
Abstract
The impact of doctor–patient interactions on patients’ service evaluations in online medical consultations (OMCs) has received considerable attention. However, prior research has mainly focused on the individual-level and statistical features of these interactions, with limited exploration of dyad-level dynamics in doctor–patient bidirectional communication. To address this gap, this study examines both individual-level and dyad-level features of online doctor–patient interactions to understand their effects on patients’ service evaluations. We characterize doctors’ individual-level communication behaviors using the quantity and informativeness of doctors’ information acquisition and provision, and capture dyad-level features by quantifying communication alignment in doctor–patient dialogues using spectral analysis. We utilize patient gratitude as an indicator of patients’ service evaluation. Drawing on expectancy violations theory, we develop a theoretical model to examine the direct and interaction effects of doctors’ communication behaviors and doctor–patient communication alignment on patient gratitude in OMCs. The model is empirically tested using a large dataset collected from a leading OMC platform in China. The analysis reveals three key findings. First, the informativeness of doctors’ information acquisition negatively affects patient gratitude, while neither the informativeness nor the quantity of information provision has a significant effect. Second, communication alignment positively influences patient gratitude. Third, communication alignment positively moderates the effects of the informativeness of both information acquisition and provision on patient gratitude. This study contributes to the literature on patients’ service evaluations, doctor–patient interactions, and communication alignment in online healthcare, and offers practical guidelines for enhancing the overall quality of online healthcare services.
Keywords
Introduction
Online medical consultation (OMC) is a widely used function of online health platforms. OMC allows users, including patients and their family members, to seek information on the treatment, prevention, or management of illnesses through formal one-on-one communications with doctors (Y. Liu et al., 2020; Tan et al., 2023). Consistent with previous studies, we use the term “patients” to refer to all users seeking medical information in OMCs (Meng et al., 2021; Wu et al., 2021). OMC services have emerged as important solutions for satisfying the growing medical needs of the Chinese population under the constraints of limited medical resources (Wang et al., 2020; Zhao et al., 2022). By October 2022, over 25.9 million OMC services had been provided nationwide (Cyberspace Administration of China, 2023). Currently, the number of OMC services exceeds 100 million annually across the country (China Internet Network Information Center, 2025).
The widespread adoption of OMCs has extended traditional face-to-face doctor–patient interactions to computer-mediated online doctor–patient communications (Guo et al., 2016; Yan et al., 2020). The features of computer-mediated communication (CMC) bring both benefits and challenges to online doctor–patient interactions. On the one hand, the connectivity of CMC breaks the time and space restrictions, providing patients with convenient access to medical information online (Rains et al., 2015; Wright and Bell, 2003). On the other hand, due to the absence of visual and verbal cues, doctor–patient interactions in CMC require greater cognitive effort and have lower interaction intimacy compared to face-to-face communications (Lewandowski et al., 2011). Additionally, the asynchronism of CMC makes it difficult to guarantee doctors’ timely responses and may lead to misunderstandings (Katz et al., 2003; Yan et al., 2020). Such challenges in online healthcare interactions cause communication issues between doctors and patients, resulting in negative service evaluations from patients and poor online doctor–patient relationships (Shah et al., 2021). To enhance the overall quality of online healthcare services, it is important to address these challenges and optimize doctor–patient interactions in the context of OMC.
In offline medical visits, doctors typically control consultation and diagnosis processes, and patients are generally passive recipients of medical information (Yellowlees et al., 2015). In contrast, effective online doctor–patient interactions require active participation from both doctors and patients, and doctors’ and patients’ communications are more interdependent (Guo et al., 2016; Liang and Scammon, 2011; Mirzaei and Esmaeilzadeh, 2021). Considering the interactive nature of OMC, this study aims to investigate both individual-level and dyad-level features of online doctor–patient interactions and assess their impact on patients’ service evaluations. Specifically, the individual-level features we consider in this study reflect doctors’ individual communication behaviors, and the dyad-level features capture doctors’ and patients’ interactive communication behaviors.
At the individual level, doctors’ communication behaviors during medical consultation serve two purposes: information acquisition and information provision (Sandvik et al., 2002; Tan and Yan, 2020). Doctors’ information acquisition refers to doctors’ information collection regarding patients’ health conditions, symptoms, lifestyle habits, etc., by asking questions to support diagnosis (Roter and Larson, 2002; Yan et al., 2020). Doctor's information provision includes delivering information and instructions related to the health condition, treatment plan, and lifestyle (Chen et al., 2020).
Previous studies have mainly investigated the role of doctors’ overall communication behaviors during an entire consultation, such as the total number of responses provided, the word counts of information shared, and the frequency of professional words used (Chen et al., 2020; Yang et al., 2015, 2019), in affecting patients’ evaluations of doctors’ services in OMCs. The recurring theme is that more doctors’ responses lead to better patients’ evaluations. However, this approach oversimplifies the complexity of effective communication. Encouraging doctors to simply increase their responses, ask more questions, or provide more information overlooks several key considerations. First, patients’ needs for information vary depending on medical situations. Sometimes, excessive responses from doctors in straightforward cases can lead to redundancy. Second, doctors’ overall communication behaviors are largely influenced by patients’ behaviors. Third, a lower quantity of interactions may, in some cases, indicate higher-quality communication. Therefore, this study shifts the focus from the overall volume to the specific characteristics of doctors’ information acquisition and information provision (e.g., quantity and informativeness) to better understand how these communication practices influence patients’ evaluations. Gaining this insight will help guide doctors in refining their communication skills, prioritizing the quality of interactions over the mere volume of communications. Therefore, this study aims to comprehensively analyze doctors’ information acquisition and information provision behaviors, and unravel their impacts on patients’ service evaluations in OMCs.
In addition to individual-level behaviors, we argue that the dyadic interactions and communication alignment between doctors and patients are also crucial in shaping patients’ service evaluations (Guo et al., 2016, 2017). Communication alignment, reflecting the extent to which interlocutors coordinate during interaction, has been extensively studied in communication and linguistics research (Fusaroli et al., 2014; Reitter and Moore, 2014). In the absence of face-to-face cues, OMCs conducted via CMC require even greater coordination between doctors and patients. As such, communication alignment plays a vital role in mitigating the negative effects of asynchronism and enhancing patients’ information processing fluency (Volk and Zerfass, 2018). Therefore, this study aims to quantify communication alignment in doctor–patient interactions to clarify the influence of dyad features on patients’ service evaluations in OMCs.
Previous studies indicate that telehealth care coordination through CMC is effective in regulating individuals’ perceptions of health care (Looman et al., 2015). Analogously, we expect that patients’ assessment of doctors’ services is likely affected by the degree of communication coordination in OMCs. Varying levels of communication alignment may lead to differences in how patients perceive and process information provided by doctors. Therefore, this study aims to investigate the interaction effects between doctors’ individual communication behaviors (i.e., information acquisition and information provision) and dyad communication alignment on patients’ service evaluations in OMCs.
Drawing on the literature on healthcare operations management, patients’ service evaluations in online healthcare, doctor–patient interactions, and communication alignment, this study develops a theoretical model to explore the influences of doctors’ individual communication behaviors and communication alignment, as well as their interaction effects, on patients’ service evaluations in OMCs. Consultation records are collected from a leading Chinese online medical consultation platform to empirically test the proposed model. The findings of this study contribute to a comprehensive understanding of doctor–patient interactions, communication alignment, and healthcare operations management in online healthcare and offer valuable guidance to improve the service quality of OMCs.
Literature Review
We review four related streams of prior literature, clarify how this study differs from previous studies, and highlight our unique contributions.
Healthcare Operations Management
Medical service quality has garnered considerable attention in the healthcare operations management literature (Bretthauer and Savin, 2018). Numerous studies have examined factors influencing medical service quality from various perspectives, including technical aspects (Miller, 2003), healthcare supply chain design (Rajapakshe et al., 2020; Sinha and Kohnke, 2009), operational and clinical decision-making processes (Janakiraman et al., 2023; Laker et al., 2018; Senot et al., 2016), and service policies and regulations (Andritsos and Tang, 2018; Mehrotra and Natarajan, 2020). With patients taking an increasingly active role in acquiring medical services, there is a growing emphasis on delivering patient-centered care that considers individual needs and preferences. Consequently, there is a growing focus on the quality of healthcare as perceived by patients (Bretthauer and Savin, 2018; Yan et al., 2019). Among these studies, doctors’ communication behaviors during doctor–patient interactions have been identified as crucial determinants of patients’ evaluations of service quality (Ko et al., 2019; Yan et al., 2022; Yang et al., 2019; Zhao et al., 2022). However, these studies primarily focus on doctors’ individual communications, with limited attention paid to the interactive dynamics of doctor–patient communications. Therefore, this study aims to identify characteristics of both individual-level and dyad-level communication behaviors in doctor–patient interactions, and assess their impact on patients’ evaluations of online medical services. By doing so, this study contributes to the healthcare operations management literature and enhances our understanding of how to improve medical service quality and manage patient-centric healthcare.
Patients’ Service Evaluations in Online Healthcare
Patients’ service evaluations in online healthcare have received considerable attention from academia, as evidenced by works such as Khurana et al. (2019), Liu et al. (2022), and Tan et al. (2023). Patient satisfaction stands out as a frequently employed outcome variable in these studies and is widely recognized as a pivotal criterion for assessing online healthcare services (Chen et al., 2020; Yang et al., 2015). A growing body of recent studies acknowledges patient gratitude as another crucial aspect of service evaluation that requires further exploration within the online healthcare context (Makri and Turner, 2020; Tan et al., 2023). In the online context, patient gratitude is frequently expressed in evaluations of doctors’ services through online reviews, thank-you letters, and digital gifts.
Previous research indicates that patient gratitude represents a more positive evaluation of doctors’ services compared to patient satisfaction (Palmatier et al., 2009; Tan et al., 2023). In terms of preconditions, the threshold for eliciting gratitude is higher than that for satisfaction. Patient satisfaction generally arises when doctors fulfill their basic responsibilities by providing the medical information patients need. In contrast, patient gratitude is aroused when doctors go beyond their obligations to make additional efforts that benefit patients. In terms of outcomes, patient gratitude is associated with a stronger motivation to reward physicians compared to satisfaction (Simon et al., 2015; Tan et al., 2023).
Although patient satisfaction is the most commonly used criterion for evaluating online healthcare services, this study adopts patient gratitude instead for two primary reasons. First, the crucial role of doctor–patient interactions in determining patient satisfaction is well-established (Chen et al., 2020; Yang et al., 2015), while there is a limited understanding of the relationship between doctor–patient interactions and patient gratitude. Second, one of our research focuses, doctor–patient communication alignment, represents a layer of service quality that goes beyond the normal metrics of service quality. Therefore, it is likely a significant determinant of patient gratitude, rather than a factor that only influences patient satisfaction. By focusing on patient gratitude, this study aims to gain deeper insights into the impacts of online doctor–patient interactions on patients’ service evaluations beyond traditional satisfaction metrics.
Doctor–Patient Interactions
Doctor–patient interactions involve a series of dynamic behaviors that facilitate the two-way exchange of information between doctors and patients (Guo et al., 2016; Ong et al., 1995). Specifically, doctors acquire diagnostic information from patients, such as symptoms, medical history, and medication usage. Patients ask questions to obtain medical information from doctors, including diagnosis, causes of illness, and treatment recommendations. Accordingly, doctors’ behaviors related to information acquisition and provision are both considered forms of instrumental communication, which serve as the “cure” part of the consultation (Bensing and Dronkers, 1992). Previous studies have extensively examined the impact of doctor–patient interactions on patients’ service evaluations in online healthcare, highlighting the significant role of doctors’ instrumental communication (often measured by doctors’ interaction frequency, word count of responses, and the number of professional terms used) in determining patients’ evaluations (Chen et al., 2020; Tan and Yan, 2020; Xing et al., 2019; Zhang et al., 2019).
However, the extant literature presents three notable gaps. First, most studies assess the quantity of information exchanged in online doctor–patient interactions using metrics such as word or sentence counts (Tan and Yan, 2020; Yang et al., 2015), while limited attention has been paid to evaluating informativeness based on information entropy. Information entropy reflects informativeness by measuring the probability of specific content occurring within a given context (Xu and Reitter, 2018). Previous research has shown that per-word entropy can quantify lexical information in natural language, and that its distribution can, to some extent, reveal discourse structure (Xu and Reitter, 2016, 2017). Thus, the information entropy of messages in OMCs can serve as an indicator of informativeness in online doctor–patient communication. By combining entropy-based informativeness with traditional quantity measures such as word count, a more comprehensive assessment of online doctor–patient interactions can be achieved.
Second, most existing studies have concentrated on analyzing doctors’ individual behaviors during interactions (Tan et al., 2023; Xing et al., 2019), while largely overlooking the role of patients in the information exchange processes. In OMCs, both doctors and patients are active contributors of information, and their information exchange is inherently interdependent (Guo et al., 2016). Recognizing and assigning importance to their interdependent communication behaviors are essential for constructing a comprehensive theoretical framework for understanding online doctor–patient interactions.
Third, several studies examining the two-way exchange of information tend to model static features of doctor–patient interactions, such as the ratio of word counts or response waiting times between the two parties (Chen et al., 2022; Zhang et al., 2019), which fail to capture the dynamic nature of their dialogues.
To address these gaps, this study uses a richer set of metrics to gain a more comprehensive understanding of dynamic online doctor–patient interactions. At the individual level, word count and information entropy are used to measure quantity and informativeness, respectively. At the dyad level, communication alignment is analyzed to capture the interactive dynamics between doctors and patients. By integrating both levels, this study aims to build a more complete framework for understanding doctor–patient interactions in OMCs.
Communication Alignment in Dialogues
In the research fields of communication, linguistics, and cognitive science, a dialogue is conceptualized as an interaction between two dynamic systems (Fusaroli et al., 2012, 2014; Reitter and Moore, 2014), and its primary goal is to align interlocutors’ situational models. Numerous studies have examined how the alignment of linguistic elements at different representation levels between interlocutors affects the success of task-oriented dialogue and the communication quality (Garrod and Pickering, 2009; Reitter and Moore, 2014).
Previous studies have examined the alignment of information contribution from two interlocutors in a dynamic dialogue (Xu and Reitter, 2017). Per-word entropy is used to quantify the amount of lexical information, and the entropy series of two interlocutors’ dialogue is analyzed using spectral analysis to capture communication alignment. Specifically, two frequency space statistics, power spectrum overlap (PSO) and relative phase (RP), are adopted to model the coupling between two interlocutors’ entropy series. PSO, reflecting the overlap of entropy series in frequency space, has been found to be negatively correlated with task success, as low synchrony—where one interlocutor provides more information and the other less—can promote mutual understanding. Additionally, delays between entropy surges (i.e., peak-to-peak RP) benefit collaborative performance by giving one interlocutor more time to process the information provided by the other, helping to prevent information overload. Thus, low synchrony and high delay indicate coordinated communication, positively predicting task success (Xu and Reitter, 2017).
Communication alignment in healthcare typically refers to a shared understanding between doctors and patients regarding key aspects of medical care such as treatment goals, plans, and patient expectations (Friedman et al., 2009). This alignment is crucial for improving healthcare outcomes, enhancing treatment adherence, and building patient trust (Li and Mao, 2015; McCabe et al., 2013). However, the characteristics of CMC create barriers to effective online information exchange, often making communication alignment more challenging (Lee and Zuercher, 2017; Yan et al., 2020). Despite its recognized importance, empirical methods for quantifying doctor–patient communication alignment and examining its effects remain underdeveloped in both offline and online contexts.
To address this gap, this study aims to quantify communication alignment in doctor–patient dialogues within OMCs, and investigate its impact on patients’ service evaluations. We assess information content based on information entropy, and apply PSO and RP to measure the alignment of information contributions between doctors and patients. Specifically, PSO quantifies the degree to which the frequency space representations of two signals overlap, reflecting the synchrony between doctors and patients in terms of their information distributions. RP measures the magnitude of delay between two signals, revealing the lag in their information contributions (Oullier et al., 2008; Xu and Reitter, 2017).
Contrary to previous findings, we argue that, in OMCs, effective alignment requires high synchrony and low delay. This proposition is based on two considerations. First, dialogues in OMCs are time- and message-limited. For example, on a certain OMC platform in China, a single consultation may last up to 48 hr and include no more than 50 messages. Second, the exchange of information in OMCs depends on mutual input: patients provide symptom descriptions for diagnosis, while doctors respond with medical information tailored to patients’ needs. Therefore, to ensure effective and efficient communication, both parties should contribute substantial information with high synchrony and minimal delay.
In summary, this study challenges the conventional definition of communication alignment from previous research and introduces measures that better align with the specific context of OMC. These measures aim to capture the dyad-level communication alignment between doctors and patients, allowing for further examination of its impact on patients’ service evaluations.
Research Hypotheses
In order to investigate the impact of doctors’ communication behaviors, communication alignment, and their interaction effects on patients’ service evaluations in OMCs, this study employs the theoretical framework of Expectancy Violations Theory (EVT) derived from expectation paradigms (Burgoon et al., 2016). EVT is adopted because it was originally proposed to explain communication-related expectations (Campo et al., 2004). In EVT, expectancy and evaluation are two key terms (Burgoon et al., 2016). Specifically, expectancy refers to abstractions about expected behaviors in a given communication context (Barry and Crant, 2000). Expectations can be either confirmed or violated by partners. Evaluation is the process of assigning a valence to a violation of an expectation, and valence can be positive or negative, depending on whether it is considered favorable or undesirable (Diehl and Poynor, 2010).
In the context of OMC, patients hold certain basic expectations regarding doctors and consultation processes. Patients anticipate quality service from professional doctors who can provide relevant information and instructions. Simultaneously, patients expect to engage in coordinated communication that allows them to comprehend and absorb information and instructions provided by doctors. Therefore, doctors’ behaviors and the ensuing communication processes can either confirm or violate patients’ initial expectations, subsequently influencing their service evaluations.
Individual Level: Doctors’ Behaviors and Patients’ Service Evaluations
Based on EVT (Burgoon et al., 2016), when a patient shares symptom information, medical test results, and consultation needs with a doctor, the patient expects a professional and experienced doctor capable of providing quality information and instructions regarding health condition, treatment plan, lifestyle habits, and so on (Roter et al., 2014; Roter and Larson , 2002). As forms of instrumental communication, doctors’ information acquisition and information provision behaviors are crucial to triggering patients’ confirmation or violation of these initial expectations.
Specifically, regarding doctors’ information acquisition, while it is often necessary for doctors to seek additional information from patients, it may not align with some patients’ initial expectations if they are primarily looking to acquire medical information from doctors. Moreover, excessive questioning by a doctor during a consultation may create an impression of inexperience or even unprofessionalism, thereby violating the patients’ expectations. An experienced doctor is expected to effectively analyze the initial information provided by patients, make accurate diagnoses, and then provide treatment recommendations without relying excessively on asking questions. By contrast, doctors’ information provision behaviors directly fulfill patients’ consultation needs, and align well with patients’ goal-oriented consumption motivation (Tan et al., 2023). For instance, more information provided by doctors about patients’ health conditions can help them better understand their health status, more detailed treatment plans can better assist patients in developing strategies to address health issues, and more advice on healthy lifestyles can help patients develop healthier habits. Based on the above elaboration, we propose the following hypotheses:
H1a: Doctors’ information acquisition in OMCs negatively affects patients’ service evaluations.
H1b: Doctors’ information provision in OMCs positively affects patients’ service evaluations.
Dyad Level: Communication Alignment and Patients’ Service Evaluations
The communication alignment of a dialogue signifies the cooperation between interlocutors. Previous studies reveal that better communication alignment leads to various favorable outcomes, including improved communication quality and task success (Fusaroli et al., 2014; Pickering and Garrod, 2004; Reitter and Moore, 2014).
In this study, the communication alignment between doctors and patients refers to the degree to which the two parties cooperate in their interactions during OMCs. A higher level of communication alignment can better satisfy patients’ expectations for the following reasons: First, better communication alignment can ensure effective interactions and communications between the two parties (Fusaroli et al., 2014; Ou et al., 2014), thereby improving patients’ perceived interactivity and social presence during the consultation. Second, better communication alignment between doctors and patients can reduce potential conflicts and uncertainty and improve doctors’ and patients’ information processing fluency (Volk and Zerfass, 2018), thus enhancing patients’ comprehension and absorption of information provided by doctors. Third, better communication alignment between the two parties also creates a sense of understanding and care for patients, contributing to a warm consultation atmosphere. Therefore, we propose H2:
H2: Communication alignment between doctors’ and patients’ messages in a dialogue positively affects patients’ service evaluations in OMCs.
Interaction Effects: Doctors’ Behaviors and Communication Alignment
Dialogues in OMC carry both individual-level and dyad-level characteristics (Chen et al., 2020; Zhang et al., 2019). Therefore, in addition to doctors’ communication behaviors (i.e., information acquisition and information provision) and communication alignment between doctors and patients, we also explore how the interaction effects between these two factors influence patients’ evaluations of consultation services.
Regarding doctors’ information acquisition, although we expect a negative impact on patients’ service evaluations due to its misalignment with patients’ primary focus on seeking answers from doctors, we posit that this negative impact will be mitigated when there is a high level of communication alignment in a doctor–patient dialogue. Better alignment of communication fosters a sense of understanding and care for patients, thus enhancing their perceived intimacy with doctors. Such a favorable feeling can mitigate the negative impact of doctors’ information acquisition to some extent.
Concerning doctors’ information provision, which is proposed to positively affect patients’ evaluations by confirming patients’ expectations, we hypothesize that this positive impact will be amplified when the communication alignment between doctors and patients is at a high level. Better alignment between the two parties improves communication quality and fluency of patient information processing (Volk and Zerfass, 2018), thus enabling patients to better comprehend and absorb the information and instructions provided by doctors. Therefore, we propose the following hypotheses:
H3a: Communication alignment between doctors and patients in a dialogue positively moderates the relationship between doctors’ information acquisition and patients’ service evaluations in OMCs.
H3b: Communication alignment between doctors and patients in a dialogue positively moderates the relationship between doctors’ information provision and patients’ service evaluations in OMCs.
Our research model and the key hypotheses are depicted in Figure 1.
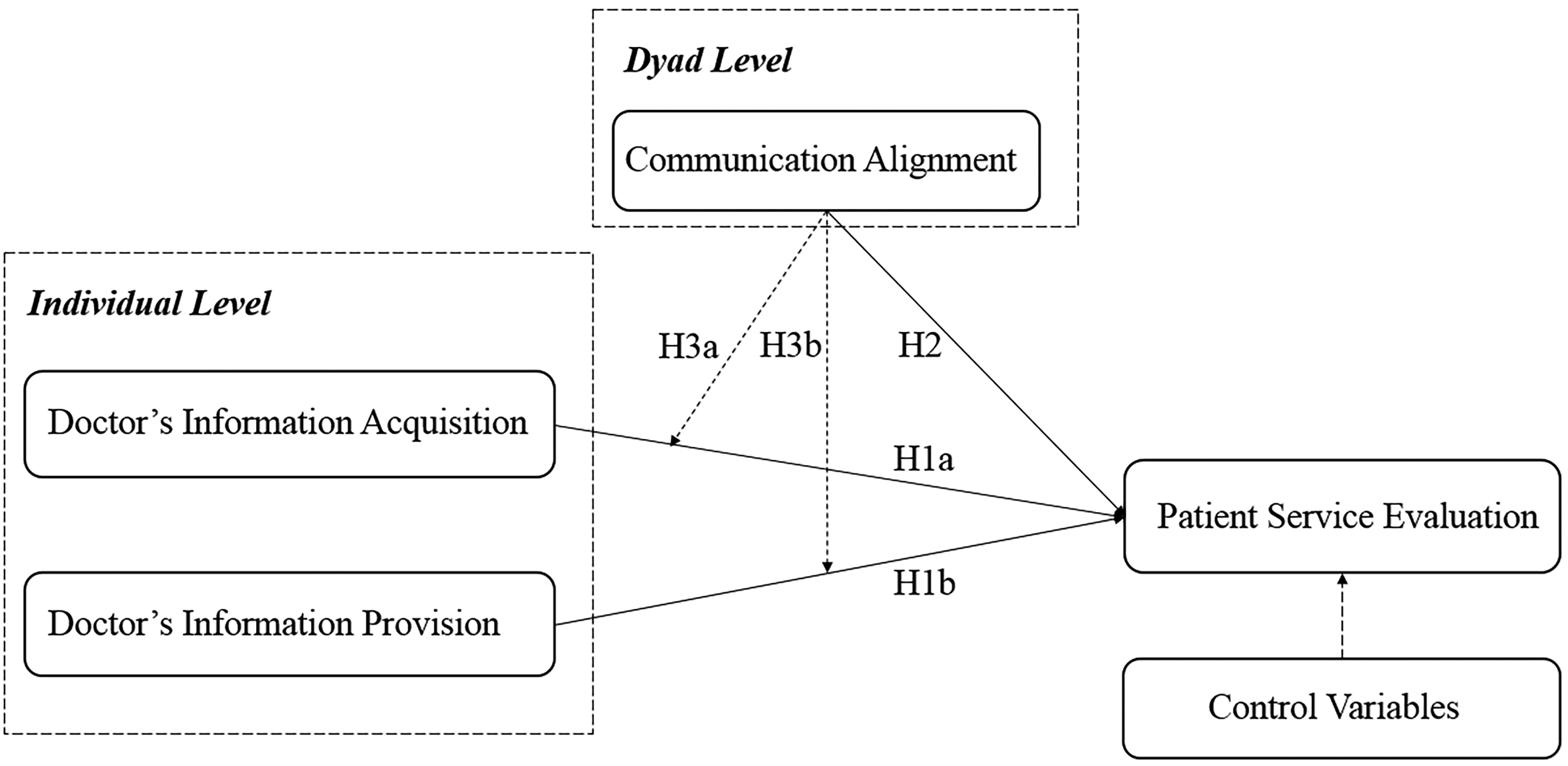
Research model.
In this section, we describe our data collection and measurement of key variables.
Research Context and Data Collection
We address our research questions using an observational dataset collected from an online medical consultation platform operated in China, i.e., Chunyu Doctor. This online platform is selected for three reasons. First, Chunyu Doctor was established in 2011, and it is a pioneer in providing OMC services. Second, to facilitate self-diagnosis and ensure service quality, Chunyu Doctor releases consultation records that show detailed communications between doctors and patients after shielding sensitive information and pictures, thus providing us with access to highly detailed individual-level communication data. Third, unlike platforms that support both online and offline services, Chunyu Doctor only offers online consultation and does not provide the function of ordering doctors’ offline services. Consequently, patients’ and doctors’ behaviors during online consultation depend exclusively on online doctor–patient interactions, thus avoiding the potential influence of offline doctor–patient relationships.
We collect all consultation records in the oncology department from January to June 2023 to obtain a dataset with desirable characteristics for our empirical analysis. Limiting the scope of data collection to one department allows us to control for the differences in disease severity and ensures the comparability of consultation records. The maximum duration of one consultation service is 48 hr, and the maximum number of conversations per service is 50. All contents of communications between doctors and patients during a service are recorded as one consultation record. A Java-based program is developed to retrieve doctors’ information and consultation records. A total of 4,497 detailed consultation records associated with 118 doctors are collected in the initial dataset. Two steps are taken to filter this data. First, consultation records with voice messages during the interactions are excluded. The number of records that contained voice messages is extremely small; excluding them eliminates the need for sophisticated speech recognition analysis without much loss of the sample size. Second, to effectively apply spectral analysis to doctor–patient dialogue sequences, we selectively retain consultation records featuring dialogue sequences comprising more than three interactions. Notably, consecutive messages from the same interlocutor are treated as a single interaction for the purpose of this analysis. After these preprocessing steps, we obtain a sample of 3,912 consultation records with 116 doctors in the final data sample.
Measurement of Variables
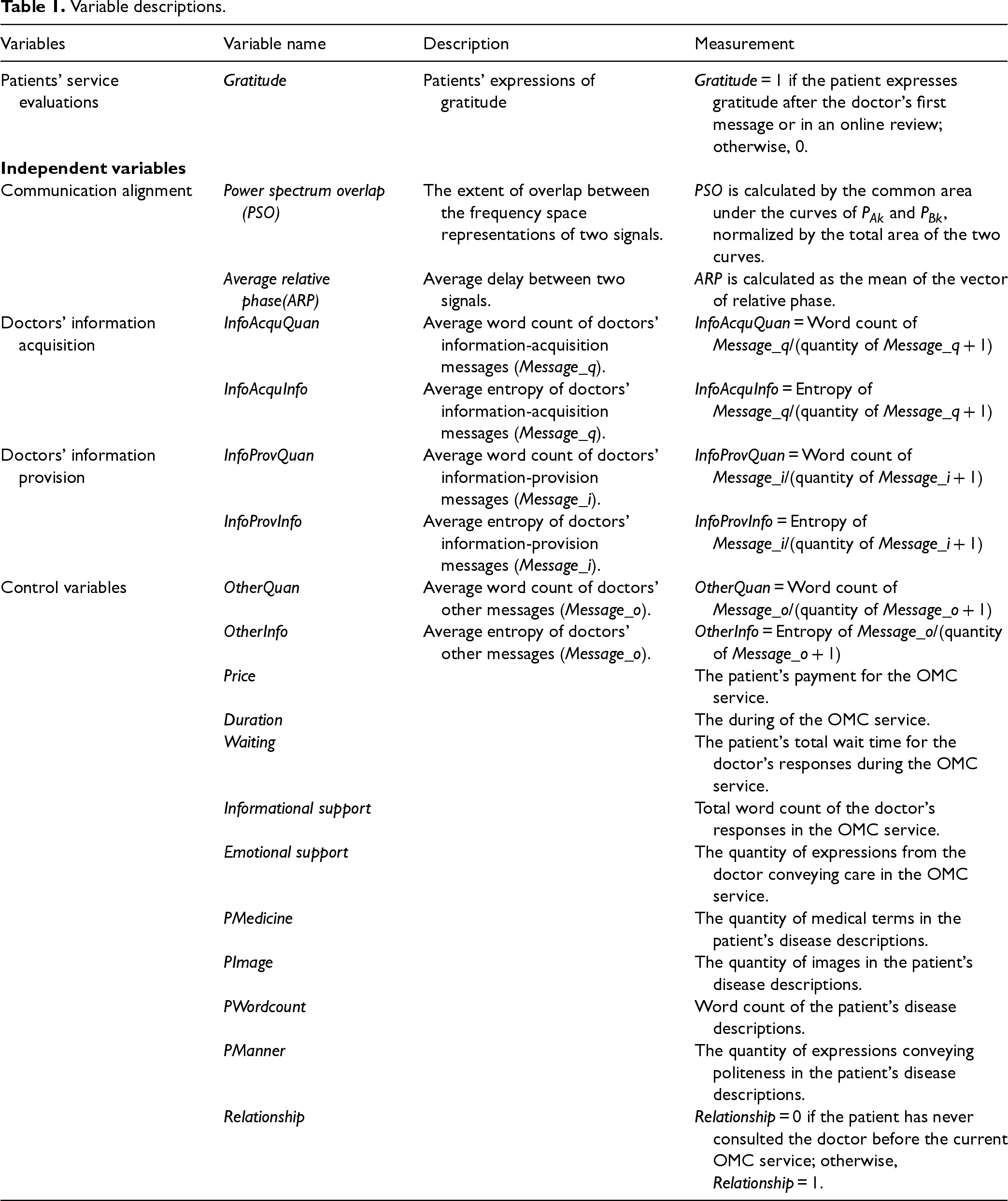
The measurement of our dependent, independent, and control variables is summarized in Table 1.
Variable descriptions.
Variable descriptions.
Dependent variables. In this study, we adopt patient gratitude as the primary indicator of patients’ service evaluations. Following previous research (e.g., Tan et al., 2023), we measure the variable of gratitude based on patients’ expressions of gratitude. Since there is no official channel on the Chunyu Doctor platform for patients to express gratitude, we chose to mine patients’ text messages during consultation or in online reviews that include phrases such as “thanks,” “thank you,” or “thanks a lot” to find expressions of patient gratitude. To prevent the bidirectional influence between doctors’ responses and patients’ gratitude, we exclude patients’ gratitude-expressing messages that occurred before doctors’ first messages. We code patient gratitude as 1 if a patient expresses gratitude after a doctor's first messages during a consultation or in an online review; otherwise, it is coded as 0.
Independent variables. As explained earlier, this study adopts two frequency space measures, power spectrum overlap (PSO) and relative phase (RP), to measure the level of communication alignment between a doctor and a patient in a dialogue. The two measures are calculated based on the following steps. First, to generate the entropy series of a doctor–patient dialogue in preparation for spectral analysis, we estimate the information density in the doctor–patient dialogue at the sentence level by computing the per-word entropy of each sentence using a trigram language model. Specifically, a sentence is a sequence of words, 
A dialogue consists of a series of messages contributed by two parties in a conversation. In CMC, one interlocutor can transmit multiple syntactically dependent or independent messages continuously to express his/her opinions. Given the asynchronous nature of CMC, in an online doctor–patient dialogue, an interlocutor has to assimilate information conveyed in all consecutive messages from the other party to obtain a comprehensive understanding of the dialogue. Consequently, we aggregate consecutive messages from one interlocutor into a unified sentence, thus converting the doctor–patient dialogue into a turn-taking interactive format. For the 
We split the entropy series
We conduct statistical tests to confirm that our data largely satisfies the assumption of stationarity, an important prerequisite for spectral analysis (Dwivedi and Subba Rao, 2011). Then, for a given dialogue
The power spectrum overlap,
The
This study employs two metrics, quantity and informativeness, to characterize doctors’ information acquisition and information provision messages in OMC. The quantity and informativeness of doctors’ information acquisition (InfoAcquQuan, InfoAcquInfo) and information provision (InfoProvQuan, InfoProvInfo) are measured by the average word count and average entropy of corresponding messages, respectively. This study applies a text classification method to identify doctors’ messages for information acquisition (
Third, six supervised learning algorithms are employed to train classification models for
Fourth, leveraging the results of text classification, we calculate the word count and the quantity of
Control variables. We include several variables to account for various aspects of the consultation service, including the service price paid by patients (Price), the duration of the service (Duration), and the waiting time experienced by patients (Waiting). We also consider the word count of doctors’ all responses (Informational support), the quantity of doctors’ caring and comforting expressions (Emotional support), the average word count (OtherQuan), and average entropy (OtherInfor) of doctors’ other messages to control for doctors’ other behaviors. To measure doctors’ emotional support, three research assistants are invited to identify instances of doctors’ caring and comforting messages within the manual coding set. They document text patterns of expressions such as “Nothing to worry about,” “Take it easy,” and “No need to be nervous.” The text patterns identified are compared, integrated, and subsequently compiled into a corpus. The frequency of these patterns in each consultation is counted as the measurement of Emotional support.
We also include control variables describing patients’ communication patterns to account for unobserved factors related to their conditions and behaviors. Considering the potential bidirectional influence of doctors’ and patients’ communication behaviors, we only analyze the patient's disease description posted before the doctor's first message in an OMC service, thus ensuring that the measured communication patterns are minimally influenced by the doctor. Specifically, we add four relevant variables as shown in Table 1. Three control variables, PMedicine, PImage, and PWordcount, not only reflect patients’ capability of describing their medical situations and needs, but also allow us to proxy for the nature of the consultations (e.g., the complexity of the health issues in a consultation). Further, PMedicine represents a patient's level of expertise in describing her medical situation, which is also a proxy for the patient's ability to comprehend the information provided by the doctor. The fourth control variable, PManner, reflects the patient's politeness towards doctors and may be positively related to their tendency to express gratitude.
Prior research shows that patients’ past interactions with doctors may affect doctor–patient relationships, which may, in turn, impact patients’ service evaluations (Liu et al., 2007). Chunyu Doctor anonymizes patients by partially masking their account IDs to protect user privacy. However, patients are required to report their gender and age when initiating a consultation, and this information is recorded in the initial messages of the consultation records. By cross-referencing the partially masked IDs with the self-reported gender and age information, we identify individual patients within the dataset. This process does not involve identifying real-world individuals, as all data used in this study is publicly available and anonymized by the platform to protect privacy. We introduce an additional control variable, Relationship, to capture whether the patient had any online consultation with the doctor before the current consultation.
The descriptive statistics and full correlation matrices for all variables are provided in Table E21 and Table E22 of the e-companion, respectively. Table 2 presents the correlation matrices for the dependent and independent variables. The results show that the majority of correlations between pairs of variables are lower than 0.40. However, there is a notable high correlation of 0.758 between InfoAcquQuan and InfoAcquInfo, which could potentially cause multicollinearity issues. To address this concern, the variance inflation factor (VIF) (O’Brien, 2007) is estimated. The VIF results for all variables are found to be less than 2.6, suggesting that multicollinearity is not a significant concern.
Correlation matrices of dependent and independent variables.
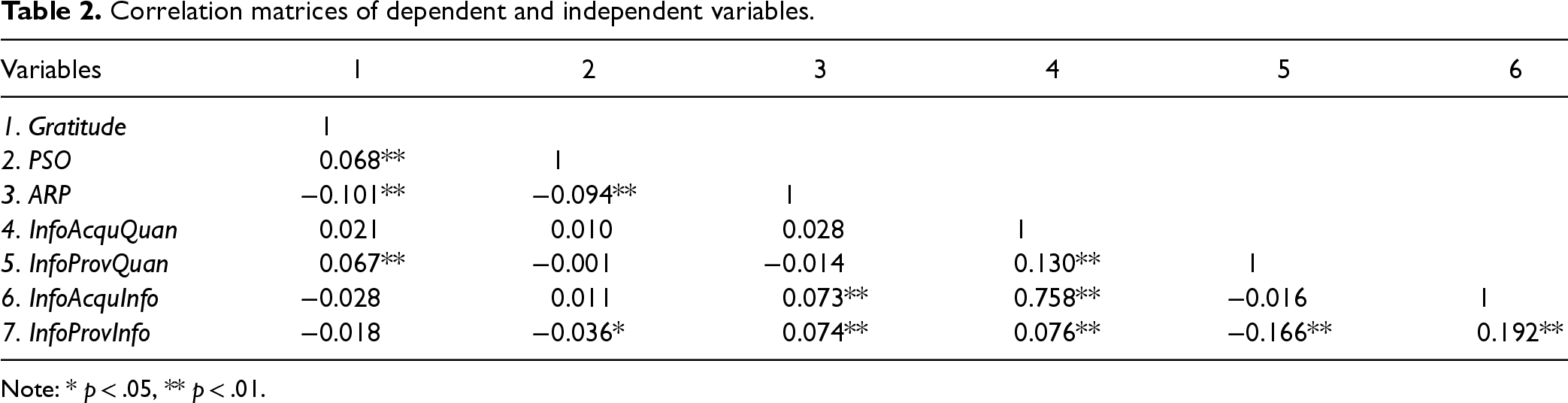
Note: * p < .05, ** p < .01.
We use several empirical strategies to investigate how doctor–patient interactions influence patient gratitude. Specifically, we begin with employing conditional logistic regression models with fixed effects. However, this approach may not support a causal interpretation due to potential reverse causality or omitted variables. For instance, both doctor–patient interactions and patient gratitude may be influenced by underlying factors such as doctor–patient relationships, disease severity, and unobserved patients’ characteristics. To address potential endogeneity concerns, we conduct additional analyses to rule out reverse causality and alternative explanations that may undermine causal inference. Furthermore, to ensure the robustness of our findings, we adopt the frequency of gratitude expressions as an alternative measure of patient gratitude and apply both count models and ordinary least squares (OLS) estimations with fixed effects as robustness checks. We also validate our main findings by incorporating dialogue-level measures of information acquisition and provision into the model. Finally, we summarize and compare the results of these checks to assess the reliability and consistency of our findings.
Main Analysis
We estimate the direct effects of doctors’ communication behaviors and doctor–patient communication alignment on patient gratitude based on Equation 3, and further examine their interaction effects based on Equation 4. In Equation 4, relevant variables are mean-centered prior to calculating interaction terms.
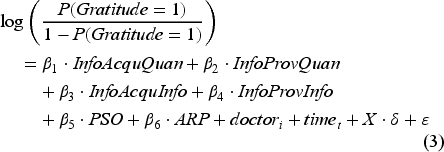
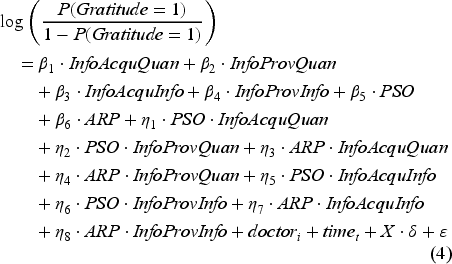
In the above specifications, the coefficients
By combining patients’ partially masked IDs with self-reported gender and age information, we identify 402 patients (out of a total of 3,092) who engage in multiple consultations, resulting in 1,222 consultation records. The remaining 2,690 patients each have only a single consultation. Additionally, we identify 157 doctor–patient pairs with repeated consultations, accounting for 477 records. These results indicate that repeated consultations by the same patient or the same doctor–patient pair constitute only a small portion of the overall dataset. Given that a logit model with fixed effects excludes groups with only positive or only negative outcomes, incorporating patient fixed effects leads to the exclusion of a substantial number of observations, leaving only patients with multiple consultation experiences and variation in outcomes. Consequently, patient fixed effects are not included in the main analysis.
To control for unobserved doctor heterogeneity, we employ a conditional logit model with fixed effects. To test the proposed hypotheses, we adopt a hierarchical regression strategy. Model 1 includes only control variables. We log-transform Duration and Wait to reduce skewness (e.g., Zhao et al., 2022). Recognizing the high correlation between InfoAcquQuan and InfoAcquInfo, we introduce variables related to the quantity and informativeness of doctors’ messages in Model 2 and Model 3, respectively. These variables are then combined in Model 4. Furthermore, PSO and ARP are included in Model 5 to explore the effect of doctor–patient communication alignment. To test moderating effects, we include interaction terms between doctors’ communication behaviors and communication alignment. We introduce interaction terms PSO/ARP × InfoAcquQuan/InfoProvQuan in Model 6, and add PSO/ARP × InfoAcquInfo/InfoProvInfo in Model 7, which helps mitigate potential multicollinearity issues caused by highly correlated interaction terms. Finally, we build a joint model with all interaction terms in Model 8. Table 3 summarizes the results of all models and illustrates the following key findings.
Effects of doctor–patient interactions on patient gratitude.
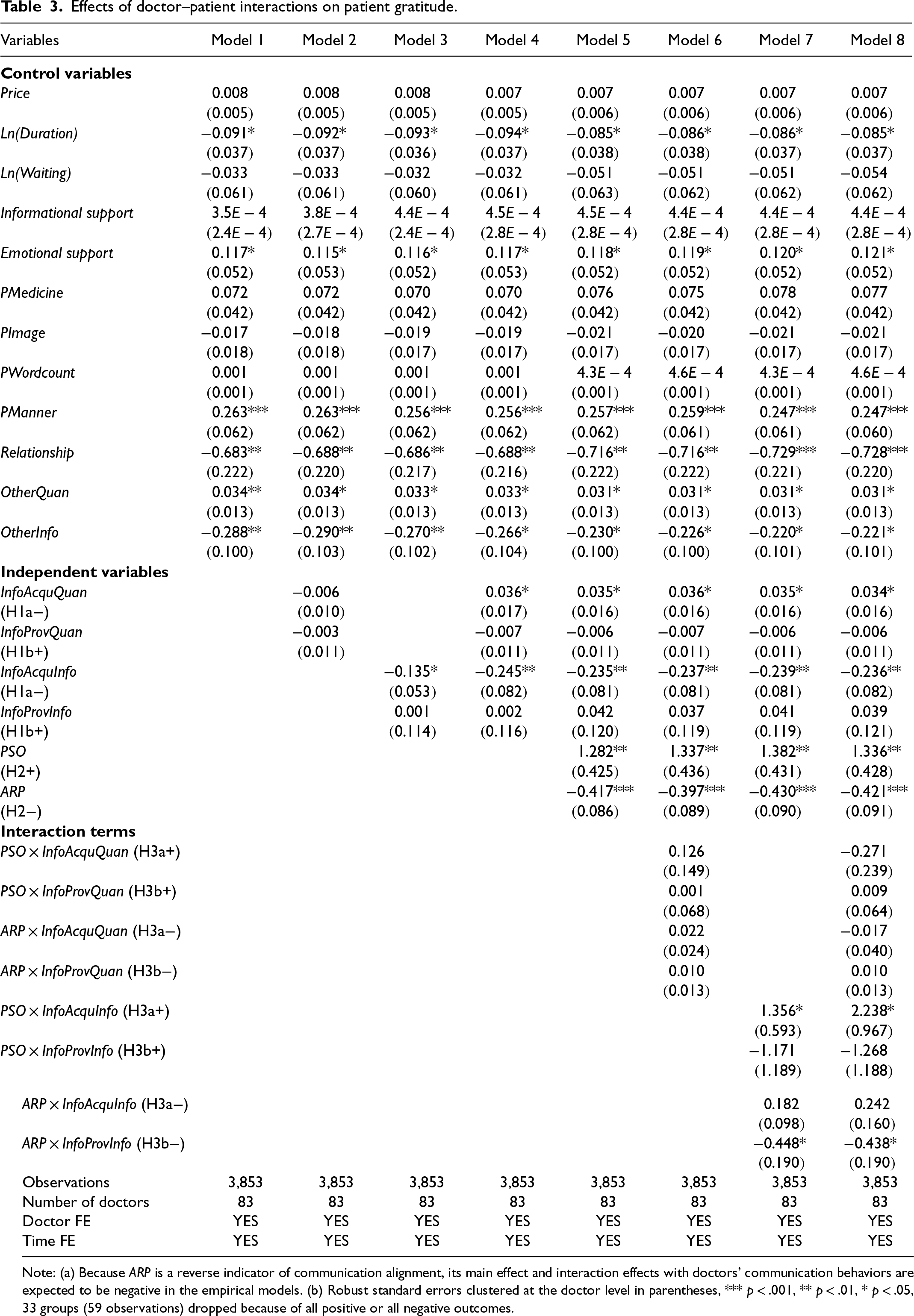
Note: (a) Because ARP is a reverse indicator of communication alignment, its main effect and interaction effects with doctors’ communication behaviors are expected to be negative in the empirical models. (b) Robust standard errors clustered at the doctor level in parentheses, *** p < .001, ** p < .01, * p < .05, 33 groups (59 observations) dropped because of all positive or all negative outcomes.
First, among the control variables in Model 1, doctors’ emotional support is found to have a positive effect on patient gratitude, consistent with previous research (Tan et al., 2023). Second, Models 2, 3, and 4 indicate that the informativeness of doctors’ information acquisition messages negatively affects patient gratitude, whereas both the quantity and informativeness of doctors’ information provision messages exhibit no significant effects. Notably, when both the quantity and informativeness of doctors’ information acquisition messages are simultaneously included in Model 4, the coefficient for quantity changes from a nonsignificant negative value in Model 2 to a significant positive one. This suggests that the effect of message quantity becomes evident only when its informativeness is considered, highlighting the critical role of informativeness in evaluating the impact of doctors’ communication behaviors. In summary, H1a is partially supported, whereas H1b is not supported.
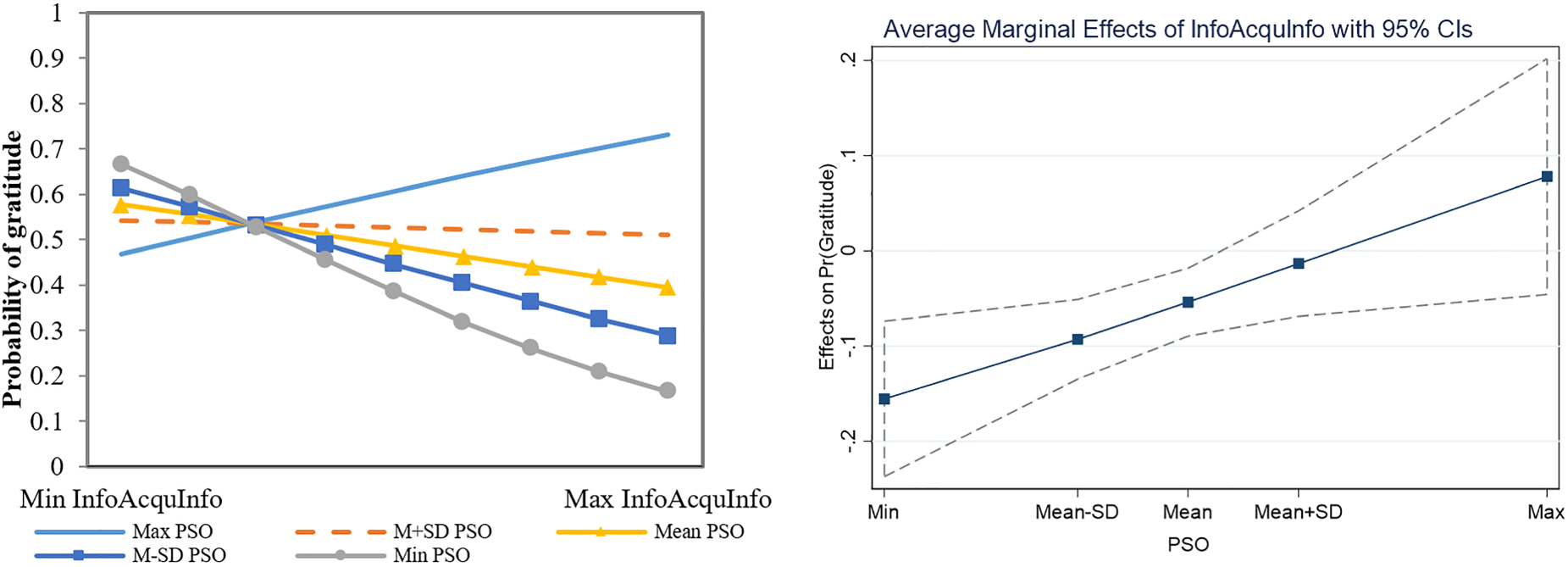
Third, Model 5 reveals that the coefficients of PSO and ARP are significantly positive and negative, respectively, indicating that doctor–patient communication alignment plays an important role in affecting patient gratitude, thus supporting H2. Fourth, the interaction effects between communication alignment and the quantity and informativeness of doctors’ messages on patient gratitude are examined in Models 6, 7, and 8. The results confirm the interaction effects between PSO and InfoAcquInfo, and between ARP and InfoProvInfo, on patient gratitude, further emphasizing the importance of communication alignment in shaping patients’ perceptions of doctors’ communication behaviors. Specifically, an increase in PSO will weaken the negative relationship between the informativeness of doctors’ information acquisition messages and patient gratitude. We plot the interaction effect of PSO and InfoAcquInfo on patient gratitude in Figure 2. Specifically, following the procedure prescribed by Aiken and West (1991), we plot the effect of InfoAcquInfo (from minimum to maximum) on patient gratitude at different levels of PSO based on the results from Model 8. As shown in the left panel of Figure 2, the negative slopes of the logit regression lines are steeper at lower levels of PSO than at higher levels. Furthermore, the average marginal effects of InfoAcquInfo on patient gratitude at different levels of PSO are visualized in the right panel of Figure 2.
Interaction effects of PSO and InfoAcquInfo on patient gratitude.
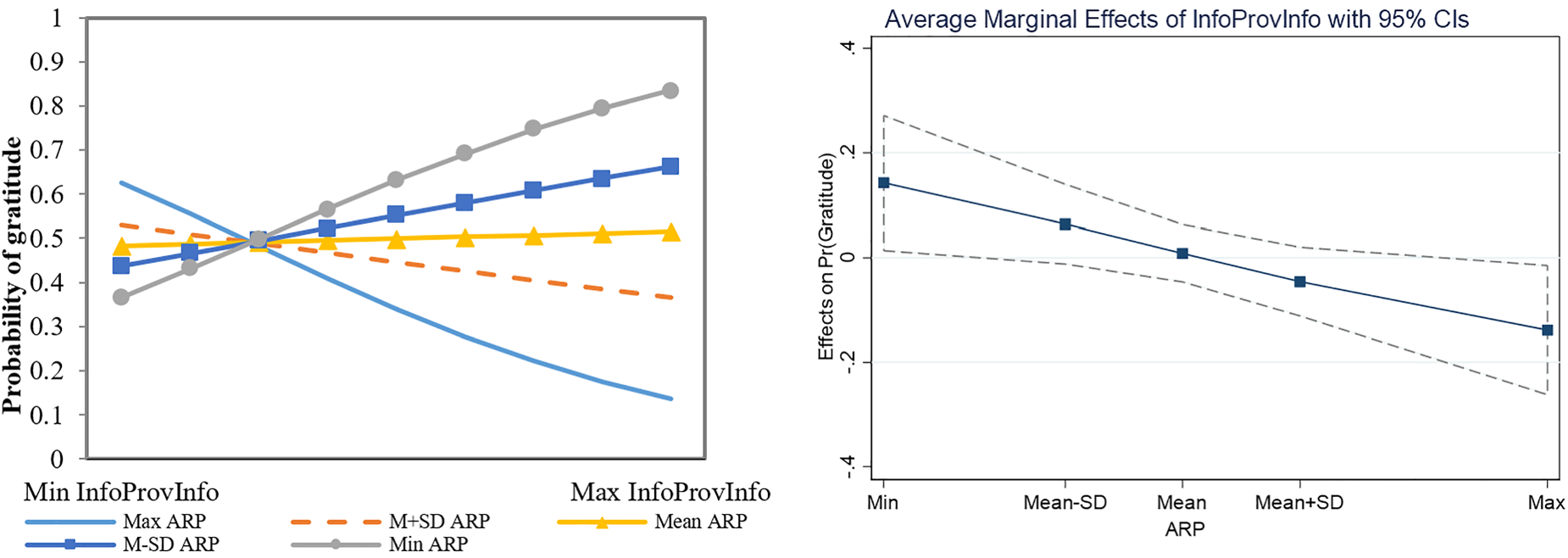
The effect of InfoProvInfo on patient gratitude is found to be insignificant. However, the coefficient of ARP × InfoProvInfo suggests a negative moderating effect of ARP on the impact of InfoProvInfo. We plot the interaction effect of ARP and InfoProvInfo on patient gratitude in Figure 3. Specifically, we plot the effect of InfoProvInfo (from minimum to maximum) on patient gratitude at different levels of ARP based on the results from Model 8. As shown in the left panel of Figure 3, the slopes of the logit regression lines shift from positive to negative as ARP increases, which indicates that, when the doctor–patient communication alignment is high, the informativeness of doctors’ information provision messages has a positive effect on patient gratitude. Conversely, this effect turns negative when the communication between doctors and patients is not well-coordinated. The marginal effects of InfoProvInfo on patient gratitude at different levels of ARP are visualized in the right panel of Figure 3.
Interaction effects of ARP and InfoProvInfo on patient gratitude.
In conclusion, H1a is partly supported, H1b is not supported, and the remaining hypotheses are supported. The results suggest that the informativeness of doctors’ information acquisition has a negative impact on patient gratitude. Specifically, when doctors tend to pose questions that are overly complex, varied, or unpredictable, patients are less likely to experience gratitude. This may be attributed to the increased cognitive load such questions place on patients, which potentially hinders effective communication between doctors and patients. Although higher informativeness of doctors’ questions can diminish patient gratitude, delivering these questions in a more elaborate or detailed manner may improve patients’ experience, ultimately enhancing gratitude.
Furthermore, doctor–patient communication alignment not only directly influences patient gratitude but also moderates the relationship between the informativeness of doctors’ messages and patient gratitude. High synchrony and low delay indicate that doctors and patients exchange information at a similar pace, which reflects a well-coordinated and efficient communication process. This communication alignment represents a level of service quality that exceeds the normal expectations in OMCs, thereby eliciting patient gratitude. Conversely, when communication alignment is low, complex or highly informative messages from doctors can increase patients’ cognitive load and require greater professional knowledge and health literacy for comprehension. As a result, the negative impact of information acquisition on patient gratitude is intensified, while the positive effect of information provision is diminished.
However, our results indicate that neither the quantity nor the informativeness of doctors’ information provision significantly influences patient gratitude. This outcome appears counterintuitive, given the common belief that providing medical information is crucial for patients’ service evaluations. We propose two possible explanations for this unexpected finding. First, the non-significant average effect of the informativeness of doctors’ information provision may stem from its divergent roles under varying conditions of doctor–patient communication alignment. Specifically, while informativeness positively impacts patient gratitude when communication alignment is high, it exerts a negative effect when alignment is low, thereby offsetting the overall effect. Second, the informativeness of doctors’ information provision may be more relevant to patient satisfaction than to patient gratitude in OMCs. Patients’ primary expectation of using OMCs is to obtain medical information to address health concerns and fulfill goal-oriented needs (S. Liu et al., 2020; Tan et al., 2023). As such, information provision is viewed as a fundamental obligation of doctors in OMCs, primarily contributing to patient satisfaction, as extensively documented in prior research (Chen et al., 2020; Yang et al., 2015, 2019). In contrast, eliciting gratitude typically requires doctors to make extra efforts that go beyond standard service expectations (Tan et al., 2023). Therefore, the mere provision of medical information—while essential for meeting patients’ informational needs—may not be sufficient to evoke patient gratitude.
To support the second explanation, we conduct an analysis where patient satisfaction is selected as the dependent variable to examine the influence of the quantity and informativeness of doctors’ information acquisition and provision messages on patient satisfaction. The new variable Patient satisfaction is measured by the rating assigned by the patient to the doctor's service. The ordered logit model with doctor fixed effects is employed for the analysis, and the results are summarized in Table E19 of the e-companion. In this table, Model 2 shows a negative effect of InfoAcquQuan on patient satisfaction, and Model 3 demonstrates that InfoAcquInfo negatively impacts patient satisfaction, whereas InfoProvInfo has a positive effect. In summary, delivering medical information in an informative manner enhances patient satisfaction, whereas lengthy or complex questions from doctors may be counterproductive. However, the coefficients of PSO and ARP are both insignificant, suggesting that communication alignment is not a crucial factor in meeting patients’ goal-oriented needs and, therefore, does not have a significant effect on patient satisfaction. These findings are consistent with our inference regarding the different impacts of doctors’ information provision messages on patient satisfaction and patient gratitude.
As discussed earlier, the relationship between doctor–patient interaction and patient gratitude may face potential endogeneity issues. In this subsection, we discuss a few possible sources of endogeneity and how they are addressed in this study.
Reverse Causality
Concerning the relationship between doctors’ communication behaviors and patient gratitude, there exists a potential issue of reverse causality. Specifically, expressions of gratitude from patients could in turn motivate doctors to engage more actively in communication. This study has employed three strategies to address this concern. First, we exclude instances of patients’ gratitude expressions before doctors’ initial response. Second, we characterize the quantity and informativeness of doctors’ communication behaviors based on average measures, primarily to reflect doctors’ inherent communication styles rather than their overall communication behaviors, which could be affected by patients’ behaviors. Third, we analyze the temporal distribution of patient gratitude within the dialogue and construct a refined measure of gratitude that includes only expressions occurring in the later stages of the conversation. Specifically, we summarize the distribution of gratitude across all dialogues in our dataset (shown in Figure E1 of the e-companion) and conduct four robustness checks by measuring gratitude based on expressions appearing beyond the 50%, 60%, 70%, and 80% points of the conversation. The corresponding results are presented in Tables E8, E9, E10, and E11 of the e-companion and are generally consistent with our main findings.
Potential Confounders
Questions may also arise regarding a few possible confounders, i.e., factors that may influence both doctors’ communication behaviors and patients’ service evaluations. We discuss how the concerns are addressed. Patient's communication behaviors. In the main analysis, we include a set of control variables that characterize patients’ communication patterns, including PMedicine, PImage, PWordcount, and PManner, to mitigate the impact of patients’ conditions and behaviors. Doctor–patient relationships. We include a control variable, Relationship, in our model, which captures whether the patient has had any prior online consultation with the doctor before the current consultation to control for the potential effect of the doctor–patient relationship. However, the relationship between a patient and a doctor may strengthen over time with repeated interactions (Zhao et al., 2022). Therefore, in an additional analysis, we use the number of times a patient consulted a doctor prior to the current consultation (i.e., nPriorConsult) as an alternative proxy for the doctor–patient relationship. The results, summarized in Table E1 in the e-companion, indicate that controlling for nPriorConsult does not materially alter the main findings of this study. Disease severity. The relationship between doctors’ communication behaviors and patients’ service evaluation may be confounded by a third variable: disease severity. Although we restrict our data collection to the oncology department to mitigate potential heterogeneity across disease types, considerable variation in disease severity still exists within this department. To address this issue, we quantify disease severity for each consultation based on doctor–patient dialogues. We use a binary variable, CanDiagnosis, to indicate whether the patient is diagnosed with cancer, and a continuous variable, Severity, to measure the level of disease severity. Specific measurements of these two variables are provided on page 2 of the e-companion.
Based on the above measurements, we employ three strategies to test the effect of disease severity. First, we adopt CanDiagnosis as a proxy for disease severity to assess whether a cancer diagnosis impacts the main results of the study. Second, we use Severity as another proxy to evaluate the influence of varying disease severity. The results, shown in Table E3 and Table E4 in the e-companion, indicate that neither CanDiagnosis nor Severity affects patient gratitude, and the main results of this study remain valid. Third, recognizing that the CanDiagnosis = 0 group may contain both non-cancer and undiagnosed cancer cases, we conduct a robustness check using the subsample with CanDiagnosis = 1. The results, shown in Table E5 in the e-companion, support our main findings and further reveal the moderating effect of Severity on the relationship between the informativeness of doctors’ information acquisition and patient gratitude. Unobserved time-invariant characteristics of patients. We employ a logit model with patient fixed effects to control for unobserved, time-invariant characteristics of patients, acknowledging that these factors may influence their service evaluations. Given that a logit model with fixed effects excludes samples with all positive or negative outcomes, adopting patient fixed effects would result in the loss of a substantial number of records, leaving only patients with multiple consultation experiences. The outcomes of this analysis, presented in Table E6 in the e-companion, reveal some differences compared to the primary findings of this study. Specifically, Model 4 in Table E6 suggests that neither the quantity nor the informativeness of doctors’ information acquisition messages has a significant influence on patient gratitude, which differs from the main results. This discrepancy may stem from sample bias in this analysis, as the analysis primarily includes experienced patients who are more skilled at understanding questions posed by doctors and more capable of engaging in detailed, professional exchanges. Additionally, the effects of ARP and the interaction between ARP and InfoProvInfo are no longer significant. Nevertheless, the positive effect of PSO remains, underscoring the importance of doctor–patient communication alignment. This alignment also affects patients’ evaluations of doctors’ communication behaviors by moderating the influence of InfoAcquInfo on patient gratitude.
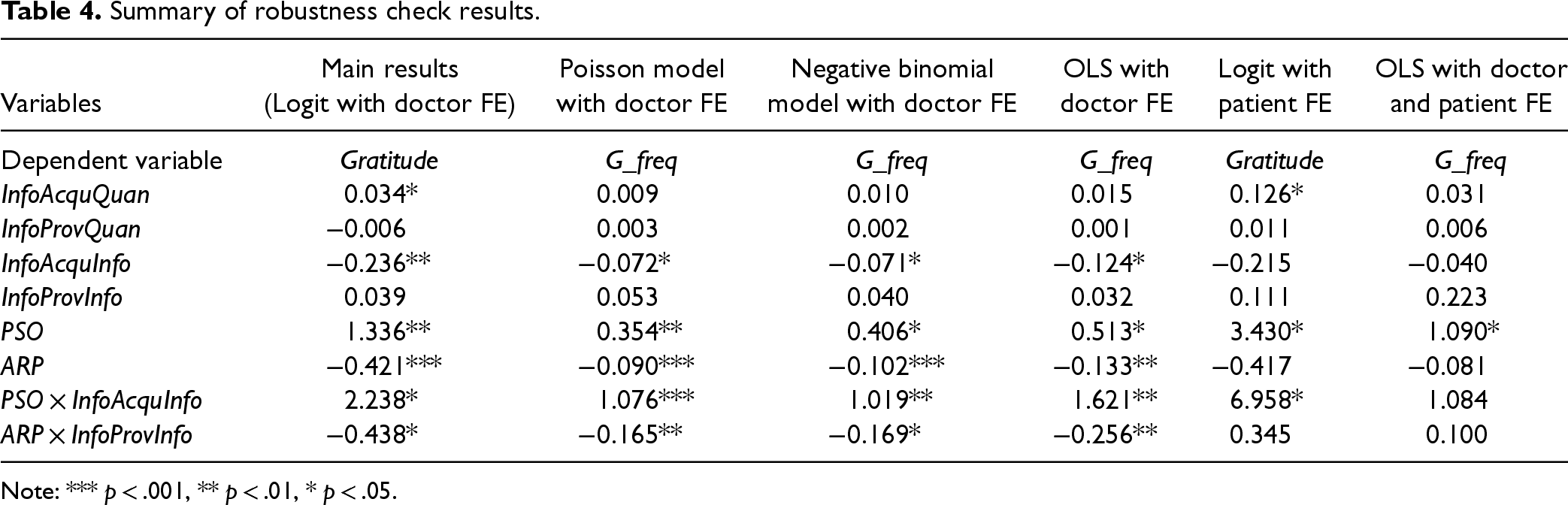
We conduct seven additional robustness checks to assess the robustness of our main findings. Instead of treating patient gratitude as a binary variable, we construct an alternative measure—gratitude frequency (hereafter,
Summary of robustness check results.
Summary of robustness check results.
Note: *** p < .001, ** p < .01, * p < .05.
In models including doctor fixed effect, most results confirm the consistency of the main results of this study, with the exception of the effect of InfoAcquQuan. This indicates that a higher quantity of doctors’ information acquisition messages is not effective in eliciting increased expressions of gratitude from patients. In OLS models incorporating both doctor and patient fixed effects (which introduces sample bias), the direct effects of doctors’ communication behaviors are not observed, in contrast to the main results. The coefficients of interaction terms PSO × InfoAcquQuan and ARP × InfoProvInfo are observed to be significant in Model 6 and Model 7, respectively, but both become insignificant when they are incorporated in Model 8, which may be caused by multicollinearity issues. Overall, the results of these analyses largely support the robustness of our key findings.
Moreover, we incorporate dialogue-level measures of information acquisition and provision into the model. Specifically, we first control for the total word counts of doctors’ information acquisition (TotalAcquQuan) and provision (TotalProvQuan) messages to examine the effects of InfoAcquInfo and InfoProvInfo. Second, we control for the total entropy of doctors’ information acquisition (TotalAcquInfo) and provision (TotalProvInfo) messages to examine the effect of InfoAcquQuan and InfoProvQuan. Third, we control for the number of doctors’ information acquisition (InfoAcqu) and provision (InfoProv) messages to examine the effects of InfoAcquQuan, InfoAcquInfo, InfoProvQuan, and InfoProvInfo. Due to the high correlation between these dialogue-level measures and the control variable Informational support, we exclude Informational support from these robustness checks. The results of these models are presented in Table E16, Table E17, and Table E18 in the e-companion, respectively. In summary, after controlling for doctors’ overall behaviors throughout the entire dialogue, the direct effect of InfoAcquInfo appears to diminish compared to our main results. However, the interaction between PSO and InfoAcquInfo remains significant across all robustness checks. This suggests that the negative effect of InfoAcquInfo on patient gratitude diminishes or even reverses as communication alignment increases, resulting in its observed non-significant overall effect. Overall, these checks reinforce the validity of our main findings.
The proper interpretation of interaction effects in binary logit specifications has been recognized as a challenging aspect in previous studies. As highlighted in Ai and Norton (2003), the interaction effect in non-linear models can exhibit variations in magnitude, significance, and sign (positive or negative) across observations. Consequently, reported coefficients of interaction terms may not precisely capture the true marginal effects. Norton et al. (2004) propose a solution for this issue through the Stata command, inteff, which correctly calculates the mean magnitudes of interaction effects in a logit model with appropriate signs and significance levels. We use the inteff module in Stata 15 (Ai and Norton, 2003; Norton et al., 2004) to further examine the interaction effects between PSO and InfoAcquInfo, and between ARP and InfoProvInfo, on patient gratitude. The results, shown in Table E23 and Figure E4 (for H3a), and Table E24 and Figure E5 for (H3b) in the e-companion, provide additional support for our hypotheses.
Discussion
Key Findings
The key findings of this study are as follows. First, this study investigates the impact of doctors’ individual-level communication behaviors—specifically, information acquisition and information provision—on patient gratitude in OMCs. The findings indicate that the quantity and informativeness of doctors’ information acquisition messages positively and negatively affect patient gratitude, respectively, whereas neither the quantity nor the informativeness of information provision messages significantly affects patient gratitude. Second, this study explores the role of dyad-level communication alignment in influencing patient gratitude, revealing that the alignment in doctor–patient communication is crucial for enhancing patient gratitude. Third, this study uncovers significant interaction effects between doctors’ individual-level communication behaviors and dyad-level communication alignment. Specifically, the negative impact of the informativeness of doctors’ information acquisition messages is mitigated by better communication alignment. Additionally, when communication alignment is low, the positive effect of the informativeness of doctors’ information provision messages is reversed.
Theoretical Contributions
This study makes several important theoretical contributions to the existing literature. First, this study pioneers in exploring the influence of dyad-level features of doctor–patient interactions on patients’ service evaluations. Doctor–patient interactions involve dynamic two-way information exchange, but existing studies have mainly concentrated on the individual-level behaviors of doctors or patients (Chen et al., 2020; Tan and Yan, 2020; Xing et al., 2019), while overlooking the dyad-level features. Moreover, previous studies have mainly modeled the static characteristics of interactions, without considering the dynamic communication processes. By applying spectral analysis techniques to the entropy series of doctor–patient dialogues (transforming time space to frequency space), this study quantifies the dyad-level communication alignment in doctor–patient interactions and examines its impact on patients’ service evaluations. The findings present a novel perspective for studying doctor–patient interactions and lay the foundation for further investigation into dynamic dyad doctor–patient interactions in the online healthcare context.
Second, this study complements existing research on online healthcare communication by incorporating the dimension of informativeness to evaluate the effects of communication behaviors. Previous studies have primarily characterized doctors’ behaviors based on the quantity of content, such as the total number of responses provided, the word counts of information shared, and the frequency of professional words used (Chen et al., 2020; Yang et al., 2015, 2019), while neglecting the content's informational value. This study introduces the information entropy measure to quantify the informativeness of messages and evaluates doctors’ communication behaviors by integrating both quantity and informativeness. The findings of this study reveal that the informativeness of doctors’ messages is a crucial determinant of patients’ service evaluations in OMCs. This underscores the importance of incorporating informativeness as a key feature in developing a more comprehensive framework for characterizing online doctor–patient communication behaviors.
Third, this study contributes to healthcare operations management literature by offering new insights into improving patients’ service evaluations in online healthcare. Delivering patient-centered care and improving the quality of patient-perceived medical service have been important topics in online healthcare (Bretthauer and Savin, 2018; Yan et al., 2019). Previous research has primarily investigated how doctors’ overall communication behaviors throughout the interaction process affect patients’ perceptions and service evaluations, and based on empirical results, often recommend an increase in the word count and frequency of doctors’ responses (Chen et al., 2020; Yang et al., 2015, 2019). However, limited attention has been given to enhancing service quality by refining individual communication behaviors. By analyzing the features of doctors’ information acquisition and information provision behaviors, this study sheds light on how doctors’ inherent communication patterns influence patients’ service evaluations, thus offering valuable insights into improving doctors’ communication skills to enhance the quality of doctor–patient interactions. Furthermore, this study elaborates on the role of dyad-level communication alignment in affecting patients’ service evaluations by confirming both its direct influence and its interaction effects with individual-level behaviors. The findings pave the way for future research on the role of dyad-level features in affecting online service evaluations.
Fourth, this study enriches the literature on communication alignment in the online healthcare context. By applying the measure of communication alignment to the realm of online doctor–patient interactions, this study enhances the understanding of coordinated communication in different research contexts. Previous studies, based on various interaction tasks in diverse research contexts, have suggested that low synchrony and high delay indicate more coordinated communication (Fusaroli et al., 2012; Xu and Reitter, 2017). By contrast, this study reveals that in online doctor–patient medical consultation, high synchrony and low delay are conducive to stimulating patient gratitude. These findings demonstrate the variability in standards for communication alignment in different settings, providing new insights into communication alignment and prompting further investigation under varied circumstances.
Practical Implications
This study offers several important practical implications. Our findings provide practical guidance for doctors to enhance their service strategies in two crucial aspects. First, doctors can significantly improve their individual communication skills by focusing more on informativeness than on merely the length of their responses. Specifically, they should put forward questions in a clear and easily understandable manner, as overly complex inquiries that require specialized knowledge may lead to negative patient experiences and hinder the development of gratitude. While providing detailed questions can partially offset these negative effects, maintaining low complexity remains essential. Additionally, emphasizing the informativeness and quality of the information provided, rather than merely increasing its quantity and length, can improve patients’ service experiences, elicit greater patient gratitude, and contribute to the establishment of long-term doctor–patient relationships.
Second, the study underscores the importance of well-coordinated communication between doctors and patients during online interactions. Doctors should prioritize maintaining high synchrony and minimize delays in terms of information contribution when they exchange information with patients. This involves aligning their responses with the topics and concerns that interest patients and ensuring that feedback matches the level of detail in patients’ inquiries. By aligning their communication with patients’ needs, doctors can foster more effective and engaging interactions, which in turn enhance patients’ understanding of the information from doctors. These strategies not only improve patients’ evaluations of service quality but also promote the overall success and efficacy of online medical consultations.
Limitations and Future Research
This study has several limitations that also represent opportunities for future research. First, our extraction of key variables from consultation records relies on text classification and pattern recognition methods. Future research could explore the potential for improved prediction performance by utilizing a more extensive dataset or incorporating state-of-the-art machine learning algorithms. Second, the data for this study is collected from the oncology department to minimize variations arising from different disease types. Future investigations could extend the analyses to other medical departments or different contexts to gain new insights. Finally, the data for this study is collected from patients who have provided service evaluations on the OMC platform. However, not all patients on the studied OMC platform provide service evaluations, resulting in missing data and introducing potential bias into our findings. Future studies could conduct experiments or surveys to capture patients’ subjective perceptions and service evaluations, thus mitigating potential sample bias and validating the results of this study.
Supplemental Material
sj-pdf-1-pao-10.1177_10591478251369159 - Supplemental material for Dyadic Interactions and Patient Service Evaluation in Online Healthcare Consultations: The Role of Communication Alignment
Supplemental material, sj-pdf-1-pao-10.1177_10591478251369159 for Dyadic Interactions and Patient Service Evaluation in Online Healthcare Consultations: The Role of Communication Alignment by Hongying Tan, Benjiang Lu, Zhengrui Jiang and Baojun Ma in Production and Operations Management
Footnotes
Acknowledgments
The authors are grateful to the department editor, senior editor, and anonymous reviewers for their insightful suggestions that have significantly improved this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Natural Science Foundation of China (Grant No: 72431008, 72172092), National Key Research and Development Program of China (2024YFB3311600), Natural Science Foundation of Sichuan Province (2024NSFSC1060), Shanghai Key Laboratory of Brain-Machine Intelligence for Information Behavior (22dz2261100), Humanities and Social Sciences Research Project of Chongqing Municipal Education Commission (23SKGH119).
How to cite this article
Tan H, Lu B, Jiang Z and Ma (2026) Dyadic Interactions and Patient Service Evaluation in Online Healthcare Consultations: The Role of Communication Alignment Production and Operations Management 35(1): 203–222.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.