
Abstract
The use of urgent care centers (UCCs) to reduce emergency department (ED) overuse has yielded mixed results in prior research. This paper investigates how the spatial proximity between UCCs and EDs drives heterogeneous effects of UCCs on ED demand. Using novel, granular encounter-level data from both EDs and newly opened UCCs within a major medical system, we leverage exogenous variation driven by institutional UCC operating hour policies to estimate causal effects. Through difference-in-differences models and generalized synthetic control methods, we find that collocated UCCs reduce ED demand for initial patient visits during UCC operating hours, with reductions spanning both nonurgent and urgent encounters. In contrast, non-collocated UCCs do not reduce ED demand. Such a difference is statistically significant. We identify queue sampling as the key mechanism driving these heterogeneous effects. Using timestamped arrival data, we show that higher ED waiting room census leads to increased arrivals at the collocated UCC, but only when the waiting room reaches visibly congested levels—in our setting, the top quintile of census distribution. This suggests patients exploit minimal switching costs to avoid observable congestion. This dynamic substitution pattern is absent at non-collocated sites, where transportation costs inhibit real-time facility switching. Our work sheds light on UCC location decisions and patients' facility choice behavior in an era of rapid UCC market expansion. For hospital managers, we show that when reducing ED demand is a primary objective, opening UCCs collocated with EDs proves substantially more effective than establishing them elsewhere in the region. For policymakers, while current UCC siting discussions focus primarily on expanding geographic access, our results demonstrate that carefully considering UCCs’ spatial configuration relative to EDs can unlock additional operational benefits beyond long-term access improvements.
Keywords
Introduction
The overuse of hospital emergency departments (EDs) has been a long-standing concern for healthcare providers and policymakers. Inefficient ED use contributes to longer wait times, worse emergent outcomes, and increased healthcare costs (NEHI, 2010; Soltani et al., 2022). A key driver of ED overuse is patients with less urgent conditions seeking treatment at an ED. One important approach to diverting these patients away is to provide cost-effective alternatives outside the ED. One widely used model is the urgent care center (UCC). According to the American Academy of Urgent Care Medicine (AACUM, 2022),
“In many ways the Urgent Care Center (UCC) is similar in some of the scopes of practice of your primary care physician, but differs in that typically the UCC can provide X-rays on-site, provide laceration repairs for minor injuries, and can do minor casting. Depending on the staffing model, some may be capable of offering simple blood tests and intravenous fluids. …Urgent Care Centers are open for extended hours, in general 12 hours a day on average …Typically, you can be seen quicker at the Urgent Care Center for minor ailments than in the hospital emergency department with a much lower co-pay and other inherent costs such as facility fees that raise costs. ”
Given their scope and lower costs, UCCs appear well-positioned to absorb less urgent ED visits. However, the choice between ED and UCC is more complex than it seems. Patients weigh not only perceived urgency, but also perceived capabilities and convenience as well as monetary and time costs.
The mixed evidence on whether access to UCCs reduces low-acuity ED visits highlights the complexity of patients’ facility choice. Some studies report significant reductions in ED use—ranging from 2.69% to 17.2% (Allen et al., 2021; Pacheco et al., 2019)—while others find no effect (Carlson et al., 2020; Yakobi, 2017). These inconclusive findings suggest a need to examine the determinants and mechanisms underlying UCC effectiveness. We focus on one such factor: the relative location of the UCC and the ED.
Specifically, we ask whether a UCC located adjacent to an ED is more effective in reducing ED demand during its operating hours than one located several miles away. If so, what mechanisms drive the shift in patient choice? Health systems routinely debate and make opposing choices of whether UCCs should be adjacent to EDs or instead distributed geographically (NHS England, 2023). Given the long-standing concern over ED overuse and the rapid growth of UCCs—expanding at 7% annually in the United States (Meyersohn, 2023), our research questions are important to both care providers and policymakers from the planning stage of new UCCs.
We collaborate with a large medical system operating hospitals with EDs and stand-alone UCCs in a major metropolitan area. Between 2013 and 2017, this system opened three new UCCs—in November 2013, June 2016, and November 2017. All three UCCs offer a similar limited range of services as described above: they treat nonurgent to urgent encounters only, have no inpatient units or observation units, and provide resources including labs and X-rays. However, they differ in proximity to the nearest EDs: one is located 0.1 miles away (directly across the street), one 0.7 miles away, and one 5.7 miles away. The closest UCC, within a 3-minute walk of the ED, is effectively collocated with the ED. We exploit this variation in proximity to study whether spatial configuration leads to UCCs’ differential impacts on ED demand.
The UCCs are open roughly 12 hours per day. Each UCC opening thus potentially introduces a shift to the diurnal arrival pattern at nearby EDs: prior to the opening, patients have limited choices; afterward, a UCC offers an alternative to the ED for part of the day. Because UCC operating hours are standardized and fixed across sites over our sample horizon, the setting provides a quasi-experimental opportunity to identify the causal effect of UCC availability on ED demand during UCC operating hours. We exploit two sources of variation: ED demand before vs. after UCC openings, and ED demand during vs. outside preset UCC operating hours. To estimate treatment effects, we implement both a difference-in-differences (DiD) model and a generalized synthetic control (GSC) method (Xu, 2017).
We observe novel, granular encounter-level data from both EDs and newly opened UCCs, spanning approximately one year before and after each UCC opening. Unlike prior studies that focus solely on ED visits and use only ED data, this dual-facility data allows us to examine not only the causal impact of UCCs on ED demand during their operating hours, but also to uncover the mechanisms—shaped by the physical proximity between UCC and ED—that drive the differential effects of UCCs on ED utilization.
We begin by empirically showing that the UCC collocated with an ED significantly reduces that ED’s demand during its operating hours, while the non-collocated UCCs do not. Specifically, during UCC operating hours, the collocated UCC shifts 3.9% of patients away from the ED as their first point of care. This substitution effect is attenuated but remains statistically significant after accounting for rerouted patients who initially visit the UCC and subsequently join the ED: total ED volume during UCC operating hours decreases by 3.0%. (More formally, these estimates capture the incremental impact of an additional UCC, given that other UCCs already operate in the local market.) When broken down by acuity, the collocated UCC reduces ED visits by 3.1% among urgent cases and by 46.1% among nonurgent cases, indicating that substitution spans a range of urgency levels. A back-of-the-envelope analysis shows that the patients substituting UCC for ED during UCC operating hours could lead to a $2.2 million ED cost reduction per annum.
In contrast, the non-collocated UCCs show no significant effect on patients’ initial care choice during UCC operating hours. However, when rerouted patients (from UCC to the ED) are included, we observe an increase in total ED demand, particularly among urgent cases. This increase is driven by same-day follow-up at the ED after the non-collocated UCC visit, rather than by changes in patients’ initial facility preferences.
The heterogeneous impact of UCCs on ED demand further motivates us to investigate the underlying mechanism—specifically, how physical proximity shapes patient behavior. We find evidence that patients take advantage of the negligible transportation cost between the ED and the collocated UCC to engage in real-time queue sampling. Using granular timestamp data for both ED and UCC arrivals, we analyze patient choices at 15-minute intervals and show that higher ED waiting room census leads to increased arrivals to the UCC. This pattern reflects dynamic decision-making: patients are more likely to opt for the collocated UCC when the ED appears visibly congested. We find no such relationship between ED crowding and UCC arrivals at the non-collocated sites. These findings suggest that queue sampling is a key mechanism driving the heterogeneous effects of UCCs on ED demand, and that it is only enabled when the UCC is sufficiently close to the ED to allow low-cost switching at the point of care.
To the best of our knowledge, we are among the first to examine how the spatial proximity between EDs and UCCs shapes patient choices between the two types of facilities. Furthermore, we leverage novel, granular encounter-level timestamp data from both UCCs and EDs to not only quantify the heterogeneous effects of UCCs on reducing ED demand by proximity but also to uncover the underlying mechanism: patients engage in real-time queue sampling, dynamically adjusting their facility choice based on observed ED congestion. While prior studies have focused on how UCC availability affects patients’ long-term care access, our findings complement this literature by showing that, beyond availability alone, UCC location choices influence ED demand through short-term (same-day), real-time substitution between facilities.
Literature Review
Our work contributes to two streams of literature: efforts to reduce ED overuse through alternative care options and the role of facility location.
Addressing ED Overuse: Access to Alternative Facilities
To reduce unnecessary ED visits, many healthcare providers and policymakers have turned to expanding access to lower cost, alternative care options, including primary care, retail clinics, and UCCs. However, the evidence on whether such alternatives reduce ED demand has been mixed.
These studies rely on geographically aggregated data and define UCC “exposure” at the ZIP code, catchment area, or regional level. This approach treats all UCC–ED pairs within an area as equivalent, regardless of their actual spatial relationship. Such aggregation risks masking important heterogeneity in patient behavior and facility substitution patterns, especially since, as discussed below, locations are known drivers of patients’ facility choices. This calls for more granular investigation into how specific spatial configurations shape ED demand and facility choices.
One exception is Carlson et al. (2020), which examines whether proximity to a UCC, defined as living within 1 mile, affects a patient’s likelihood of visiting the ED for a low-acuity condition. The outcome is binary: whether an ED visit is low-acuity, and the independent variable is also binary: whether the patient making the visit lives within 1 mile of any UCC. Using encounter-level data in two EDs and a logistic regression model, the authors find mixed results: a lower odds of low-acuity ED visits among patients living within 1 mile of a UCC at one medical center, and no significant effect at another. This design essentially estimates whether proximity affects the type of ED visits patients make, but not whether total ED demand changes; a shift in odds does not necessarily imply a reduction in volume. In line with Carlson et al. (2020), we contribute to the literature on location heterogeneity in UCC effects, but our research question differs. We estimate the heterogeneous causal impact of UCC on total ED arrivals by ED–UCC proximity during UCC operating hours, especially among lower acuity patients.
More importantly, examining UCC impact through patient–UCC proximity or regional-level UCC availability, as in Carlson et al. (2020) and the aggregate-level studies, addresses a different set of questions and yields different practical implications than our focus on ED–UCC proximity. Patient–UCC proximity speaks to how long-term care-seeking behavior is shaped by the greater cost-effectiveness and geographic accessibility of a UCC relative to an ED. In contrast, our ED–UCC proximity analysis holds constant these inherent cost and convenience advantages of UCCs and asks whether UCCs’ spatial configuration relative to the ED has additional effects on ED demand.
Our study complements long-term access-focused analyses by showing that facility siting itself can influence patient choices between EDs and UCCs in ways that the general features of UCCs and patient–UCC proximity—such as lower cost, shorter waits, and no appointment requirements—cannot fully explain. From a policy and planning perspective, our work offers new insight for facility location design: two UCCs may serve the same population and provide similar long-term access benefits, yet their impact on ED demand can differ markedly depending on their spatial configuration relative to the ED. Particularly, a collocated setup may unlock additional UCC impact by removing frictions that hinder switching between facilities.
Collocating Facilities and Spatial Configuration
The importance of facility location in shaping service outcomes has been well-documented. Stahl (1982) finds that collocated facilities and sellers reduce customers’ search costs. The benefit of collocation is considered to be particularly salient when service requires visual inspection and when service heterogeneity is high (McCann and Folta, 2008). These findings suggest that physical proximity may enable real-time decision-making—behavioral patterns that are unlikely to arise when facilities are spatially separated.
Several studies have examined the impact of physically collocating healthcare facilities. Collocating a psychiatric emergency center and a general ED reduces wait time for psychiatric patients (Frank et al., 2005); collocating mental and physical health resources reduces patient length of stay, readmission rate, and suicidal behavior (Ahuja et al., 2026). In the context of the British National Health Service, collocating walk-in centers 1 alongside EDs does not seem to bring in evident changes in ED patient volume in one study (Salisbury et al., 2007). Later work in a different city, however, does find an 8% reduction in nonurgent ED attendances (Arain et al., 2015).
Only two studies, to the best of our knowledge, have directly examined the collocated UCC–ED configuration. Raidla et al. (2020) show that managing one triage line across the collocated UCC and ED leads to a decrease in length of stay and door-to-doctor time of the patients triaged to the UCC. In our setting, patients choose the facility for themselves as opposed to being directed through a triage process. Agarwal et al. (2012) conducted an interview focusing on why patients first present to the ED despite being eligible for UCC care. Neither of the two studies estimates the causal impact of UCC proximity on ED volume.
Compared to the extensive literature examining how UCCs and other alternative facilities affect ED demand at an aggregate level, there is limited empirical work on whether the impact of UCCs varies by their spatial proximity to EDs. Yet this potential heterogeneity is important: understanding how physical proximity shapes patient choice has direct implications for system-level decisions on where to place new UCCs and how to configure them relative to existing EDs. We address this gap by comparing the effects of collocated and non-collocated UCCs on ED demand during UCC operating hours, offering new insight into how location-specific design choices influence patient facility choice outcomes.
Research Question: Proximity and Patient Facility Choice
Whether ED–UCC proximity leads to different patient behavior is not clear a priori. If patients make care decisions entirely before arrival and based solely on static criteria such as clinical condition, monetary costs, and geographic convenience to patient location—then the spatial relationship between the ED and UCC may have little impact. However, if patients are also responsive to factors such as perceived capability of facility types or (perceived) wait time (Agarwal et al., 2012; Durand et al., 2012; Turnbull et al., 2019: p. 25), then ED–UCC proximity may meaningfully shape patients’ facility choices. Prior studies offer evidence for both types of considerations in patient decision-making.
On one hand, if all current ED patients believe their medical needs cannot be met by UCCs and if clinical need is the sole driver of facility choice, then neither a newly opened collocated nor non-collocated UCC would serve as a substitute. In this case, UCC openings would have no effect on ED demand, regardless of proximity. Patient interviews suggest that proximity to home or work is a major factor in choosing the ED, even when patients acknowledge that their condition does not require emergency care (Agarwal et al., 2012). When a UCC, whether collocated with the ED or not, opens near these convenience-driven patients, offering an even more geographically accessible and lower cost option, they may opt for the UCC instead of the ED. In this scenario, both collocated and non-collocated UCCs could reduce ED volume by serving as more convenient and cost-effective alternatives, but in a similar manner, yielding no differential impact by proximity. Thus, in either case, ED–UCC proximity would not result in heterogeneous outcomes.
On the other hand, if patients make real-time decisions upon arrival to the ED, ED–UCC proximity may lead to heterogeneous impacts on ED volume. Multiple interview studies (Agarwal et al., 2012; Durand et al., 2012; Turnbull et al., 2019: p. 25) indicate that many less severe patients choose the ED not because of clinical need, but because of uncertainty—they are reassured by the availability of diagnostic tools in EDs (e.g., X-rays) and the opportunity to receive care in one place. For these patients, the ED serves as a safe default when they are unsure whether their condition warrants emergency treatment (Turnbull et al., 2019: p. 53). When such patients arrive at an ED with a collocated UCC, they retain the reassurance that their condition will be addressed at the site, but face lower switching costs between the two facilities. This flexibility allows them to postpone their final choice of facility until they can assess the situation on-site. As Vice President of Intuitive Health—a Texas-based firm whose business model centers on collocating EDs and UCCs—Mason Deal explains, collocated models spare patients from the burden of deciding where to go for appropriate care before seeking treatment (Mugford, 2020). In this way, the collocated UCC effectively gets a second look, serving as a fallback that can draw patients away from the ED once they arrive.
We expect that ED congestion is likely to prompt such final facility decisions. In particular, patients who initially enter the ED may observe a crowded waiting room and reconsider their choice. While our partner’s EDs do not communicate expected wait times, patients can infer congestion from the visible census. At a collocated site, this may prompt them to switch to the adjacent UCC, especially when the perceived benefits of ED care no longer justify the cost of delay. In contrast, such dynamic substitution is unlikely at non-collocated sites, where switching to a UCC requires nontrivial travel. Therefore, the added benefit of collocation arises precisely from its ability to accommodate uncertain, delay-sensitive patients who are not fully committed to the ED and are responsive to real-time conditions.
This leads to our primary research question: How does the proximity of a UCC to an ED affect patient substitution between the facilities during UCC operating hours? Further, if there is an effect, what mechanism leads to the substitution? We are among the first to examine how ED–UCC proximity shapes patients’ facility choices. Whereas prior studies treat UCC openings as exogenous shocks and focus solely on ED volume changes using encounter data from the ED alone, we go further: analyzing both ED and UCC arrivals and uncovering the mechanism by which UCC proximity affects ED use.
Empirical Setting and Data
To explore our research question, we collaborate with a major medical system. In this section, we introduce our empirical setting and data.
Overview of the Hospital-based EDs
At our partner medical system, EDs operate 24 hours a day. Upon arrival to the ED, patients check in and wait to be called to the triage desk, where a triage nurse records their chief complaints and vital signs. The triage nurse then assigns an acuity level to the patient following the Emergency Severity Index (ESI) algorithm. Acuity levels range from 1 to 5, corresponding to immediate, emergent, urgent, less urgent, and nonurgent, respectively. Lower scores generally indicate more severe cases. Acuity levels 1 and 2 reflect distinctly higher urgency than levels 3, 4, and 5. Levels 3, 4, and 5 are distinguished mostly by the number of types of resources (e.g., labs, X-rays, electrocardiogram, etc.) required to make a diagnosis (Gilboy et al., 2005). Lower scores involve more required resources. Level 5 requires no resource, while Levels 4 and 3 require at least one type of resource.
After triage, patients return to the waiting area and wait to be called to the treatment area. No wait time information is disclosed to the patients. The waiting and treatment areas are physically separated; importantly, the treatment area is not visible to patients from the waiting area. The triage nurses manage the patient flow from the waiting area to the treatment area and assign patients to care teams. Once inside the treatment area, the patient occupies an ED bed and is treated by providers affiliated with the assigned team.
The care team is responsible for evaluating the patient and ultimately making a diagnosis and disposition decision. The physician’s disposition decision determines whether the patient will be discharged, admitted (into the inpatient unit for follow-up care), or transferred (to other healthcare facilities). Patients who are discharged—those requiring no further care—typically leave the ED shortly after the disposition decision is made. In contrast, patients who require follow-up care (i.e., will be admitted or transferred) remain in the ED until an inpatient bed becomes available or transportation to the receiving facility is arranged. During the time between the physician’s admission or transfer decision (i.e., bed request) and the patient’s actual departure from the ED, the patient will be boarding in the treatment area.
Overview of the UCCs
UCCs are not new to the residents who live in and around the metropolitan area we study. Across healthcare systems, UCCs in the region offer similar ranges of services and maintain comparable operating hours.
UCCs operated by our partner medical system are physically separate from EDs. They operate between 8:00 a.m. and 7:45 p.m. or 8:00 p.m., seven days a week, offering a limited range of services. In particular, UCCs treat nonurgent to urgent (acuity levels 3 to 5) encounters such as minor illness (e.g., cold, flu, sore throat, diarrhea), minor injuries (e.g., cuts, bites, sprains), and common issues like pink eye, urinary tract infections, and skin irritations. To support diagnosis and treatment, UCCs are equipped with some resources such as labs and X-rays. However, UCCs do not offer any observation units or in-hospital services. If a physician deems a patient’s condition too severe to be managed at the UCC, the patient will be redirected to an ED. The operating hours, service scope, and test capabilities reflect nationwide standards for UCCs, as summarized by the American Academy of Urgent Care Medicine (AACUM, 2022) and referenced in Section 1. Conversely, ED care providers cannot divert ED patients to a UCC.
Information about UCCs mentioned so far is readily available online. Physicians have also contributed to raising awareness of UCC service capabilities, limitations, and their relative time and cost advantages. As a result, patients should be familiar with the hours and scope of UCC services.
UCC Openings and ED–UCC Pairs
We observe three UCC openings in our focal medical system between 2013 and 2017: November 2013, June 2016, and November 2017. 2 For each UCC, we identify the ED in the medical system that is geographically closest to it. As we will elaborate further in Section 3.4 and Figure EC.1, we show that each UCC opening has limited (indeed, for most cases, negligible) impact on EDs other than the closest ED. We therefore define each newly opened UCC and its nearest ED as a pair. The focus of our study is how differences in the relative location of each ED–UCC pair lead to heterogeneity in the UCC’s impact on ED demand.
The distances between the UCCs and their paired EDs (in chronological order of their openings) are 0.7 miles, 5.7 miles, and 0.1 miles, respectively, based on the driving distance according to Google Maps. For the third ED–UCC pair, the 0.1-mile distance amounts to a 3-minute walk from door to door, effectively negligible. For the other two pairs, transportation between the facilities imposes a non-negligible cost. We refer to the third pair as collocated, and the remaining pairs as non-collocated.
To publicize a UCC opening, the medical system announces it through local news outlets, social media (e.g., Facebook), and highly visible banners placed at the facility. Note that all UCCs in our setting, whether collocated or non-collocated, are operated within the same system and therefore have identical monetary costs, all lower than ED costs. Insurance coverage is the same across all UCC–ED pairs, as both UCCs and EDs are part of the same medical system. Against this backdrop, two questions arise: Do patients switch away from EDs when a new UCC opens? And does the relative proximity of the two facilities influence patients’ facility choices? To address these questions, we obtain encounter-level data surrounding the three UCC openings from our partner medical system.
Data Description
Our partner medical system collects data through its electronic health record (EHR) systems. We focus on encounters made by adult patients at both EDs and UCCs.
To comply with our partner medical system’s data privacy policy, all encounter dates were deidentified prior to analysis. Specifically, within each sample, each unique date is assigned a binary indicator for whether it falls before or after the sample UCC opening date. Dates are then randomly shuffled within each sample, with each date retaining all of its encounters and the binary label. For example, if two encounters in our data fall on Date 1 and Date 2, the visit dates alone do not reveal which one actually occurred first, unless one was before the paired UCC opened and the other after.
Although the chronological ordering of dates is obscured, two key sources of variation are fully preserved. First, within-day arrival patterns remain intact: all encounters on a given date do show the actual time of the day and therefore retain their relative ordering within the day. Second, the binary indicator identifying whether each date falls before or after the sample UCC opening date is retained. Our empirical strategy (Section 4.1) exploits these two preserved features of the data.
Combining the unique patient identifier with the preserved within-day timestamps enables us to track a patient’s movements across facilities within the same day. For instance, if a patient visits an ED and a UCC on the same day, we can observe the timing of their arrival at each facility. Among dates following UCC opening, 49.2% had at least one patient who visited both the sample UCC and the collocated ED on the same day; the corresponding figure for the non-collocated ED was 41.1%. This provides evidence of patient flow between UCCs and EDs, suggesting that UCC openings can plausibly influence ED demand. We further observe each patient’s ESI acuity level, admission source, and disposition decision.
Particularly, for each window and its corresponding sample, we first identify all patients who visited the sample UCC inside the window. We then examine the ED encounters made by these patients and calculate the share of those encounters that occurred at each ED in the medical system. We label the EDs as “Nearest,” “Second Nearest” to the sample UCC ranked by the UCC–ED relative distance. All other EDs are labeled as “Others.” We find that sample UCC patients almost exclusively flow to the nearest ED, that is, focal ED by our definition, in samples 1 and 3 (
Empirical Strategy
Identification Strategy
The discussion thus far highlights key features of our data: (1) we observe three separate samples, each centered on a different UCC opening and including encounters from both the sample UCC and all EDs in our partner medical system; (2) within each sample, we observe granular ED arrival timestamps for all encounters before and after the UCC opening, although the actual calendar dates are obscured, with only a binary indicator denoting before- versus after-opening. Our identification strategy builds on these data features. We start by describing our identification strategy within each sample; our main specification then pools across the three samples for estimation.
Instead, we adopt a within-day difference-in-differences (DiD) framework to estimate the causal effect of UCC openings on ED patient arrivals during UCC operating hours. In each sample, there is one focal ED (the nearest to UCC), as discussed. We exploit two sources of variation in this focal ED: (1) UCC operating hours (8 a.m. to 8 p.m., which we refer to as daytime) versus non-operating hours (8 p.m. to 8 a.m., which we refer to as nighttime), and (2) dates before versus after UCC opening. For the bulk of our analysis, we work with 15-minute intervals. Our unit of analysis is ED
Our estimator leverages this policy-driven temporal discontinuity by comparing ED arrivals during UCC operating hours with arrivals during non-operating hours, within the same date. Because the operating schedule is not chosen in response to short-run demand fluctuations, there is no inherent reason for untreated potential outcomes to exhibit a discontinuous change at the operating-hour boundary. That is, absent UCC operations, the treated–control difference in ED arrivals should not shift specifically at the operating-hour boundary. Therefore, any divergence between treated and control dates that emerges specifically at the boundary is unlikely to reflect other coincident changes, and instead points to UCC availability. This institutional feature ensures that the treatment switch itself is exogenous to local ED demand conditions.
Second, the comparison across dates eliminates confounders that affect overall ED demand but are unrelated to the within-day pattern. As we compare each ED to itself before and after UCC opening, time-invariant ED characteristics are differenced out. Moreover, by focusing on a 1-year window before and after each UCC opening, we limit exposure to slow-moving changes in, for instance, patient composition and behavior. Over a relatively short horizon, it is less likely that features of the ED or its underlying patient base change sharply enough to generate differential time-of-day patterns unrelated to UCC operations.
Unlike a multi-ED DiD design that compares different EDs, our identification does not exploit variations across EDs. UCC placement across EDs may reflect strategic planning considerations and therefore raise concerns about endogenous treatment at the ED level, potentially biasing cross-ED estimates. By instead exploiting within-ED variation in UCC operating status, holding the ED fixed, and using a predetermined on/off schedule, our design avoids this source of selection bias.
Variable Construction
Independent Variable
The treatment in our identification strategy is the operating status of the UCC. Depending on the relative distance between the UCC and the ED, there are two types of treatments in our analysis: operating collocated UCC and operating non-collocated UCC. We therefore denote
ED Demand Outcomes
We denote
First, the daily number of initial encounters, denoted as
Second, we analyze the total daily number of ED encounters, including both initial visits and those rerouted from UCCs, denoted as
Model-free Evidence
We first present model-free evidence in Figure 1, which shows one subfigure for each sample. The facet labels show the distance (in miles) between the focal ED and UCC in the sample. The horizontal axis plots the hour of day. The vertical dashed line at 8:00 a.m. marks the time when UCC operations begin, and treatment is considered “switched on.” For each hour, we calculate the average number of less severe encounters during that hour across 1) control dates (dates before UCC opening), and 2) treated dates (dates after UCC opening). We then apply a log transformation to each of the two averages and compute their differences: the logged average on treated dates minus the logged average on control dates. The vertical axis plots the resulting differences. This difference in logs is consistent with a Poisson model—a log link function applied to a conditional mean—which we adopt to model counts in our main specification.
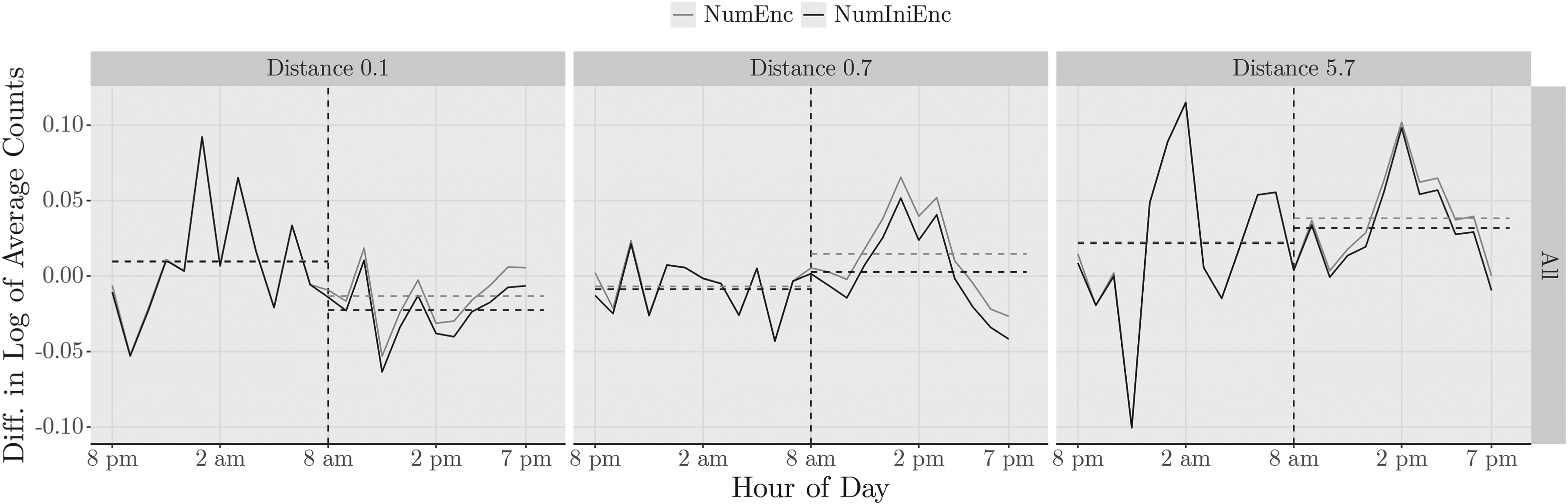
Model free evidence: ED encounters before vs. after UCC opening.
Figure 1 shows that less severe encounters decrease in the ED that is collocated with a UCC (Distance 0.1). The reduction in patients’ initial ED visits (
In Table 1, we report means and standard deviations for the outcome variables, stratified by operating status (operating or non-operating hours), date types (before or after a UCC opening), and UCC types (collocated or non-collocated). We also provide the mean and standard deviations of the daily share of encounters by acuity and the daily number of encounters at the sample UCCs. ED arrivals during non-operating hours (nighttime) are highly stable before and after UCC opening: for collocated EDs, nighttime encounters average changed from 44.0 to 44.4 per day; for non-collocated EDs, it changed from 27.9 to 27.8. In contrast, differences appear primarily during operating hours (daytime): when a collocated UCC opens, daytime ED arrivals decline from 87.0 to 84.6, while non-collocated case exhibits a modest increase.
Summary statistics.
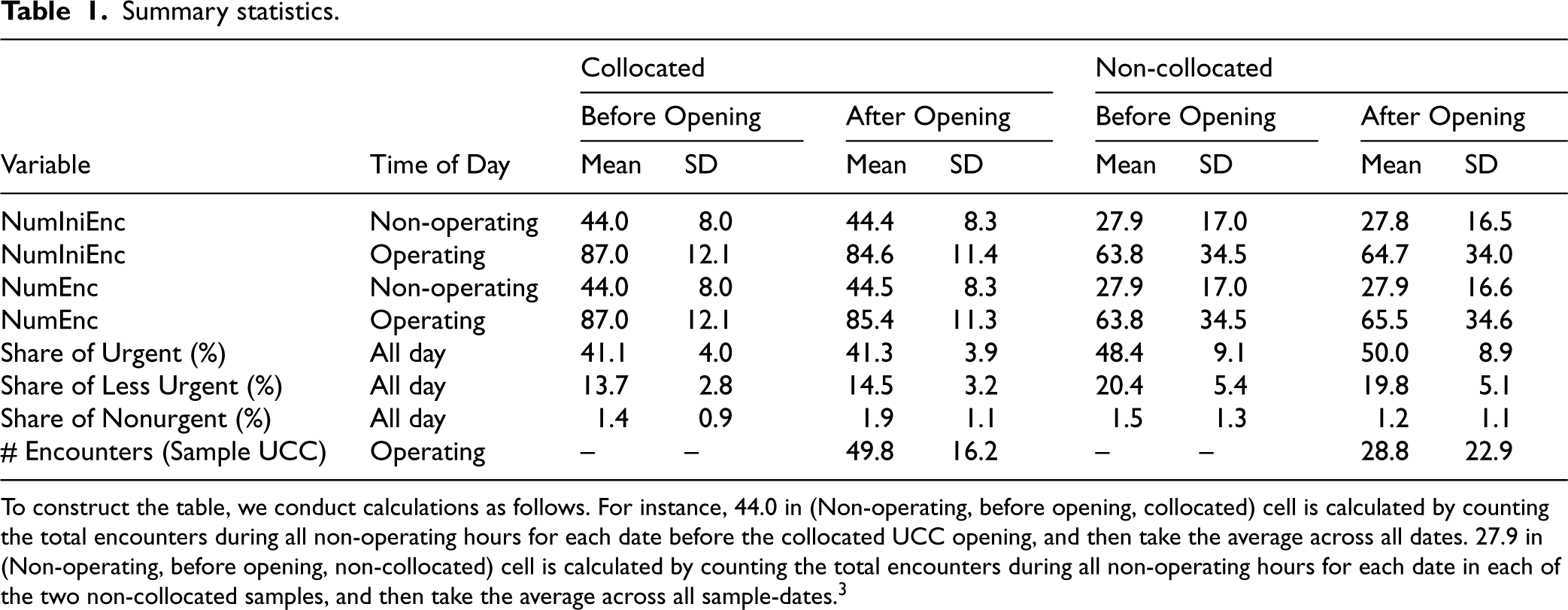
To construct the table, we conduct calculations as follows. For instance, 44.0 in (Non-operating, before opening, collocated) cell is calculated by counting the total encounters during all non-operating hours for each date before the collocated UCC opening, and then take the average across all dates. 27.9 in (Non-operating, before opening, non-collocated) cell is calculated by counting the total encounters during all non-operating hours for each date in each of the two non-collocated samples, and then take the average across all sample-dates. 3
Formally, we stack all dates observed across the three samples and estimate the following specification:

The outcome variable
We also include additional covariates in
Second, we control for system-wide demand fluctuations using two covariates measured at the ED
To model the number of arrivals in 15-minute intervals, we employ a count model and obtain a Poisson quasi-maximum likelihood estimator (QMLE). Using Poisson regression to model counts is common in the operations literature (Li et al., 2022). Our coefficients of interest are
Conditional on the fixed effects and covariates described above, our identifying assumption, as discussed in Section 4.1, is that there are no shocks that coincide with dates of UCC openings (treated versus control dates) and alter the within-day distribution of ED arrivals, in particular, the arrival pattern over operating versus non-operating hours. This is an analogue of the parallel-trends assumption in canonical DiD designs, which assumes that there are no shocks coinciding with treatment timing that differentially affect treated and control units. Although not directly testable, we conduct extensive plausibility checks of our identifying assumption, including pre-trends tests on non-operating hours in Section 6.1, relaxing the strict requirement of a stable within-day arrival pattern absent UCC operations by implementing the generalized synthetic control method (Xu, 2017) in Section 6.2, and addressing alternative demand- and supply-side shifts that might alter within-day arrival patterns and confound our estimate in Section 6.3.
The Impact of UCCs on ED Demand
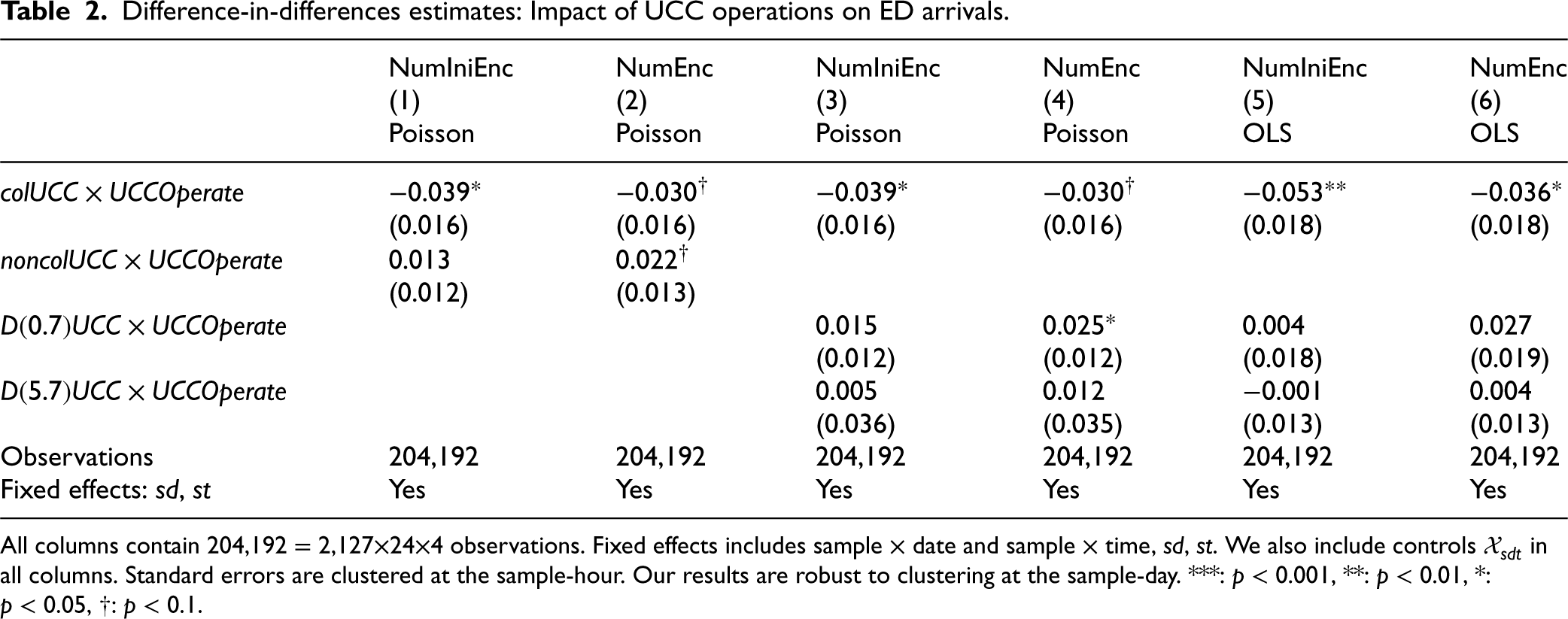
We begin by investigating percentage changes in ED arrivals for patients with acuity levels 3 to 5 during UCC operating hours. The results are reported in Table 2.
Difference-in-differences estimates: Impact of UCC operations on ED arrivals.
Difference-in-differences estimates: Impact of UCC operations on ED arrivals.
All columns contain 204,192 = 2,127
For overall ED patient arrivals
In contrast, for the non-collocated UCC, we find no significant decrease in total ED arrivals; in fact, the coefficient for
Our goal is to assess whether collocated and non-collocated UCCs have significantly different impacts on ED demand. To this end, we compare the coefficients on the interaction terms
The heterogeneous impact of UCCs on ED demand remains robust when examined by distance. When the UCC is located 0.7 miles away from the ED, we observe an increase in total ED arrivals and no effect in the initial ED arrivals (see coefficients of
Difference-in-differences estimates: Impact of UCC operations on ED arrivals (by acuity).
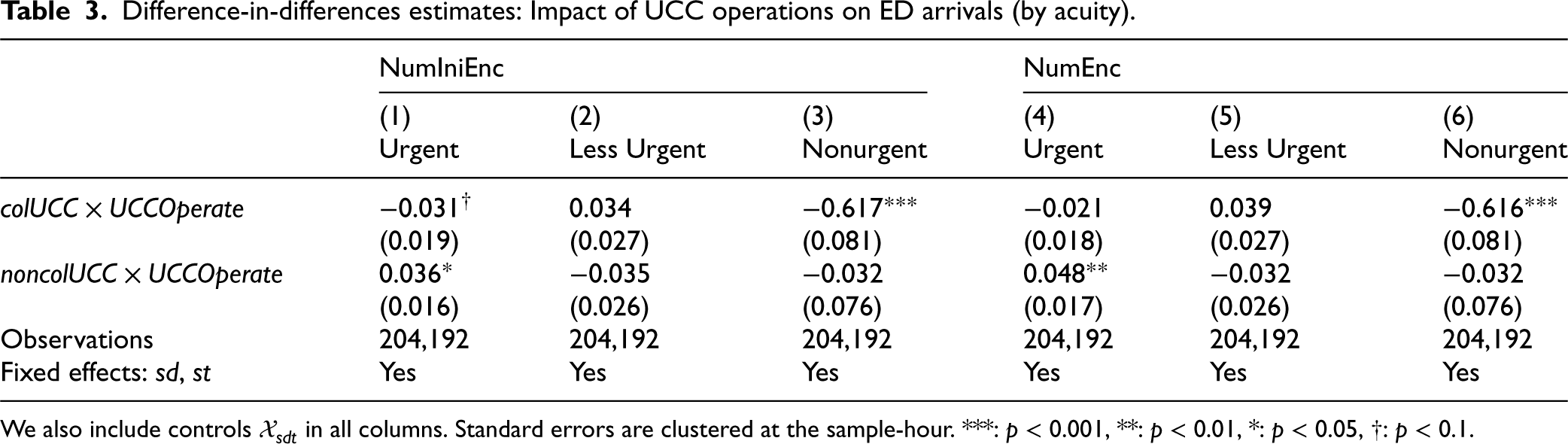
We also include controls
Table 3 column (3) shows that the opening of a collocated UCC leads to 46.1% fewer nonurgent encounters per 15-minute interval during UCC operating hours. The effect is consistent for urgent encounters as well. Table 3 column (1) shows a 3.1% reduction per 15-minute interval. These effects correspond to approximately 2 fewer urgent and 1 fewer nonurgent patient per day during UCC operating hours.
To contextualize the impact, we conduct a back-of-the-envelope annual ED cost savings analysis. The observed reductions imply roughly 3 fewer patients would choose ED as their initial care facility each day during UCC operating hours. 4 At an average cost of $2,256 per ED visit and an average cost of $220 per UCC visit among lower-acuity cases (Burke, 2026), this yields approximately $2.2 million in annual cost savings. When same-day rerouted visits are included, the results remain directionally consistent, though attenuated. For non-collocated UCC, we observe statistically insignificant changes in less urgent and nonurgent cases (columns (2) and (3) of Table 3), but a significant and positive coefficient for urgent cases (column (1) Table 3). The urgent cases increase by 3.7% after a non-collocated UCC opening during UCC operating hours. Overall, collocated UCCs demonstrate greater success in reducing ED volume compared to non-collocated UCCs. Importantly, however, the absence of ED volume reduction should not be interpreted as evidence that non-collocated UCCs have limited value. The positive coefficients for urgent encounters are consistent with the possibility that non-collocated UCCs play a different role. They may expand access by bringing patients into the healthcare system who would otherwise have forgone care, some of whom may subsequently require ED follow-up.
We next examine the mechanisms that explain why collocated UCCs successfully facilitate switching encounters away from the ED, whereas non-collocated UCCs do not.
Our variable
The first column in Table 4 reports the Poisson regression results. We find that the coefficient of lagged EDWaitRoomCensus is positive and significant (
Poisson QMLE and 2SRI estimates for queue sampling mechanism analysis.
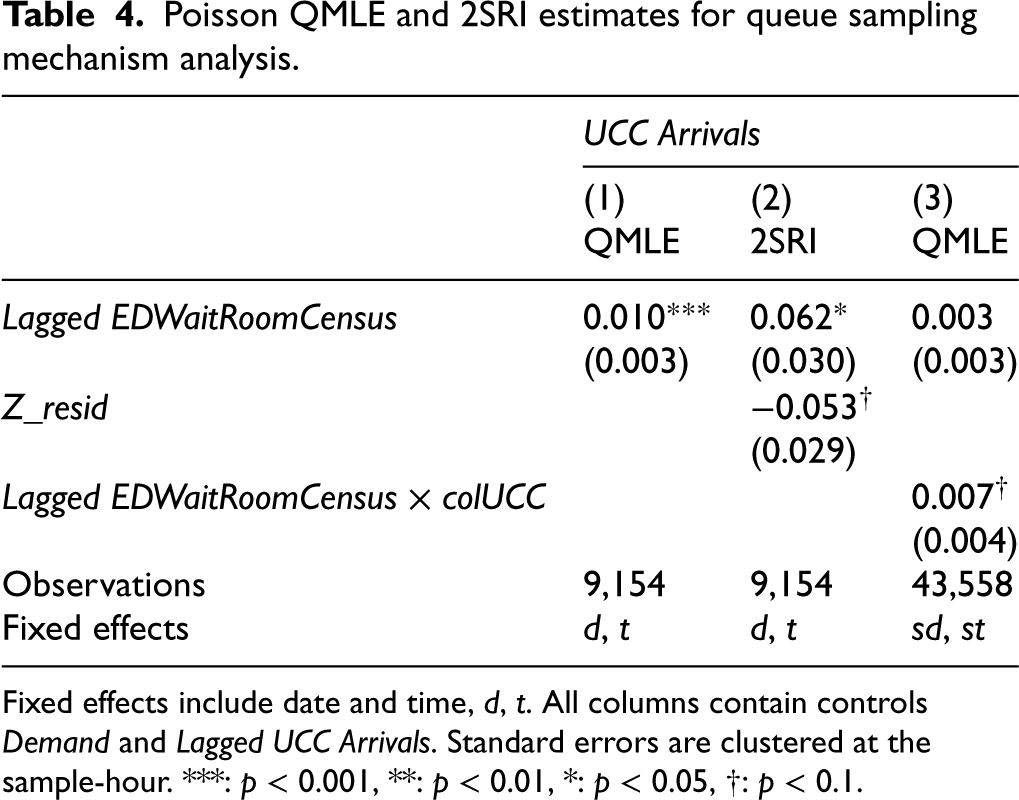
Fixed effects include date and time,
We use lagged
For this IV to be valid, it must satisfy the relevance and exclusion restriction conditions. The
For the exclusion restriction to hold, the instrument must be uncorrelated with unobserved drivers of UCC arrivals conditional on our controls and fixed effects, and it must affect UCC arrivals only through its impact on ED waiting-room census. We next address the primary channels through which this condition could be violated and explain why the exclusion restriction is plausible in our setting.
One concern is that unobserved demand shocks may simultaneously drive both ED boarding counts and UCC arrivals, thereby violating the exogeneity of our instrument. Our specification mitigates this concern at multiple time levels. First, we include date fixed effects, which absorb all date-level demand fluctuations, including flu outbreaks, weather shocks, and seasonal patterns that may simultaneously influence ED and UCC arrivals. Consequently, any remaining unobserved demand variation must occur within a given day. To address such within-day shocks, we further control for total hourly arrivals to the ED–UCC pair and the time-of-day fixed effects, which capture short-run fluctuations in aggregate demand.
At still finer time intervals, events might cause sudden, localized demand shocks that simultaneously increase ED boarding and UCC arrivals. The lag structure of our instrument mitigates this concern. Specifically, ED boarding census at time
Finally, the ED waiting area and the boarding area are physically separated in our setting, and arriving patients in the waiting area do not observe the number of boarded patients. Therefore, substitution to the UCC is unlikely to be directly influenced by boarding census. These features, namely, controls and fixed effects, the lag structure, and the physical separation between the waiting and boarding areas, collectively support the plausibility of the exclusion restriction in our setting. We acknowledge, however, that the IV estimate still rests on the remaining identifying assumption that, conditional on date fixed effects, hourly demand controls, and time-of-day fixed effects, lagged ED boarding census affects current UCC arrivals only through lagged ED waiting-room census.
Using this IV, we estimate a two-stage residual inclusion model. The 2SRI approach is preferred over the traditional two-stage least squares (2SLS) when the second-stage model is nonlinear, as it produces consistent estimates (Terza et al., 2008). This method suits our context, as our second-stage model is a Poisson regression for a count outcome. We write the first stage regression in equation (3), and the second stage regression in equation (4).
Consistent with the model without an IV, the coefficient for
To test for nonlinear effects, we modify model (2) and replace the continuous measure of
The coefficients of
To this end, we estimate model (2) on all three ED–UCC pairs. In particular, we modify model (2) by interacting
Our findings carry two important implications for practitioners and policymakers. First, we document that the effectiveness of UCCs in reducing ED demand is not uniform—it depends on physical proximity to the ED. While previous work and public discourse often focus on placing UCCs based on regional population needs or ZIP code-level access gaps, our findings highlight that relative positioning between UCCs and EDs is also important. If the goal is to relieve overuse at a particular ED, placing a UCC collocated with that ED is far more effective than adding a UCC elsewhere in the region. Our findings speak to an ongoing and unsettled debate over whether expanding access to UCCs meaningfully reduces ED demand. Our study offers new insight into when and how UCCs can serve as an effective lever to reduce ED demand during UCC operating hours.
Second, we identify queue sampling—patients observing ED crowding and switching to the collocated UCC in real time—as a plausible mechanism driving the heterogeneous treatment effects by ED–UCC proximity. Importantly, patients switch from ED to UCC only when the ED is visibly congested, precisely when reducing ED demand is most needed, and when the UCC is collocated. An additional analysis shows that census count is a highly significant positive predictor of door-to-provider wait time (see Section EC.4.7), suggesting that patients responding to census congestion are, in effect, responding to a wait time signal. This points to a practical implication: posting real-time wait times in the ED waiting room could lower the cognitive burden of queue sampling and encourage more real-time switching to a collocated UCC. Because queue sampling reflects a general behavioral trade-off between waiting time costs and switching costs among other factors, this mechanism and the resulting substitution across facilities in a collocated setup are likely generalizable beyond our specific healthcare facility.
These insights have clear operational and policy relevance. For hospital managers, collocated UCCs should be viewed not merely as standalone facilities but as flexible capacity extensions that can absorb less severe, delay-sensitive patients during periods of high ED demand. Our findings offer one empirical lens on the ongoing debate over whether UCCs should be collocated with the ED or distributed geographically: we empirically show that when the goal is to relieve demand at a specific ED, proximity matters. Furthermore, the local markets where our ED–UCC pairs are located already had UCCs in operation prior to the new UCC openings. Our estimates therefore reflect the incremental impact of an additional UCC. Notably, the collocated UCC was introduced last and in the setting with the highest baseline UCC density (see Section EC.5), suggesting that any diminishing marginal benefit of UCC access would bias our estimate downward. This makes our estimated reduction conservative: even in an area already served by several UCCs, collocation still proves effective in alleviating ED demand during its operating hours. This setting mirrors today’s healthcare landscape, where new UCCs almost always enter regions with existing facilities. Our findings therefore speak directly to the practical question of whether adding a collocated UCC continues to deliver meaningful relief for ED demand when the UCC operates.
Whereas prior work has emphasized long-term effects of UCC availability on future ED use, our study demonstrates that ED–UCC proximity can further shape real-time patient decisions under congestion. By identifying queue sampling as a facility choice mechanism enabled by collocation, we clarify not just whether UCCs reduce ED demand, but when and why they do, providing actionable guidance for both facility planning and daily ED operations. As the UCC market continues to grow, identifying locations that support seamless, real-time switching of patients from the ED may unlock the full potential of UCCs as tools for ED congestion relief during UCC operating hours.
Identifying Assumption and Robustness Checks
We present robustness checks that test the internal validity of our main findings presented in Section 5.1. We begin by assessing the plausibility of our key identifying assumption: absent UCC operations, the difference in ED arrivals between treated and control dates (i.e., dates after and before UCC opening) would be stable across time-of-day intervals. First, we analyze pre-trends on non-operating hours and assess the within-day comparability of ED arrivals (Section 6.1). Second, we estimate a generalized synthetic control model (Xu, 2017) to relax the strict stability requirement (Section 6.2). Third, we provide additional evidence to address alternative mechanisms that could shift within-day diurnal patterns (Section 6.3).
More robustness checks and placebo tests are presented in the E-companion. In Section EC.4.4, we examine the robustness of our results to alternative covariate sets, time binning choices, and parametric assumptions. We also show that our results are directionally consistent with estimates from two benchmark comparisons: a before-and-after UCC opening comparison and a cross-ED comparison. In Section EC.4.5, we conduct placebo tests to ensure that our identification strategy does not detect effects where none should exist. These comprehensive checks reinforce the credibility of our main findings.
Pre-treatment Parallel Trends and Within-day Comparability
Both pieces of evidence suggest that the arrival pattern of treated and control dates has a stable difference during non-operating hours. Particularly, in the collocated sample, leads-and-lags coefficients show that the divergence between treated and control dates emerges specifically from when UCC starts operating (EC.4.1), is sustained during UCC operating hours, and is absent during non-operating hours. This is consistent with UCC operations driving the change in arrival patterns.
Generalized Synthetic Control: Relaxing the Parallel Trends Assumption
Although our DiD estimator passes the pre-treatment trend tests in Section 6.1, those tests only detect confounders that meaningfully shift non-operating hour arrival patterns. A confounder that gradually alters within-day patterns may not be strong enough to be detected by standard pre-trend tests. Furthermore, these pre-trend tests cannot inform the pattern during operating hours. To address both of these concerns, we implement the generalized synthetic control (GSC) proposed by Xu (2017). We use the GSC framework to flexibly model unobserved confounders that vary across time of day and alter within-day arrival patterns.
In particular, the GSC framework accounts for these confounders through an interactive fixed effects (IFE) model with latent factor components. The IFE model is estimated using only the control dates, recovering the latent factors and their factor loadings, and therefore learning the within-day arrival pattern (trajectory) on control dates. For each treated date, the factor loadings are estimated by projecting the non-operating hour outcomes onto the latent factor space identified from control dates. The counterfactual operating-hour pattern is then imputed using the estimated IFE model together with the estimated date-specific factor loadings. This approach is valid as long as non-operating hours are informative of operating hours on the same date. That is, the within-day arrival pattern is a coherent whole, such that a treated date’s non-operating hour pattern is mostly sufficient to locate it within the latent factor space learned from control dates. Such within-day coherence is plausible given the comparable patient composition across operating and non-operating hours shown in Section 6.1.
Formally, let
Examining Alternative Mechanisms
So far, Section 6.1 tests for confounders that would manifest in non-operating hours; Section 6.2 further addresses confounders whose effects on within-day arrival patterns can be captured by the latent factors in control dates. These checks progressively narrow the space of viable confounders. Combined with the controls in model (1), any remaining confounding variation would need to be an ED-specific, volume-independent shock that coincides with dates after UCC opening and the specific 8 a.m. operating-hour boundary. In this section, we examine specific mechanisms that could plausibly generate such a variation.
We return to the discussion in Section 4.3. Non-operating-hour ED demand remains highly stable before and after UCC opening, whereas changes occur primarily during operating hours. This pattern suggests that our estimated effects are driven by changes during UCC operating hours, with limited evidence of substantial substitution from non-operating hours. To further address this concern, we redefine our indicator
We can further assess this concern through door-to-provider times (the time from arriving at the ED waiting room to the time leaving the ED waiting room), using them as a proxy for staffing and workflow conditions. Using the same specification as our main analysis with average door-to-provider time as the outcome, we find that door-to-provider times decrease during UCC operating hours at the collocated ED (
Given the stability during non-operating hours, any confounding variation in patient mix or patient behavior that differentially affects day versus night would need to coincide precisely with both dates after UCC opening and the specific 8 a.m. operating-hour boundary. Such a confounding event is unlikely in our setting, except for patient behavior shifts directly induced by UCC availability—patients’ timing substitution around the operating-hour boundaries, which we addressed above. Finally, we note that this assumption is standard in difference-in-differences designs. In a canonical cross-ED DiD, patient mix stability must hold along the calendar-time dimension and can only be assessed through pre-treatment trends. Our design in fact imposes a stricter requirement: any confounding change must coincide with not only the calendar date of UCC opening but also the specific time-of-day window of UCC operation.
Conclusion
Whether opening a UCC reduces ED overuse has been the subject of ongoing debate; we contribute new evidence by showing that this impact depends critically on spatial proximity between UCC and ED. Using granular, timestamped ED encounter-level data across multiple UCC openings, we exploit institutional policies on UCC operating hours as exogenous variation and estimate both difference-in-differences and generalized synthetic control models. We find that, during UCC operating hours, collocated UCCs reduce nonurgent-to-urgent encounters choosing the ED as their first point of care by 3.9%, while non-collocated UCCs have no detectable effect. Formal hypothesis testing confirms that the impact of collocated UCCs is both statistically significant in isolation and significantly stronger than that of non-collocated UCCs.
A distinctive feature of our data is that we observe timestamped encounters from not only the EDs but also the newly opened UCCs. Leveraging this, we investigate why proximity matters. We show that when ED waiting rooms are visibly crowded—specifically, in the top quintile of their census distribution—arrivals to a collocated UCC increase, whereas no such relationship exists for non-collocated sites. These findings support a behavioral mechanism of queue sampling: patients assessing ED congestion on site and diverting to the UCC when switching costs are minimal. In this way, UCCs function as operational levers to absorb lower-acuity, delay-sensitive patients who have not fully committed to ED care upon arrival at the ED. Because this responsiveness to time costs reflects general human decision-making, our findings that a collocated setup encourages more patients to switch from ED to UCC during ED congestion are likely generalizable.
Our results highlight proximity as a key determinant of UCC effectiveness in reducing ED demand. For hospital managers seeking to reduce ED overuse, collocated UCCs can serve as capacity expansions with limited capability for lower-acuity cases during UCC operating hours, particularly during ED congestion. For policymakers planning future UCC sites, current discussions often focus on population coverage and regional UCC accessibility; our findings suggest that spatial configuration relative to EDs is also important. Collocation enables real-time facility switching, offering benefits beyond the long-term access gains.
Although our primary focus is on substitution under collocation, our findings are also consistent with the possibility that non-collocated UCCs may expand healthcare access, in line with prior work (Magnolfi et al., 2024). This interpretation also aligns with our exploratory comparison of total system volume, defined as the combined ED and UCC encounters at each ED–UCC pair, before and after UCC opening: total volume increases for both collocated and non-collocated pairs (see Section EC.4.9). However, since we cannot rule out cannibalization of primary care or other care modes by the UCC, this evidence of access expansion remains suggestive. Richer data, including full records of patients’ healthcare interactions and preserved calendar dates over a longer horizon, could rigorously test whether UCCs serve as an entry point for previously untreated patients and decompose the extent to which UCC openings expand access versus redistribute demand across facilities depending on ED–UCC proximity.
Supplemental Material
sj-pdf-1-pao-10.1177_10591478261468124 - Supplemental material for Proximity Matters: The Impact of Urgent Care Centers on Emergency Department Arrivals
Supplemental material, sj-pdf-1-pao-10.1177_10591478261468124 for Proximity Matters: The Impact of Urgent Care Centers on Emergency Department Arrivals by Simin Li, Achal Bassamboo and Martin A Lariviere in Production and Operations Management
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. This work was supported in part by the Northwestern Medicine Enterprise Data Warehouse.
Notes
How to cite this article
Li S, Bassamboo A and Lariviere MA (2026) Proximity matters: The impact of urgent care centers on emergency department arrivals. Production and Operations Management x(x): 1–20.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.