limited or Interrupted Formal Education (SLIFE) classrooms. Deb observed, “So, in this [Newcomer] school…students have either had a three-year gap in education or no formal education. If you conceptualize no formal education, what does that mean as far as healthcare goes?”
The Burden of Living in Fear of Deportation
Most SNs believed that fear of deportation has increased dramatically in the current political climate in which some children are “afraid of having their families ripped apart.” Several SNs described parents who did not want children to go to the school-based health center because of not wanting to be on the radar of needing something from the government, even if the child needed medical care. SNs described the “heightened awareness,” “secretiveness,” and “fear that kids walk around with.” Several SNs who work in a sanctuary city reported that fear of deportation was less problematic due to the limited cooperation with the federal government’s effort to enforce immigration law. Sofia shared, “We’re instructed not to speak to ICE [i.e., U.S. Immigration and Customs Enforcement] and send them to our Central Office or superintendent…We [are directed] to say, ‘I cannot speak to you…speak to the administration.” Sofia believed most newly arrived children and families “are here legally.” Emma voiced, “Our families are protected. ICE cannot come into a school system and have our children deported, so we’re very protective of them.” Ava voiced, “They’re very scared to give some of their information. So, it crosses my mind if they’re undocumented immigrants and, they’re just afraid to give too much.”
School Nurses Admire Newly Arrived Children’s Resilience
The SNs expressed admiration for the resilience and strength of newly arrived children in the face of difficult acculturation. Stephanie voiced admiration for the unyielding spirit of the medically fragile children: “the smile, the resilience and happiness…you can’t teach it, you can’t read it, you have to see it and experience it…it is the reason I go to work every day.” Many SNs shared that newly arrived children have peer communities where children speak the same language (e.g., Spanish, Portuguese, Haitian, Chinese, Vietnamese, Arabic) which helps with acculturation. Likewise, SNs identified families who found strength through community supports, especially those living in neighborhoods highly concentrated in their native culture.
As an example of this resilience Elena shared her favorite story about a young girl from the Middle East with a chronic medical condition and needed to be taught a self-care procedure: “When she came into our school, she spoke no English and by the next year, she was fluent. And by the time she was in sixth-grade, she sang at the graduation in her [own] language.”
Theme Two: Walk a Mile in My Shoes
Theme two reflects the SNs’ perspectives of what caring for a newly arrived children population entails on a day-to-day basis. SNs revealed tackling incomplete health records and incomplete immunization records while managing the challenge of newly arrived children and families’ lack of knowledge on the health requirements. Theme Two features the following five Categories.
Challenging Tasks for School Nurses
The SNs concurred that getting follow-up vaccines for newly arrived children is among the most trying aspects of the role. They described school registration centers that vary greatly in vetting processes to secure vital health records and immunizations. According to Deb, “Most of our kids come with no records of any immunizations.” The SNs repeatedly cited the recent Measles outbreak has spurred a call to action in getting children up to date with vaccines. Deb voiced that when children are registered for school, “They’re essentially getting a whole slew of first-round vaccines…I might be the first [healthcare provider] they see…. So, they’re leery of medicine.” The importance of establishing a relationship with a PCP is often lost on newly arrived children and families arriving from completely different healthcare systems where preventative care may not be the cultural norm.
Second, participants noted policies such as national immunization registries that link state to state might help SNs to deliver care to newly arrived children more effectively and efficiently. Julia noted “chasing down” vaccines “is a larger systemic problem…larger than just the local school [and] should be addressed systems wide. And it’s not.” Similarly, SNs agreed that newly arrived families frequently are unable to return phone calls or answer repeated letter requests for health records. The SNs reported newly arrived families leaving sick children at school because they are in the hands of a trusted medical professional and the families often refer to the SN as “doctor.”
SNs described how the SN role has changed over time in response to the changing student demographics. Most SNs voiced an increase in caring for a bilingual population and a heavier caseload. Elena explained, “We’re not seeing nearly the influx of immigrants that we have had in years past…when they were coming in [they came] through two [refugee] agencies.” Lisa spoke of extra children added to the school where she is an SN due to a sister middle school shutting down for renovations. Lisa lamented that the elimination of a bilingual guidance counselor was especially painful. These challenges test the most seasoned of SNs in meeting the goals of the SN practice to care for newly arrived children.
Caring for Newly Arrived Children in the United States for Advanced Medical Treatment
SNs also noted that complex, chronic, and/or advanced medical health problems were reasons for some families to bring their children to the United States: congenital disorders, cerebral palsy, osteogenesis imperfecta and seizures. Newly arrived children with unmet chronic conditions such as diabetes or disabilities further complicate healthcare navigation. Case management, continuing care, and follow-through are high priorities for immigrant families who also require education on serious health conditions and, as Emma noted, may need more education “on what’s next.” Several SNs identified the need to assist newly arrived families with follow-up for critical appointments as well as transportation to and from the specialist (i.e., to make the appointment happen.) Stephanie gave an example of a newly arrived child who had complex care needs and limited insurance. That child was denied formula for G-tube feedings, “the one piece he needs to be healthy.” Stephanie also described locating a wheelchair and a headrest that they adapted using “pool noodles and duct tape.”
Moreover, the SNs described newly arrived children and families who do not understand that dental health is important to overall health and well-being. Linda explained, “Sometimes they smile, and you’re shocked to see all of the metal and silver caps.” Many newly arrived children have never seen a dentist; and thus the SNs consistently referred to the children’s poor oral hygiene and problems such as black or broken teeth, severe oral pain, gum abscesses, halitosis, and general dental neglect. Most newly arrived families were characterized as “poor” and not able to attend to badly needed dental care as it is not prioritized in the hierarchy of survival. Some SNs advocated and defended a family’s decision to come to the United States to seek help by acknowledging the impact of poverty on families and by asking people to consider what they would do if they were in the same position.
Lost in Translation
The SNs described language barriers as the biggest challenge to their role in working with limited English-proficient children and families. With regards to overcoming language barriers, Deb discussed that “even having a translator, things get lost in translation.” Ava emphasized the importance of using an adult interpreter with children as opposed to native-speaking peers “to get to the bottom of the story.” In some cases the SNs relied on bilingual staff in the schools. Beth described an ESL (English as a Second Language) teacher who spoke Chinese. “She’ll drop what she’s doing, I’ll man her class…and she’ll come and make phone calls for me… That’s the biggest help.” Lisa was among several SNs who described using phone applications (such as Google Translate) to translate “very rudimentary things.” However, all SNs concurred that an interpreter is necessary for most, if not all, conversations with parents. Most SNs had access to a three-way phone interpretive services such as Language Line Services or Lionbridge but budgetary expenditures for such helpful mechanisms varied.
Regardless of the source, interpreter services and the quality of translation also varied. School-based health centers (SBHCs) often assist SNs by offering interpreter services on-site. Further, the SNs discussed the communication challenges when dealing with multiple dialects and native indigenous languages. Beth shared, “Certainly, within a year of being here, I see them speaking fluent English. Now, do they understand everything I’m saying, the nuances? Probably not.”
Newly Arrived Children with Identified Psychosocial and Behavioral Needs
The SNs identified newly arrived children with mental health issues such as PTSD, bipolar disorder, ADHD, anxiety, selective mutism, and depression. The SNs told stories that brought up the challenge of educating children with severe trauma histories. Several SNs spoke about newly arrived children who were cutting. Lisa shared a story about a newly arrived child with what she described as “true cutting,” adding “You could tell the cutting had been going on for a very long time in the upper thigh where you wouldn’t see it when she had her clothes on.” Several SNs had also observed some newly arrived children with what to them looked like hyper-startle responses to loud noises such as someone yelling or the sudden noise of books being slammed. Underlying many of the mental health issues is a history of trauma.
The SNs also described somatization that may manifest as a stomachache, headache or unexplained discomfort. The child may cry and be upset out of frustration. SNs noted the demands of acculturation on newly arrived children’s coping, which can then impact their ability to learn and form healthy relationships in school. For some, the stress of not being able to communicate in English can lead to acting out and physical altercations. Navigating mental health issues for newly arrived children is challenging and SNs expressed the need for more treatment options both in and outside of school.
School Nurses Coping and Responding in the Context of Trauma
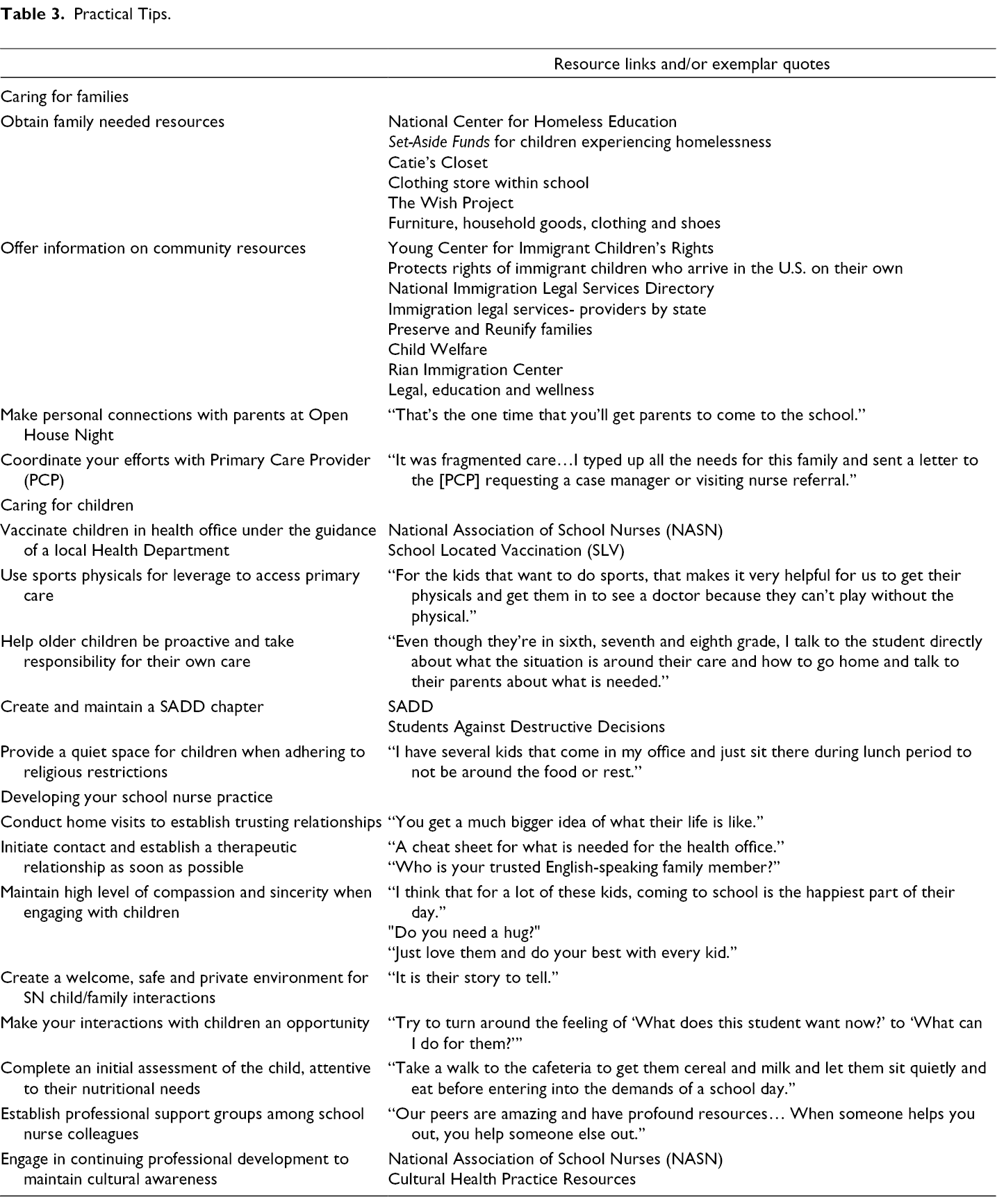
The SNs articulated practical tips or strategies for coping and responding that pervade all resulting themes and are summarized in Table 3. As they shared stories about serving on the frontlines and witnessing the impact of trauma among newly arrived children, some shed tears as they discussed challenging experiences that triggered feelings of helplessness, sadness and frustration. Stephanie voiced that caring for newly arrived children can be “sad, eye-opening and hard.” Most SNs revealed that coping might entail crying and venting to colleagues, family, and friends. Conversely, many SNs also used humor to cope. Physical activities such as going to the gym, swimming, dancing and digging in the garden provided another outlet for their job stress. The SNs’ empathy for immigrant children often circled back to personal protective feelings associated with their own children or grandchildren. Linda described the importance of saving emotional energy for her young daughters at home.
Practical Tips.
Theme Three: Being a Trusted Health Navigator
Establishing trust with newly arrived children and their families meant taking the time and seizing upon opportunities to build relationships. SNs assumed the role of a health navigator to bridge gaps in or barriers to services and to coordinate care with the school support team and community partners/healthcare providers. Theme Three features the following six Categories.
Building Bridges Between the Families and the School
Kim described the importance of the SN as the “tri-care provider” in the contexts of school, home and the medical community. The SNs described newly arrived children and families who do not know how to navigate the educational and healthcare systems. Emma voiced, “So it’s our role as school nurses to try to hook them into services.” The SNs recognized the importance of newly arrived families establishing a relationship with a PCP to avoid partial or piecemeal care; and to prevent overuse of Emergency Rooms for episodic illnesses that could be managed in a clinic setting (e.g., minor asthma symptoms, earaches, sore throats). The theme of being a trusted healthcare navigator conjures up the metaphor of building bridges. SNs are a bridge between the school and the School Based Health Centers, especially when both are housed in the same building, and they promote access to: (a) health insurance; (b) immunizations and physical exams; and (c) mental/behavioral health counseling. Some of the SBHCs with which the SNs worked had formal links with government programs for refugees (including unaccompanied minor children.) Overall, SNs described the local community health center as the main source of healthcare for newly arrived children and families.
School Nurses Work to Address Structural Determinants
Several SNs described their work that extends into children’s homes or classrooms as directly mitigating the severe impact of scarce resources on health. These efforts included home visits to conduct first-hand assessments and providing food and supplies to children. The SNs also offered resources to newly arrived children and families ranging from bags of food, toiletries and clothing to arranging cultural support groups at school. One SN offered a weekly peer group for parents that served coffee and celebrated holidays. The SN recounted a new mom who she “pushed” into the support group and asked the other “ladies” to help her out. Such supports help families to acculturate to their new surroundings and reduce isolation.
School Nurses Provide Care in Spite of Health Insurance Barriers
Health insurance is key in accessing healthcare for newly arrived children and families. The SNs concurred that referring to community health centers was the most effective strategy to help families access health insurance or free care. Several SNs could relate to the family’s plight of tackling health insurance and shared personal stories of their own insurance nightmares. It can be a double-edged sword for families if accessing health insurance increases their visibility and vulnerability for discovery (i.e., red flag for deportation.) Deb described a “mindboggling” scenario about a newly arrived refugee child from Africa who needed assistance locating a PCP. The parents sent paperwork from his assigned refugee agency with the word “help” on it. Deb spent three hours trying to locate a PCP for the child, calling eight primary care clinics including the biggest family healthcare center in her city which typically accepts refugee children. “So, we ended up finally finding some [refugee] agency that was willing to take them on…just having someone that can speak to them is the biggest problem.”
The Health Office is a “Safe Zone” for Newly Arrived Children
In the United States there is no consideration of documentation status when it comes to schools which was viewed as instrumental in gaining the trust of newly arrived children and families. The SNs described their health office as a refuge for newly arrived children to take a break from the stress of the day. Newly arrived children who come in regularly for medications or treatments are especially comfortable with the SN and thus may be more apt to freely express their thoughts and fears. Kim offered a story of a (Caribbean) boy who asked, “Does it make me bad because I’m here and I’m not supposed to be?” Kim recalled feeling overwhelmed by the boy’s question and stated that she had to take a moment to regain her composure. The same (Caribbean) child also revealed, “Sometimes my dad yells, because we don’t have enough food in the house. And I’m worried.” Kim responded, “This is a very hard time, but those are adult issues… and we’ll work with your mom and dad to make you safe.” Schools are a safe place where newly arrived families can expect their children to be supported academically and emotionally.
One School
The SNs often described the importance of school unity and feeling connected to the school team. Many SNs recognized the need for the principal’s support in their practice caring for newly arrived children, particularly with regards to interpreters and backing for requests for state-mandated vaccines. Kim voiced appreciation that her principal includes her in “common planning time” when she meets with the Student Support Team and invited community partners to discuss the needs of children, most of whom are English Language Learners. The fact that one SN received space for her parent mentor group signified that the school administrator was empathetic to her work. Olivia recounted lessons learned from her work with a young boy from [the Middle East] who presented with a “mangled arm” that he tried to hide under a sweatshirt. The child had been made fun of in the past. “So, we went to the classroom [and I said] this is what makes him special and I know you guys will be good to him.” This approach appeared to work as the boy went on to wear short sleeves. Olivia explained: “I think if something’s going on, it’s better to talk to the kids and explain it. Don’t let them figure it out.” Her approach was intended to tap into her school’s community spirit and the protection of its members.
Culture Matters: Global School Nursing
The SNs told stories of cultural sensitivity and accommodating cultural practices and differences, describing “small” and “undernourished” newly arrived children struggling to adapt to eating American food. The SNs touched on the pride of newly arrived families and discussed honoring boundaries even when they knew the child could benefit from help (e.g., not offering clothing or food to families who are not receptive to handouts.) Two SNs detailed their first encounters with the Asian healing practice of “cupping” (i.e., circular pronounced bruises) remnants of which the SNs mistook as possible signs of abuse until they were educated by colleagues about the custom. Other SNs voiced unease over Ramadan fasting and detailed challenges with tired and hungry children. Stephanie told a frenzied story of a new [African] child who was “pulling out yellow pills” which her parents had given her to take during the school day: “The girl was screaming and trying to run away...We had to find somebody that could speak to the family to explain to them [school policy]…And the parents were lovely. ‘We are so sorry. It won’t happen again’.”
Constitutive Pattern: The Role of School Nurse in the Context of Trauma
The constitutive pattern that emerged across all interviews was the SN’s role in the context of trauma and challenges to caregiving. SNs told rich and often raw stories about caring for newly arrived children with trauma from acculturation or histories of trauma pre-, post-, or during migration. The SNs encounters with newly arrived children and their families, many of whom had experienced and/or were continuing to experience trauma, had a profound effect on the way they perceived their role as a trusted health navigators. They illustrated the importance of empathy and compassion in providing culturally sensitive and holistic nursing care. See Table 2 for the exemplar quote that captures the meaning of the role of the SN in the context of trauma.
Discussion
This phenomenological study explored the lived experiences of 20 SNs caring for newly arrived children in urban public schools, grades K-8. The SNs experiences reflected the inherent complexity of caring for newly arrived children and their families. The SNs shared stories about working with these linguistically and culturally diverse children, many of whom presented with health issues that threatened their physical, emotional and social well-being. The SNs voiced concern about the gaps in health and mental health service utilization among newly arrived children, who may be the most underserved segment of the U.S. population (Hacker et al., 2015; Toppelberg et al., 2013). Study findings enhance our understanding of the SN’s role in the context of trauma and challenges to caregiving. The Community/Public Health component of the Framework for 21st Century School Nursing Practice promotes population-based care, access to care, health equity and health education (ANA & NASN, 2017).
The SNs identified the credible fear of undocumentedness (i.e., lack of birth certificate or citizenship) creates a barrier to accessing healthcare in general and mental healthcare in particular, underscoring the critical need for education on health and guidance for access to services (Hilfinger Messias et al., 2015; McGuire, 2014). McGuire (2014) has suggested that the social construction of undocumentedness may be regarded as a kind of violence toward the immigrant because of the marginalization, trauma and suffering it creates. SNs offer a safe haven for the provision of services to newly arrived children, and by extension, they may have the opportunities to help immigrant parents and immigrant communities overall (Capps et al., 2015).
The SNs shared stories about the impact (stress, sorrow) that fear of deportation has on newly arrived children and their families, suggesting that the fear of deportation has increased dramatically under the current political climate. The intensified fear of deportation affected SNs decision making around when/how to contact parents in order to avoid disturbing them at work or calling attention to their employers. Our findings indicate that parents’ legal vulnerability to detention or deportation are indeed associated with stigma, fears of separation, anxiety, depression and social isolation (Ataiants et al., 2018; Dreby, 2012; Toppelberg et al., 2013; Zayas & Heffron, 2016). Understanding parents’ fear of detention and deportation has important implications for promoting health and well-being of newly arrived children and families.
The SNs provided narrative accounts of structural deficits (i.e., lack of food, stable housing, parental supervision, healthcare access.) Indeed, newly arrived children undergo a profound disruption in essential experiences of security and structure that are critical for healthy development (Seery et al., 2015). Promising practices point to directives/policies at the Federal and State levels that can address structural deficits and poverty among newly arrived children. For example, SNs can connect newly arrived families to programs such as “WIC” (i.e., special supplemental nutrition programs for women, infants and children). Further, SNs can advocate that WIC be expanded to newly arrived children over 5 years old to improve nutrition, screening and referrals to health, welfare and social services (United States Department of Agriculture, 2019).
SNs also observed that newly arrived children under their care, who had come to join their parents in the United States, may suffer psychological damage caused by years of separation (Nazario, 2014). The mental health toll was most evident within stories of SNs working with SLIFE children (Students with Limited or Interrupted Formal Education). As an advocate, the SN plays a vital role in the assessment of the physical and emotional needs of SLIFE children; and in assuring that appropriate referrals and follow-through are carried out with regards to immunizations, dental and physical/mental healthcare. Further, SNs validated their role in the protective circle of security that supports children who are separated from detained or deported parents; children who present with loss of appetite, stomachaches, headaches, poor sleep, nightmares, crying, clingy behavior, anger, fear, anxiety, and withdrawal (Chaudry et al., 2010; Dreby, 2012; Park & Katsiaficas, 2019).
SNs expressed admiration for the resilience and strength of newly arrived children in the face of the challenges to acculturation. Witnessing the resilience and strengths of newly arrived children and families spawned hope and appeared to be a critical factor for SNs continuing to care for this unique population who have endured difficult circumstances. In response to stressors triggered by their work with newly arrived children, the SNs identified coping strategies such as venting, crying, praying and exercise. A recent qualitative study of Swedish SNs described experiences working with unaccompanied refugee children and adolescents (Musliu et al., 2019). The authors highlighted the importance of SNs’ self-awareness to promote self-care. SNs also expressed a need for personal and professional development in trauma focused care for children and adolescents who had been exposed to chronic trauma and adversity (Musliu et al., 2019).
SNs play an essential role in health promotion and chronic disease management for newly arrived children (ANA & NASN, 2017; Council on School Health, 2016; Maughan et al., 2018). This study underscores the critical role of SNs as trusted health navigators and the importance of forming partnerships and alliances with families and community providers to promote newly arrived children’s health and safety, which in turn impacts their educational achievement. Narratives of the SNs succinctly echo the sentiment of the American Academy of Pediatrics that no child should live in fear and that what newly arrived children deserve the most is to be healthy and safe (Stein, 2017).
Study Limitations
Despite the strengths of this study, there are also some limitations. This study used a small purposive sample of SNs recruited from urban public schools in Massachusetts, thus limiting transferability to SNs working in other states and school settings. Furthermore, in comparison to many other states, Massachusetts is considered to offer more generous health services and benefits to newly arrived children (Capps et al., 2015).
Although the participants in this study reflect national demographics (gender and race/ethnicity) for SNs, they lacked diversity in that they were all female, Non-Hispanic, and predominantly White. Walter (2017) argues the voice of White privilege (i.e., “unearned privilege”) in nursing is the result of unequitable social systems that award dominance to some groups and subordination to others. The majority of the SN workforce identifies as female (98%) and White (87%) (Willgerodt et al., 2018). We acknowledge our study presents narratives (i.e., results) based on individual participant’s bias and stereotypes inevitably brought to the table.
Implications and Recommendations for School Nursing Practice and Research
An essential component to ensuring a well-prepared SN workforce is education, whether that be in the form of their professional development (i.e., continuing education) or advancing their degrees. A well-educated SN workforce is better prepared to lead care navigation with community partners and to advocate for and connect newly arrived children and families to needed services and resources. Nursing’s workforce in general and school nursing in particular could greatly benefit from attracting a more racially/ethnically diverse workforce, one that more closely represents the diversity of the populations they serve.
It is imperative for interdisciplinary efforts to critically examine current school health policies and procedures and to work collaboratively to make improvements as needed. For example, assistance with language barriers is vital to working with newly arrived children and families. SNs need access to cultural brokers, interpreters, high quality three-way phone interpretive services, translated documents and language classes. Additional school policy-related actions on behalf of newly arrived children and their families include: (1) National Immunization Registries; (2) Entitlement to comprehensive health insurance including mental and behavioral healthcare; (3) Support for and addition of more SBHCs in communities with growing numbers of newly arrived children and families; and (4) Fostering professional development for all school personnel on trauma informed care and cultural humility. For example, SNs need federally funded state-level immunization information systems to link immunization data across states to decrease reliance on medical record abstraction or parental report (Fuller et al., 2017). Further, SNs would benefit from support groups to talk about their own “trials and triumphs” regarding this unique population.
The following are suggested research priorities for supporting the SN role when caring for newly arrived immigrant and refugee children: (1) exploring barriers and facilitators to accessing and engaging in routine pediatric healthcare; (2) investigating child health outcomes related to care coordination and continuity tailored to the needs of newly arrived children; (3) studying the impact of access to comprehensive health insurance on newly arrived children’s physical and mental health outcomes; (4) examining best practices in schools for promoting holistic health and cultural humility to support healthy development; and (5) exploring the impact of incorporating trauma informed care into school health. Acquiring new knowledge through research can increase our understanding about how to tailor school-based, health-related interventions for newly arrived children and enhance their educational achievement.
Conclusion
SNs are accountable health professionals working with vulnerable newly immigrated children and play a pivotal role in engaging families and helping to manage the children’s healthcare needs and are uniquely positioned to provide needed care. Many of these families are living in abject poverty, with the credible fear of deportation. Laws and policies related to immigration affect newly arrived children’s physical health, mental health, and psychosocial well-being. Therefore, it is incumbent on all school personnel to consider what may be at stake if newly arrived children do not receive effective health services and interventions to promote well-being and academic achievement. Healthcare and education for all children is a moral imperative.
Footnotes
Acknowledgment
The authors offer sincere thanks to Dr. Allan Osborne for his expert consultation and generous time supporting this manuscript’s publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Theta-at-Large and the Gamma Epsilon Chapters of Sigma Theta Tau and the Massachusetts School Nurse Organization.
Author Biographies