
Abstract
Telehealth services became popular due to the COVID-19 pandemic, yet their operational impacts on healthcare organizations are not well-understood. Patient behaviors can vary significantly between telehealth and in-person appointments, introducing new challenges and opportunities for healthcare delivery. We examine two key behaviors contributing to nonadherence to medical appointments: No-shows and unpunctuality. Analyzing 412,415 telehealth and in-person appointments across a major US medical system from 2020 to 2022, we find that telehealth appointments reduce no-shows by 3.0 percentage points (23.1%) and late-arrivals by 11.4 percentage points (35.6%), indicating significant improvements in appointment adherence. We also find that telehealth is particularly effective in improving adherence to follow-up appointments but may be less suitable for initial consultations with new patients. In addition, telehealth improves adherence most among demographic groups with historically lower in-person attendance—women, racial minorities, Medicaid patients, and younger adults—underscoring its potential to reduce disparities in access. Our analysis suggests that while telehealth may increase patient revisit rates and create extra work for providers, the gains from reduced no-shows, particularly for follow-ups, lead to a net boost in provider productivity. Finally, we explore the best strategies to integrate telehealth into a provider’s daily scheduling template, showing that scheduling telehealth appointments before in-person visits enhances operational efficiency compared to the opposite sequence. Policymakers should recognize telehealth’s capacity to improve appointment adherence, reduce disparities, and enhance productivity, and support its adoption through appropriate regulations. Healthcare organizations should strategically deploy telehealth to address the root causes of patient nonadherence. By offering telehealth appointments to patients facing barriers to in-person care, they can simultaneously optimize both access and productivity.
Introduction
Telehealth, or telemedicine, refers to the remote exchange of medical services via telecommunication and electronic technologies (Tuckson et al., 2017). It includes synchronous exchanges, such as video/audio calls between patients and providers, and asynchronous communications through emails and text messages. We focus on the synchronous form of telehealth visits in the ambulatory setting, which has diagnostic and therapeutic functions and can serve as a substitute for conventional in-person visits. Telehealth visits were not widespread before the COVID-19 pandemic, as the Centers for Medicare & Medicaid Services (CMS) only reimbursed such services in rural areas and specific medical facilities (Tuckson et al., 2017). However, the COVID-19 pandemic significantly increased the prevalence and recognition of telehealth visits and their benefits.
The first case of COVID-19 in the United States was reported in January 2020 (CDC, 2020). Shortly thereafter, cases were detected in all 50 states, prompting the need for significant measures to contain the virus. On January 31, the federal government declared COVID-19 a public health emergency (Azar, 2020). In response, federal and local governments implemented lockdowns and stay-at-home orders, suspending all nonessential in-person economic and social activities. To ensure continuity of care, the federal government temporarily relaxed restrictive telehealth reimbursement policies. It began reimbursing video telehealth visits for all Medicare beneficiaries at the same rate as office visits, allowed out-of-state physicians to provide telehealth services, and approved the use of applications such as Skype, FaceTime, and Zoom for medical appointments (CMS, 2020). Private payers adopted similar policies.
These changes led to a significant increase in telehealth visits early in the pandemic. According to CMS, virtual ambulatory visits jumped from 13,000 per week before the pandemic to nearly 1.7 million per week in April 2020, with over 9 million beneficiaries using telehealth through June 2020 (Verma, 2020). However, as COVID-19 cases declined, states reopened their economies and healthcare providers resumed in-person visits. Consequently, telehealth visits decreased but stayed higher than prepandemic levels, raising questions about the future of telehealth postpandemic. Surveys indicate that patients are satisfied with telehealth visits and many are willing to continue virtual appointments (Accenture, 2020). However, healthcare providers may reduce telehealth services if prepandemic restrictions are reinstated. Policymakers are currently debating telehealth provisions (Schatz et al., 2023).
Overall, the evidence suggests that telehealth is here to stay and that virtual visits will continue to play a significant role in ambulatory care. However, fundamental questions remain regarding the best ways to use this relatively new mode of care delivery. There is still limited knowledge about the impact of telehealth on patient and provider outcomes and clinic operations.
In this study, we address this gap by exploring the impact of telehealth on an important operational outcome: Patient adherence to medical appointments. We focus on two behaviors that result in nonadherence: (a) No-shows (not showing up without notice) and (b) unpunctuality (showing up late). Both behaviors contribute significantly to inefficiency in the healthcare industry, negatively affecting patient outcomes, provider productivity, and clinic operations (Gupta and Denton, 2008). Gier (2017) estimates that patient no-shows alone cost the US healthcare system $150 billion annually. Some medical providers perceive unpunctuality even more disruptive than no-shows (Martin et al., 2005).
Does telehealth reduce patient no-shows and improve punctuality, thereby improving adherence to medical appointments? Research has identified transportation issues, competing priorities, inconvenience, and health and safety concerns as primary drivers of patient no-shows and unpunctuality in in-person appointments. Telehealth mitigates these concerns by allowing patients to visit their providers remotely. Therefore, we hypothesize that telehealth decreases patient no-shows and unpunctuality.
To test our hypotheses, we partnered with a major university-affiliated medical system operating dozens of outpatient facilities in Florida. In 2020, the medical system substantially increased its telehealth capabilities due to the COVID-19 pandemic. We analyze a large dataset including 412,415 in-person and telehealth appointments from 129,256 patients across multiple specialties between 2020 and 2022. We use an instrumental variable (IV) approach to estimate the impact of telehealth on patient no-shows and punctuality, while controlling for a wide range of patient and appointment characteristics and environmental factors.
The key findings and conclusions from our empirical analyses are summarized below:
Our empirical analyses highlight the benefits of telehealth in improving patient adherence to scheduled appointments and enhancing provider productivity. To translate these insights into actionable strategies for clinics, we investigate how telehealth can be integrated into optimized scheduling practices. Specifically, we use discrete stochastic optimization methods to explore the optimal sequencing of telehealth and in-person appointments within a clinical workday. We extend the scheduling model developed by Zacharias and Yunes (2020) to accommodate heterogeneous appointment types—telehealth versus in-person, and new patient versus follow-up visits—while accounting for no-shows, unpunctuality, and general stochastic consultation times. Our computational analysis reveals that heterogeneity in patient no-shows and punctuality across appointment types significantly impacts operational performance. Notably, scheduling telehealth appointments before in-person visits leads to greater clinic efficiency compared to the reverse sequence.
Our findings carry important policy and managerial implications. While telehealth’s potential to improve access is often highlighted in the context of rural patients who lack in-person care options, our results show that it also improves access by increasing appointment adherence, even in large metropolitan areas. These gains are especially pronounced among groups with historically lower adherence rates. Policymakers should account for these benefits when shaping telehealth regulations and reimbursement models. For healthcare organizations, telehealth provides a practical and effective tool to reduce appointment nonadherence by lowering logistical and structural barriers to attendance, while also enhancing provider productivity, particularly for follow-up care. We elaborate on the implications of our findings in Section 8.
Literature Review
Our study bridges two bodies of literature: (1) Research on telehealth and its effects on operational performance, and (2) studies on patient nonadherence to medical appointments. First, we review existing research in each area. Next, we explore where these fields intersect, identify gaps, and describe our contributions.
Another stream of this literature explores the impacts of telehealth services on provider and patient outcomes. Bavafa and Terwiesch (2019) find that the introduction of online messaging in an American healthcare system increased physicians’ working hours. Sun et al. (2020) find that the availability of telemedicine in New York State hospitals reduced average patient length of stay without compromising care or cost. Li et al. (2021) find that the introduction of telehealth services prompted mental health providers to schedule follow-up visits more closely initially, leading to increased patient throughput but later resulting in heavier workloads and longer visit intervals.
There are also studies that investigate the design and impacts of telehealth services using analytical modeling. They address topics such as the impact of e-visits on patient health and physician capacity and compensation (Bavafa et al., 2021; Zhong et al., 2018), the effects of telemedicine on patient utility, provider productivity, and social welfare in chronic care (Rajan et al., 2019), the design of on-demand telemedicine platforms integrating general and specialty care (Savin et al., 2021), the impact of telemedicine on health disparities among socioeconomic groups (Sunar and Staats, 2022), and telehealth pay parity and patient access in acute care (Çakıcı and Mills, 2025).
Another stream of research focuses on strategies to improve patient appointment adherence, including overbooking, rescheduling, reminders, and financial penalties (Selim et al., 2023). Liu et al. (2019) find accommodating rescheduling requests from patients reduces no-shows, particularly among follow-up appointments. Li et al. (2019) develop a Bayesian nested logit model that considers patients’ responses to appointment reminders and other variables to predict no-shows. Liu and Kc (2023) find that including wait time information in appointment reminder texts significantly reduces no-show rates. Williams et al. (2014) find that that withholding care for unpunctual patients effectively improves their punctuality.
There is also extensive literature on optimizing patient flow management, focusing on addressing variability in patient arrivals (such as no-shows and unpunctuality) in scheduling practices (see Cayirli and Veral, 2003 and Ahmadi-Javid et al., 2017 for surveys of such models). They address topics such as determining patient base size, daily capacity levels, and appointment window choices (Green and Savin, 2008; Liu, 2016; Zacharias and Armony, 2017), optimizing intraday scheduling templates (Wang et al., 2020; Zacharias and Yunes, 2020), and managing dynamic appointment scheduling systems under uncertainty (Feldman et al., 2014; Zacharias et al., 2024).
Adepoju et al. (2022) conduct one of the few studies that control for observable patient characteristics, including demographics and medical history. They find that telehealth is associated with reduced odds of missed appointments, particularly among patients with frequent prior visits and those seeking mental health services. Additionally, Qin et al. (2024) explore how socio-demographic factors impact no-show rates in in-person and telehealth appointments differently. They report that Medicaid status, Black ethnicity, and younger age are stronger predictors of no-shows for in-person appointments compared to telehealth, suggesting that telehealth may mitigate access disparities. Finally, Qin et al. (2025) examine how physician availability affects service completion rates for in-person versus telehealth appointments. They find that delayed care initiation leads to higher rates of service incompletion for telehealth appointments, primarily due to patients leaving before being seen, whereas in-person appointments are unaffected by such delays.
We extend the scope of previous studies by utilizing data from 27 facilities and multiple medical specialties between 2020 and 2022. This extended timeline captures both the pandemic’s initial disruptions and the postpandemic context. Throughout this period, telehealth evolved from a temporary substitute for in-person care to a potentially permanent mode of healthcare delivery (Mikie, 2021). Our extensive dataset enables us to control for a wide range of observable patient and appointment characteristics. Leveraging our granular data, we propose an identification strategy to mitigate potential unobservable confounding factors, thereby strengthening evidence for a causal relationship between telehealth and appointment adherence. We explore how the impacts of telehealth on appointment adherence vary across different appointment types and patient demographics to identify scenarios where telehealth is most effective. Our findings indicate that telehealth significantly enhances adherence for follow-up appointments compared to initial visits. Additionally, patients with historically lower rate of adherence to in-person appointments—women, racial minorities, Medicaid patients, and younger adults—demonstrate the greatest improvement in adherence through telehealth, underscoring telehealth’s potential to mitigate access disparities. Our study offers one of the first empirical analyses of telehealth’s impact on patient punctuality. This often-overlooked outcome in the operations literature has significant implications for clinic efficiency as demonstrated in Section 7. We also explore how telehealth affects patient revisit rates to provide a comprehensive view of its impact on provider productivity. Our findings suggest that while telehealth appointments may prompt earlier patient revisits and additional workload, the reduction in no-shows, especially for follow-up visits, offsets these factors, indicating improved provider productivity through telehealth. We draw on recent advances in stochastic intraday scheduling to examine how telehealth capacity can be effectively integrated into optimized scheduling. Specifically, we extend the scheduling model proposed by Zacharias and Yunes (2020) to account for heterogeneity by appointment modality and types to identify the optimal sequence of these appointment types to enhance clinic efficiency.
Hypotheses Development
Studies have identified five main reasons for patients’ appointments nonadherence: (1) Forgetfulness, (2) transportation challenges, (3) schedule conflicts, (4) inconvenience, and (5) safety and stigma concerns.
First, patients may miss their appointments or arrive late simply because they forget the appointment time (Campbell et al., 2000). Second, patients may face transportation problems (Samuels et al., 2015). For example, according to the American Public Transportation Association, 45% of Americans have no access to public transportation (APTA, 2019). The lack of transportation options creates significant barriers for people who require regular medical care but cannot find practical ways to get to their appointments. Third, competing commitments and obligations often clash with scheduled appointments (Martin et al., 2005). For example, parents may struggle to find alternative childcare, and employees may not be able to obtain time off work (Campbell et al., 2000; Samuels et al., 2015). Fourth, to complete an in-person appointment, patients must navigate various stages, from traveling to and from the clinic to completing paperwork and waiting in the clinic. The actual time spent with the healthcare provider is often disproportionately short compared to the overall time spent in the process. This can discourage some individuals from adhering to their appointments (Anderson et al., 2007), especially healthier patients with less urgent needs (Chu et al., 2019). Lastly, concerns about health risks and societal judgments contribute to appointment nonadherence. Factors such as bad weather conditions, heavy traffic, the potential for contracting contagious illnesses like COVID-19, or fears of being stigmatized for seeking specific types of care can deter patients from fully adhering to their appointments (Henderson et al., 2013).
The two most common tactics used by clinics to address patient appointment nonadherence are overbooking and appointment reminders (Selim et al., 2023). Overbooking tackles the problem at the clinic level but does not address the underlying issues mentioned earlier. In contrast, appointment reminders are effective in mitigating patient forgetfulness (Liu and Kc, 2023). However, these reminders do not address challenges related to transportation, scheduling conflicts, inconvenience, and safety or stigma. Selim et al. (2023) underscore the need to explore digital solutions that address these barriers. One such solution is conducting appointments through telehealth.
Telehealth reshapes patient-doctor interactions by facilitating remote consultations from the comfort of one’s home or workplace, effectively mitigating the underlying factors contributing to appointment nonadherence. First, for telehealth appointments, patients only need an electronic device, cellular or internet connectivity, and a secure setting. Surveys by Pew Research Center indicate that 97% of American adults have phones, 85% own smartphones, 77% have computers, 93% can access the internet, and 77% enjoy high-speed broadband at home (Pew Research Center, 2021a, 2021b). By reducing travel burdens, telehealth allows patients with transportation problems to better adhere to their appointments. Second, patients with competing commitments—such as parents caring for children or employees unable to secure time off—can engage in telehealth appointments without leaving their caregiving duties or workplace behind. Third, telehealth appointments are much more convenient than in-person appointments. Patients can check in online, complete assessment forms through their electronic devices, wait within their personal spaces, and directly consult with their providers. This increased convenience may improve appointment adherence, particularly among healthier patients who might view in-person appointments as less worthwhile. In addition, this increased convenience enhances the ability of patients with disabilities or physical restrictions to attend appointments. Lastly, the elimination of the need to travel and interact in public spaces creates a safer environment for patients to access care, thereby addressing safety and stigma concerns.
Overall, telehealth reshapes healthcare delivery, alleviating obstacles linked to travel, conflicting commitments, inconvenience, and safety and stigma. Hence, we hypothesize that it can reduce no-shows and improve patient punctuality, thus improving adherence to medical appointments.
Hypothesis 1: Telehealth appointments reduce no-shows and enhance punctuality, thereby improving patient adherence to medical appointments.
Next, we explore how telehealth affects appointment adherence across various appointment types to identify those that may benefit more from telehealth. Specifically, we compare appointments for new patients with follow-up appointments. New patients typically visit the provider for the first time, often presenting new and pressing conditions that require timely intervention or consultation (Liu et al., 2019). In addition, they may be navigating the system for the first time and are motivated to establish trust with their healthcare provider (Kajaria-Montag et al., 2024). In contrast, patients attending follow-up appointments typically have less urgent needs and are often engaged in ongoing care plans, returning to the provider for monitoring or treatment adjustments (Liu et al., 2019). Moreover, they are familiar with the system and have an established relationship with the provider. Therefore, while new patients prioritize timely access to care and trust-building (Osadchiy and Kc, 2017), those with follow-up appointments often prioritize convenience (Liu et al., 2019). Reflecting this distinction, Liu et al. (2019) find that new patients seek quicker access and shorter wait times, whereas patients with follow-up appointments value more flexibility in scheduling.
Telehealth appointments offer greater convenience than in-person visits, which is especially advantageous for follow-up appointments where patients prioritize ease and efficiency. Conversely, new patients, driven by urgent care needs and the desire to build trust, may attend their appointments regardless of the modality. Therefore, telehealth may more effectively reduce no-shows in follow-up appointments. However, the convenience of attending the appointment from one’s personal space should improve punctuality for both patients groups. We formalize these hypotheses below:
Hypothesis 1: Telehealth appointments reduce no-shows more significantly for follow-up appointments than for new patient appointments, while also improving patient punctuality across both appointment types.
Lastly, we investigate how telehealth affects appointment adherence across various demographic groups to determine patient types that benefit the most from remote consultations. Research has found that women, racial minorities, Medicaid patients, and younger adults tend to have lower odds of appointment adherence than others (Campbell et al., 2000; Dantas et al., 2018; Qin et al., 2024; Samuels et al., 2015). We observe similar patterns in our data. Across the in-person appointments, the no-show and late-arrival rates are: 1.4 and 2.8 percentage points (pps) higher among women than men, 5.3 and 4.5 pps higher among racial minorities than Whites, 12.5 and 1.5 pps higher among Medicaid patients than those with other insurances, and 6.3 and 11.4 higher among patients under 50 years old than older ones.
The literature provides several explanations for these disparities: (1) Women are more likely than men to face competing priorities with respect to childcare and household duties (Campbell et al., 2000); (2) racial minority and Medicaid patients tend to have a lower socioeconomic status and more limited access to resources such as transportation or paid time off (Lowes, 2005); and (3) younger adults are generally healthier and face fewer health repercussions if they miss their appointments (Dantas et al., 2018). Since telehealth mitigates issues related to competing priorities, transportation, and the inconvenience of attending appointments, we hypothesize that it has a stronger effect on the no-show and punctuality outcomes of these underserved groups, thereby reducing disparities in accessing care.
Hypothesis 3: Telehealth is more effective in reducing no-shows and improving punctuality among demographic groups with historically lower adherence to in-person appointments—women, racial minorities, Medicaid patients, and younger adults—thereby reducing disparities in access to care.
Data and Variable Definitions
Data Description
To test our hypotheses, we partner with a large university-affiliated medical system with more than 1,200 physicians and scientists providing care across dozens of outpatient sites and several hospitals in the state of Florida. The medical system significantly expanded its telehealth capacity in 2020 in response to the COVID-19 pandemic. We access 974,269 appointment-level records across 27 outpatient facilities. This includes all appointments for adult patients in three departments, General Medicine, Neurology, and Dermatology, from January 2019 through December 2022. All appointments were scheduled in advance (no walk-in appointments). Each record includes some information about the patient (gender, race, age, and insurance type), the appointment (status, type, modality, scheduled length and time, location), the medical provider who saw the patient, and several timestamps including the patient’s check-in time.
We selected general medicine, neurology, and dermatology after consulting our healthcare partner, who believes these specialties are well-suited for telehealth. General medicine covers primary care, neurology deals with nervous system disorders, and dermatology addresses skin disorders. Recent technological advances have enabled remote diagnosis and treatment for many conditions in these fields. The differences in these specialties further allow us to study the effect of telehealth across various patient types and service capacities. In Appendix EC.1.1, we explore the heterogeneous effects of telehealth across these specialties.
Data Selection
We conduct the following data selection process. First, our partner medical system began to offer telehealth appointments in 2020. Thus, we only focus on the appointments that took place in the year 2020, 2021, and 2022. We use the 2019 data to create a proxy variable for the patients’ condition based on the volume of their past visits. Second, the status of each appointment is labeled as “completed” (57%), “no-show” (8%), or “canceled” (35%). We focus only on completed and no-show appointments and exclude canceled appointments for several reasons. First, in this health system, patients receive appointment reminders 7, 3, and 1 day before the appointment (if they have not responded to previous reminders). According to health system practitioners, cancelations are less of a concern than no-shows because patients often cancel in advance electronically, allowing the system to update and enabling schedulers to fill vacated slots with patients on the waiting list. Second, including cancelations would introduce a separate behavioral dimension, conflating appointment adherence with proactive rescheduling decisions. Cancelations may also be influenced by external factors, such as provider availability, rather than a patient’s intent to attend their appointment. Finally, our data does not capture the reasons for cancelations or whether these appointments were rescheduled. Given these considerations, excluding cancelations is a standard approach in studies of appointment adherence (e.g., Liu et al. (2019)). Second, the type of each appointment is labeled as “new patient” (23.0%), “follow-up” (66.7%), “procedure” (10.1%), “study” (0.1%), or “others” (0.1%). There are no telehealth records for the last three types of appointments, which require a physical examination or a procedure that can only be carried out in-person. As such, we only include appointments with new patient and follow-up types. Finally, to remove the effect of outliers, we only include appointments for providers that had at least one in-person and one telehealth appointment between 2020 through 2022 (96.2%). Our final sample includes 412,415 appointments involving 129,256 patients and 176 medical providers.
Variable Definition and Summary Statistics
Second, we control for the type of appointment (
Third, since our data collection partially overlap with the COVID-19 pandemic, we control for several pandemic-related variables to mitigate its effects on patient outcomes. Specifically, we control for the per-capita number of reported COVID-19 cases, deaths, and hospital admissions in the county during the week of appointment
We also control for provider heterogeneity by creating a dummy variable (
Besides these factors, patients’ health conditions can also influence both appointment choice and adherence outcomes. Since we lack direct measures of health status, we construct several proxies to approximate their care intensity. First, following Adepoju et al. (2022), we use the number of visits in the past 12 months (
Model and Identification Strategy
An ideal experiment to test our hypotheses would involve randomly assigning patients to telehealth and in-person appointments and comparing their outcomes. However, this is not practical due to ethical and operational issues. Instead, we use observational data. We begin by developing an econometric model to analyze the impacts of telehealth on patient outcomes and then discuss potential econometric challenges and our identification strategy.
Econometric Model
Our dependent variables are

The synchronous form of telehealth was not used in our partner medical system before the COVID-19 pandemic. The first case of COVID-19 in Florida was reported on March 1, 2020. Florida Governor Ron DeSantis declared a public health emergency on March 9 and issued an executive order limiting all nonessential activities on April 1 (DeSantis, 2020b). At the end of April, the governor instituted a three-phase recovery plan, which was completed on September 25 when he nullified all COVID-19 public health measures (DeSantis, 2020a). In Appendix EC.1.3, we detail the timeline of the pandemic policies in Florida and rerun our main analyses across different time periods.
Figure 1 displays the number of telehealth and in-person appointments during each month of 2020, 2021, and 2022 in our data. Observe how the composition of the appointments changed in response to the pandemic-related policies. Our partner healthcare system introduced telehealth appointments in mid-March 2020. By April and May, the majority of appointments were conducted via telehealth. In subsequent months, telehealth remained an option for all patients. New patients were able to select the modality of their appointments and a range of available dates. A scheduler would then confirm both the date and modality. For follow-up appointments, the provider recommended an approximate time (e.g., 4 weeks) and assessed whether telehealth was a suitable modality, after which the patient communicated the exact time and chosen modality to the scheduler. While our analysis includes a comprehensive set of controls to account for factors influencing patients’ decisions, unobservable variables may still affect their choices. Some of these unobserved factors could also be correlated with no-show and punctuality outcomes, potentially introducing bias into our estimations. For example, patients with severe illnesses, such as autoimmune disorders, and those who live far from clinics may prefer telehealth to reduce COVID-19 exposure or travel burden, respectively. Thus, patients’ condition severity and distance to clinic may be positively correlated with
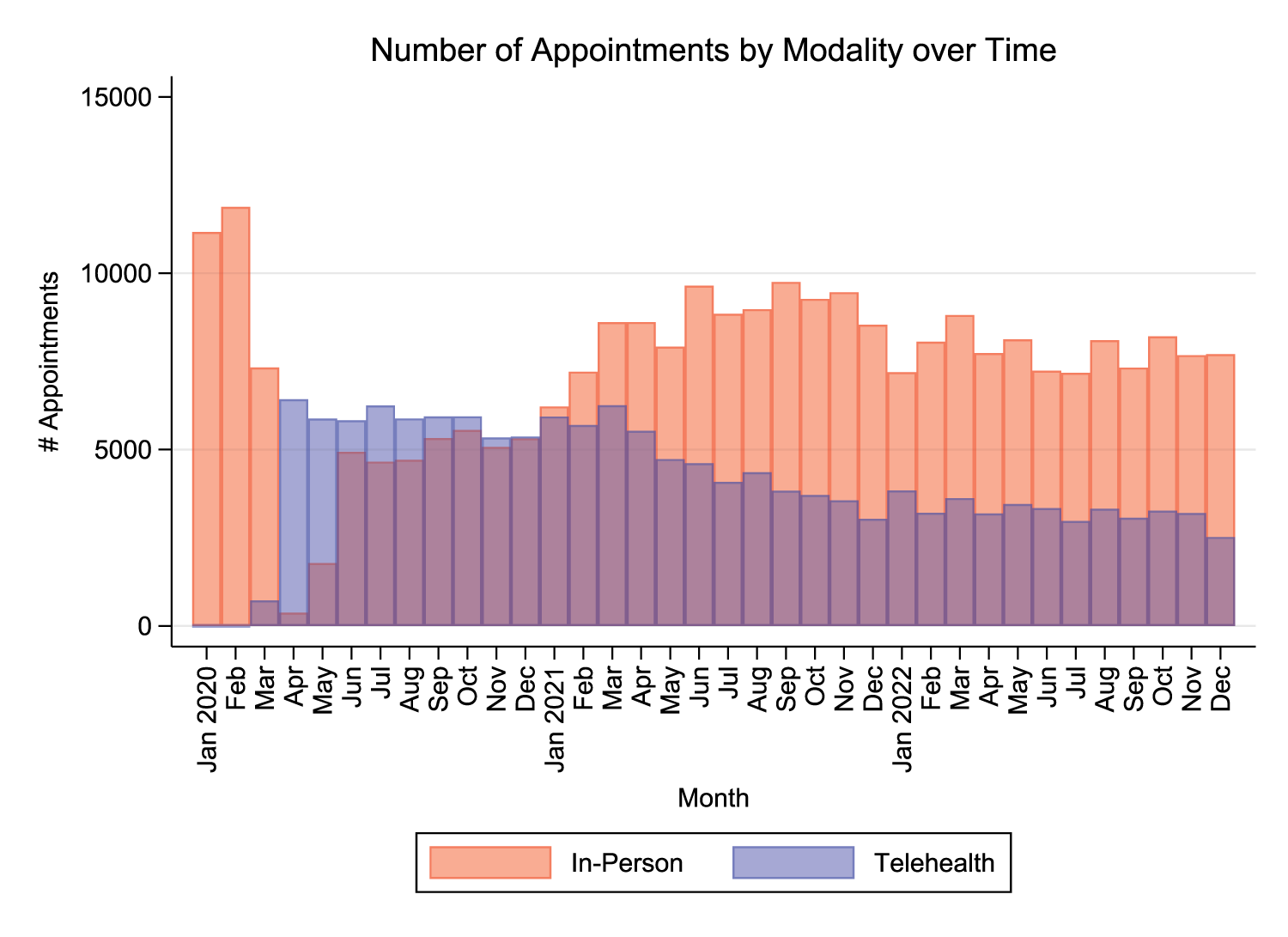
Number of appointments over months (the transparent bars for in-person (red) and telehealth (blue) visits overlap).
Now, consider the no-show outcome. Patients with more severe illnesses tend to prioritize attending appointments to prevent their condition from worsening. This may lead to a negative correlation between a patient’s health condition and
Next, consider the punctuality outcome. Although a patient’s condition may not consistently influence their punctuality, greater distances to the clinic are frequently cited as a significant factor contributing to lateness (Alibeiki et al., 2022). Consequently, distance to the clinic may be positively correlated with both
Given that our dependent variables (
We formulate the patients’ choice of modality using a probit model as follows:

While the inclusion of an IV is not required to get consistent estimates, it is recommended that we identify at least one IV that affects the propensity that an appointment is telehealth (relevance criteria) but does not affect the patient’s no-show and punctuality outcomes (exclusion criteria) (Wooldridge, 2010). We leverage the medical providers’ daily capacities and schedules to construct an IV. First, we calculate the number of appointments scheduled by the provider in appointment
Although it is not possible to statistically validate the exclusion restriction directly, there are compelling conceptual reasons to believe our instrument satisfies this criterion. The 7-day rolling percentage of telehealth visits reflects provider-level scheduling patterns, which are unlikely to directly affect an individual patient’s no-show or punctuality outcomes on the focal day. These outcomes are primarily driven by the patient’s own choices and behaviors, which are independent of the broader composition of their provider’s appointments. Patients are unlikely to have knowledge of their provider’s overall schedule or the modalities of other appointments during the preceding week. That said, there could be indirect links between providers’ scheduling practices and patient adherence. For instance, if some providers schedule telehealth visits on specific hours or weekdays associated with higher no-show or punctuality issues, this could introduce a potential relationship. To address such possibilities, we include a robust set of controls that capture key factors related to provider schedules. First, we include physician fixed effects, which account for all time-invariant provider characteristics, such as their scheduling preferences or technological tendencies. Second, we control for hour-of-day and day-of-week fixed effects to account for systematic differences in appointment modalities and patient outcomes across hours and weekdays. Third, we control for the providers’ proportion of follow-up appointments on the focal day to control for patterns in appointment types that may be correlated with telehealth usage and patient nonadherence. With these controls, the instrument’s effect on appointment adherence should operate solely through its impact on the modality of the focal visit.
To account for the endogeneity of
Results of the estimation and average marginal effect (AME) of (1) for
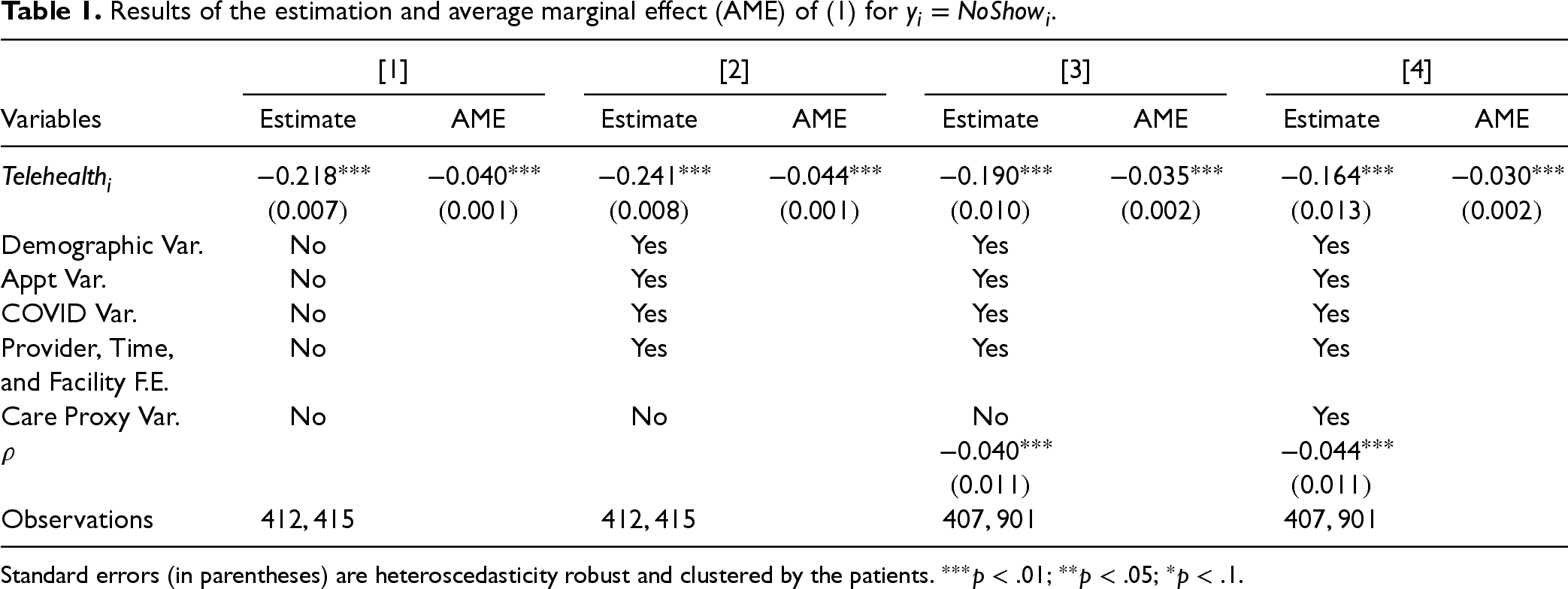
Standard errors (in parentheses) are heteroscedasticity robust and clustered by the patients.
In Section 6, we conduct additional analyses to test the robustness of our approach. First, we explore several alternative IVs to demonstrate the robustness of our findings to IV selection. Second, we incorporate patient fixed effects to control for unobservable, time-invariant patient characteristics. We also use a linear probability model to confirm that our results are robust across different model specifications. Third, we use propensity score matching to minimize differences between the patients using telehealth versus in-person appointments. We then run regressions on the matched sample, both with and without patient fixed effects and endogeneity adjustments. Fourth, we conduct placebo tests by randomly assigning modalities to appointments. Lastly, we propose an alternative identification strategy using a difference-in-differences framework, leveraging variations in telehealth adoption rates across physicians. Across all these robustness checks, our findings remain consistent with the main results presented in the following section.
In Section 5.1, we present the main results on the effect of telehealth on patient no-show and punctuality outcomes. In Section 5.2, we study how these effects vary between new patients and follow-up appointments. In Section 5.3, we explore how patient socio-demographic factors moderate the effects of telehealth on appointment adherence. In Section 5.4, we examine the impact of telehealth on patients’ revisit rate, to explore the productivity implications of telehealth for medical providers.
Main Results
Table 1 reports the estimation results of model (1) for
Column [1] reports the results of the probit regression of (1) in the absence of control variables and endogeneity adjustment. The
Table 2 reports the estimation results of model (1) for
Results of the estimation and average marginal effect (AME) of (1) for
.
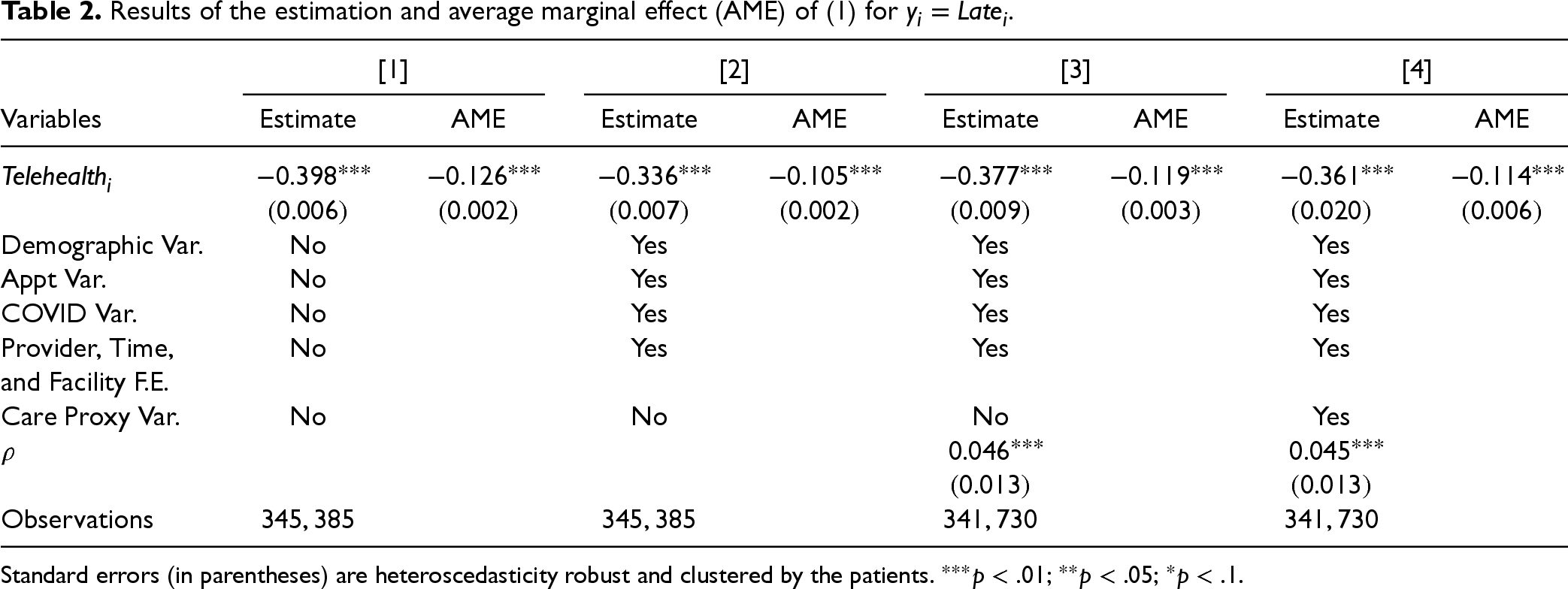
Results of the estimation and average marginal effect (AME) of (1) for
Standard errors (in parentheses) are heteroscedasticity robust and clustered by the patients.
Overall, our analyses suggest that telehealth appointments reduce the no-show and late-arrival rates, thereby improving patient adherence to medical appointments.
In this section, we explore how the effects of telehealth on patient no-show and punctuality outcomes vary between appointments for new patients and follow-up appointments. We hypothesized that telehealth is more effective in reducing no-shows for follow-up appointments where patients have stronger preference for convenience, while it enhances punctuality across both appointment types.
To test this hypothesis, we add an interaction term between the
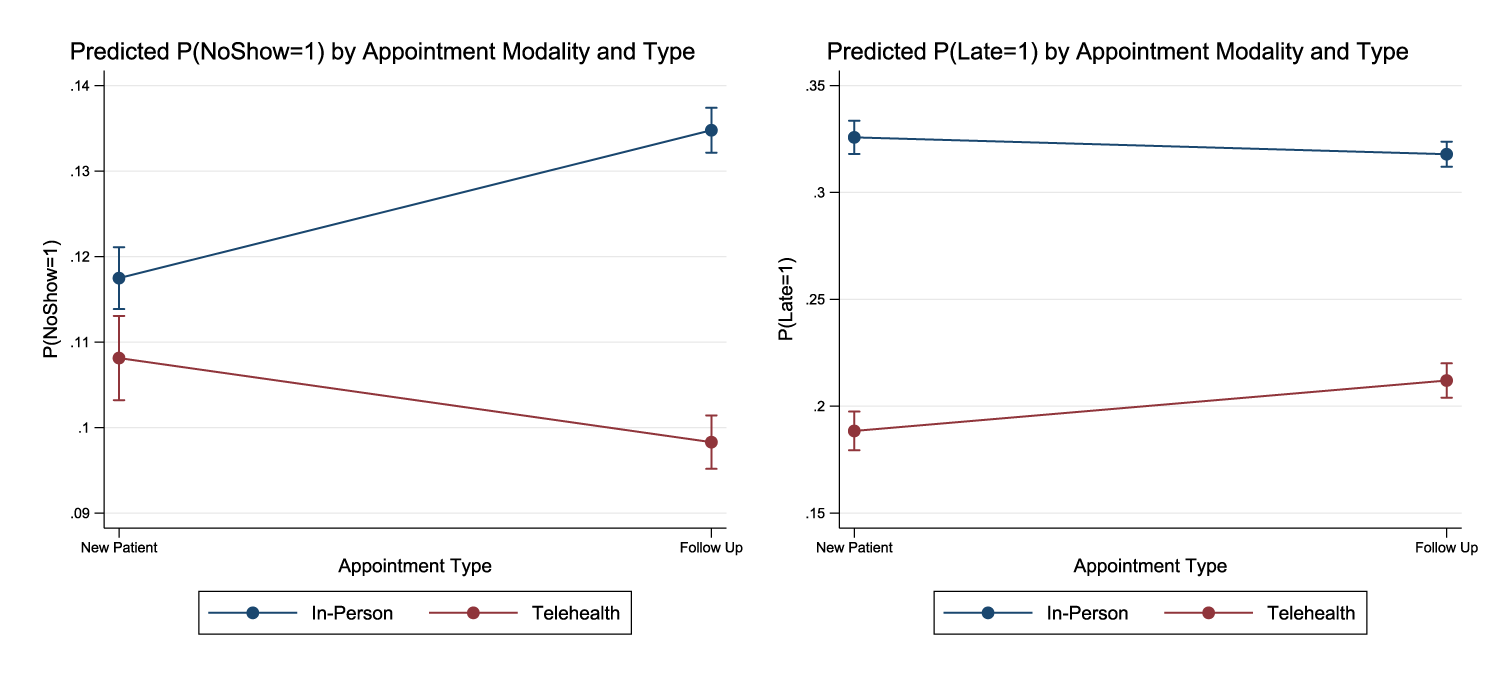
Predicted no-show and late-arrival probabilities with 95% confidence intervals by appointment modality and type.
The moderating effect of
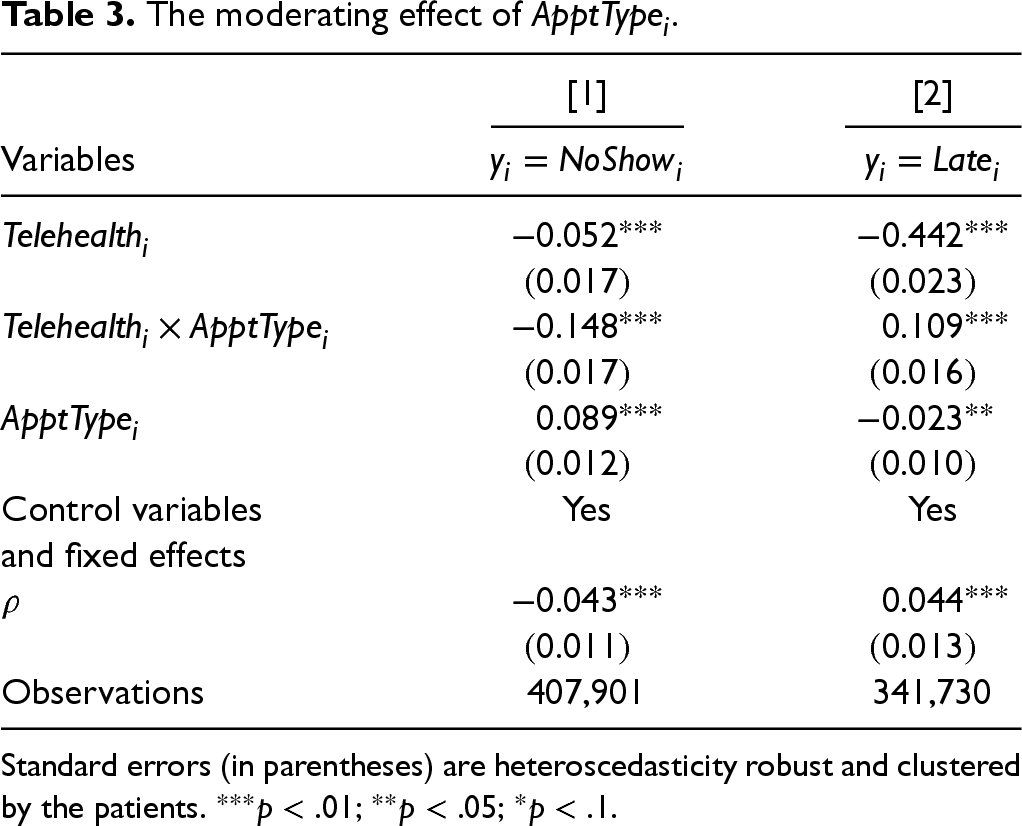
Standard errors (in parentheses) are heteroscedasticity robust and clustered by the patients.
Overall, our findings support Hypothesis 2, suggesting that telehealth is particularly effective in improving adherence to follow-up appointments, where patients may have a stronger preference for convenience due to their less acute needs. Additionally, while the reduction in no-shows for new patients is less significant, there is still a sizable improvement in patient punctuality. These findings highlight the telehealth’s potential to streamline clinic operations across various appointment types.
In this section, we explore the effect of telehealth on patient no-show and punctuality outcomes across patients from different socio-demographic groups. We hypothesized that patients with the lowest rates of adherence to in-person appointments—women, racial minorities, Medicaid patients, and younger adults—show the greatest improvements in adherence through telehealth.
To test our hypotheses, we introduce interaction terms between the the no-show and late-arrival probabilities decrease more for women (by 3.7 pps and 12.3 pps) than for men (by 1.6 pps and 9.8 pps), the no-show probability decreases more for Blacks (by 4.3 pps) and other non-Asian minorities (by 8.2 pps) than for Whites (by 2.6 pps), the no-show probability decreases more for Medicaid patients (by 7.2 pps) than for Medicare patients (by 0.5 pps) and those with commercial insurance (by 3.2 pps). The late-arrival probability decreases substantially more for patients with commercial insurance, who are more likely to be employed and experience schedule conflicts when attempting to attend their appointments on time, the no-show and late-arrival probabilities decrease significantly more among the younger adults.
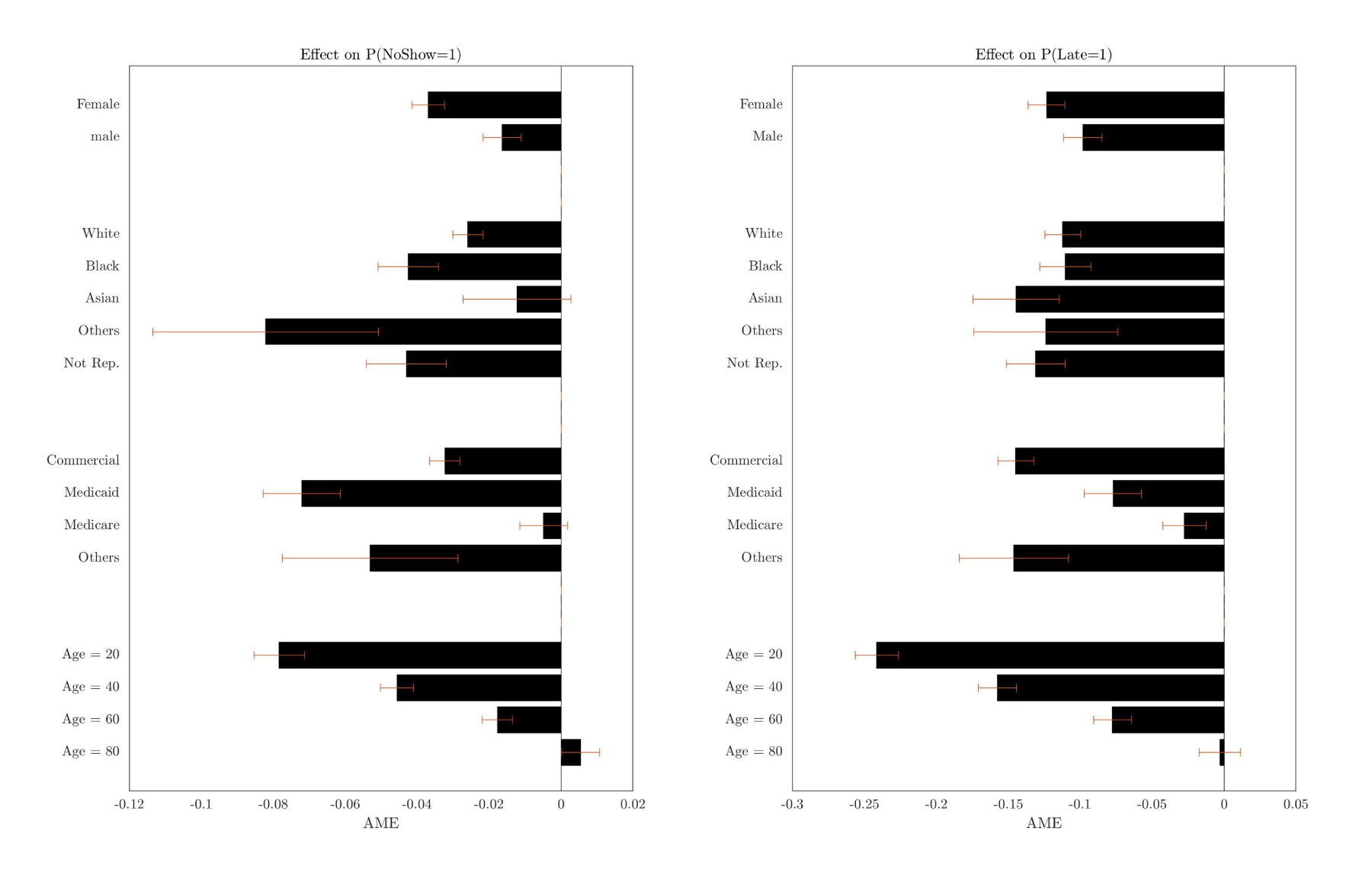
Average marginal effect of telehealth on the no-show and late-arrival probabilities with 95% confidence intervals.
These results suggest that telehealth can help reduce disparities in appointment adherence by addressing barriers faced by patients who struggle with in-person visits. However, for these improvements to translate into broader reductions in access disparities, telehealth should be used consistently across different patient groups. The estimation results for the first stage of our bivariate probit model, presented in Appendix EC.3, reveal small differences in telehealth usage by gender, race, and insurance status. Women are 1.5 pps more likely than men to use telehealth, minority patients are 0.3 pps more likely than White patients, and Medicaid patients are 1.0 pps more likely to use telehealth. The most notable difference is by age, with patients under 40 being 3.6 pps more likely to use telehealth compared to older patients. Overall, these findings reinforce the conclusion that telehealth helps reduce access disparities by significantly improving appointment adherence among groups with historically lower adherence rates.
Our analyses show that telehealth significantly improves appointment adherence, which in turn can help healthcare providers boost throughput and productivity. However, these benefits are contingent on telehealth being at least as effective in diagnosis and treatment as in-person visits. The literature is mixed on this point: Some studies suggest telehealth cannot fully replace in-person visits (e.g., Lekwijit et al., 2023), while others indicate it may be comparably effective in specific contexts (Ayabakan et al., 2024).
To draw meaningful conclusions about the benefits of telehealth in improving provider productivity, we examine its effect on patients’ revisit intervals with the same provider—a common metric for assessing quality and productivity (Kajaria-Montag et al., 2024). If telehealth appointments are as effective as in-person visits, we would expect no significant difference in revisit intervals. Conversely, a shorter revisit interval may indicate that patents’ concerns were not fully addressed during telehealth appointments.
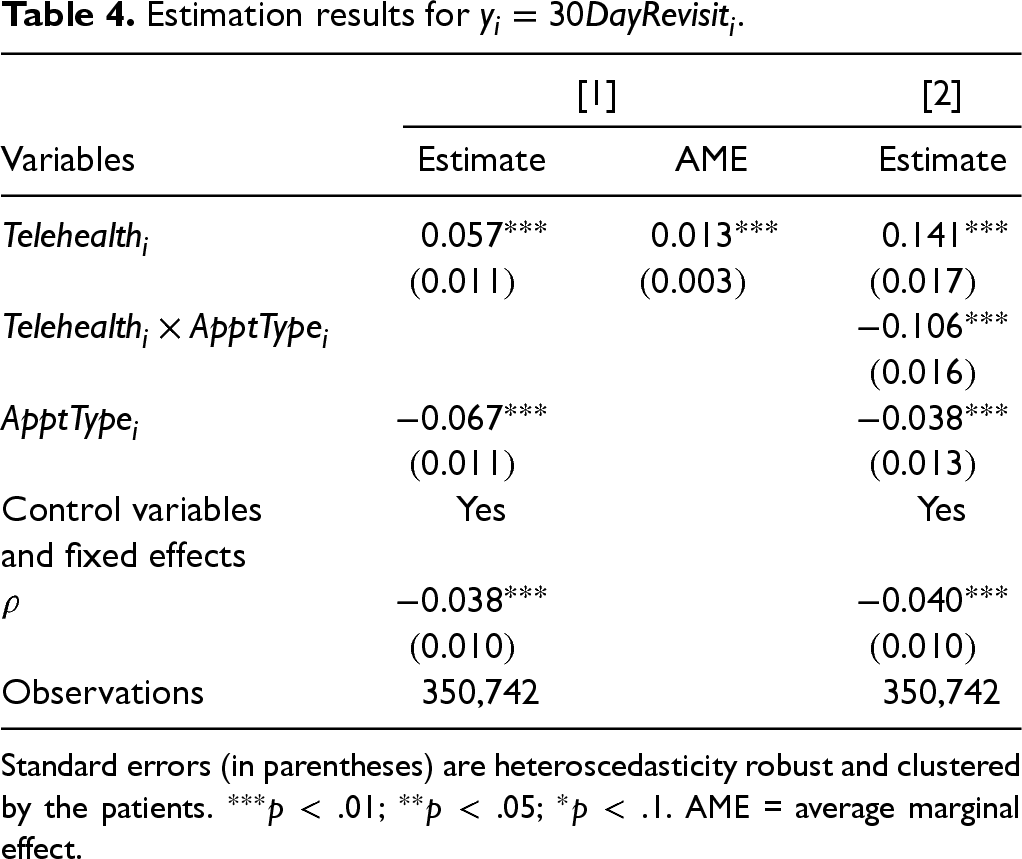
Let
Column [1] in Table 4 presents the estimation results. The AME is 0.013, indicating a 1.3 pps higher 30-day revisit probability for telehealth appointments compared to in-person appointments (19.3% versus 18.0%, a 7.2% increase). These findings suggest that telehealth appointments may not be perfect substitutes for in-person appointments. However, the magnitude of this effect is considerably smaller than the 3.0 pps reduction in the no-show probability, implying a net gain in provider productivity with telehealth.
Estimation results for
.
Estimation results for
Standard errors (in parentheses) are heteroscedasticity robust and clustered by the patients.
In column [2], we examine the moderating effect of appointment types. Figure 4 illustrates the predicted 30-day revisit probability by appointment modality and type. We observe a 3.6 pps increase in revisit probability for new patients (22.1% versus 18.5%, a 19.5% increase) and a 0.8 pps increase for follow-up appointments (18.5% versus 17.7%, a 4.5% increase). When comparing these results with our earlier findings—a 0.9 pps reduction in no-shows for new patients and a 3.7 pps reduction for follow-ups—telehealth emerges as an effective substitute only for follow-up appointments. In contrast, conducting initial consultations via telehealth may lead to additional workload for providers.
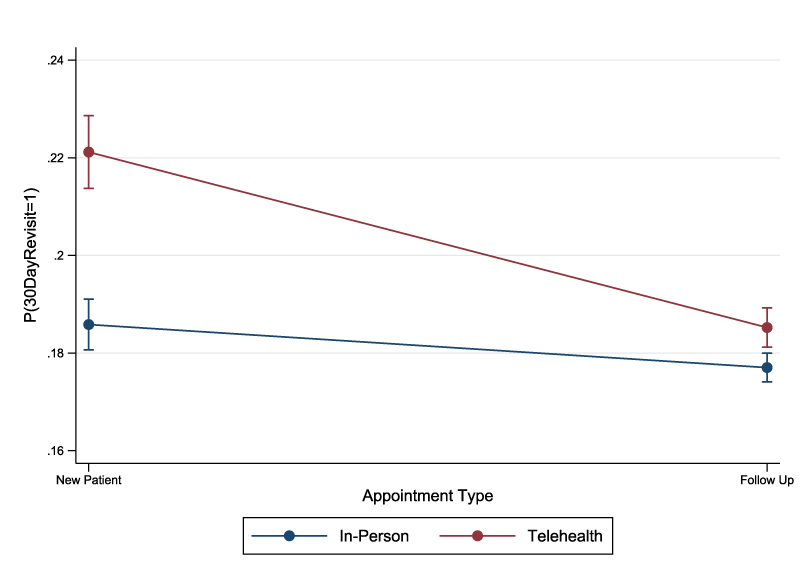
Predicted 30-day revisit probability with 95% confidence intervals by appointment modality and type.
In this section, we discuss several robustness analyses. We present the full results in Appendix EC.5.
Implications of Telehealth on Appointment Scheduling Practices
Our empirical analysis suggests that telehealth is particularly effective in improving adherence to follow-up appointments, but may be less suitable for initial consultations with new patients. To translate these findings into actionable insights for clinics, this section explores strategies for integrating telehealth into optimized scheduling practices. Specifically, we examine the optimal sequencing of follow-up telehealth visits and in-person appointments (for both follow-up and new patients) within a day.
The goal is to determine the optimal timing and sequence of appointments to balance two competing objectives: Efficient use of provider time and shorter patient wait times. These goals often conflict due to variability in arrivals and consultation durations (Zacharias and Yunes, 2020). We address this trade-off using a weighted penalty function that captures the relative importance of different scheduling outcomes. Below, we provide a summary of the model, which accounts for stochastic factors such as no-shows, unpunctuality, and general stochastic consultation times. See Appendix EC.6 for the detailed model.
The regular length of a workday is
We extend the methodology proposed in Zacharias and Yunes (2020) to approximate heuristically the problem with heterogeneous patients, and we assess the performance of different sequencing rules. In particular, we perform a two-step approach. In the first step, we assume that all three appointment types share a homogeneous no-show probability, and that they check in on time when they show up. Under these assumptions, Algorithm 2 in Zacharias and Yunes (2020) terminates in polynomial time with an optimal aggregate schedule. In the second step, we account for heterogeneous show-up and on-time probabilities, and we assess the performance of different sequencing rules applied on the scheduling template from the first step.
A fraction A fraction By solving 8 Linear Programs (4 for each
The aggregate schedule that heuristically solves the corresponding homogeneous problem with no-show probability 
For the second step in our two-step approach, we construct four scheduling templates based on different sequencing rules. We consider sequencing rules such that the provider has to switch delivery method between in-person and telehealth only once during the day, to avoid potential “switching costs.” This constraint reflects a realistic operational consideration: Switching between in-person and telehealth modes often involves logistical or cognitive costs, such as relocating to a different setting, changing workflows, or adjusting communication styles. By limiting mode-switching to once per day, we model a more practical and manageable scheduling structure for providers, aligning the analysis more closely with real-world conditions. Accordingly, we consider and contrast the following four sequencing rules:
We denote the cost of a sequencing rule with

Figures 5 and 6 show pairwise performance comparisons between the four sequencing rules, based on % performance gap, for fixed These results suggest that the order of in-person appointments (new vs. follow-up) has little effect on performance, as long as they are grouped together—either before or after telehealth visits. There is little difference between
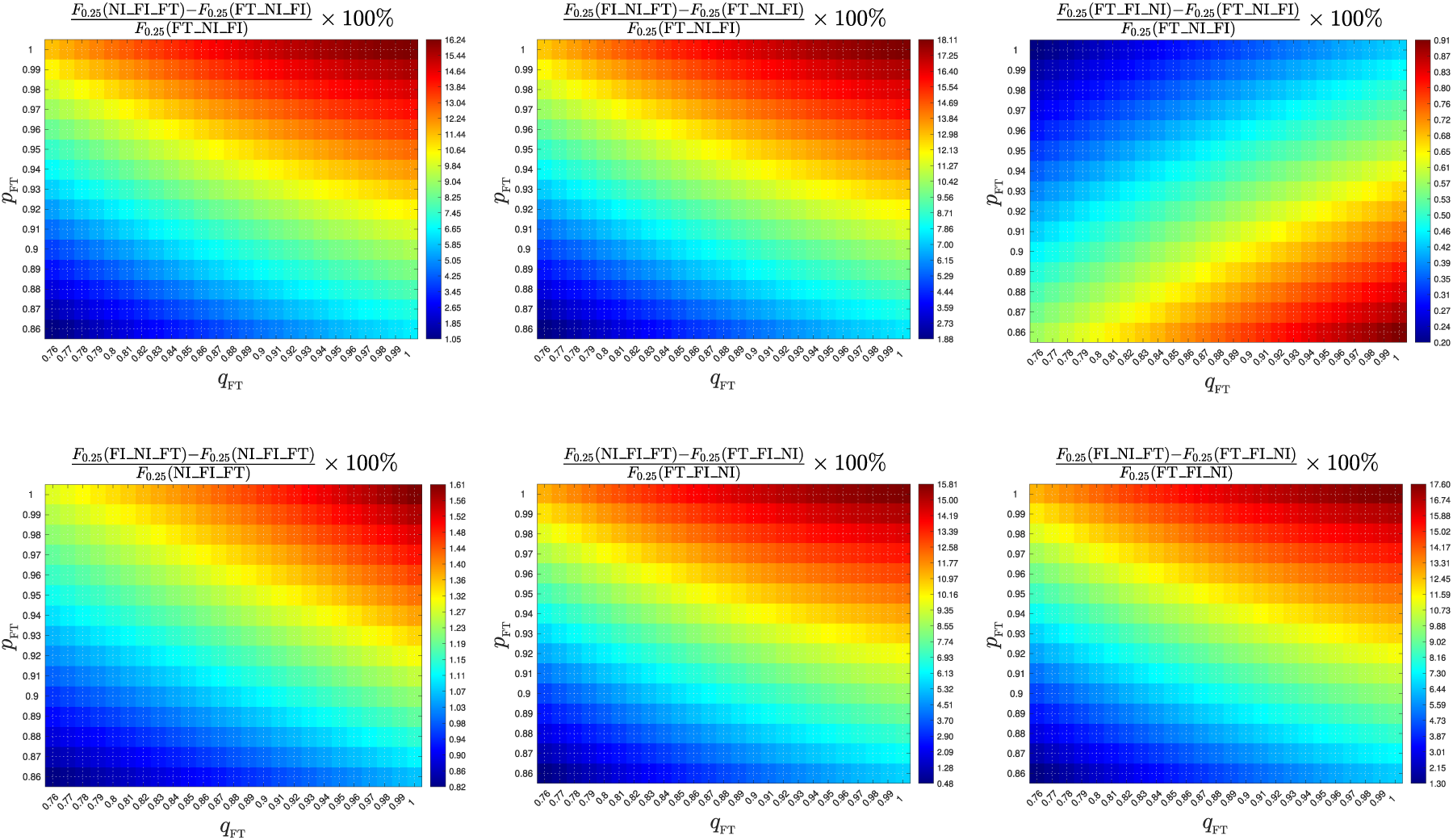
Pairwise comparisons of the four sequencing rules with 25% telehealth appointments.
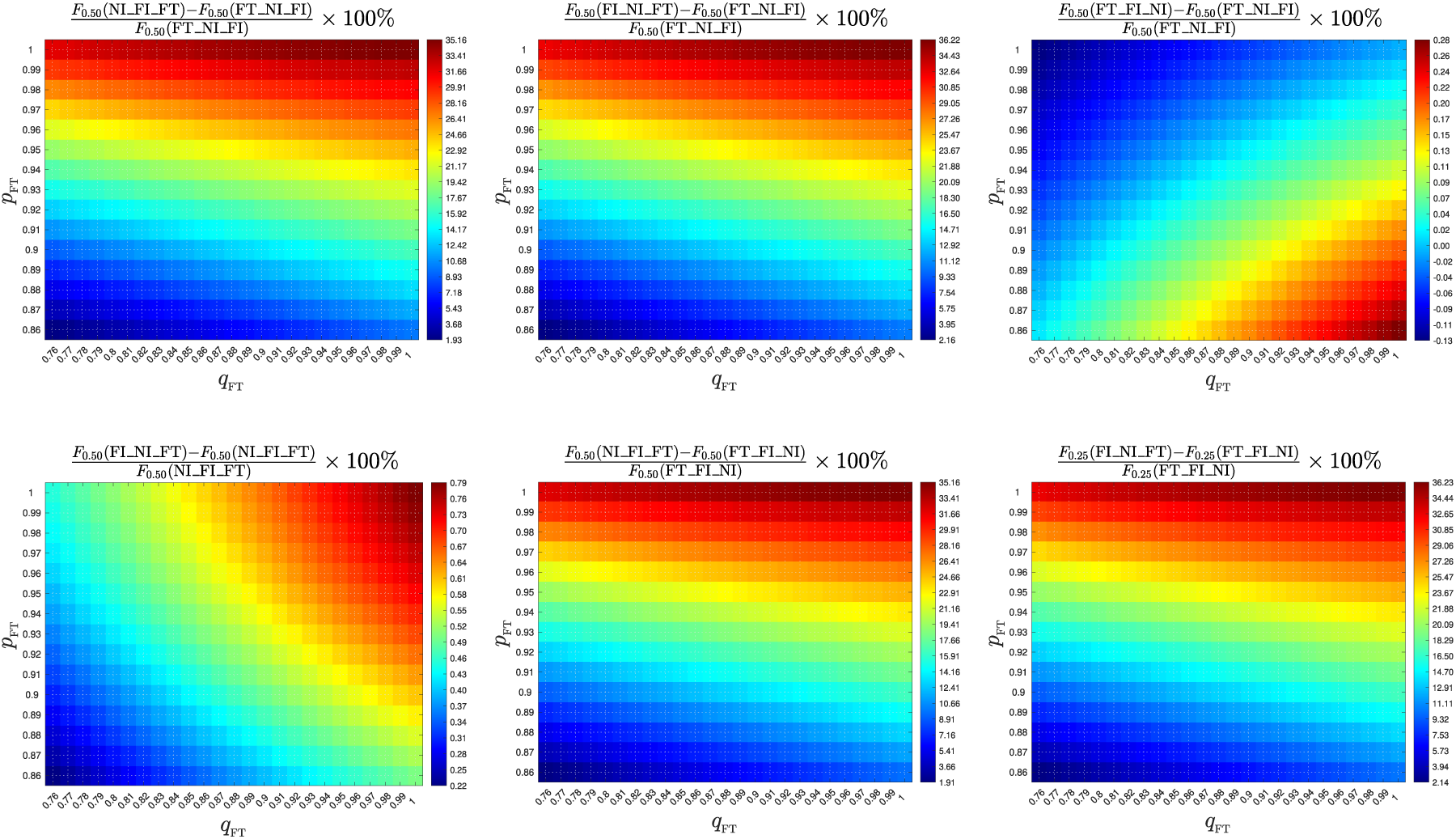
Pairwise comparisons of the four sequencing rules with 50% telehealth appointments.

Impact of telehealth capacity on operational performance.
Based on these insights, we recommend the following scheduling guidelines for clinics: Heterogeneity in no-show and punctuality rates between telehealth and in-person appointments significantly impacts operational efficiency and should be incorporated into scheduling templates. A segregated scheduling template should sequence telehealth appointments before in-person visits. The order of in-person visits—whether follow-ups or new patients—has little effect on performance.
We empirically investigate the impact of telehealth appointments on patient adherence to medical appointments and provider productivity. Using a comprehensive dataset of 412,415 appointments from a major American medical system, we analyze how telehealth affects patient no-shows and punctuality. Our findings reveal that telehealth significantly reduces no-shows and improves punctuality, especially for follow-up appointments and patient groups historically less adherent to in-person visits. We also observe that while telehealth appointments may increase revisit rates, the decrease in no-shows results in a net improvement in provider productivity, particularly evident with follow-up appointments. Finally, our study explores optimal scheduling strategies, highlighting that scheduling telehealth appointments before in-person visits throughout the day enhances operational efficiency compared to scheduling in-person visits first. These findings hold substantial implications for policymakers and healthcare organizations.
Supplemental Material
sj-pdf-1-pao-10.1177_10591478251375299 - Supplemental material for Breaking Barriers: Improving Patient Adherence to Appointments and Provider Productivity Through Telehealth
Supplemental material, sj-pdf-1-pao-10.1177_10591478251375299 for Breaking Barriers: Improving Patient Adherence to Appointments and Provider Productivity Through Telehealth by Masoud Kamalahmadi, Christos Zacharias, Howard Gitlow, Stephen Demers, Cristina Rubio-Delgado and KatelynWalker in Production and Operations Management
Footnotes
Acknowledgment
The authors gratefully acknowledge our industry partner for providing the data and the support of Winston Galiz, Anantha Gangadhara, Elizabeth Overstreet, and Ishwar Ramsingh.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Notes
How to cite this article
Kamalahmadi M, Zacharias C, Gitlow H, Demers S, Rubio-Delgado C and Walker K (2026) Breaking Barriers: Improving Patient Adherence to Appointments and Provider Productivity Through Telehealth. Production and Operations Management 35(4): 1333–1352.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.