
Abstract
The COVID-19 crisis has starkly highlighted the vulnerability of businesses and underscored the critical importance of organizational resilience. Firms across multiple sectors—particularly non-essential businesses—have suffered a heavy blow during the height of the pandemic. Guided by the resource dependence theory and using a proprietary and rich dataset from a leading online-to-offline platform for medical aesthetics services—a typical type of non-essential business—we find that the pandemic adversely affects clinic performance in terms of the number of orders a clinic received on the platform. However, the adoption of telemedicine enables clinics to mitigate the negative impacts of the pandemic on clinic performance, which is referred to as “digital resilience.” Moreover, we reveal that the mitigating effect of telemedicine adoption on clinic performance is stronger for smaller clinics and those focusing on lower-risk products. Additional analyses reveal that telemedicine also bolsters consumer interest in specific products during the pandemic, regardless of the product risk level. Furthermore, telemedicine takes effect amid the pandemic mainly by cultivating the interests of more experienced consumers. Our study contributes to the operations management literature by exploring the impacts of COVID-19 and digital resilience in non-essential sectors. It also offers practical insights for these businesses to improve their crisis responses and gain strategic digital resilience in the face of a sudden crisis.
The COVID-19 pandemic that began at the end of 2019 has infected over 765 million people and caused more than 6 million deaths around the world (WHO, 2023). COVID-19 and the attendant containment policies have caused devastating disruptions across many industries (Chetty et al., 2024; Ge et al., 2022; Liu et al., 2023). An important issue thus arises regarding how firms can effectively respond to a sudden crisis and develop organizational resilience (Dohmen et al., 2022). Specifically, attention needs to center on how firms can preserve their core functions, persist through and adapt to the adverse environmental changes, and ultimately reduce losses and survive the crisis.
Faced with the pandemic, many brick-and-mortar firms turned to online-to-offline (O2O) platforms, and those already online sought to deploy digital technologies more actively to reach and retain consumers (Han et al., 2022). For instance, healthcare providers adopted telemedicine, restaurants and retailers offered contactless orders, and insurers relied on online self-service claim assessments to maintain business (McKinsey, 2020). Firms’ deployment and use of such digital technologies to resist and recover from disruptions is generally referred to as digital resilience (Reeves and Whitaker, 2020). Although the pandemic calls for special attention to digital resilience, there is still insufficient empirical evidence on whether, how, and when active adoption of digital technologies is effective in coping with the crisis.
Furthermore, the pandemic crisis may have affected different businesses and sectors differently. Existing research has predominantly examined the impacts of COVID-19 on overall consumption patterns (e.g., Bartik et al., 2020; Chen et al., 2021; Chetty et al., 2024) and essential businesses like groceries, catering, and healthcare (Glaeser et al., 2021; Liu et al., 2023; Raj et al., 2020). There is also a body of literature in operations management (OM) that has specifically focused on how COVID-19 affects the performance of essential businesses via operational capabilities such as logistics capacity (Blackmon et al., 2021; Delasay et al., 2022; Han et al., 2022; Shen and Sun, 2023). However, the impact of COVID-19 on non-essential businesses whose products or services are not necessary to people's daily lives (e.g., personal care, public entertainment)— has received much less attention. Governments usually enforce much more stringent policies, such as mandated closures, on non-essential businesses during the pandemic (Bartik et al., 2020; Cox et al., 2020). Extant empiricism has also suggested that a crisis like COVID-19 can affect consumers’ consumption patterns and shift their attention more to essential (vs. non-essential) consumption (Goolsbee and Syverson, 2021). The heightened operational disruptions in non-essential businesses create an urgent need to understand how operational transformation, particularly through digital capabilities, can enhance organizational resilience during the pandemic crisis.
In this paper, we focus on a unique non-essential industry, medical aesthetics, to examine the impact of the pandemic and digital resilience. Medical aesthetics refers to a branch of medical services that aim to improve patients’ physical appearance, rather than to cure a disease, and are provided by professionals with aesthetic training (Yuan et al., 2024). It is thus considered non-essential but life-enhancing and highly identity-relevant (Marinova et al., 2017). The services range from less invasive dermatological treatments (e.g., laser and light treatments, neurotoxin injections) to more invasive plastic surgeries (e.g., nose augmentation, invasive face lifting) that carry higher risk and uncertainty (Yuan et al., 2024). The industry is fast growing, with a global market size valued at US$22.84 billion in 2023 and a projected annual growth rate of 13.0% between 2024 and 2032 (Fortune Business Insights, 2024). Due to various containment policies imposed on this industry, such as mandated closures and restricted capacity, the entire industry suffered significantly in the first quarter of 2020 after the initial outbreak of the pandemic (BCG, 2020). In fact, 77.8% of medical aesthetics clinics closed temporarily due to COVID-19 (ISAPS, 2020). As a result, many of them turned to online platforms and adopted digital tools to maintain business continuity.
This paper examines whether, how, and which types of medical aesthetics clinics can gain business and reduce loss through adopting digital technologies amid the pandemic. Specifically, we focus on the provision of telemedicine—a form of remote diagnosis via information and communication technologies—and aim to investigate whether medical aesthetics clinics can gain resilience through the adoption of telemedicine. Additionally, we explore how such effects may vary depending on the types of clinics. We draw on the resource dependence theory (RDT), which provides a framework for understanding how organizations are dependent on the external environment for the provision of vital resources, as well as how they can manage and reduce this dependence to sustain operations when facing resource constraints (Pfeffer and Salancik, 2003). During the pandemic, medical aesthetics clinics were faced with reduced supplies, financial capital, labor, business hours, and suppressed demand for their services. Such destabilized resource access led to decreased clinic performance. We predict that clinics can mitigate such resource constraints and regain resources during the pandemic through adopting digital service delivery, telemedicine. However, how effectively clinics can leverage telemedicine to regain resources and sustain business also depends on their ability to understand the technology and assimilate it into daily operations—known as absorptive capacity (Cohen and Levinthal, 1990). Accordingly, we further propose that the mitigating effect of telemedicine during the pandemic will vary based on the type of clinics in terms of clinic size and the nature of products offered, which could affect clinics’ absorptive capacity in utilizing telemedicine.
To verify our predictions, we collaborated with a leading O2O platform for medical aesthetics services in China, where clinics can promote their doctors and products, and prospective consumers can browse and search for information, add desired items to their favorites or shopping carts, and place orders. After placing orders, consumers can schedule appointments with the clinic through the platform and receive the actual treatments offline. Figure EC-A1 describes a typical flow of consumer activities on the platform. While all the treatments are offline, clinics can choose to offer telemedicine services on the platform for pre-treatment activities such as consultation, diagnosis, and recommendations, which are free to consumers.
Using a proprietary and rich dataset from this platform, we show that the pandemic negatively affects clinic performance (i.e., the number of orders the clinic received on the platform). Nonetheless, clinics can alleviate such adverse effects through the provision of telemedicine on the platform. Our findings thus affirm the critical role that digital technologies play in creating organizational resilience in response to the pandemic crisis. Furthermore, the observed mitigating effect of telemedicine is more pronounced for smaller clinics and those specializing in lower-risk products. Additional analyses on consumers’ product interest (i.e., add-to-favorite and add-to-cart behaviors) reveal that the mitigating effect of telemedicine on product interest is stronger for smaller clinics, while it holds irrespective of clinics’ product risk level. We further find that telemedicine takes effect mainly by helping more (vs. less) experienced consumers cultivate interests.
Our research makes several contributions to the literature. First, it extends OM literature beyond essential business operations during COVID-19 (Blackmon et al., 2021; Delasay et al., 2022; Han et al., 2022) by examining how non-essential service operations adapt to pandemic disruptions. Second, by exploring the mitigating effect of telemedicine adoption, a new form of service delivery, and its boundary conditions of clinic size and product risk level, our empiricism adds to the growing literature on digital resilience amid the pandemic (Dohmen et al., 2022; Liu et al., 2023; Swink et al., 2025). Third, we join the small number of studies within the healthcare IT arena, extending the focus to telemedicine, and establishing its economic value during the pandemic. Finally, our study expands the scope of RDT by applying it to a new situation—the resource dependence of non-essential business amid a pandemic crisis—and explores the effectiveness of a novel form of resource dependence management strategy, specifically, the adoption of digital services.
Literature Review
Related Work on Impacts of COVID-19
The extant OM literature has examined the impacts of COVID-19 and the corresponding containment policies on people's health outcomes (e.g., Wang, 2022), as well as business performance (Blackmon et al., 2021; Delasay et al., 2022; Ge et al., 2022; Martinez-de-Albeniz et al., 2025; Shen and Sun, 2023). For instance, research shows that offline consumption in China in 2020 decreased by an estimated 1.22 trillion RMB, or 1.2% of China's 2019 GDP (Chen et al., 2021). E-commerce consumption, though, was more resilient during the pandemic with a significant drop and recovery pattern, which could be explained by logistic capacity (Han et al., 2022).
Our research transcends this stream of literature in two ways. First, extant work has predominantly focused on the impact of COVID-19 on essential businesses, such as groceries, food delivery, or healthcare (Delasay et al., 2022; Liu et al., 2023; Raj et al., 2020), while attention to non-essential sector has been sparse (with the exception of Sim et al. (2022), which shows that the pandemic has reduced music consumption because of reduced mobility and commuting time). Second, how firms, especially non-essential businesses, can build resilience in response to COVID-19 remains largely unexplored. Our work differs from prior studies on digital resilience (Cong et al., 2024; Liu et al., 2023) by centering on a non-essential healthcare industry, medical aesthetics, amid the pandemic. Unlike traditional healthcare, the pandemic may have more severely affected the supply and demand of medical aesthetics services. Moreover, cultivating consumer interest in specific products may not be a significant concern for essential healthcare, but it plays a critical role in the continuation of non-essential business. Understanding the extent to which medical aesthetics clinics are affected by the pandemic and how they can gain resilience via digital technologies is thus of crucial importance.
Related Work on Telemedicine
Telemedicine is a telehealth service that enables physicians to connect with patients to make a diagnosis, suggest specific solutions and guide treatments, and provide support at a distance in real time. Prior research in OM and IS literature has found that telemedicine, in general, can improve hospital or physician outcomes, including increased care efficiency (Li et al., 2016; Sun et al., 2020), offline visits (Bavafa et al., 2018; Wang et al., 2020a), and productivity and revenue (Liu et al., 2023; Rajan et al., 2019). However, whether telemedicine augments consumer access and clinic performance in non-essential healthcare amid the pandemic is opaque. Different from the use of telemedicine in traditional healthcare domains, such as emergency rooms (Sun et al., 2020) and chronic care (Rajan et al., 2019)—which has been almost compulsory during the pandemic—consumers of medical aesthetics services may have simply delayed their consultations and consumption during the pandemic rather than opting for other forms of service delivery (i.e., telemedicine). In addition, deploying an alternative service delivery method amid the pandemic also requires swift and careful management of various operational aspects. Hence, questions remain as to whether, how, and under what situations telemedicine may help medical aesthetics clinics gain resilience amid the pandemic.
Theoretical Foundation: Resource Dependence Theory (RDT)
RDT posits that an organization's vital resources—such as capital, labor, and materials—are often constrained by its external environment (Pfeffer and Salancik, 2003). These resources are crucial for survival, so organizations rely on the external environment but must also strategically manage these dependencies to ensure continued access to resources. RDT is one of the most influential theories in strategic management (Drees and Heugens, 2013), and has recently been applied to explain the resource dependence and disruption caused by external crises, such as the pandemic (e.g., Craighead et al., 2020; Gebhardt et al., 2022). The pandemic and associated containment policies have resulted in tighter constraints on firms’ essential resources. In this highly disruptive and uncertain environment, reducing resource dependence to build resilience presents a critical challenge for firms. However, whether organizations can effectively reduce resource dependence during the pandemic through new technology adoption remains under-researched (Gebhardt et al., 2022). RDT thus provides a suitable framework for understanding the pandemic's impacts on firm performance and evaluating the effectiveness of strategies aimed at reducing resource dependence (Craighead et al., 2020).
Furthermore, firms vary in terms of their absorptive capacity, that is, their capability to recognize, assimilate, and apply new knowledge (e.g., new technology) based on their specific needs (Cohen and Levinthal, 1990). Consequently, the extent to which firms can regain resources and sustain organizational performance through management strategies to navigate crises may be contingent upon their absorptive capacity (Drees and Heugens, 2013; Wang et al., 2020b; Zahra and George, 2002). Prior research has shown that absorptive capacity is largely affected by organizational characteristics; firms with a rich base of knowledge, efficient communication structure, and an environment of learning and innovation are better equipped to appreciate the relevance and potential applications of new technologies (Cohen and Levinthal, 1990; Jansen et al., 2005).
This paper builds upon RDT and examines how telemedicine can help clinics reduce resource dependence and thus achieve digital resilience amid the pandemic. Furthermore, drawing on studies related to absorptive capacity, we posit that clinics may differ in their absorptive capacities in using telemedicine to reduce resource dependence amid the pandemic. This study focuses on two important characteristics of clinics that may affect their absorptive capacity, that is, clinic size and the nature of products provided, which reflect their organizational structure as well as prior knowledge in delivering certain types of services, respectively (Cohen and Levinthal, 1990; Jansen et al., 2005).
Hypothesis Development
Figure 1 presents the conceptual framework of this paper. Guided by the resource dependence theory, we hypothesize that the pandemic intensifies clinics’ constraints on resources, thereby impairing their performance (H1). However, clinics can reduce this resource dependence and regain resources by adopting telemedicine, which mitigates the adverse influence of pandemic (H2). Furthermore, clinics vary in their absorptive capacity to leverage telemedicine to regain resources amid the pandemic, hence the moderating role of clinic size (H3) and the nature of products (H4). Below, we will elaborate on each hypothesis.
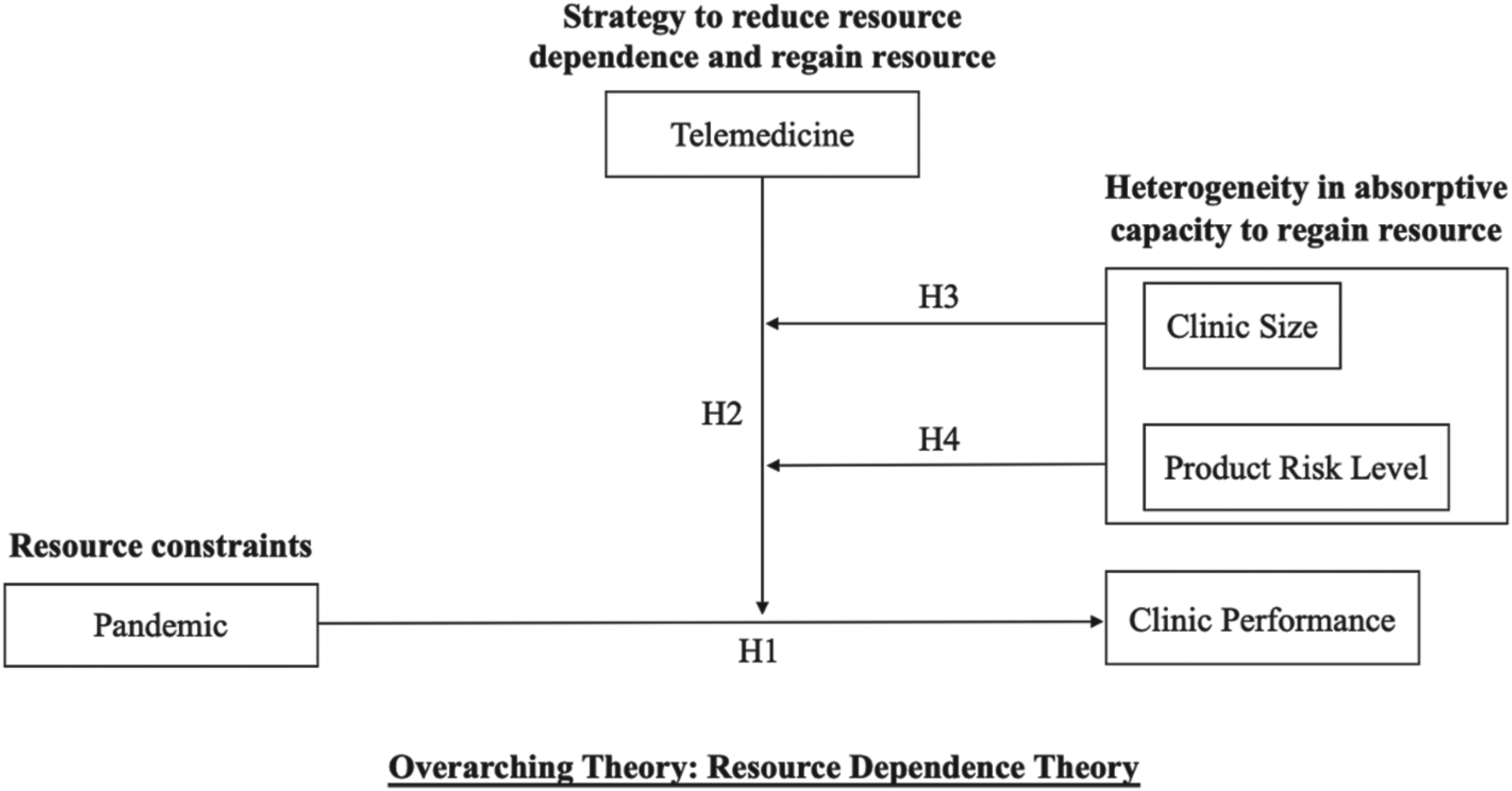
Conceptual framework.
As RDT suggests, firms need to rely on the external environment for resource access to survive and succeed, and their service capacity is vulnerable to environmental uncertainty (Pfeffer and Salancik, 2003). The non-essential nature of the medical aesthetics industry also makes market demand especially critical to the growth and survival of clinics during the pandemic. As such, we predict that the pandemic will constrain the critical resources medical aesthetics clinics require with respect to both operational capacity and consumer demand. Consequently, their performance will be impaired. We define clinic performance as a clinic's ability to generate revenue—which is typically measured by the number of orders received on the platform.
On the supply side, clinics are highly dependent on their external environment for vital resource access, including human capital and operational capacity, raw material supplies, and financial funding, that are necessary for production and operations (Pfeffer and Salancik, 2003). The pandemic-induced lockdowns and restrictions have resulted in delays or complete halts in the supply of critical inputs such as medical supplies. Additionally, government mandates have forced them to shut down their offline operations or reduce business hours during the pandemic (Bartik et al., 2020). Some employees have been unable to return to work because of the home quarantine practices. The economic downturn triggered by the pandemic has also led to tightened financial markets, making it more difficult to secure necessary funding (Ding et al., 2021). Overall, with various resources disrupted amid the pandemic, clinics’ production capacity is severely constrained, thereby adversely affecting their performance.
On the demand side, the pandemic has altered consumer behavior and demand patterns, resulting in a significant decline in demand for non-essential services. In particular, the pandemic has threatened many consumers’ basic living needs for health and food (i.e., temporary food supply shortage), as well as induced possible financial changes (i.e., loss of job or other sources of income) (Cox et al., 2020). Hence, consumers are unlikely to consider non-essential medical aesthetics services until their basic needs are fulfilled. The limited interactions outside the home, as well as concerns about the evolving pandemic and fears of infection (Goolsbee and Syverson, 2021), may have potentially decreased consumers’ emphasis on their appearance, which in turn reduced the market demand for medical aesthetics services. Limited market resources, particularly consumer access, thus led to dampened clinic performance amid the pandemic. Therefore, we propose,
H1: The pandemic has had a negative impact on clinic performance.
Mitigating Effect of Telemedicine (Digital Resilience)
Resource dependence theory (RDT) suggests that firms adopt different coping strategies to manage their resource dependence on external environment and minimize losses when faced with crises (Pfeffer and Salancik, 2003). We predict that clinics can reduce resource dependence amid the pandemic through adopting telemedicine. This approach enables clinics to stabilize the supply of critical resources necessary for operations (Drees and Heugens, 2013) and stimulate consumer demand amid an environmental crisis (Ahuja, 2000). These efforts ultimately help clinics cultivate consumers’ product interest and mitigate the negative impact of the pandemic on their performance.
On the supply side, telemedicine may help clinics overcome the resource constraints imposed by the pandemic and related containment policies. In particular, telemedicine reduces the need for physical space and associated expenses such as utilities and in-clinic staffing, thereby easing financial burdens and lowering the need for supplies. Clinics can also leverage the expertise of professionals who are physically absent from the clinics, hence expanding their pool of available staff.
On the demand side, telemedicine allows clinics to overcome the time and location barriers for consumers by reducing the cost associated with visiting clinics (Hwang et al., 2022). Therefore, clinics have more opportunities to access consumers amid the pandemic. When offline services are suspended or limited during the pandemic, connecting consumers with doctors via telemedicine can be an effective way to maintain customer relationships, cultivate their product interests, and reduce uncertainty (Gillman-Wells et al., 2021; Liu et al., 2020). This is particularly important for increasing conversions for medical aesthetics services, given their non-essential, high uncertainty, and identity-relevance nature.
With no telemedicine services available, clinic performance is largely dependent on the impact of the pandemic and the corresponding containment policies. The pandemic has likely decreased clinics’ offline service capacity and customer demand, leading to a strong negative impact on clinic performance. Therefore, we propose,
H2: Telemedicine adoption mitigates the negative impact of the pandemic on clinic performance.
Moderating Effect of Clinic Size
Drawing upon RDT and studies on adsorptive capacity, we predict that the effectiveness of using telemedicine to reduce resource dependence during the pandemic hinges on clinic size as firm size is often considered a major determinant of a firm's absorptive capacity (Cohen and Levinthal, 1990; Ding et al., 2021). We argue that, either larger or smaller clinics may have developed enhanced resilience to cope with resource dependence through telemedicine amid the pandemic. While large firms tend to have access to more resources, smaller firms may have the ability to stay nimble in the face of adversity (Ambulkar et al., 2015), which could affect the extent to which a clinic can effectively leverage telemedicine amid the pandemic (Ge et al., 2022). Hence, we propose two competing hypotheses regarding the moderating role of clinic size.
On one hand, we expect that larger clinics will be better equipped to survive the pandemic crisis through the active adoption of telemedicine. Compared to smaller firms, larger firms can leverage their plethoric managerial resources—such as financial capital, technology, expertise, and experience—to understand and apply new technology solutions. They also have the necessary organizational processes (i.e., staff training and scheduling, appointment and service procedure) to effectively deploy and integrate telemedicine into their workflow during the pandemic. Such high absorptive capacity implies that large clinics are more capable of leveraging telemedicine to regain resources and sustain business during the pandemic (Cohen and Levinthal, 1990; Sullivan-Taylor and Branicki, 2011). Small clinics, due to their limited resources, may struggle to deploy and scale up telemedicine solutions when faced with disruptive events.
On the other hand, it is also possible that smaller clinics benefit more from telemedicine amid the pandemic than larger clinics because they are more agile and adaptable (Martinez-de-Albeniz et al., 2025; Sukwadi et al., 2013). Smaller clinics have fewer hierarchical levels and fewer staff to manage, which can result in higher absorptive capacity (Jansen et al., 2005). Communication and decision-making can be more efficient when it comes to new technology adoption and use (Knott and Vieregger, 2020). Therefore, smaller clinics may find it easier to make necessary adjustments (i.e., structural, technical, and funding changes) in response to sudden disruptions (Gilbert, 2005; Parker and Ameen, 2018). For instance, they can swiftly reconfigure physicians and supporting staff for online and offline arrangements. Furthermore, adapting an IT system to include telemedicine services can be less cumbersome when the existing infrastructure is less complex. This high absorptive capacity allows smaller clinics to effectively shift to telemedicine to reach consumers and to regain business amid the pandemic, hence alleviating their resource dependence (Zahoor et al., 2022). Larger clinics, though, may have faced more challenges in implementing telemedicine and adapting their workflows in response to the pandemic shock due to their complex organizational structure and layers. They may experience augmented resistance and inertia from employees accustomed to traditional methods of care delivery (Wiersema and Bantel, 1992). Hence, larger clinics may be less likely to derive resilience via telemedicine.
Together, we propose two competing hypotheses, as follows:
H3a: The mitigating effect of telemedicine adoption is stronger for larger clinics.
H3b: The mitigating effect of telemedicine adoption is stronger for smaller clinics.
Moderating Effect of Product Risk Level
We further predict that the extent to which clinics can utilize telemedicine to gain resilience depends on the nature of their products. This is because different clinics might have varying levels of absorptive capacity depending on the level of fit between telemedicine and their focused products (Cohen and Levinthal, 1990). A high level of fit between a technology and a product implies that the technology aligns well with the firm's existing practices and capabilities in service delivery. This alignment makes the potential value of the technology more apparent, facilitating firms’ assimilation of the technology into the current workflow. Conversely, if the technology does not align well with the firm's existing offerings, it might be more challenging for the firm to capitalize on its advantages, potentially leading to high resistance and costs in its application.
In the current context, we focus on the level of risk associated with the medical aesthetics products provided by clinics, which can be broadly categorized based on whether they require surgery. We expect that, during the pandemic, the mitigating effect of telemedicine has been more effective for clinics offering lower-risk or nonsurgical products (e.g., Botox injections). Specifically, because lower-risk products involve less uncertainty (Yuan et al., 2024), consumers’ purchase decisions can be largely informed via telemedicine. This means that for clinics focusing on lower-risk products, the fit between telemedicine and their services is generally higher, allowing them to leverage their existing knowledge and experience in consumer interactions when learning and applying telemedicine (Cohen and Levinthal, 1990). This strong absorptive capacity enables these clinics to effectively leverage telemedicine to cultivate consumer interests and maintain revenue streams during the pandemic.
Products involving higher risk or surgical procedures (e.g., breast augmentation), however, are usually more complex, have more attributes and tradeoffs, and involve higher uncertainty. They necessitate increased information search before purchase decision-making (Yuan et al., 2024). For these products, telemedicine can be used for initial consultations, but it may not be sufficient for preoperative care or decision-making. Consumers may still have to rely on offline resources such as personal interaction and medical equipment for checkups. This implies a lower fit between higher-risk products and telemedicine, and hence, lower absorptive capacities for these clinics in deploying telemedicine to regain resources. Therefore, during the pandemic, clinics focusing on higher-risk products are more likely to depend on offline service delivery and are less likely to generate business through telemedicine. Therefore, we propose,
H4: The mitigating effect of telemedicine adoption is stronger for clinics focusing on lower-risk products.
Setting, Data, and Models
Empirical Setting
We collaborated with a leading O2O platform of medical aesthetics services in China, which had 3.67 million monthly active users and 2138 registered medical aesthetics clinics at the time this study was conducted. Telemedicine was introduced on this platform in 2019, and clinics could choose whether to adopt it. For the clinics that adopted telemedicine, consumers could consult doctors of the clinics on their specific problems through one-on-one video chats. Telemedicine was offered to all consumers for free. It did not direct consumers to any product page, and consumers could search for more information on the relevant products on the platform. Overall, while telemedicine is not a necessary step prior to purchases on this platform, it is an important tool that enables clinics or doctors to communicate with their potential consumers directly.
General Trends of Consumer Activities Before and During the Pandemic
Because consumers’ activities on the platform cover the full phase of their shopping process, before delving into clinic performance, we first sought to form a general understanding of how consumer behaviors had changed since the advent of the pandemic. The purchase funnel model suggests that consumers move through different stages during their purchase process: awareness, consideration, and purchase (e.g., Todri et al., 2020). Accordingly, we considered two broad sets of consumer activities. One pertained to general browsing behaviors (i.e., an early stage of the funnel), which included browsing the main page which listed all key resources (e.g., clinics, doctors, products, posts) on the platform (
We retrieved consumer activity data and aggregated them each day during a selected period: around two months before and after the start of the pandemic. In particular, the pandemic began on 21 January 2020, when the National Health Commission of China first reported the number of confirmed cases across China. 1 The end point of the first round of the pandemic was set to 8 April 2020, based on the official permission allowing outbound traffic from Wuhan, 2 which marked a temporal end of the pandemic in China. Our data period thus covered between 1 November 2019 and 7 April 2020. 3
Figure 2 shows the trends of consumers’ general browsing behaviors (a, b, and c) as well as specific product evaluation behaviors (d, e, and f) before and after the pandemic (also see E-companion Part A for detailed analysis). We found that, after the outbreak of the pandemic, consumers’ general browsing behaviors on the platform were not reduced and even grew quickly when the pandemic became less severe. However, following the start of the pandemic, consumers’ specific product evaluation behaviors declined dramatically, with product page views and cart-adding behaviors gradually returning to pre-pandemic levels over time, while the number of orders remained stagnant. This implies that, when facing the pandemic shock, the platform could still help clinics acquire potential consumers. This was possibly due to consumers spending more time online as offline activities were restricted. However, moving these consumers to the later stage and persuading them to make purchases was difficult. Indeed, the sharply reduced consumer interests in specific products and purchases due to the pandemic became the key challenge for clinics to survive. Next, we focused on testing our hypotheses.
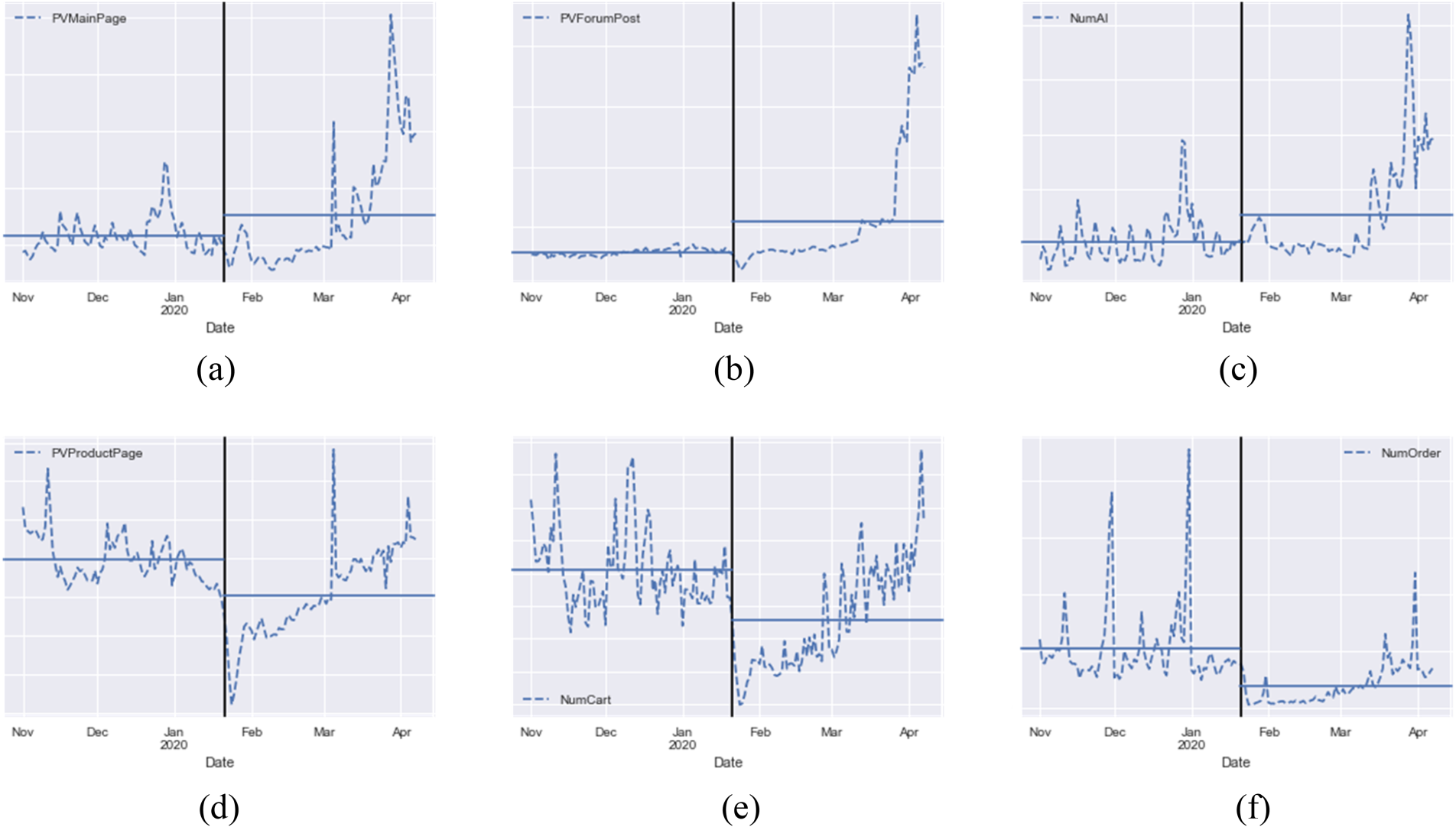
Consumer activities at early (a, b, c) and later stages (d, e, f) of the purchase funnel. 11 (a) Page views of the main page. (b) Page views of forum posts. (c) Number of AI system uses. (d) Page views of product pages. (e) Number of add-to-cart behaviors. (f) Number of orders.
To examine the impact of the pandemic on clinic performance and how the adoption of telemedicine helped clinics build digital resilience, we constructed a clinic-day panel dataset. Specifically, we chose clinics located across ten major cities in China 4 and selected a time window containing a pre-pandemic period and an in-pandemic period, both around two months, for each city. We then aggregated data on each day at the clinic level. For different cities, the outbreak date and the end date of COVID-19 were slightly different (see Table 1, the in-pandemic period was longest in Wuhan and shortest in Hangzhou). We determined the outbreak date of the pandemic based on the official disclosure of the first confirmed case in each city and the end date based on the local government's official announcement of its having reduced the local pandemic risk level to “low”. 5 For example, for Beijing, our pre-pandemic period was from 1 November 2019 to 20 January 2020, and the in-pandemic period was from 21 January 2020 to 22 March 2020. The clinic-day panel data included 174,470 observations on 1265 clinics over the pre- and in-pandemic periods. 6
Starting and end dates of the in-pandemic period by city.
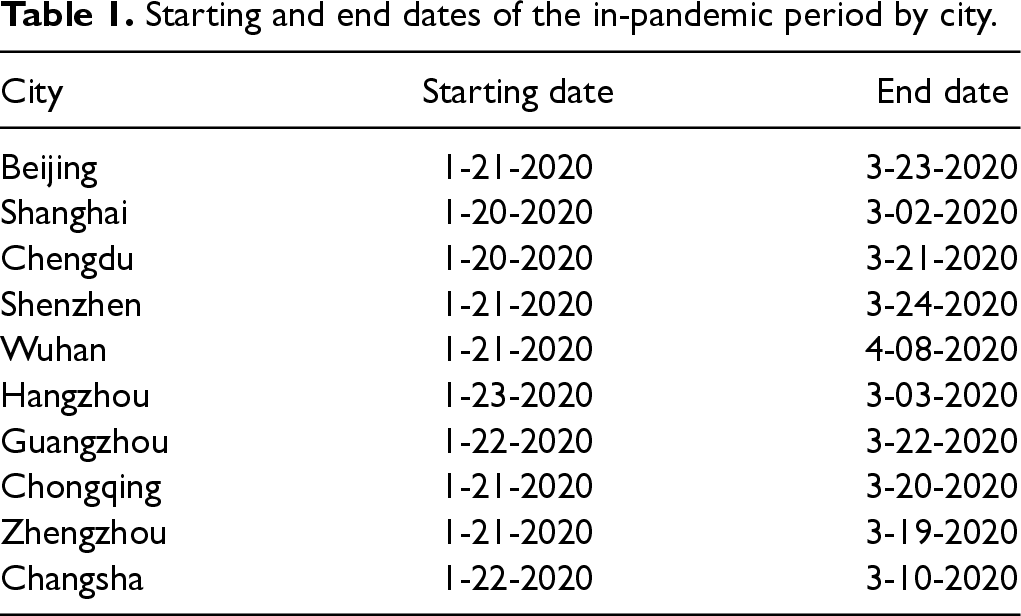
Starting and end dates of the in-pandemic period by city.
We first provided model-free evidence for the general impact of COVID-19 on clinic performance, as measured by the daily number of orders received by these clinics on the platform. As illustrated in Figure 3 7 , following the outbreak of the pandemic, the medical aesthetics clinics experienced a significant decrease in the daily count of orders (i.e., from 3308 daily orders, on average, before the outbreak to 1,219, on average, after the pandemic arose). Figure 4 shows the daily count of telemedicine services these clinics provided. As exhibited, the number of telemedicine services increased after the outbreak of COVID-19 (i.e., from 255 telemedicine services daily, on average, before the outbreak to 619, on average, after the pandemic began).
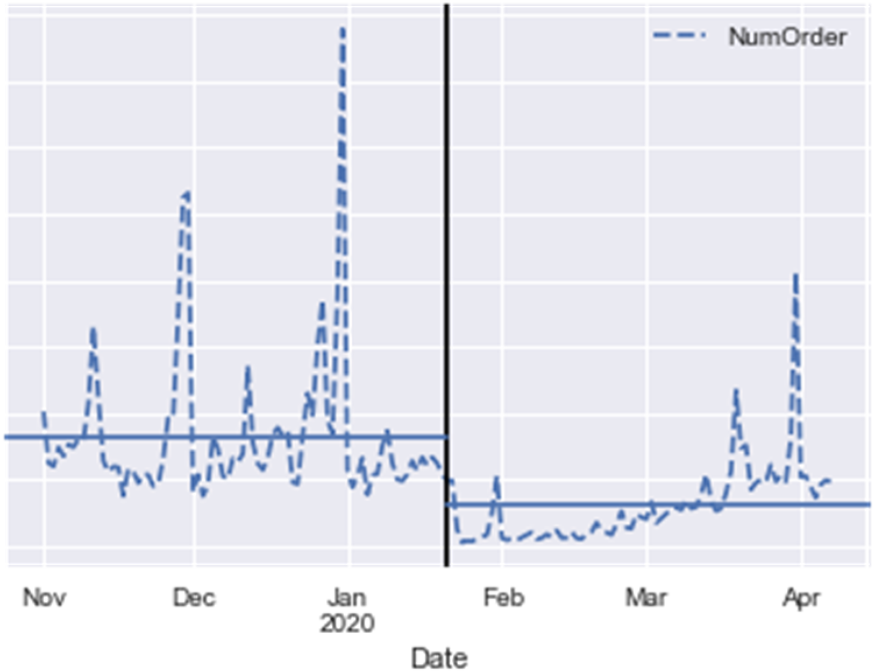
Daily count of orders.
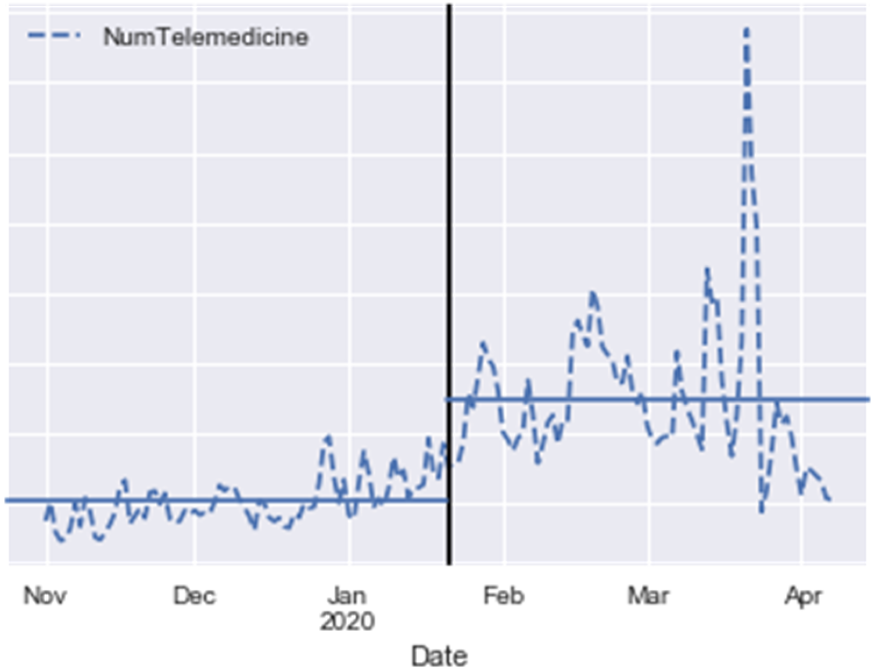
Daily count of telemedicine.
To estimate the impact of the pandemic on clinic performance (H1) and the mitigating role of telemedicine (H2), we adopted a Poisson model with a clinic-level fixed effect, as specified in Equations (1) and (2), respectively. We did so because the dependent variable (i.e., the number of orders) was in the form of count data. The results of the Hausman test supported our choice of the fixed-effects model instead of the random-effects model.


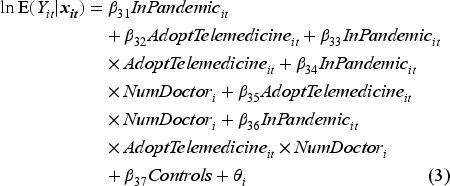
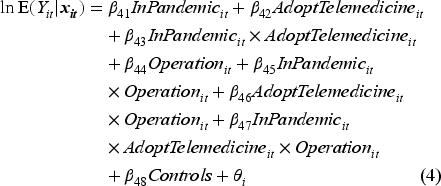
The models estimating the moderating effects of clinic size (H3) and product risk level (H4) are specified in Equations (3) and (4), respectively:
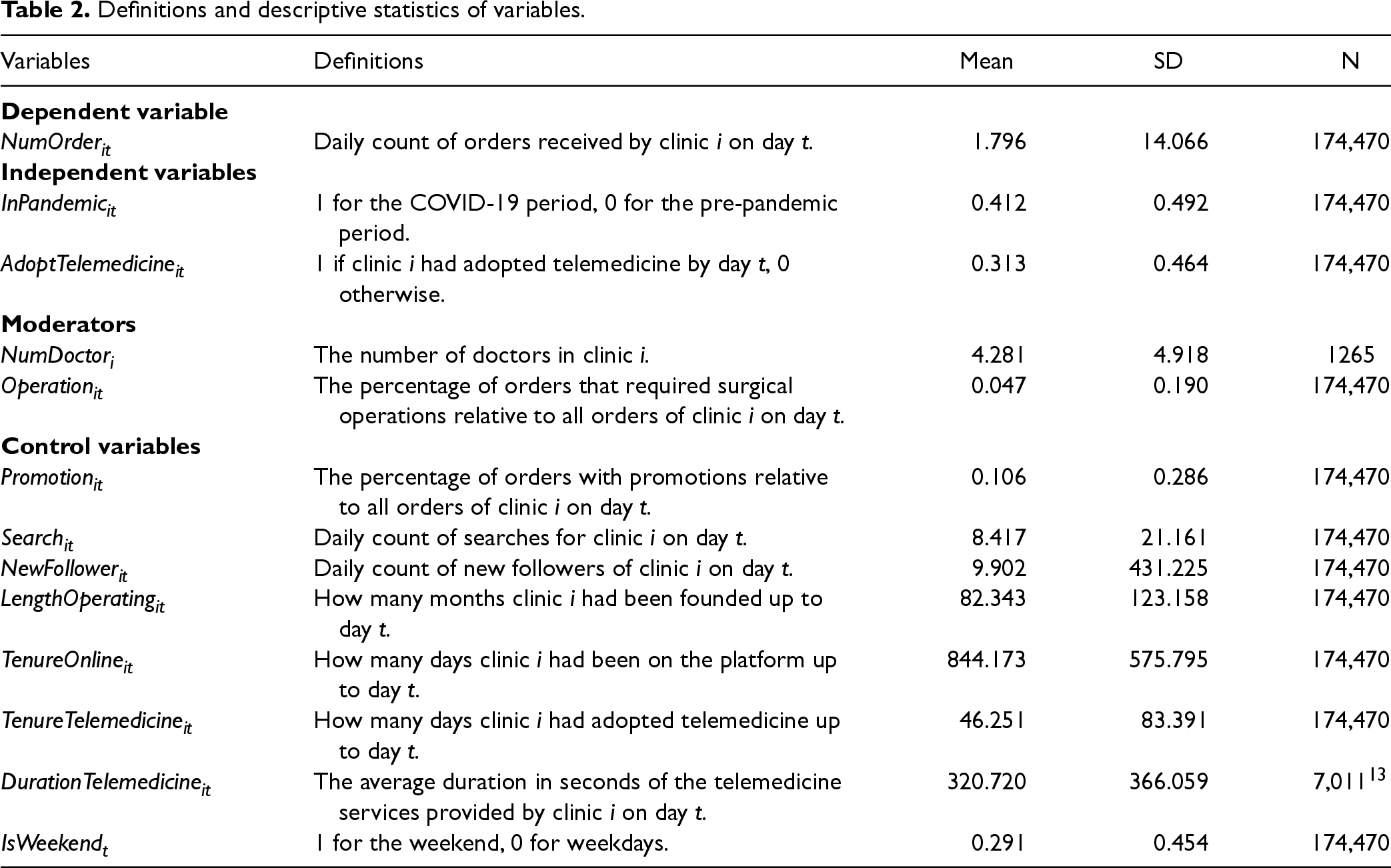
The definitions and descriptive statistics of the dependent variable, independent variables, moderators, and control variables are shown in Table 2. In our regressions, we standardized the moderators and all continuous control variables.
Definitions and descriptive statistics of variables.
The correlation coefficients and variance inflation factors are shown in E-companion Table EC-B1. All the variance inflation factors were smaller than 5, indicating that multicollinearity was not a major concern in our study.
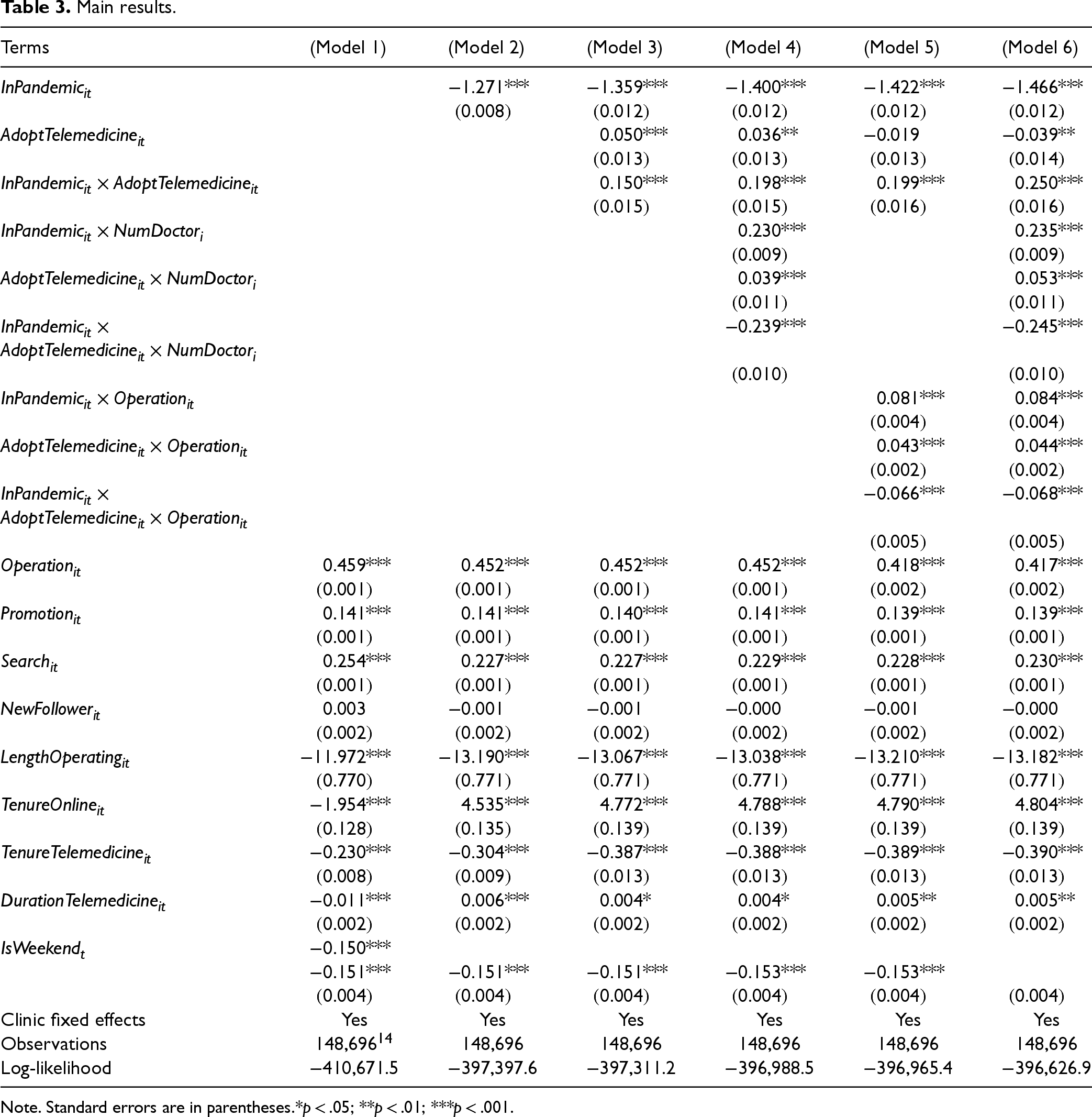
We adopted the step-wise approach, first including control variables (Model 1 in Table 3) and then adding independent variables, moderators, and their interaction terms to the models: Model 2 for testing H1 (i.e., the negative impact of the pandemic), Model 3 for testing H2 (i.e., the mitigating effect of telemedicine), Model 4 for testing H3 (i.e., the moderating effect of clinic size), Model 5 for testing H4 (i.e., the moderating effect of product risk level), and Model 6 including all terms.
Main results.
Main results.
As shown in Model 2, the coefficient of
As depicted in Model 3,
The results of Model 4 revealed that the coefficient of the three-way interaction term (i.e.,
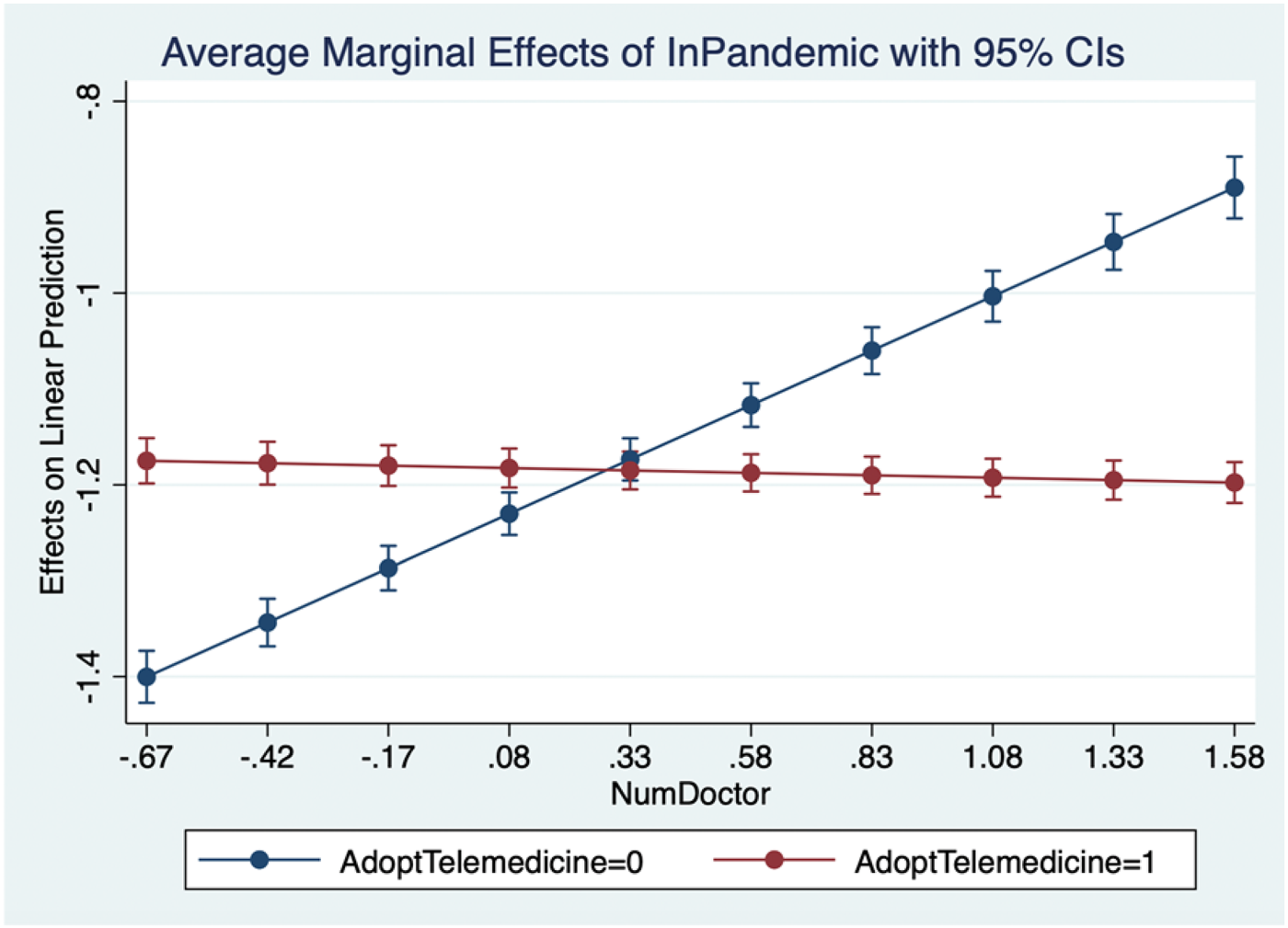
Average marginal effects of the pandemic for different clinic sizes. 12
The results of Model 5 revealed that the coefficient of the three-way interaction term (i.e.,
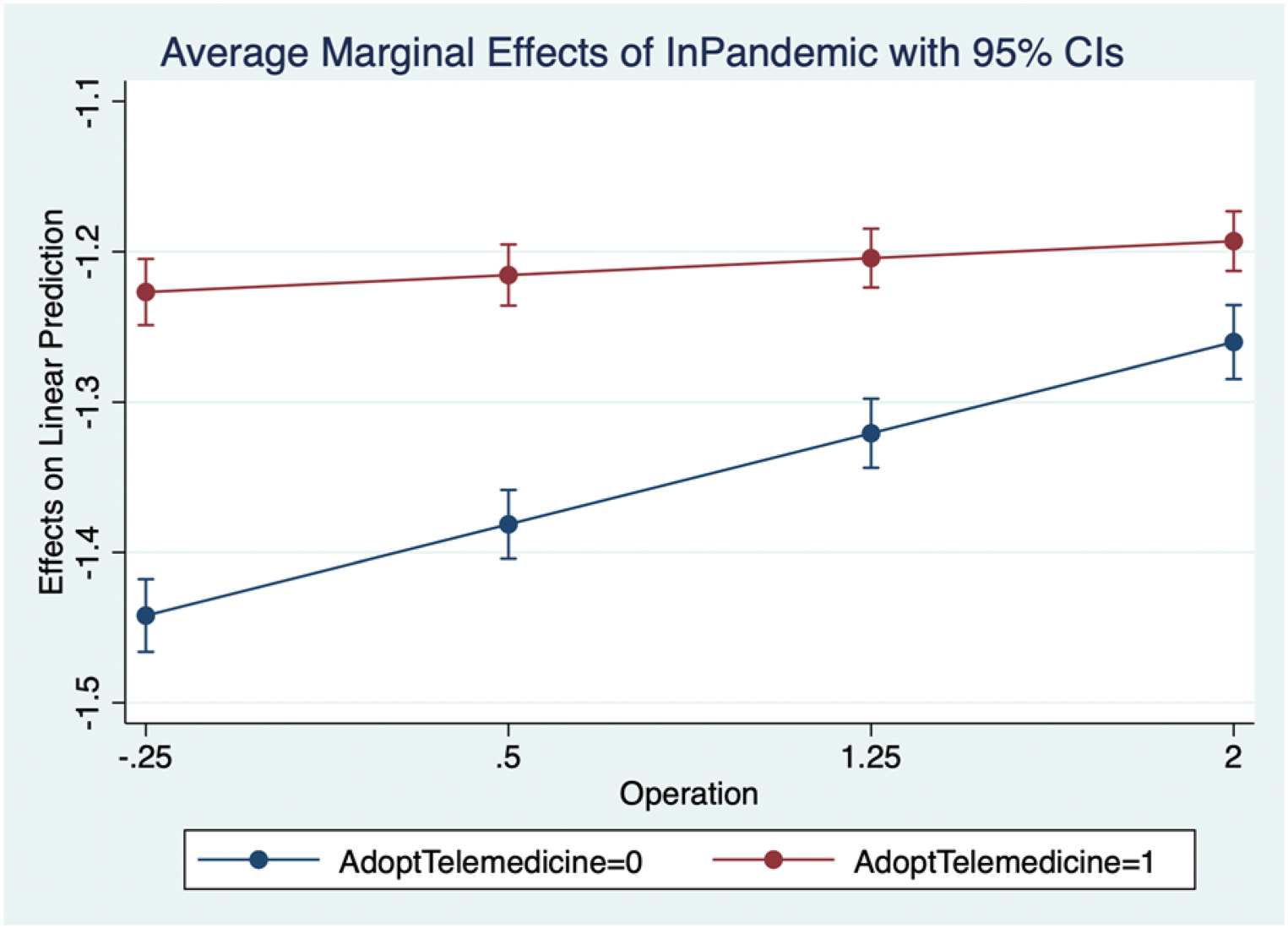
Average marginal effects of the pandemic for different product risk levels.
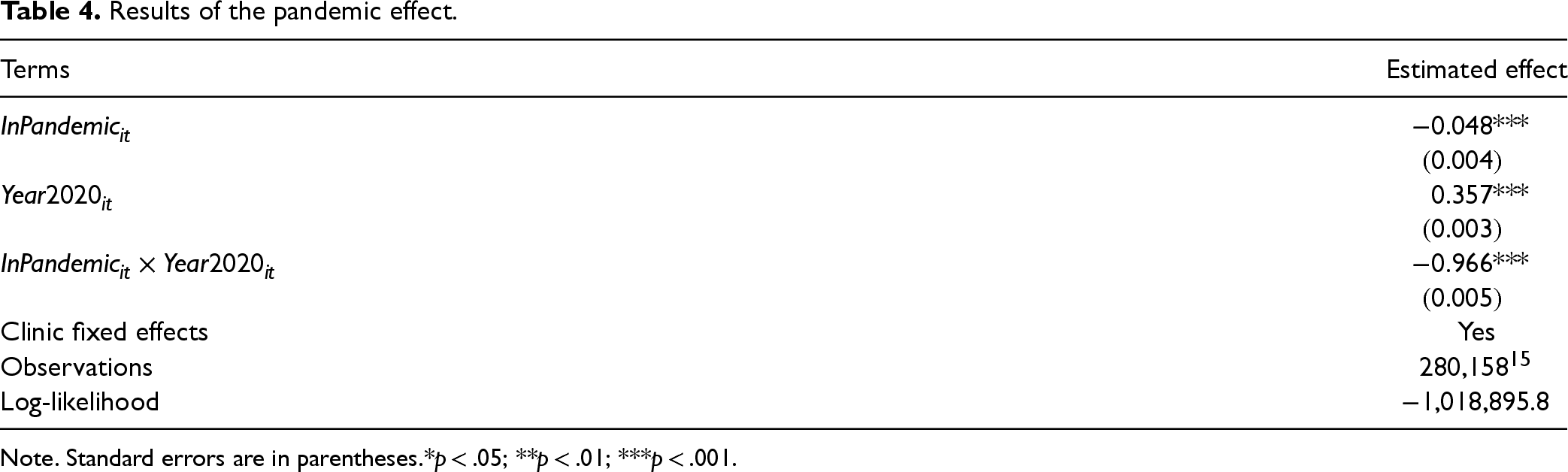
In China, COVID-19 first erupted a few days before the Chinese Lunar New Year—the most important festival in China—which occurred on 25 January 2020. The seasonality this festival causes may have complicated the estimation of the negative effect of the pandemic. This is because medical aesthetics consumption may decline at this time period, as consumers travel to their hometowns (often from major to smaller cities) for the Lunar New Year. To address this concern, we collected data from the previous year and matched them with our main dataset based on the Chinese lunar calendar (Han et al., 2022). The main dataset contained the time period from 1 November 2019 to 7 April 2020; the dataset of the previous year encompassed the period between 12 November 2018 and 19 April 2019. We estimated the following model:

Results of the pandemic effect.
Comparison between two groups after matching on
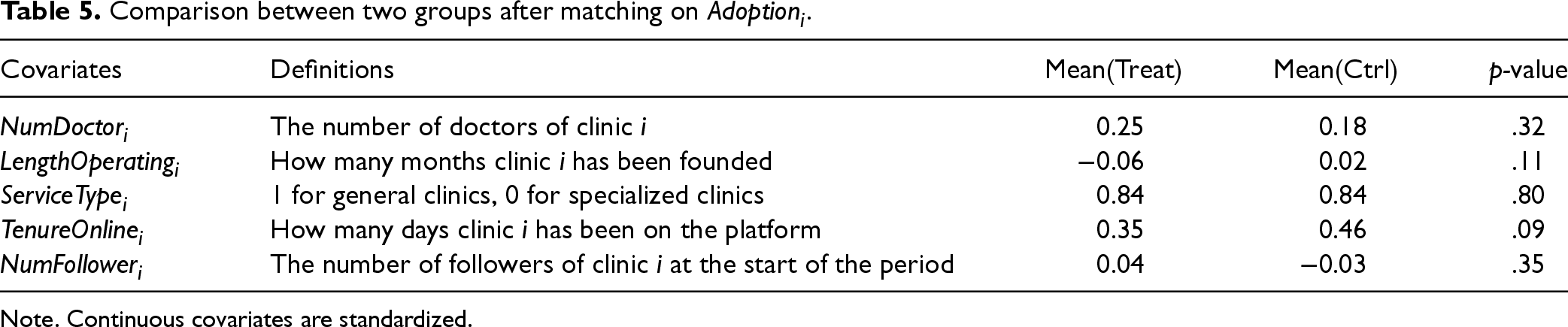
As our analysis focused on how telemedicine mitigated the negative impact of the pandemic, a concern was that clinics’ telemedicine adoption might not be random; if not, this limitation could result in endogeneity of the independent variable
We conducted PSM at the clinic level and used
We conducted the main models on the clinic-day panel using data from the matched clinics of
Results on the panel of matched clinics on
.
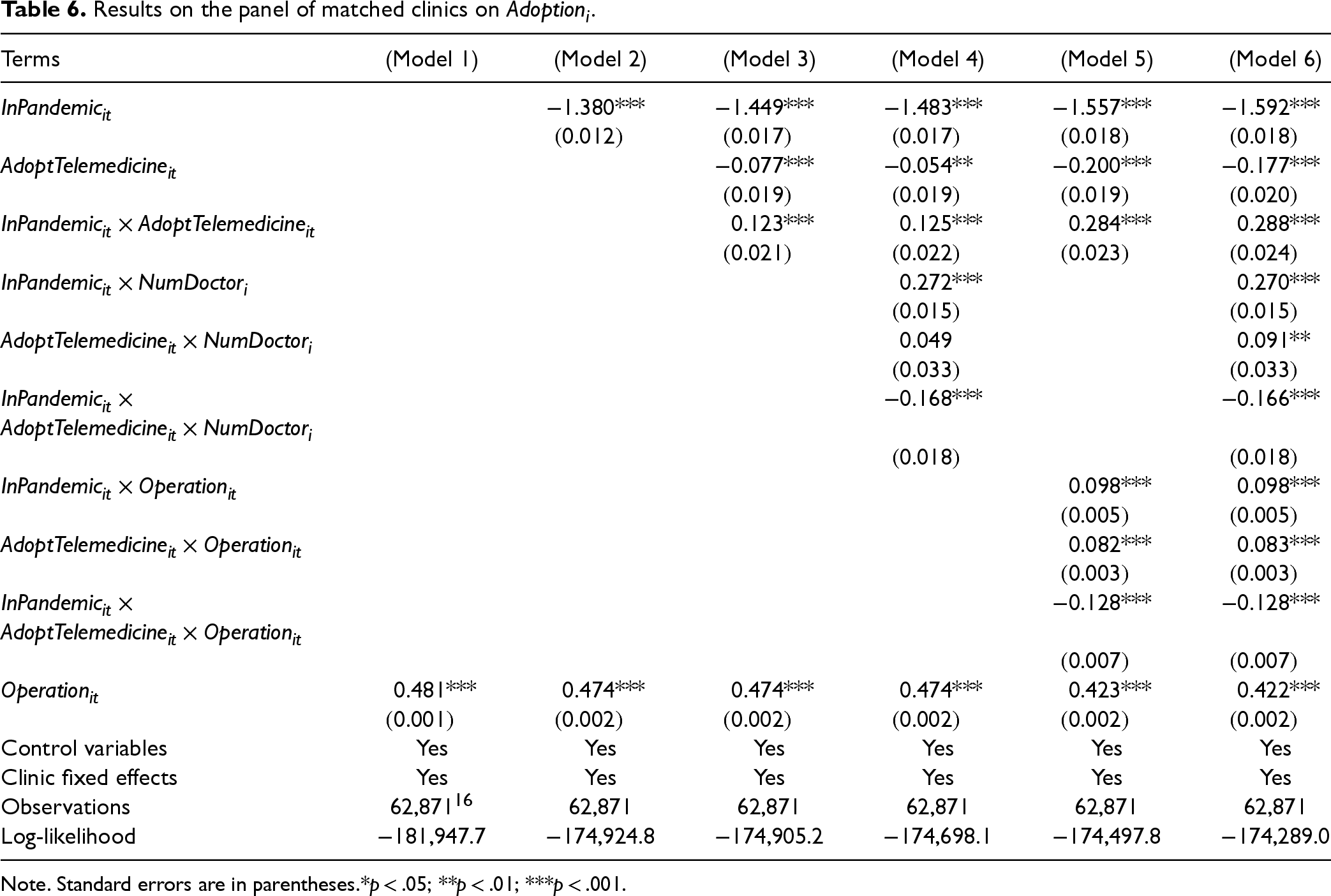
Results on the panel of matched clinics on
Purchase Amount as an Alternative Dependent Variable
In our main models, we used the number of orders as the dependent variable. However, aside from that, we can also gauge the effects with purchase amount (i.e., the total monetary value of sale orders a clinic made on day t) as an alternative measurement of clinic performance. The results were consistent with our main findings (see Table EC-D1 of E-companion).
Alternative Pandemic Cut-off Point
We chose 25 January 2020 as an alternative cut-off point for the pandemic. On 25 January 2020, the government launched a series of policies for pandemic prevention, including restrictions on transportation. 9 These restrictions affected logistics and the flow of people, thus heavily reducing the resources that clinics could acquire. The results using this alternative cut-off point were consistent with our main findings (see Table EC-D2 of E-companion).
Simultaneity Bias
To address potential simultaneity bias, we replaced the control variables
Time Fixed Effects
To control for unobserved time-varying factors, we included time fixed effects in the main models as a robustness check. Since day-level time indicators were highly correlated with our independent variable (
Additional Analyses
Our primary findings suggested that telemedicine mitigated the negative impact of COVID-19 on clinic performance in terms of order volume. Closely related to consumers’ order-taking behavior are their indicated interests in specific products, such as adding products to their favorite lists or shopping carts. Forming product interests is often a crucial precursor to purchases and plays a vital role in the long-term recovery of businesses, especially those offering non-essential goods. Hence, we conducted additional analyses on consumers’ specific product interests to explore how telemedicine influences the interest-forming process and to better understand its role in mitigating the pandemic's impact. Specifically, we analyzed the mitigating effect of telemedicine on consumers’ product interests in terms of add-to-favorite (
While our main models focus on the effect of telemedicine adoption on user behaviors, the adoption of telemedicine by clinics directly influences the actual provision of telemedicine services, which, in turn, affects users’ product interests and purchase behaviors. Accordingly, to elucidate the mechanisms underlying the effect of telemedicine adoption on consumers’ product interests, we analyzed this relationship in two stages: first, adoption increases the provision of telemedicine services, and second, these services foster consumer interests. Econometrically, we thus treated telemedicine adoption (
Effect of Telemedicine on Cultivating Consumer Interests for Specific Products
We first ran a fixed-effects model for
In addition, the moderating effect (i.e., the three-way interaction term) of clinic size was negative on
Effect of Telemedicine for Different Consumer Groups
Another crucial factor in medical aesthetics consumption is consumer type. Consumers who are less familiar with medical aesthetics services often require a significant amount of information for educational purposes. Due to the high uncertainty and identity relevance of such services, they need to be well-informed before they can develop product interests and make purchase decisions. For more experienced consumers, it can be more effective to target their specific needs and doubts and pique their interests in specific services via telemedicine. Hence, to further understand the effectiveness of telemedicine, we analyzed how its mitigating effects on fostering consumer interests varied between different consumer groups.
We categorized consumers into two groups based on their experience level on the platform: more experienced and less experienced consumers. Specifically, for all consumers who had added products to favorite lists or shopping carts on day t, we defined more experienced consumers as those who had been registered users on the platform for more than seven days, while less experienced consumers as those who had registered on the platform within the past seven days. We then retrieved the count of products added to favorite lists and shopping carts by both groups for each clinic on each day.
We conducted the aforementioned two-stage regressions separately on the number of add-to-favorite and add-to-cart made by more and less experienced consumers. The results held true for more experienced consumers but not the less experienced ones (see Part F of E-companion). This suggests that telemedicine mainly cultivates product interest among experienced consumers. Experienced consumers have spent more time browsing and searching for products and clinics on the platform. Since these consumers have some existing knowledge about the services, communicating with them via telemedicine is more likely to clear their doubts and generate interests in specific products (e.g., add-to-favorites/-carts).
Discussion
Using RDT as our overarching theory and employing a rich and proprietary dataset from a leading O2O platform in China for medical aesthetics services (i.e., a typical non-essential business), we documented the severe negative impact of the pandemic on clinic performance in terms of the number of orders. We further showed that the adoption of telemedicine effectively reduced clinics’ resource dependence during the pandemic, helping clinics regain critical resources and alleviating the negative effect caused by the pandemic. Furthermore, different clinics varied in their absorptive capacity in leveraging telemedicine to gain business during the pandemic. Specifically, smaller clinics benefited more from telemedicine adoption amid the pandemic as they may have exhibited higher flexibility and efficiency in making organizational changes when facing the pandemic. Also, the mitigating effect of telemedicine services was stronger for clinics focusing more on lower-risk products, as consumption decisions of these products were better supported by telemedicine (i.e., a higher fit).
With additional analyses, we also found that telemedicine contributed to cultivating consumer interests in specific products (i.e., adding to their favorites lists and shopping carts) amid the pandemic. While this effect was stronger for smaller clinics, it held true for clinics providing both high- and low-risk products. Further, this mitigating effect of telemedicine seemed to have been primarily derived from assisting experienced consumers’ interest development, suggesting that telemedicine took effect mainly by helping clinics maintain relationship with existing consumers rather than reaching new consumers.
Theoretical Contributions
This study makes several contributions to the literature. First, it extends the growing work in OM literature by investigating how digital service delivery can help build resilience for non-essential businesses during crises. While existing OM research has largely focused on essential businesses’ operational responses to COVID-19 (Blackmon et al., 2021; Delasay et al., 2022; Liu et al., 2023; Shen and Sun, 2023), non-essential businesses faced more severe adverse effects. Our study reveals how telemedicine, as an innovative operational capability, can mitigate these effects and identifies the conditions under which such digital transformation is most effective.
Second, our study also advances knowledge on crisis management and organizational resilience broadly, investigating a novel type of crisis and resilience. Compared with other economic or financial crises, the pandemic arrived more unexpectedly and quickly and has had critical consequences on economic and social activities, as well as on individuals’ health (McFarland et al., 2020). Our undertaking enriches the literature on organizational resilience, affirming the critical role telemedicine plays in mitigating the disruption of the pandemic crisis on firm performance.
Third, this study extends the literature on OM and IS by examining how telemedicine adoption creates operational value during crisis situations. While prior OM research has focused on telemedicine's outcomes under normal conditions (e.g., Bavafa et al., 2018; Rajan et al., 2019; Sun et al., 2020; Wang et al., 2020a), we demonstrate its economic potential as a resilience-building operational capability during sudden disruptions. By investigating telemedicine in the medical aesthetics industry, a typical non-essential sector, we reveal how digital service delivery contributes to consumer interest cultivation and converting interested consumers to purchasers during crises, expanding our understanding of operational adaptability in healthcare settings.
Fourth, our work extends the scope of RDT, applying this theory to a new situation of an uncertain environment—the pandemic—and identifying a novel form of coping strategy (i.e., provision of telemedicine services) to manage resource dependence. Prior research has mainly focused on resource dependence in regular situations and the effectiveness of inter-organizational arrangements, such as joint ventures, mergers and acquisitions, and alliances (Drees and Heugens, 2013), as coping strategies to reduce such dependencies. We transcend the prior work by examining the effectiveness of another form of coping strategy—the adoption of new technology—in reducing resource dependence amid the pandemic crisis.
Managerial Implications
This research benefits policymakers and managers who are seeking effective crisis management tactics in response to COVID-19—or other sudden crises.
By quantifying the economic impact of telemedicine amid the pandemic crisis, we affirm the critical role that digital innovation plays in achieving resilience and contributing to firm survival. Our results suggest that brick-and-mortar firms should proactively employ digital tools to cultivate consumer interests and to gain business when offline operations are down or suspended. Because many crises happen unexpectedly but have enormous disruptions, firms are advised to prepare through proactive design and utilization of digital platforms and tools to maintain smooth and close communications with their consumers.
Our findings also suggest that, when facing a crisis, different firms might benefit differently from digital technologies. Companies, therefore, should take advantage of digital innovations strategically. Specifically, small firms could undertake a more active initiative to design and utilize digital platforms and technologies to acquire consumers and provide services, while larger firms should focus on becoming more agile in adapting to such transformation. Furthermore, depending on the product nature and its fit level with digital technologies, firms focusing on less resource-dependent products (i.e., lower-risk medical aesthetics products) should adopt a more proactive approach when employing digital tools. However, firms centering on high resource-dependent products may also benefit from digital innovation in terms of enhancing consumer interests in specific products.
We believe that our results can be generalized to other non-essential business sectors, for instance, fitness and personal care. Following the outbreak of COVID-19, many offline gyms have turned to online fitness platforms on which trainers offer video-based courses to reach consumers and gain business. RDT, together with our findings, suggests that gyms may be able to mitigate the negative effect of the pandemic through providing virtual fitness services (e.g., video-based training courses). Furthermore, it is plausible that smaller (vs. larger) gyms and those specializing in “light” (vs. “intense”) workouts might enjoy better resilience with the adoption of virtual fitness platforms.
Limitations and Future Research
Certain study limitations exist and are suggestive of further research opportunities. First, this investigation only examined the impact of COVID-19 on one type of non-essential business, medical aesthetics, and investigated the digital resilience effect of one digital tool, telemedicine. Future research should expand the scope to other non-essential businesses and digital technologies to support further the generalizability of the digital resilience effect. Second, our data only captured the initial outbreak of the pandemic in early 2020. Because the pandemic has gone through several waves of outbreaks across countries, further research is needed to investigate the effects of the pandemic and digital resilience across different waves of the pandemic. Third, while our analysis captures valuable data on telemedicine adoption, there are additional factors that could enhance our understanding of how telemedicine enables digital resilience, such as how clinics allocate their resources for online and offline operations, the specific categories and content of telemedicine consultations, and consumer characteristics (e.g., age and gender). Unfortunately, due to data limitations, we were unable to incorporate these details into our analysis, hence providing limited insights into how to implement telemedicine services amid the crisis. Therefore, future research should conduct a more in-depth investigation into how firms can strategically allocate resources for new technology solutions to gain digital resilience.
Supplemental Material
sj-docx-1-pao-10.1177_10591478251325750 - Supplemental material for Digital Resilience to COVID-19: Evidence From the Medical Aesthetics Industry
Supplemental material, sj-docx-1-pao-10.1177_10591478251325750 for Digital Resilience to COVID-19: Evidence From the Medical Aesthetics Industry by Lili Wenli Zou, Mengxin Li, Cheng Yi and Harry Jiannan Wang in Production and Operations Management
Footnotes
Acknowledgments
We thank the department editor, senior editor, and the three anonymous reviewers for their constructive feedback, which substantially improved this paper. We also gratefully acknowledge the corporate support provided for this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the National Natural Science Foundation of China [Grants 72425003, and 72421001].
Notes
How to cite this article
Zou LW, Li M, Yi C and Wang HJ (2025) Digital Resilience to COVID-19: Evidence From the Medical Aesthetics Industry. Production and Operations Management 34(11): 3438–3456.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.