
Abstract
The opioid epidemic poses widespread societal challenges. In response, electronic prescribing for controlled substances (EPCS), which requires prescribers to use the e-prescribing system, has begun attracting attention to combat the opioid epidemic by helping prescribers detect doctor shoppers and prevent forged prescriptions. However, a concern is that limited access to opioids after EPCS mandates may cause drug users to cross borders and travel to other areas without EPCS. Grounded in the tension on the efficacy of EPCS, this study aims to assess the impact of EPCS on the opioid dispensing rate. Leveraging a U.S. county-level data set from 2010 to 2020 and employing a quasi-experiment setup with matching, we find that counties without an EPCS mandate but adjacent to a state with an EPCS mandate experience an increase in opioid dispensing rates. Specifically, a neighboring-state EPCS mandate is associated with a 7.56% increase in the opioid dispensing rate in an adjacent county on average. The findings reveal that the negative spillover effect spreads deeper in areas with lenient illicit drug controls, in urban regions, and in areas with high poverty levels. Moreover, we estimate the overall efficacy of EPCS mandates by combining both the positive direct effect and the negative spillover effect of EPCS. We discuss theoretical and policy insights for the effective operation of EPCS mandates.
Keywords
Introduction
The ongoing opioid 1 epidemic is presenting severe public health challenges. Of the approximately 0.5 million drug-related deaths annually, opioids contribute to more than 75% of these fatalities (WHO, 2023). The United States stands out as one of the countries most severely affected by the opioid crisis. The number of opioid-related overdose deaths in 2021 was tenfold higher than that recorded in 1999, with opioids contributing to the fatalities of more than 80,000 people per year. Opioid usage and overdoses have caused serious societal issues, including substantial job losses (Azagba et al., 2021), elevated rates of crime, and transmission of the human immunodeficiency virus (Hodder et al., 2021). Considering that 25% of patients receive long-term opioid therapy in a primary care setting in the United States, opioid overdose presents significant challenges for the broader population, especially people with chronic pain (Banta-Green et al., 2009).
As 80% of opioids are dispensed by authorized prescribers in the United States, healthcare pundits suggest that the over-dispensing of opioids is a major cause of opioid overdose (Makary et al., 2017). To combat the opioid epidemic, there have been efforts at both the federal and state levels to adopt a supply-side policy—namely, electronic prescribing for controlled substances (EPCS)—that enforces the transmission of opioid prescriptions to pharmacies through a secure e-prescribing system. The end-to-end electronic transmission of scripts directly reduces illegible prescriptions (Abouk and Powell, 2021). Moreover, many e-prescribing systems have features that provide medication history that can help prescribers detect doctor shoppers. Thus, EPCS may help decrease opioid dispensing rates (Danovich et al., 2019). Along with these benefits are concerns about the negative spillover effect of EPCS: the stringent control of within-state opioid supply may more strongly induce cross-border substitution. This, in turn, may inadvertently prompt drug users to seek prescriptions in areas where the EPCS has not been mandated. In line with rational choice theory (Cornish and Clarke, 1985), drug users may find obtaining opioids from prescribers easier and less risky in nearby areas without EPCS mandates. For example, studies show that doctor shoppers tend to travel greater distances, with a median of 83.8 miles, to fill opioid prescriptions (Cepeda et al. 2013).
Grounded in this tension, this study aims to empirically examine the spillover effect of EPCS on the opioid epidemic. Specifically, we investigate whether counties without an EPCS mandate but adjacent to a state with such a mandate experience an increase in opioid dispensing rates (i.e., negative spillover effect). We are also interested in unpacking social conditions that influence the negative spillover effect. To delve deeper into the mechanism underlying this effect, we test whether the observed results are driven mainly by drug users’ cross-border behavior. Moreover, we examine the net effectiveness of EPCS mandates by combining the negative spillover effect and the positive direct effect of these mandates.
To this end, we exploit a quasi-experimental setting in which the EPCS mandate of the neighboring states serves as an exogenous shock. Specifically, we compare the opioid dispensing rates in counties adjacent to states with EPCS mandates (treatment group) with rates in counties not adjacent to states with EPCS mandates (control group) under a staggered difference–in–differences design. To alleviate concerns about structural differences between the treatment and control counties, we apply a matching technique. Our county-year-level balanced panel data set comprises 22,033 observations, covering 2,003 counties during the 11-year span from 2010 to 2020.
Our analyses show that, after the EPCS mandate in a neighboring state, the opioid dispensing rate increased in the focal county where EPCS had not been mandated, suggesting a negative spillover effect. Our findings reveal that illicit drug accessibility heightens the negative spillover effect. Moreover, the findings show a heterogeneous spread of the negative spillover effect by urbanization and poverty level. We also provide indirect empirical evidence that the negative spillover effect is driven by drug users crossing the state border. Furthermore, we find that the negative spillover effect may negate the positive direct effect of EPCS (i.e., decreasing opioid dispensing rates in mandated areas), and therefore, the overall impact of EPCS on national-level opioid dispensing rates is effectively nil. A series of robustness checks and falsification tests, including the relative time model and random implementation tests, substantiate the validity of our findings.
Broadly, this research aims to contribute to the literature on healthcare operations management (Dai and Tayur, 2020) by quantifying the spillover effect of EPCS mandates. Given that healthcare systems are often heavily regulated, policy plays a critical role in the healthcare ecosystem. Therefore, examining the impact of policy intervention that aims to boost health IT use on outcomes is crucial (Tuohy and Glied, 2011). While prior works have examined the impact of EPCS mandates on opioid dispensing, they have largely concentrated on the direct impact of EPCS mandates and limited their focus to the adopted area (Abouk and Powell, 2021; Danovich et al., 2019), without considering spillover effects on non-adopted areas. This limited focus clouds the understanding of the overall efficacy of EPCS mandates. Our study bridges this gap by empirically examining the spillover effect of EPCS mandates on healthcare outcomes in non-adopted areas, thereby extending understanding of the policy's dynamic effects within and across states and providing a comprehensive assessment of its efficacy.
In addition, our research contributes to the operations and management literature addressing the role of health IT in improving care delivery (Hydari et al., 2018; Lu et al., 2018). Amid the promise of health IT (e.g., e-prescribing system), particularly in opioid dispensing and overdose scenarios, our study shows that such promise may be unfounded. We demonstrate that while EPCS mandates, which guarantee e-prescribing system use in the healthcare delivery settings, lead to a decrease of opioid dispensing in the adopted area (i.e., direct positive effect), this positive effect is canceled out by negative spillovers in areas adjacent to a state with EPCS mandate, leading to a net effect of EPCS mandates on opioid dispensing rates close to zero. This finding emphasizes the importance of coordinated and simultaneous policies to boost health IT use across areas and healthcare delivery organizations. Moreover, our findings underscore the importance of considering the behavior of the target population (i.e., doctor shoppers and drug users) to unlock the efficacy of health IT.
Finally, this study has policy implications for federal health policymakers and state coordinators. While focal counties may not influence adjacent states’ legislative decisions to mandate EPCS, the implementation of proactive and protective measures in these counties could prove instrumental in reducing the negative externalities. Specifically, the implementation of lenient drug control policies and measures exacerbates the negative spillover effect. Furthermore, our findings indicate that the negative spillover effect spreads more rapidly in metropolitan areas and in regions with high poverty levels. This knowledge can help regulators identify areas vulnerable to the negative spillover effect. Overall, our study provides valuable insights into the ongoing policy debate surrounding EPCS mandates.
Related literature
Spillover effects of operational systems
The spillover effect is a substantial area of research in operations management literature. For example, Agrawal et al. (2020) investigate how quality knowledge developed by firms from their suppliers can spill over to other firms working with the same suppliers, with a specific focus on how organizational knowledge depreciation affects the quality gains obtained from such spillovers. Hu et al. (2020) contribute insights into an innovator's outsourcing decisions under spillover risks, distinguishing between technical and non-technical innovations and their respective channels of spillover. Qi et al. (2015) reveal the preferences of investing and non-investing firms regarding spillovers. Modi and Cantor (2021) propose that a competitor firm's environmental performance has a discernible spillover effect on a focal firm's environmental practices.
Aside from studies geared toward understanding the broad concept of spillover effects, a growing body of work has assessed the spillover effect of specific operational systems or strategies on outcome measures. Dong et al. (2014) show that vendor-managed inventory not only provides benefits to downstream firms in terms of inventory reductions but also has spillover effects on manufacturers by reducing downstream firms’ inventory variability. Cheng and Nault (2007) propose that quality benefits from upstream suppliers’ IT use and investments have a positive impact on downstream industries, increasing the total output produced. Belderbos et al. (2004) find that through information exchange with vertical partners in the supply chain, companies can obtain positive knowledge spillovers, thereby improving their financial performance. Lim et al. (2024) suggest that off-service placement, a typical operation strategy to resolve mismatches in supply and demand, has significant, negative spillover effects on the service efficiency delivered to customers who are placed on service.
Narrowing the scope to the healthcare domain, research endeavors have mainly focused on direct effects of operational systems in general and health IT in particular; relatively scant attention has been given to spillover effects. Regarding direct effects, Lu et al. (2018) find that the adoption of health IT can enhance the automation of nursing tasks. LaGanga and Lawrence (2012) suggest that a flexible appointment scheduling model can reduce the detrimental effects of patient no-shows. Regarding electronic health records (EHRs), Hydari et al. (2018) report a 17.5% decline in patient safety events, and Pang et al. (2021) find a decrease in opioid dispensing rates after EHRs adoption. Conversely, Laker et al. (2018) caution that easy access to clinical information in the form of EHRs can lead to information overload, potentially compromising both productivity and the quality of care. Only a few studies have addressed the spillover effect of health IT adoption and use. For example, Ayer et al. (2019) find that operational enhancements through health information exchanges have positive spillover effects by improving coordination in emergency departments. Similarly, Atasoy et al. (2018) show that the adoption of electronic medical records has positive spillover effects by decreasing the healthcare costs of the other hospitals in the same region. Our study extends this stream of literature by assessing the spillover effects of the EPCS and corresponding e-prescribing usage, with particular attention paid to social-level outcomes.
EPCS mandate
To combat the opioid epidemic, federal and state governments have adopted policies to boost health IT. Health IT is the suite of information technologies and systems that comprise the input, transmission, use, extraction, and analysis of information in the healthcare sector (e.g., e-prescribing system, EHRs) (NIH, 2023), and policies, such as prescription drug monitoring program (PDMP) laws and EPCS mandates are aimed at promoting and governing the use of such health IT to reduce opioid supply.
States began enacting laws to establish PDMPs—statewide electronic databases for tracking controlled-substance prescriptions—in the early 2000s. By providing prescribers with databases about patients, they are intended to help flag high-risk prescribing and potential illegal activity (Bao et al. 2016). For example, Bao et al. (2016) show that PDMPs are effective in reducing the number of prescriptions for opioids. However, by design, PDMPs do not secure the issuance or transmission of prescriptions and, consequently, may be constrained in the prevention of post-prescription forgery (e.g., fraudulent scripts) after a prescription leaves the prescriber's hands. In addition, adoption and use policies (must-access vs. optional) and reporting intervals (daily vs. monthly) vary widely between states (CDC, 2024; PDMP TTAC, 2021). For these reasons, some studies have reported no significant effect of PDMP use on reducing opioid prescribing (Stucke et al., 2018; Sun et al., 2018).
The EPCS mandate—enforcing the process of transmitting prescriptions for opioids to the pharmacy through the secure e-prescribing system—may address these limitations and also deliver unique benefits. First, while PDMPs do not secure the transmission of prescriptions, under EPCS, prescriptions must be transmitted exclusively in electronic form without any alteration or conversion to fax. This directive substantially reduces the risk of post-prescription forgery, such as theft of prescriptions, handwritten modifications, or quantity alterations. Before e-prescribing, prescriptions were written by hand or faxed, with illegible prescriptions often increasing medication errors (Ammenwerth et al., 2008). Moreover, hand or faxed prescriptions are vulnerable to fraud by tampering, with individuals substituting a different drug, adding refills, or inflating pill counts. Given that up to 9% of people misusing opioids obtained pills with forged prescriptions (Abouk and Powell, 2021), end-to-end electronic transmission of scripts under EPCS substantially decreases such fraud. Second, unlike PDMPs, whose use is not compulsory in many states, EPCS mandates the process by which prescribers electronically send error-free prescriptions directly to a pharmacy through a secure network. 2 In other words, the EPCS mandate requires the routine use of the e-prescribing system in daily practice. Third, many e-prescribing systems have features that give physicians decision support and provide a complete and accurate medication history, which can detect doctor shoppers (Gabriel et al. 2016). For example, Surescripts, a major e-prescribing system provider in the United States, allows prescribers to access comprehensive medication histories of patients at the point of prescribing (Aldughayfiq and Sampalli, 2021). In line with this, the Drug Enforcement Administration (DEA) suggests that the electronic transfer of controlled substance prescriptions can decrease the potential for duplicate prescriptions and thus reduce the opportunity for opioid diversion or misuse (DEA, 2023). As such, EPCS can stringently control opioid supply in the mandated areas. In line with this, prior studies suggest that the EPCS mandate is associated with decreased opioid dispensing rates in mandated areas. For example, Abouk and Powell (2021) report that the implementation of the EPCS mandate in New York led to a reduction in opioid prescribing. Similarly, Danovich et al. (2019) find that opioid prescribing by emergency physicians decreased after the implementation of EPCS mandates.
As such, efforts to enforce EPCS mandates have increased at the national level. For example, the DEA regulation permits electronic prescriptions for controlled substances and provides the requirements for EPCS systems, such as encryption and digital signature. The regulation also permits pharmacies to receive, dispense, and archive electronic prescriptions. The DEA's (2010) Interim Final Rule on EPCS (Docket No. DEA–218) became effective on June 1, 2010. In addition, through the Substance Use Disorder Prevention that Promotes Opioid Recovery and Treatment for Patients and Communities Act, enacted in 2018, the Centers for Medicare & Medicaid Services requires at least 70% of Medicare Part D Schedule II-V controlled substance prescriptions to be electronic. The first measurement year for compliance with the requirements of the EPCS program was 2023, and prescriptions written for a beneficiary in a long-term care facility are to be included in determining compliance no earlier than January 1, 2028 (CMS, 2023). In response to these national-level efforts, several states introduced EPCS mandates during the 2010–2020 period. 3
With the growing adoption of EPCS, research has increasingly examined the efficacy of EPCS mandates (see Table A1 in Appendix A of the E-companion); however, important knowledge gaps remain.
Most prior studies have limited their focus to measuring the direct impact of EPCS-adopted states or hospitals (Abouk and Powell, 2021; Danovich et al., 2019). Although these studies are insightful, the spillover effects of EPCS remain underexplored. Moreover, the existing literature evaluating EPCS primarily tests a one-directional hypothesis—reporting positive or null effects in adopting areas only (Abouk and Powell, 2021; Danovich et al., 2019; Everson et al., 2020). As such, they are unable to capture dynamics across borders and therefore cannot thoroughly measure EPCS's overall effectiveness. To close this gap, we investigate the negative spillover effects of EPCS through a quasi-experiment setting with a large-scale panel data set. Going beyond analyses that quantify only the spillover effect, we jointly estimate direct and spillover effects to obtain a comprehensive estimate of the net effect.
Rational choice theory
To establish the link between EPCS mandates of a neighboring state and opioid dispensing rates of the focal county (without EPCS and adjacent to the state with EPCS), we adopt rational choice theory (Cornish and Clarke, 1985) as our theoretical lens; this theory is arguably the most emphasized framework for explaining socially undesirable behavior, such as theft (Matsueda et al., 2006), violence (Brownstein et al., 2014), and fraud (Kuo and Tsang, 2023). The theory posits that to optimize utility, individuals engage in rational decision-making by evaluating the costs and benefits associated with their choices. A key component in this rational calculation is the perceived likelihood of being arrested. For example, in a drunk-driving scenario (Greenwood and Wattal, 2017), an individual may perceive a ride-sharing service as economically feasible for the journey home. Alternatively, the individual may choose to drive drunk when the cost of ride-sharing services is too high.
Applying this theory to the drug use scenario, drug users struggling with opioid addiction are notably compelled to continue using opioids because of the intense and aversive experience of “dope sick” or opioid withdrawal. Drug users anticipate the future consequences of their current behavior and act in their own best interests to maximize utility. These individuals may try to substitute with a different drug, add refills, inflate pill counts, or obtain pills with forged prescriptions (Abouk and Powell, 2021). Moreover, they may seek opioid prescriptions from multiple healthcare providers, securing legal quantities each time (i.e., doctor shopping). By hiding their drug use intentions, drug users minimize the risk associated with criminal activities, thus ensuring a more enduring and less detectable means of securing opioids.
With the EPCS mandated in a focal state, obtaining prescribed opioids within the state becomes challenging, as prescribing history is traced and shared with the doctor via the e-prescribing system. Moreover, EPCS requires end-to-end secure electronic transmission of prescriptions—as mentioned, handwritten or faxed prescriptions are prohibited—thereby directly reducing opportunities for prescription fraud, even after a prescription leaves the prescriber's hands. Faced with this obstruction, drug users may resort to crossing state lines and visiting neighboring counties where EPCS is not mandated. Several studies suggest the potential for drug users to travel to other areas or cross state borders to feed their habit. For example, Johnson et al. (2013) show that suburban and urban drug buyers are willing to travel to various locations to obtain drugs. Gomes et al. (2012) find that drug users engage in international border travel to exploit favorable opioid regulations. Building on these findings, we predict that when neighboring states enact EPCS mandates, bordering counties without EPCS will experience an increase in opioid dispensing rates, as EPCS mandates stringently control the opioid supply of the adopted state.
Methodology
Research setting
To investigate whether counties with no mandated EPCS and adjacent to a state with such a mandate experience an increase in opioid dispensing rates, we adopt a common staggered DID design, with the EPCS mandate of the neighboring state serving as an exogenous shock. The EPCS mandate of neighboring states is an as-good-as-random treatment, as its implementation is decided independently by the neighboring state. Consequently, the treated county (i.e., experiencing the EPCS mandate of the neighboring state) is randomly affected by this decision and thus unable to self-select as treated, thereby alleviating concerns about endogeneity issues.
Based on the DID assumption that the control and treatment groups are not influenced by any factors other than the treatment (i.e., EPCS mandate of the neighboring state), the treatment group consists of counties without an EPCS mandate, but that experienced the EPCS mandate of the neighboring state at any point in time during the study period. 4 By contrast, the control group consists of counties where neither they themselves nor their neighboring counties had mandated EPCS during the study period. In other words, the control group consists of counties with no EPCS mandate, and that did not experience the EPCS mandate of the neighboring state during the study period. This restriction ensures that the control group counties do not experience any geographic spillover effects of EPCS mandates of neighboring states. For example, when Minnesota mandated EPCS, the bordering counties that had not mandated EPCS (black area in Figure 1) would be considered the treatment group. We argue that drug users in Minnesota might try to obtain opioid prescriptions from these bordering counties, potentially leading to an increase in opioid dispensing rates in those areas. Under the DID framework, we examine and compare opioid dispensing rates in counties adjacent to states with an EPCS mandate (treatment group) with those in counties without any geographic influence of an EPCS mandate (control group).

Example of treated counties.
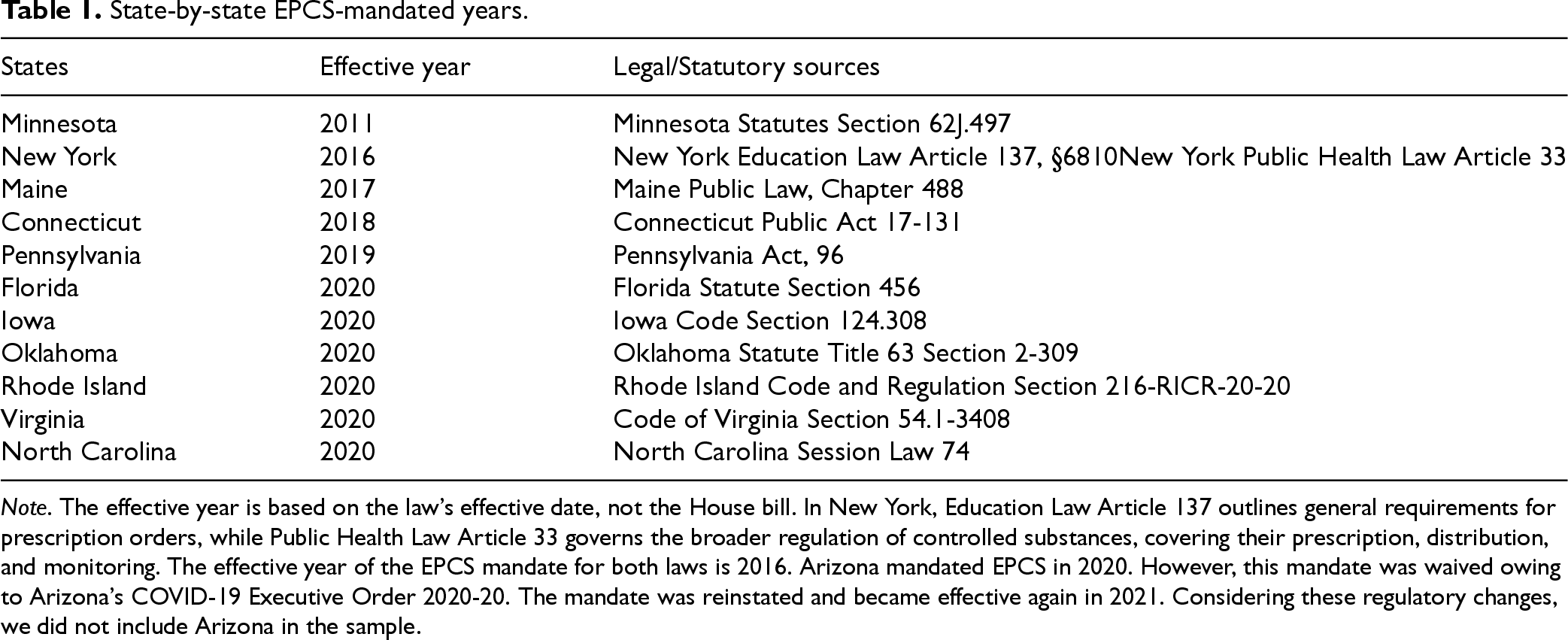
For the state-to-state effective year of EPCS mandates, we rely on information directly from each state's laws/statutes, instead of relying on commercial websites of EPCS vendors (i.e., e-prescribing system vendors). Table 1 presents the state-by-state EPCS-mandated years and the legal/statutory sources for each state. As the table shows, during the study period (2010–2020 5 ), 11 states implemented the EPCS mandate. As the EPCS mandate was implemented in different states at different times, this staggered rollout allows us to leverage a staggered DID setup. We further conducted robustness checks to account for the potential variation in the implementation timing of EPCS mandates across states. Details and results are reported in Appendix B of the E-companion. The web sources for EPCS mandates for each state are in Appendix A, Table A2.
State-by-state EPCS-mandated years.
State-by-state EPCS-mandated years.
Note. The effective year is based on the law's effective date, not the House bill. In New York, Education Law Article 137 outlines general requirements for prescription orders, while Public Health Law Article 33 governs the broader regulation of controlled substances, covering their prescription, distribution, and monitoring. The effective year of the EPCS mandate for both laws is 2016. Arizona mandated EPCS in 2020. However, this mandate was waived owing to Arizona's COVID-19 Executive Order 2020-20. The mandate was reinstated and became effective again in 2021. Considering these regulatory changes, we did not include Arizona in the sample.
Our data are at the county level, which is the most granular data available for the dependent and control variables during the study period. In constructing the treatment group, we limited our empirical focus to the counties directly adjacent to the state with EPCS mandates (i.e., bordering counties). We assume that counties located directly on the border, rather than those farther away, will be directly affected by the EPCS mandate of adjacent states. The rationale is that drug users are more likely to visit these bordering counties given the shortest time and lowest cost associated with travel to seek opioids. The dependent variable is the opioid dispensing rate, and these data come from the CDC. Opioid-related studies (Guy et al., 2019) and official CDC reports (García, 2019) have also extensively used this data set.
We control for various demographic and socioeconomic factors to address potential confounders. For demographic factors, we control for population size, gender (male), age (25–34 years), and race composition (white) in each county. Prior studies suggest that population size is positively related to higher opioid dispensing rates because the larger a city, the greater is the chance that a substantial proportion of its population is in demographic categories known to have a higher risk of opioid overdose (Altekruse et al., 2020). We added gender and race compositions to account for potential differences in seeking opioid prescriptions. Research suggests that opioids are more likely to be prescribed for men (Silver and Hur, 2020) and whites (Pletcher et al., 2008). Finally, a national survey found that the percentage of trips made by people aged 25–34 years who traveled to neighboring states was higher than that of any other age group (Federal Highway Administration, 2017). Moreover, we control for socioeconomic factors, as these can determine the living conditions and resources that directly exacerbate opioid-seeking behavior. Specifically, the unemployment rate and labor force are factors consistently associated with higher opioid use (Böckerman et al., 2021). Moreover, we include income as an additional control, as economic disadvantage is associated with greater exposure to and use of prescription opioids (Friedman et al., 2019). Opioid-related factors, accessibility to substance abuse treatment facilities, uninsured rates, and PDMP adoption also serve as additional controls. Research suggests that county-level uninsured rates have a positive impact on the increased level of opioid dispensing rates (Guy et al., 2019). Substance abuse treatment facilities directly provide treatment for opioid overdose, potentially influencing local dispensing rates. Last, state-run PDMPs advocate pharmacies to transmit data on all filled prescriptions for controlled substances to a centralized repository and thus are associated with the reduction of opioid overdoses (Bao et al. 2016). 6
The data for the control variables came from various official sources, including the CDC, American Community Survey, Small Area Income and Poverty Estimates, Bureau of Economic Analysis, and PDMP Training and Technical Assistance Center. We list the specific sources for the data and variable definitions in Table A3 in Appendix A in the E-companion. When combined, our initial sample (before matching) is a balanced panel data set consisting of 192 treatment counties and 1811 control counties across 11 years (2010–2020). Table 2 provides summary statistics, and Table A4 in Appendix A presents a correlation table.
Summary statistics.
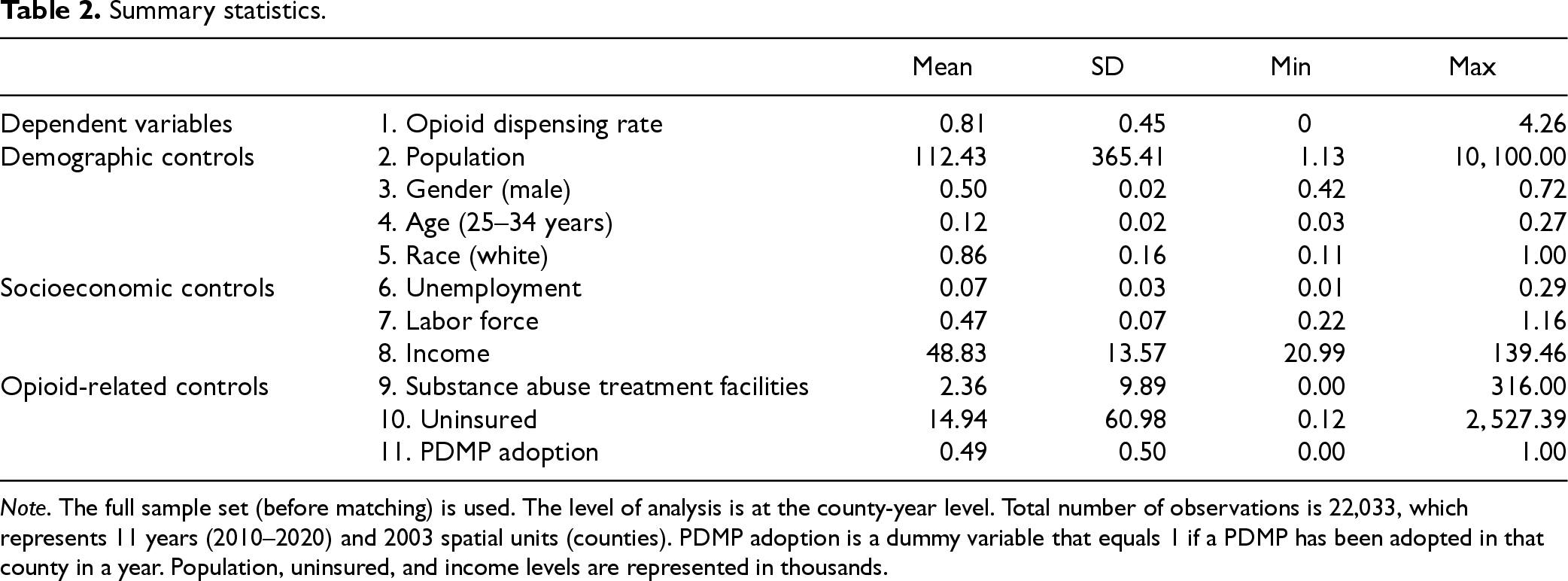
Note. The full sample set (before matching) is used. The level of analysis is at the county-year level. Total number of observations is 22,033, which represents 11 years (2010–2020) and 2003 spatial units (counties). PDMP adoption is a dummy variable that equals 1 if a PDMP has been adopted in that county in a year. Population, uninsured, and income levels are represented in thousands.
We employ a common staggered DID design and use the EPCS mandate of neighboring states as an exogenous shock. In our context, the DID estimation compares the opioid dispensing rates of treatment counties experiencing geographic spillover of EPCS mandates from neighboring states with the rates of control counties without any influence of an EPCS mandate geographically. By accounting for changes in the control group, the DID framework enables us to effectively control for various confounding factors in addition to the treatment effect. The DID framework relies on the assumption that the treatment and control group counties are comparable in the absence of treatment. To mitigate potential systematic differences between treatment and control (Blackwell et al., 2009), we execute the matching following the recent studies in management and economics (Burtch et al., 2018; Greenwood and Wattal, 2017). Specifically, we pair the control county with the treated county through matching and then examine the DID estimator on the basis of these matched treatment–control pairs. This approach improves the causal effect of the treatment by limiting the difference between the treatment and control groups (Overby and Forman, 2015).
Following prior studies, we executed matching using covariates measured one year before each treatment cohort's adoption (Burtch et al., 2018; Li et al., 2001; Lu and Greevy, 2023; Rosenbaum, 2020). Specifically, we execute matching in sequential order (Li et al., 2001; Lu and Greevy, 2023; Rosenbaum, 2020)—that is, for each cohort, the treated county adjacent to a state with EPCS mandates (i.e., treatment group) with a control county that did not experience any geographic influence of EPCS mandates (i.e., control group)—using four criteria: opioid dispensing rates, demographic characteristics (i.e., population), socioeconomic characteristics (i.e., unemployment), and opioid-related characteristics (i.e., substance abuse treatment facilities and uninsured)
7
in the year before treatment. If a control county is paired with multiple treated counties, we allow each control unit to be matched with only one treated county by retaining only the pair for which the treatment occurs earliest, following prior research (Burtch et al., 2018).
8
After matching, the differences across matching covariates between the treatment and control groups are substantially smaller, indicating statistical balance. Specifically, after matching, the two-tailed t-tests showed no significant differences in the mean values of pre-opioid dispensing rate (t = −0.02, p = .985), population (t = −0.12, p = .906), unemployment (t = −0.08, p = .933), number of substance-abuse treatment facilities (t = 0.73, p = .466), and uninsured rate (t = −0.92, p = .356) between the treatment and control groups. The final matched sample consists of 10,923 observations, covering 9504 observations in the control group (i.e., 864 counties across the 11-year span) and 1419 observations in the treatment group (i.e., 129 counties across the 11-year span). Our model specification is as follows:

Main results
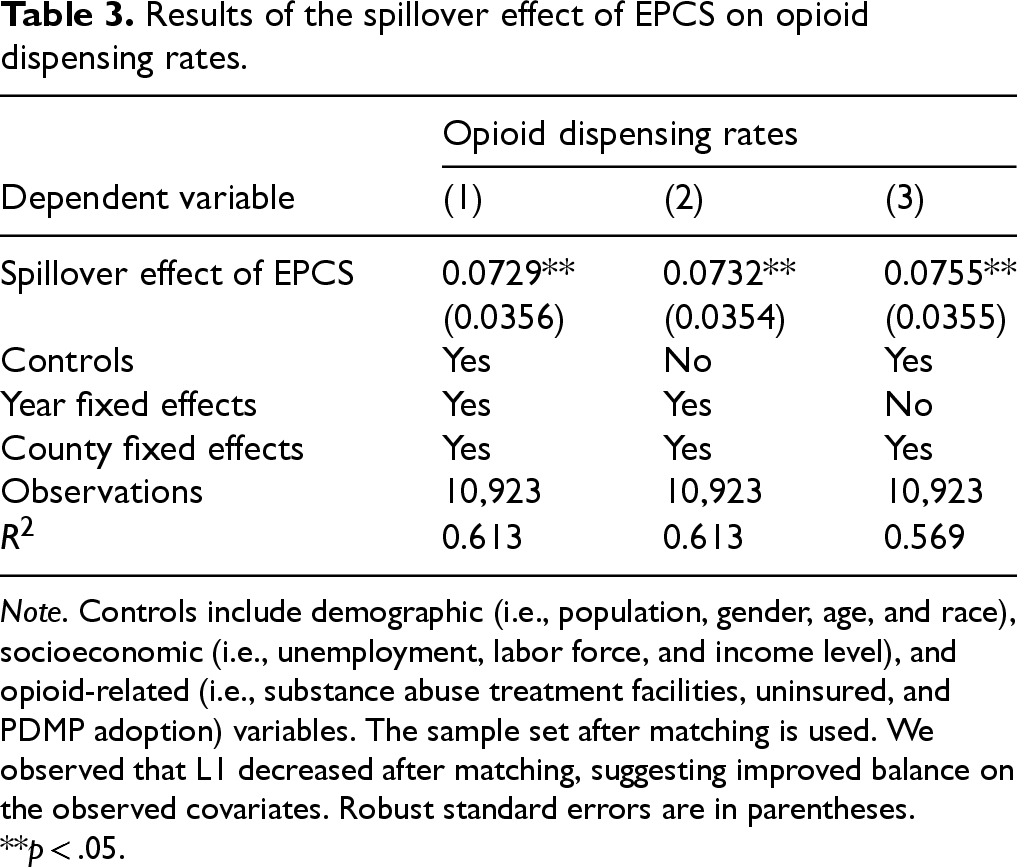
Table 3 reports the estimation results of our model. In Column (1), Table 3, the coefficient of interest is positive and statistically significant (0.0729, p < .05). The positive coefficient indicates that the opioid dispensing rate increased in the counties adjacent to EPCS-mandated states (treatment group), compared with the counties without any geographic influence of an EPCS mandate (control group), after the EPCS mandate in neighboring states. This result is robust under the model without control variables (Column (2)) and year fixed effects (Column (3)). Furthermore, the analysis results using the panel data set before matching are consistent with our results using the matched sample, ensuring the robustness of our findings. The result can be found in Table A5 of Appendix A in the E-companion.
Results of the spillover effect of EPCS on opioid dispensing rates.
Results of the spillover effect of EPCS on opioid dispensing rates.
Note. Controls include demographic (i.e., population, gender, age, and race), socioeconomic (i.e., unemployment, labor force, and income level), and opioid-related (i.e., substance abuse treatment facilities, uninsured, and PDMP adoption) variables. The sample set after matching is used. We observed that L1 decreased after matching, suggesting improved balance on the observed covariates. Robust standard errors are in parentheses.
**p < .05.
Sensitivity tests
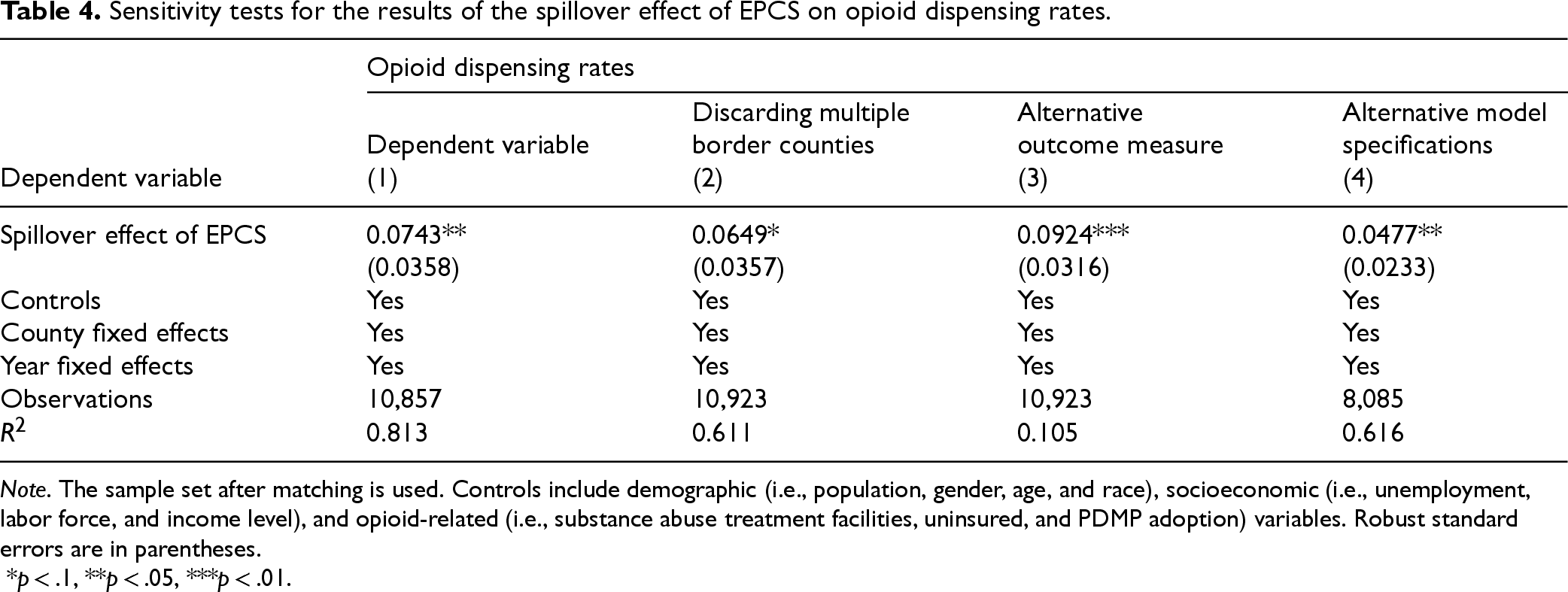
We conduct a series of sensitivity tests to ensure the robustness of our findings. First, counties exposed to more than one treatment (i.e., share borders with more than one EPCS-adopting state 10 ) might experience a larger spillover effect, which in turn could inflate the average treatment coefficient. To rule out this possibility, we exclude multiple-border counties in our sample, so that only counties with a single treated neighbor remain in the treatment group. We then repeat the matching, and re-estimate the baseline model. If counties do share borders with more than one EPCS adopting state, thereby creating a larger spillover effect, we might observe a decreased effect size or a non-significant effect when removing those counties. In Column (1), Table 4, we consistently observe the negative spillover effect of the EPCS mandate. We also conduct a Z-test, comparing coefficients from the sample without multiple treated counties (0.0743) with coefficients of our main result (0.0729). The result reveals no statistical difference between the coefficients (Z-score = 0.0276, p > .1). These results confirm that the potential heightened impact due to multiple-border counties is not the main driver of our results. Second, to address a concern that our results may be driven by the choice of outcome measure (i.e., the opioid prescribing rate), we use the logged number of opioid prescriptions as an alternative dependent variable. We rerun the analysis using the same specification (1). As we show in Column (2) in Table 4, the coefficient remains positive and statistically significant. Third, we implement an alternative model, and the result in Column (3) of Table 4 shows a positive and significant coefficient, consistent with our main findings. Finally, to address the potential effect of the COVID-19 pandemic, 11 we exclude counties that received treatment after 2019 (i.e., those treated in 2020) in our sample. After that, we re-conduct the matching and estimation. As Column (4) in Table 4 shows, the results remain the same, alleviating concerns about the potential influence of the COVID-19 outbreak. As a whole, our results are robust to alternative model specifications or outcome measures. In addition, they are not driven by specific counties or events.
Sensitivity tests for the results of the spillover effect of EPCS on opioid dispensing rates.
Sensitivity tests for the results of the spillover effect of EPCS on opioid dispensing rates.
Note. The sample set after matching is used. Controls include demographic (i.e., population, gender, age, and race), socioeconomic (i.e., unemployment, labor force, and income level), and opioid-related (i.e., substance abuse treatment facilities, uninsured, and PDMP adoption) variables. Robust standard errors are in parentheses.
*p < .1, **p < .05, ***p < .01.
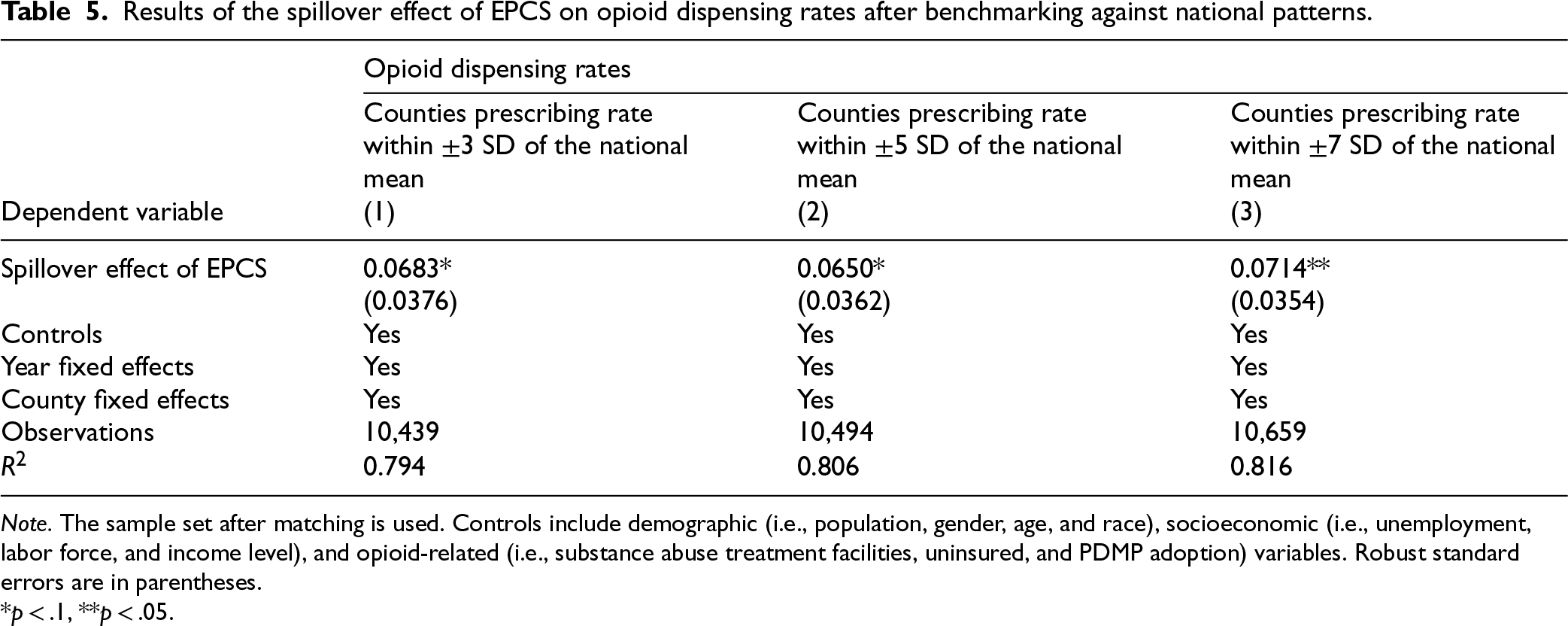
Given that our main study goal is to examine the spillover effect of EPCS, our sample consists of treatment counties that show rapid post-treatment increases and control counties in unregulated states. To avoid conflating spillover with direct effects, our sample intentionally excludes counties located inside EPCS–mandate states—that is, regions expected to have lower opioid prescribing rates as a result of the EPCS mandate. This sample composition may naturally yield a higher-than-national-average rate during the study period (2010–2020). To improve comparability with the national average and enhance generalizability, we reconstructed the sample sets to counties whose mean rates during the study period fall within ±3, ±5, and ±7 standard deviations of the national mean 12 ; we then repeated the matching and reran analysis.
If the spillover coefficients remain stable across these samples, we can decrease potential differences relative to the national sample and increase the generalizability of our findings. The results in Columns (1)–(3) in Table 5 show that EPCS mandates of neighboring states continue to drive increased opioid prescribing rates of focal counties adjacent to the states enacting EPCS. To assess whether the spillover coefficients from the restricted samples differ significantly from the main-analysis coefficient (0.0729, Column (1), Table 3), we performed Z-tests. The results indicate no statistically significant differences among the coefficients (p > .1). 13 Overall, these findings suggest that the observed negative spillover effect is not attributed to the counties with high prescribing rates, improving the generalizability of our findings.
Results of the spillover effect of EPCS on opioid dispensing rates after benchmarking against national patterns.
Results of the spillover effect of EPCS on opioid dispensing rates after benchmarking against national patterns.
Note. The sample set after matching is used. Controls include demographic (i.e., population, gender, age, and race), socioeconomic (i.e., unemployment, labor force, and income level), and opioid-related (i.e., substance abuse treatment facilities, uninsured, and PDMP adoption) variables. Robust standard errors are in parentheses.
*p < .1, **p < .05.
A possible concern is that an idiosyncratic characteristic of counties, such as an unobserved policy change, might affect the results. Although we include county-level fixed effects in our estimation and thus account for structural differences across the treatment and control counties to a certain extent, we conduct a random shuffle test (see Bertrand et al., 2004) to ensure the robustness of our results. Specifically, we shuffle the treatment indicators representing the EPCS mandate of neighboring states in our original sample, thereby generating a pseudo-treatment indicator. After replicating 1000 iterations, we obtained the distribution of the estimated DID coefficients (Figure 2). The results indicate that the average estimated β (pseudo-treatment) is not statistically significant (–0.00041, p > .1). In addition, using the mean and standard deviation of the placebo coefficients, we compared the genuine estimated β with the placebo distribution and found that genuine estimated β is statistically different from the mean placebo coefficient (p = .000042). Overall, these results show the validity of our treatment, and therefore, we can conclude that the estimated treatment effect is not driven by chance.
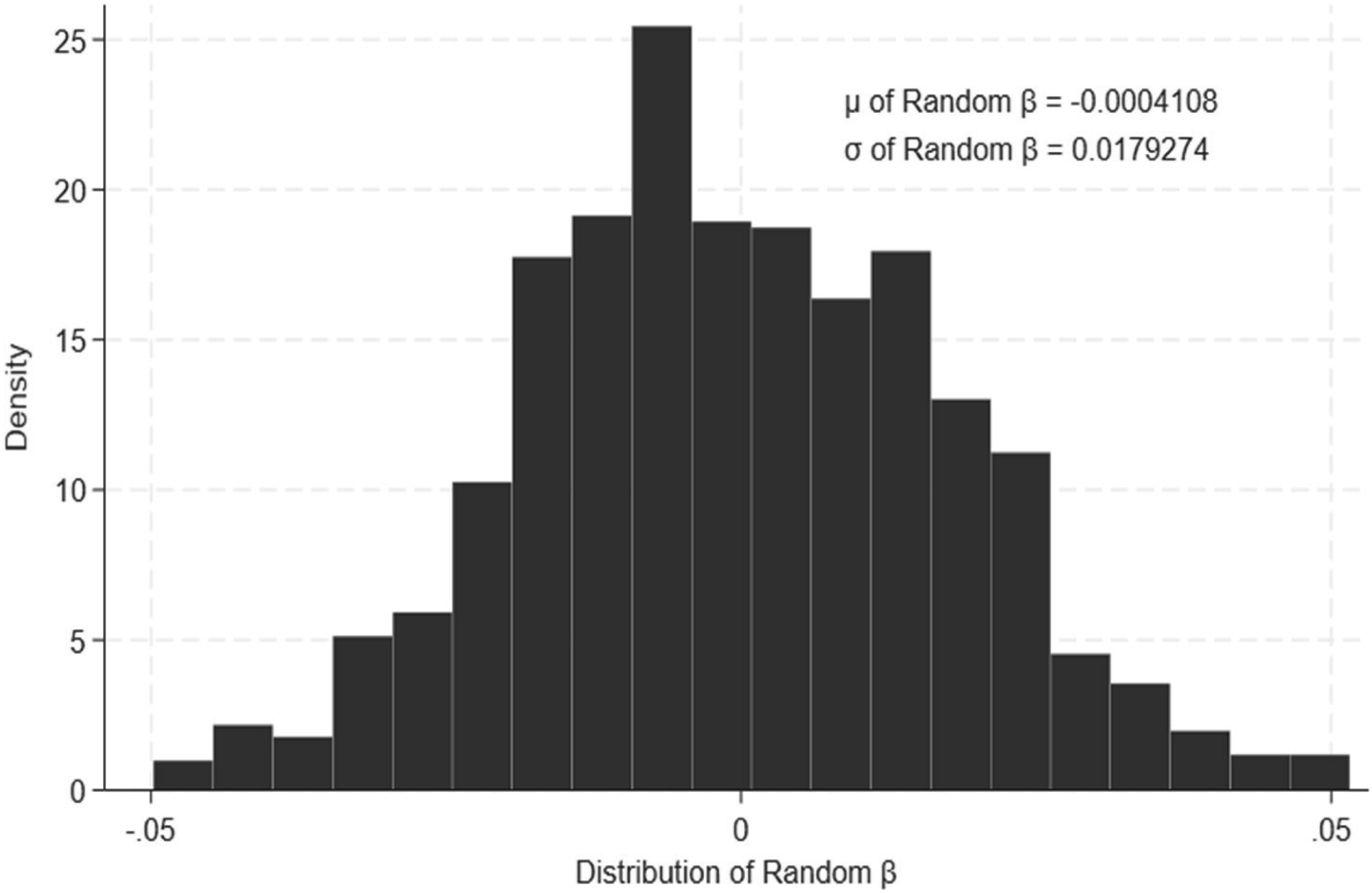
Distribution of coefficients from randomly shuffling the treatment indicator. Note. Distribution is derived from 1,000 iterations.
To validate the parallel trends assumption underlying the DID model, we investigate whether the pre-treatment trend of opioid dispensing rates differs between the treatment and control groups, using the relative time model (Burtch et al., 2018; Greenwood and Wattal, 2017). We replicate our estimations with this model as follows:

Relative time model results of the spillover effect of EPCS on opioid dispensing rates.
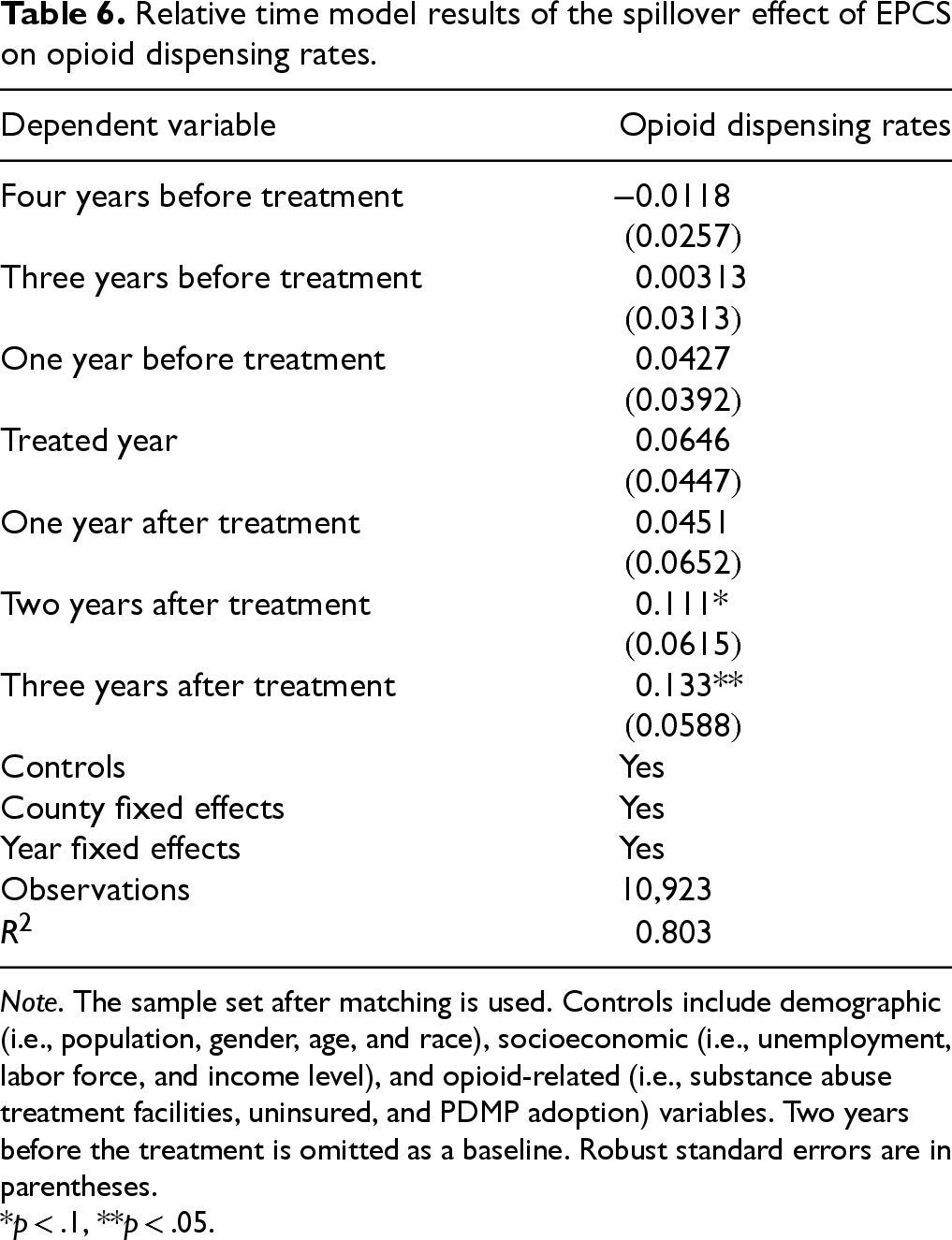
Note. The sample set after matching is used. Controls include demographic (i.e., population, gender, age, and race), socioeconomic (i.e., unemployment, labor force, and income level), and opioid-related (i.e., substance abuse treatment facilities, uninsured, and PDMP adoption) variables. Two years before the treatment is omitted as a baseline. Robust standard errors are in parentheses.
*p < .1, **p < .05.
In this section, we aim to unpack moderators that influence the magnitude of the effect (section 5.1) and underlying mechanisms (section 5.2), to provide a deeper understanding of the negative spillover effect of EPCS. In addition, we assess the overall efficacy of EPCS mandates by combining both the direct effects and the spillover effects (section 5.3).
Moderators
We investigate social conditions that may influence the magnitude of the negative spillover effect. First, we focus on the urbanization level. The predicted impact of urbanization on the negative spillovers of EPCS is not straightforward. On the one hand, urbanization may increase the magnitude of the negative spillover effect. Studies imply that obtaining opioid prescriptions may be relatively easier in metropolitan areas than in nonmetropolitan areas, given the higher density of prescribers and opioid availability (McDonald et al., 2012). Indeed, prior work shows that increasing urbanization and availability of prescribers are associated with increasing opioid dispensing rates (Wright et al., 2014). In line with this, Rigg and Monnat (2015) find that urban adults are more likely to misuse prescription opioids than rural adults. Overall, the higher density of available opioids may create a more favorable environment for doctor shopping and forged prescriptions. On the other hand, studies suggest that negative spillover effects can be heightened in nonmetropolitan areas. Specifically, opioid regulations in micropolitan and rural areas tend to be less stringent than those in metropolitan areas, potentially facilitating easier access to forged prescriptions (Leukefeld et al., 2007). Given the lack of a clear expectation for these effects, our investigation relies on empirical analysis for guidance. To this end, we used Rural-Urban Commuting Area codes from the Economic Research Service of the U.S. Department of Agriculture as a proxy for urbanization level (i.e., metropolitan vs. nonmetropolitan).
14
We used the following model specification:

Sensitivity tests for the results of the spillover effect of EPCS on opioid dispensing rates.
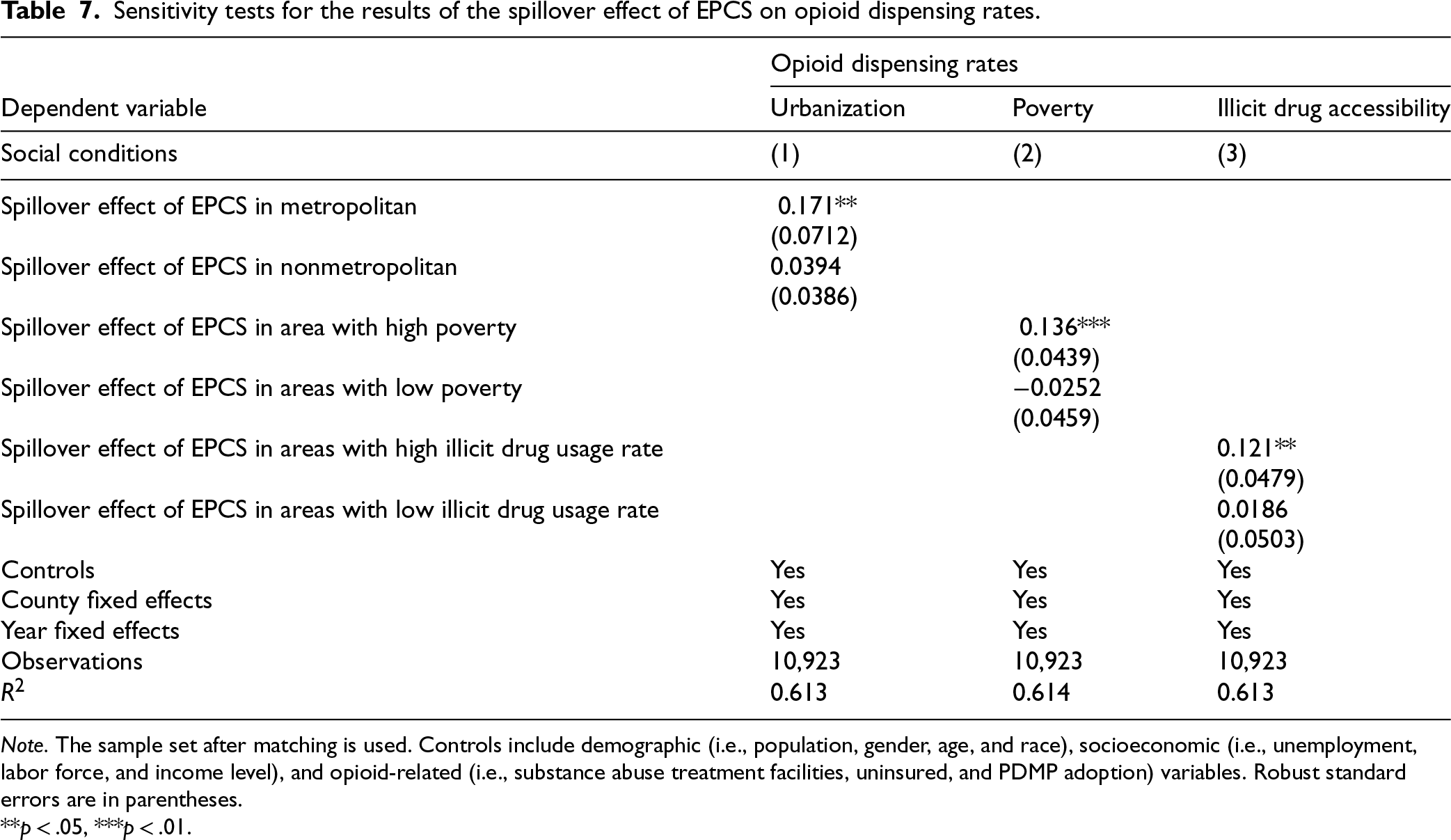
Note. The sample set after matching is used. Controls include demographic (i.e., population, gender, age, and race), socioeconomic (i.e., unemployment, labor force, and income level), and opioid-related (i.e., substance abuse treatment facilities, uninsured, and PDMP adoption) variables. Robust standard errors are in parentheses.
**p < .05, ***p < .01.
Second, we treat the level of poverty as a potential moderator that influences the negative spillover effect. Poverty is associated with higher levels of stress and chronic pain, which can lead to increased opioid use (Dasgupta et al., 2018). Indeed, the risk of filling an opioid prescription was 72% higher for the most deprived areas than the least deprived areas (Kurani et al., 2020). Related to this, the CDC shows that chronic pain and high-impact chronic pain are significantly more prevalent among adults living in or near poverty, raising exposure to and use of prescription opioids (CDC, 2018). The frequent use of opioids and their increased availability in deprived areas may create favorable conditions for opioid diversion, further accelerating the negative spillover effect. To test this issue, we retrieved poverty rate data from the U.S. Census Bureau and calculated the average poverty rate during the study period by each county. Then, we generated two variables, 
All other terms are defined as in the main specification (1). Column (2) of Table 7 shows that higher poverty intensifies the negative spillover effect. Specifically, the negative spillover effect of EPCS is positive and statistically significant in high-poverty areas but is statistically non-significant in low-poverty areas. These results suggest that the strength of the negative spillover effect depends on social conditions. Overall, the heterogeneous spread of the negative spillover effect, influenced by urbanization and poverty levels, can help social planners effectively allocate limited resources to vulnerable areas.
Finally, we examine the moderating effect of illicit drug accessibility. When a neighboring state adopts the EPCS mandate, drug seekers may cross state lines to obtain opioids from focal counties without EPCS mandates. However, implementation of stricter drug control measures, to help limit access to illicit drugs, will reduce the overall availability of drugs and opioids in the focal county and discourage individuals from obtaining opioids. By contrast, a focal county's lenient drug control measures are likely to encourage more drug shoppers to cross the border to obtain opioids. Consequently, the focal county's lenient regulations are likely to increase the negative spillover of neighboring states’ EPCS mandates. To test this conjecture, we calculated the average illicit drug usage rate during the study period by each state, retrieved from the Substance Abuse and Mental Health Services Administration. We implement the same model specification as in specification (4). In this analysis,
In this section, we investigate whether the observed results are mainly driven by drug users’ cross-border behavior in seeking opioids. If the negative spillover effect of EPCS is indeed due to drug users crossing state lines into neighboring counties without EPCS mandates, the negative spillover effect will be most prevalent in the bordering counties while diminishing as the distance from the border increases. The rationale is that drug users and/or doctor shoppers are more likely to visit bordering counties given the lower time and cost associated with crossing state borders. The greater the distance and the more time required to travel, the less motivated drug users are likely to be to make the journey.
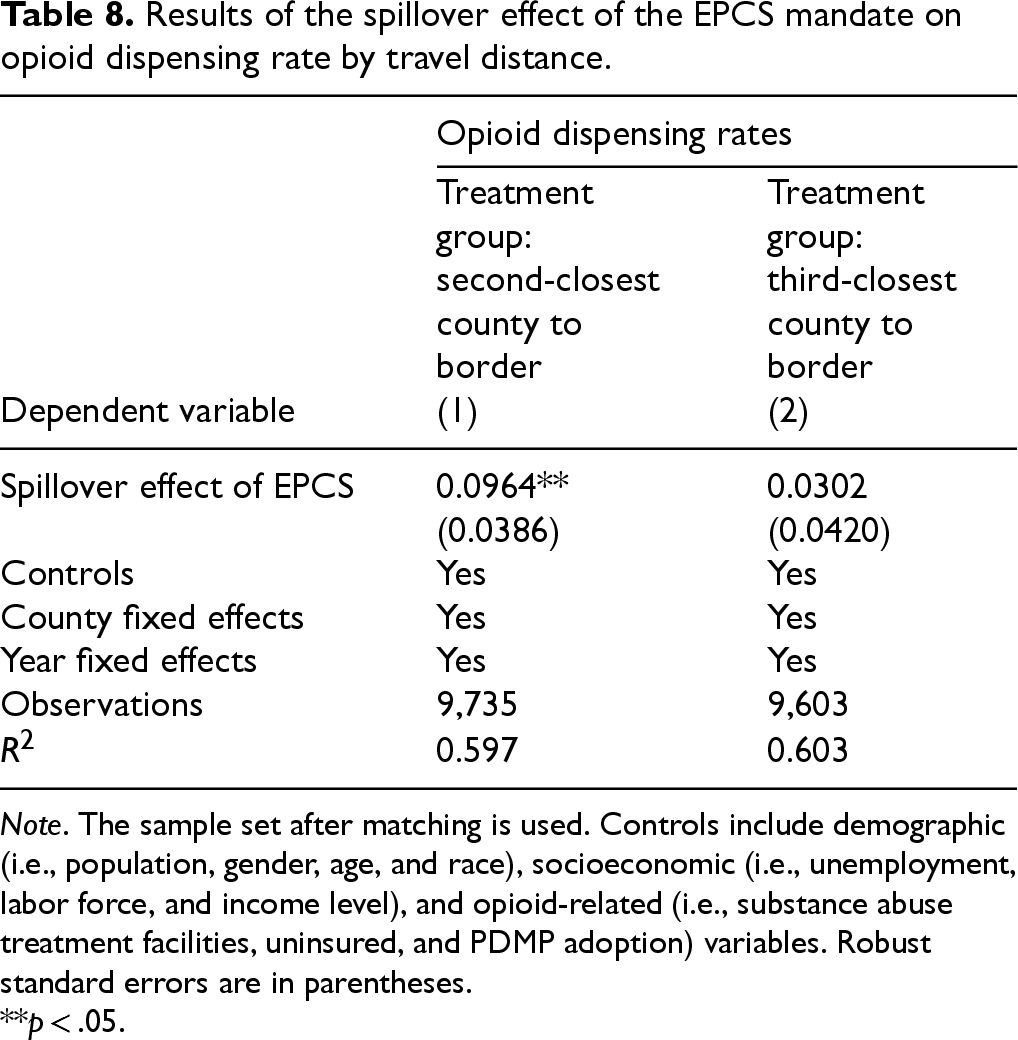
To test this conjecture, we constructed two treatment groups: one with counties in non-mandate states that are the second-closest to a mandate-state border at any point in time during the study period and one with counties in non-mandate states that are the third-closest counties to the border at any point in time during the study period. We re-estimate the models under each alternative treatment definition while holding the control group fixed. We assume the third-closest counties to have the highest cost of travel and the second-closest counties to face higher travel costs than the closest counties (i.e., our initial treatment group). Therefore, we expect the negative spillover effect of EPCS to weaken or turn non-significant in the second- and third-closest counties. To test this, we calculated the DID estimates separately for the second- and third-closest counties to the border. As Table 8 shows, the coefficients for the second-closest counties are positive and significant; however, third-closest counties become non-significant. These results suggest that the spillover effect is strongest in counties closest to the border and weakens as time and travel costs increase with distance. In other words, drug users are more likely to go doctor shopping in the border counties, which involve less travel distance and cost. These findings provide indirect evidence that the negative spillover effect of EPCS is likely driven by drug users crossing state lines to buy opioids in neighboring counties without EPCS mandates.
Results of the spillover effect of the EPCS mandate on opioid dispensing rate by travel distance.
Results of the spillover effect of the EPCS mandate on opioid dispensing rate by travel distance.
Note. The sample set after matching is used. Controls include demographic (i.e., population, gender, age, and race), socioeconomic (i.e., unemployment, labor force, and income level), and opioid-related (i.e., substance abuse treatment facilities, uninsured, and PDMP adoption) variables. Robust standard errors are in parentheses.
**p < .05.
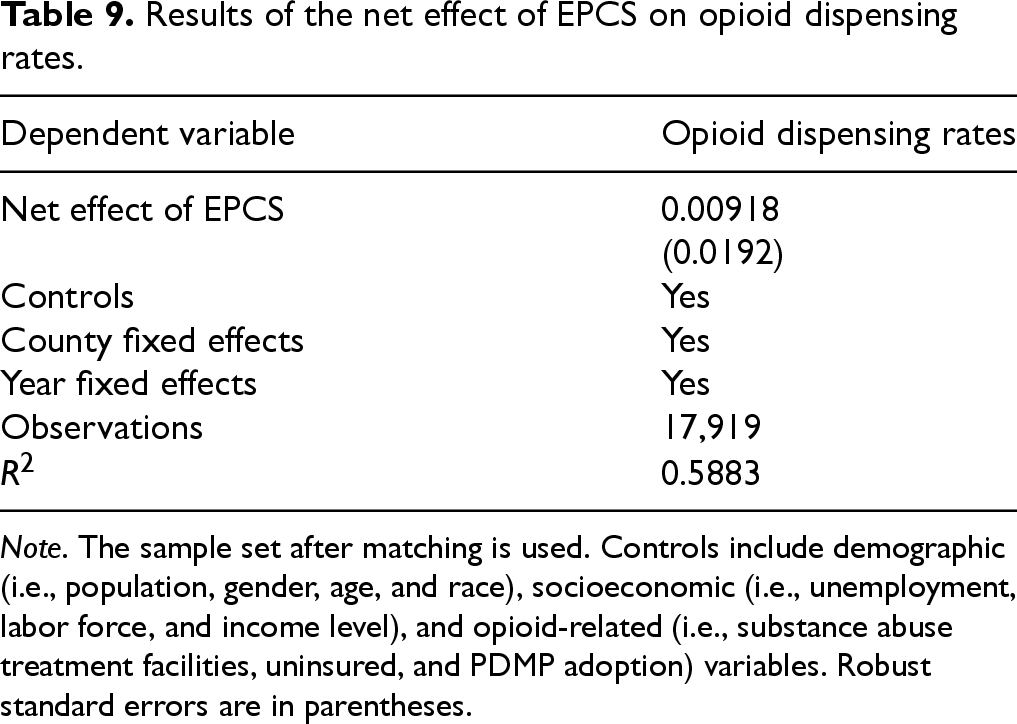
In this section, we estimate the net effect of EPCS mandates by combining both the direct and the spillover effects of EPCS. To this end, we restructured treated counties by including two groups: counties adjacent to states mandating EPCS (spillover effect group) and counties subject to EPCS mandates (direct effect group). By incorporating all counties positively and negatively affected by the EPCS mandates into a single treatment group, we capture the net effect of these mandates. The model specification is as follows:

Results of the net effect of EPCS on opioid dispensing rates.
Note. The sample set after matching is used. Controls include demographic (i.e., population, gender, age, and race), socioeconomic (i.e., unemployment, labor force, and income level), and opioid-related (i.e., substance abuse treatment facilities, uninsured, and PDMP adoption) variables. Robust standard errors are in parentheses.
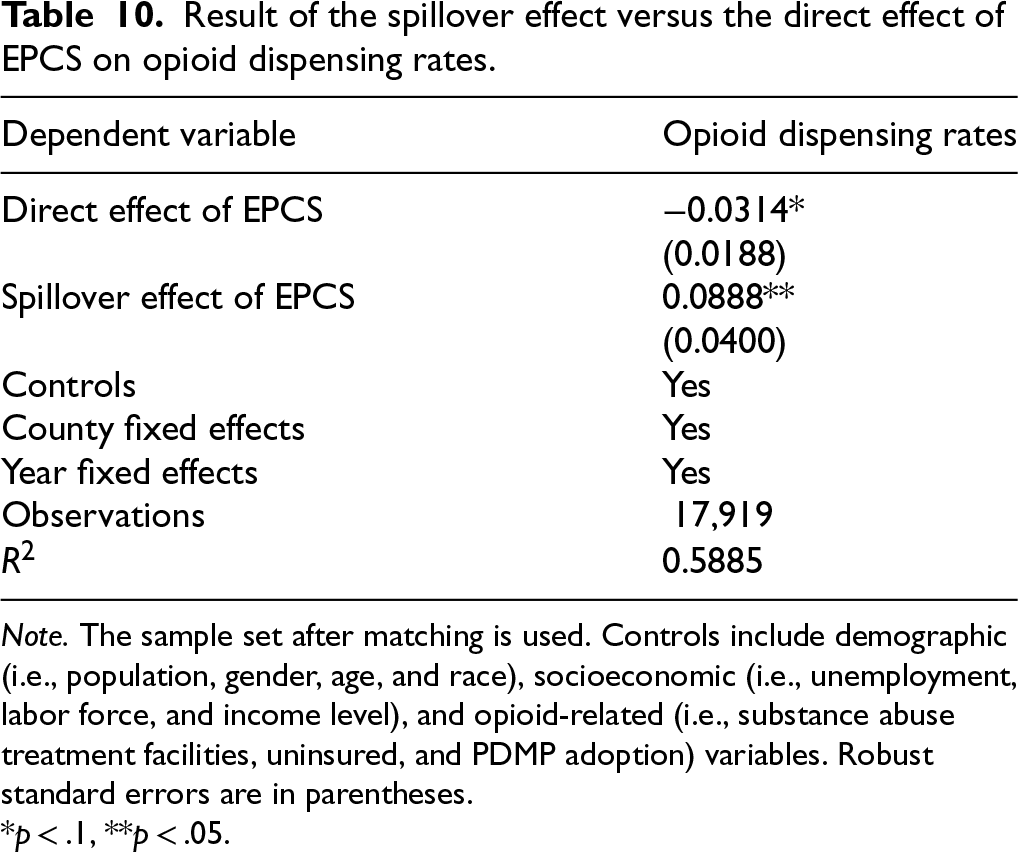
Next, we estimated the direct and the spillover effects in a single model to assess their relative strength. We implement the estimation with the following model:

Result of the spillover effect versus the direct effect of EPCS on opioid dispensing rates.
Note. The sample set after matching is used. Controls include demographic (i.e., population, gender, age, and race), socioeconomic (i.e., unemployment, labor force, and income level), and opioid-related (i.e., substance abuse treatment facilities, uninsured, and PDMP adoption) variables. Robust standard errors are in parentheses.
*p < .1, **p < .05.
We found that the EPCS mandate was associated with a reduction of approximately 3,114,054 opioid prescriptions annually in the mandated areas (i.e., direct effect group). However, this reduction appears to be largely offset by negative spillover effects, which are associated with an increase of approximately 3,758,860 opioid prescriptions annually in areas adjacent to states mandating EPCS (i.e., spillover effect group). Taken together, the overall effect of EPCS appears relatively modest, with an estimated net increase of 644,806 opioid prescriptions annually nationwide, potentially due to offsetting spillover effects. Although EPCS is designed to reduce opioid prescribing rates, our results show that the negative spillover effects are not minimal and may offset its intended effect. This finding validates the need for cross-state collaboration on EPCS and supports the importance of coordinated adoption both within and across states.
With the rapid increase of opioid overdoses, understanding the efficacy of supply-side policies to curb the opioid epidemic has moved to the forefront of attention of both health policymakers and researchers. In this study, we examine how the EPCS mandate and corresponding e-prescribing system use in a neighboring county affects the opioid dispensing rate in an adjacent focal county without an EPCS mandate, using a quasi-experiment of counties in the United States from 2010 to 2020. The findings indicate that the EPCS mandate of the neighboring county is associated with an increase in the opioid dispensing rate of the focal county without an EPCS mandate. However, the magnitude of this negative spillover effect is heterogeneous by social conditions such as urbanization, poverty levels, and accessibility to illicit drugs. Our findings also indicate that drug users tend to seek opioids in the nearest counties located on the border and are unlikely to cross more than two county lines to obtain opioid prescriptions. Moreover, the negative spillover effect of EPCS may attenuate the positive direct effects of EPCS mandates, potentially limiting their overall effectiveness.
Our study generates valuable insights for theory and practice. First, our work provides one of the first pieces of empirical evidence of the negative spillover effect of EPCS, and therefore contributes to the literature on how policy aims to boost health IT and corresponding health IT usage influences the opioid epidemic (e.g., Pang et al., 2021). Prior research on PDMP documents direct (Stucke et al., 2018; Sun et al., 2018) and spillover (Shen and Li, 2019) effects, whereas relatively little attention has been paid to EPCS (e-prescribing system use) or has evaluated it mainly for direct effects (Abouk and Powell, 2021; Danovich et al., 2019; Everson et al., 2020). To our knowledge, no study has examined spillovers from EPCS. Given that the mechanisms and roles affecting opioid prescribing under EPCS do not fully align with those under PDMP, an in-depth investigation of EPCS is warranted. Our study fills this missing piece by providing the first empirical evidence of a negative spillover from EPCS. Furthermore, prior studies on EPCS have focused on a single area (Abouk and Powell, 2021) or a specific group (Danovich et al., 2019). While these studies may provide a more nuanced understanding within their scope, our large-scale analyses provide a synthesized, system-level understanding of the efficacy of EPCS mandates.
Second, we go beyond prior studies on EPCS mandates by estimating the dynamic effects of EPCS using large-scale data, thereby advancing the debate on the effectiveness of supply-side policies in addressing the opioid epidemic. To our knowledge, our work is the first to examine the comprehensive effect of supply-side policy (i.e., EPCS) by considering both adopted and non-adopted neighboring areas. Given the substantial investments being made in EPCS mandates, which may fundamentally alter prescribers’ day-to-day routines (Everson et al., 2020), a rigorous assessment of their performance remains essential for both research and practice. Yet the existing literature evaluates EPCS primarily within adopted states, reporting positive or null effects in these areas only (Abouk and Powell, 2021; Danovich et al., 2019; Everson et al., 2020). Shen and Li (2019) test whether a supply-side policy (PDMP) has a negative spillover effect on opioid dispensing; however, their study is unable to tell whether this effect is large enough to offset the intended effect. While insightful, prior literature is unable to capture the dynamics across borders and therefore cannot tackle the policy's nationwide consequences. Our contribution extends this one-directional view with a two-channel, dynamic evaluation that jointly estimates the direct effect in adopting areas and the spillover effect in neighboring, non-adopting areas and traces both over time. Our results suggest that the negative spillover effect (higher dispensing in neighboring areas) may attenuate the positive direct effect (lower dispensing in adopting areas). Drawing on our findings, we urge cross-state implementation of EPCS mandates.
Third, our study is unique in that we provide insights into plausible mechanisms driving the negative spillover effect of EPCS mandates. Although Shen and Li (2019) investigate whether a supply-side policy (PDMP) has a negative spillover effect on opioid dispensing, insights into the underlying reason for this effect are lacking and thus warrant closer attention. We provide indirect evidence that individuals cross nearby borders to obtain opioids after their state's EPCS mandate. Because they seek to minimize time and effort, they are unwilling to travel long distances, and thus spillovers decline with distance. Furthermore, we provide an in-depth understanding of EPCS mandates by showing that EPCS's negative spillover effects are contingent on social characteristics. We offer evidence that the negative spillover effect is strengthened in areas with lenient illicit drug controls and in regions with high poverty levels. This knowledge can help regulators identify target areas and allocate limited resources to these vulnerable areas.
Our study offers practical implications. By providing indirect empirical evidence for cross-state travel of drug users, we inform policymakers about how policy interventions reshape drug and opioid use behavior. Extending the study of Gomes et al. (2012), who show that drug users engage in international border travel to exploit favorable drug policies, our study reveals cross-state travel for obtaining opioid prescriptions due to EPCS mandates. Our findings suggest that drug users tend to seek opioids in the nearest counties located in borderline states. Given that the travel costs between counties or from state to county are relatively lower than crossing international borders, as suggested by Gomes et al. (2012), we infer that the absence of EPCS in bordering counties creates a more accessible opportunity for individuals seeking opioid prescriptions, thereby intensifying prescription opioid misuse. Overall, our study underscores the importance of considering the behavior of the target group (e.g., drug users) when enacting state-run policy interventions.
Last, our findings advocate for integrated health IT adoption across regions and healthcare delivery organizations. Our findings suggest that the positive effect of EPCS (i.e., decreasing opioid dispensing rates in mandated areas) may be offset by negative spillovers in areas where EPCS mandates have not been implemented, leaving the net effect of EPCS mandates on opioid dispensing rates close to zero. Although EPCS is designed to reduce the opioid prescribing rate, our findings suggest that negative spillovers may be nontrivial, as they may offset the intended effect. This finding validates the need for cross-state collaboration on EPCS and supports the importance of coordinated adoption both within and across states. Overall, aligning health IT adoption with coordinated regulatory frameworks could provide an enhanced mechanism for surveillance, potentially offering a more comprehensive approach to reduce opioid prescriptions and thereby tackle the opioid crisis.
Our study has several limitations that provide opportunities for future research. First, we acknowledge that our findings are not based on a randomized experiment. Although we adopt an as-good-as-random shock and confirm the absence of heterogeneity across treatment and control counties in the pre-treatment periods, our study relies on a natural experiment setting. Second, we do not account for patterns related to alternative drugs to opioids. We therefore encourage future studies to incorporate the potential effects of opioid alternatives or other illicit drugs to unpack the dynamics of EPCS's impact. Third, we acknowledge that our sample may not be perfectly representative of the United States. We note that sample composition produces opioid-prescribing rates that are higher than the national average. Although empirical samples are necessarily defined by the focal research question, and we carried out robustness checks to benchmark against national patterns, the observed findings should be carefully interpreted. Finally, we conduct our analysis at the county level. Therefore, we call for future studies to use more granular geographic-level data to gain a nuanced understanding of the negative spillover effect.
Despite these limitations, this research sheds new light on the negative spillover impact of EPCS mandates on opioid dispensing rates. We hope that this work serves as a springboard for more sophisticated and deeper examinations of supply-side policies and health IT use to curb the opioid epidemic, to provide further implications for policymakers, practitioners, and researchers working to reduce the over-prescription of opioids.
Supplemental Material
sj-docx-1-pao-10.1177_10591478261442316 - Supplemental material for The negative spillover effect of electronic prescribing for controlled substances on the opioid epidemic
Supplemental material, sj-docx-1-pao-10.1177_10591478261442316 for The negative spillover effect of electronic prescribing for controlled substances on the opioid epidemic by Nakyung Kyung and Xiaoyu Liu in Production and Operations Management
Footnotes
Acknowledgments
The authors thank the Senior Editor and the anonymous reviewers for their valuable and insightful suggestions that significantly improved this research, and Jungpil Han for his constructive feedback and support on the early version of this paper. The paper benefited from valuable feedback from participants and discussants at the International Conference on Information Systems (ICIS).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a Start-up Grant from the National University of Singapore.
Notes
How to cite this article
Kyung N and Liu X (2026) The Negative Spillover Effect of Electronic Prescribing for Controlled Substances on the Opioid Epidemic. Production and Operations Management xx(x): 1–18.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.