
Abstract
While many studies have investigated the consequences of psychological safety for behavior, there is little theorizing on the mechanisms that account for these effects. Since psychological safety makes individuals feel safe to express their true self, we argue that it should act as a catalyst for alignment between individual beliefs and behavior. Drawing on the reasoned action model, we postulate that psychological safety interacts with individuals’ attitudes and perceived norms in predicting intention and behavior. We tested our model with physicians’ influenza vaccination behavior. We surveyed 208 physicians from a Swiss hospital before and after the vaccination phase. Results show that the effect of attitude, but not perceived norm, on intention to get vaccinated was moderated by perceived psychological safety in the physicians’ team: High psychological safety strengthened the effect of physicians’ attitude on their intention, which in turn predicted actual vaccination behavior. We provide first evidence that high psychological safety may render individuals more comfortable to act in accordance with their attitudes. Depending on whether attitudes are in line with organizational goals, increasing psychological safety could facilitate positive or negative consequences. This more differentiated understanding of psychological safety can fruitfully inform both future research and organizational practice.
Psychological safety—defined as a belief that it is safe to take interpersonal risks in a team (Edmondson, 1999)—is widely considered an important team climate that yields several beneficial outcomes for the team and its members as well as for organizations (Edmondson & Lei, 2014; Frazier, Fainshmidt, Klinger, Pezeshkan, & Vracheva, 2017; Newman, Donohue, & Eva, 2017). Among these effects are increases in speaking up or voice (e.g., Bienefeld & Grote, 2014; Detert & Burris, 2007), reporting of patient treatment errors (Leroy et al., 2012), learning behavior in teams (e.g., Edmondson, 1999; Kostopoulos & Bozionelos, 2011), perceived quality of care (Stühlinger, Schmutz, & Grote, 2019), and general team performance (Schaubroeck, Lam, & Peng, 2011). The vast body of literature on psychological safety’s beneficial effects stirs practitioners in one direction—increasing psychological safety in their teams.
However, we currently know little about psychological safety’s potential detrimental effects (Newman et al., 2017). Only very few studies have considered unintended effects that may be engendered or facilitated by psychological safety. Pearsall and Ellis (2011) investigated unethical behavior in student teams and found that utilitarianism—an ethical orientation aimed at maximizing the utility or pleasure for actors (Mill, 1863)—was more strongly associated with team cheating behavior in teams with high rather than low psychological safety. Deng, Leung, Lam, and Huang (2019) developed and tested a conceptual model with two effect paths with one of them explicating that psychological safety may lower group average work motivation and thus impair group risk-taking behaviors such as learning behavior. These first findings on detrimental effects of psychological safety illustrate how important it is to better understand the construct’s mechanisms of action. If creating or enhancing psychological safety may not only facilitate speaking up or learning behaviors but also increase unethical behavior and decrease work motivation, this will be very important information for practitioners.
In order to understand if and how psychological safety may engender detrimental effects, a theory on how psychological safety affects individual behavior is needed. While a number of theories have been used to explain specific relationships between psychological safety and other constructs (e.g., social learning theory or social exchange theory; see Newman et al., 2017), there is still little work on psychological safety’s theoretical underpinnings.
With our study, we aim to contribute to the psychological safety literature by presenting and testing a fundamental theoretical model on how psychological safety affects individual behavior. In our model, the individual behavior will not be restricted to desirable behavior—it will also allow to predict undesirable behavior. First, we flesh out a general theoretical model on psychological safety’s mechanisms of action. We draw on the reasoned action model (RAM; Fishbein & Ajzen, 2010) as the basic theory to predict individual behavior and explain how psychological safety acts as a moderating climate which interacts with individuals’ attitudes and perceived norms to shape behavior. Based on Kahn (1990), who has found that psychological safety allows individuals to express their true selves, we argue that psychological safety should act as a catalyst for alignment between individual beliefs and behavior. The fundamental notion is that if the individual beliefs are desirable or beneficial, psychological safety will facilitate desirable or beneficial behavior. However, if individual beliefs are undesirable or detrimental, the behaviors that psychological safety will facilitate will be also.
Second, we put the proposed model to the test by applying it to an individual behavior of high social relevance: influenza vaccination behavior of physicians. Not getting vaccinated can pose health risks for healthcare workers themselves but more importantly can endanger patients. Research has shown that vaccinated healthcare workers have a lower incidence rate of influenza infections than unvaccinated healthcare workers (Kuster et al., 2011) and that higher vaccination rates of healthcare workers are associated with lower mortality in elderly patients (Carman et al., 2000; Hayward et al., 2006; Lemaitre et al., 2009; Potter et al., 1997). We gathered real-life data from a local hospital on physicians’ individual beliefs on influenza vaccination and their vaccination behavior in order to see if our theoretical model could predict this safety-relevant behavior and what role psychological safety plays in it. Hence, we offer theoretical insights into the mechanisms underlying the effects of psychological safety and also provide empirical evidence for those mechanisms in a highly relevant application domain using real-life data.
Psychological Safety and Reasoned Action
Psychological safety is widely understood to constitute a specific climate, which allows individuals to feel safe to challenge the status quo in their social context, for example, by speaking up about errors or by suggesting changes (Edmondson & Lei, 2014). It permits “to show and employ one’s self” (Kahn, 1990, p. 708) without fear of negative consequences, such as feelings of embarrassment triggered by others’ reactions. We argue that in order to better understand the mechanisms by which psychological safety influences individual behavior, the relationship between individual beliefs, intentions, and behavior in social contexts should be examined. To this end, we will first explicate the RAM, which constitutes the foundation of our research model, and apply it to our chosen context of physicians’ influenza vaccination behavior. In a second step, we will explain psychological safety’s role in predicting individual behavior.
The RAM (Fishbein & Ajzen, 2010) is among the best-known theories for predicting behavior. With “reasoned action model” or “RAM,” we refer to the newest formulation of the theory by Fishbein and Ajzen (2010). Its earliest form was the theory of reasoned action (Ajzen & Fishbein, 1980; Fishbein & Ajzen, 1975), which was developed to predict behavior under volitional control. Later, it was extended by perceived behavioral control to the theory of planned behavior (Ajzen, 1991), which could also be used to predict behavior not fully under an individual’s control. The current form of the RAM includes little tweaks over the theory of planned behavior such as a broadened definition and renaming of the subjective norm into the perceived norm (Fishbein & Ajzen, 2010). Over the last decades, the RAM has (in its various forms) been found to predict a wide range of behaviors (Albarracin, Johnson, Fishbein, & Muellerleile, 2001; Armitage & Conner, 2001; Godin & Kok, 1996), such as losing weight (Schifter & Ajzen, 1985), pro-environmental behavior (De Leeuw, Valois, Ajzen, & Schmidt, 2015), or entrepreneurship (Kautonen, van Gelderen, & Fink, 2015). The core assumptions of the RAM are that attitudes toward a behavior, perceived norms, and perceived behavioral control predict an individual’s intention to engage in a specific behavior, which in turn predicts the individual’s actual behavior (Ajzen, 1991; Fishbein & Ajzen, 2010). A positive attitude—that is, a positive evaluation of the behavior and its anticipated outcomes—will make an individual intend to act out that behavior. Perceived norms create pressure to (not) perform a behavior (Fishbein & Ajzen, 2010). These norms can be injunctive—what other people consider the right thing to do—or descriptive, that is, what most people actually do (Cialdini, Kallgren, & Reno, 1991; Cialdini, Reno, & Kallgren, 1990). Finally, perceived behavioral control over performing (or not performing) a behavior influences the intention to perform that behavior (Ajzen, 1991; Fishbein & Ajzen, 2010). In the RAM, perceived behavioral control is also used as a proxy for actual control, which acts as a facilitator in the relationship between an individual’s behavioral intentions and actual behavior (Fishbein & Ajzen, 2010).
Predicting Influenza Vaccination Behavior of Physicians
We applied the RAM to influenza vaccination behavior of physicians (see Figure 1). We chose this behavior because it is clear-cut (getting vaccinated or not), highly relevant, and happens in a social context which is suitable to test the role of psychological safety in the prediction of individual behavior. Coworkers are usually aware of each other’s vaccination status and may challenge individuals for their decision to get vaccinated or not, creating a situation of interpersonal risk. In addition, some healthcare workers fear vaccine side effects or question the vaccine’s effectiveness (e.g., Abramson & Levi, 2008; Heimberger et al., 1995). Therefore, physicians can develop different attitudes toward influenza vaccination. While the seasonal influenza vaccination is mandatory in some US hospitals, it is only recommended in others (Greene et al., 2018), including most hospitals in Switzerland and other European countries (Galanakis, D’Ancona, Jansen, Lopalco, & Gatekeepers, 2014; Maltezou & Poland, 2014). Since physicians are free to get vaccinated or not, the behavior is under volitional control of the individual and perceived behavioral control less important. Due to this and, more importantly, because we did not anticipate perceived behavioral control to be affected by psychological safety, we did not include perceived behavioral control as a predictor of intention in our model.1 The RAM has been used in previous studies to predict vaccination behavior of healthcare workers (Cornally et al., 2013; Godin, Vézina-Im, & Naccache, 2010; Kung, 2013), which shows that the model can be applied to vaccination behavior. Hypothesized moderated mediation model. Note. H7 signifies the moderated indirect effect from (a) attitude and (b) perceived norm through intention to vaccination behavior.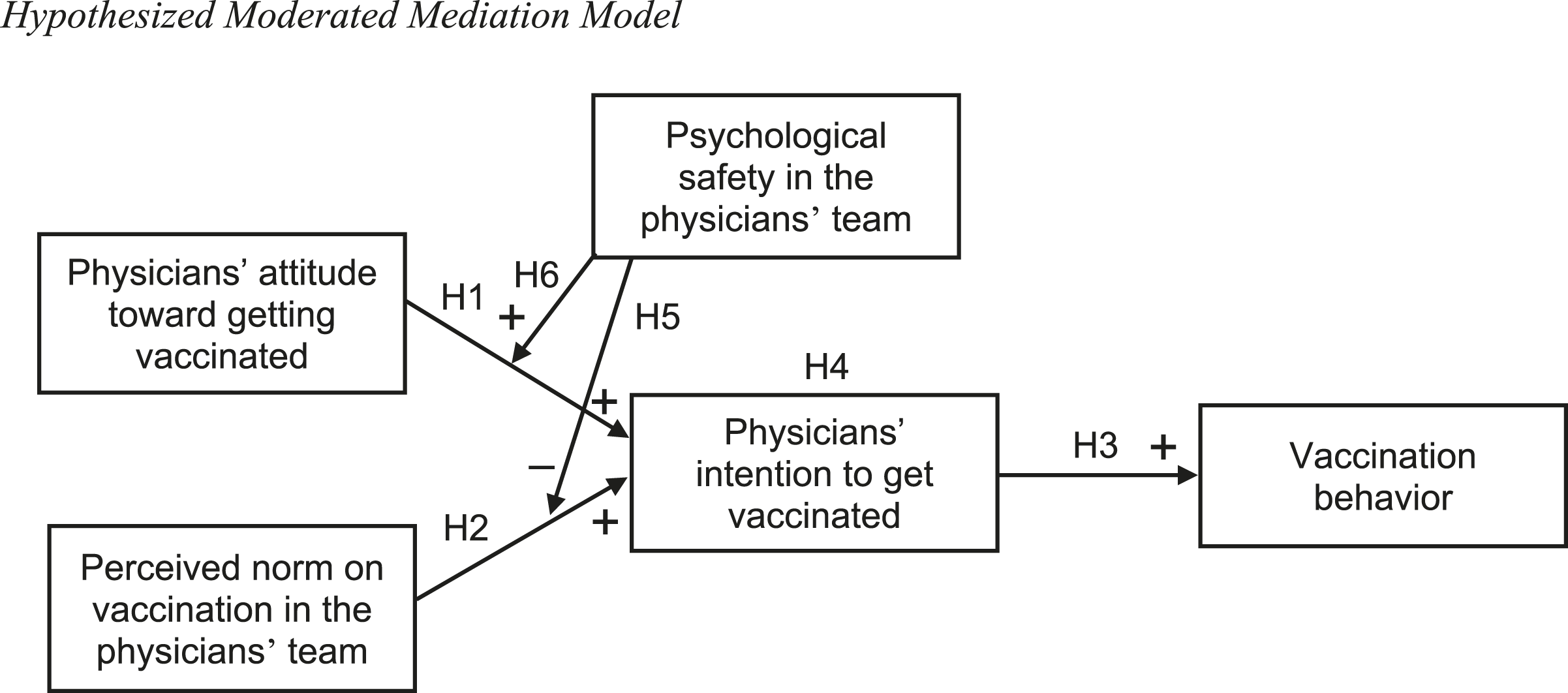
Based on the RAM, we hypothesize that physicians’ attitude toward getting vaccinated is positively related to their intention to get vaccinated. According to the RAM, physicians’ attitude toward getting vaccinated is represented by how they evaluate the influenza vaccination and its potential effects. The more positive and stronger the attitude is, the stronger the physicians’ behavioral intention should be. There is empirical support for this assumption. For example, several studies have found that individual beliefs about the effectiveness of the vaccine are positively associated with vaccination behavior (e.g., Nichol & Hauge, 1997; Wooten, Wortley, Singleton, & Euler, 2012). Behavioral beliefs are included in the RAM as antecedents of attitude (Fishbein & Ajzen, 2010). For example, an individual’s belief that getting vaccinated against influenza will help to decrease the probability to acquire influenza (which is a belief about the vaccine’s effectiveness) will translate into a positive attitude toward getting vaccinated. A few studies have also shown direct support for the relationship between healthcare workers’ attitude toward getting vaccinated and their vaccination intention (e.g., Cornally et al., 2013; Godin et al., 2010). Based on theoretical reasoning and empirical support, we hypothesize that physicians’ attitude toward getting vaccinated and their intention to do so are positively related.
Further, the RAM states that the perceived norm impacts the individual’s intention (Fishbein & Ajzen, 2010). In our context, the reference team (i.e., the team to which psychological safety and perceived norm are referred to) is the physicians’ team, which is a uni-professional team consisting only of physicians. In the hospital context, this should be the group with which physicians most strongly identify, and they should therefore be influenced by that group’s norms (Hogg & Reid, 2006). Again, there is empirical support for this relationship in the vaccination literature: Healthcare workers’ perceived norm (also called subjective norm) has been found to be related to their vaccination intention (e.g., Cornally et al., 2013; Godin et al., 2010). Accordingly, we propose that the perceived norm with regard to influenza vaccination within the physicians’ team influences physicians’ intention to get vaccinated.
Further, based on the RAM, we hypothesize that physicians’ vaccination behavior will depend on their behavioral intentions. The stronger their intention to get an influenza vaccination, the more likely it should be that they indeed get vaccinated (Godin et al., 2010; Thompson et al., 2012).
Finally, the RAM states that intention is actually the mechanism through which attitude and perceived norm affect an individual’s behavior (Fishbein & Ajzen, 2010). Therefore, we propose that physicians’ intention to get vaccinated acts as a mediator between their attitude toward getting vaccinated and their perceived norm on vaccination in the physicians’ team and their vaccination behavior.
Psychological Safety’s Role in Predicting Vaccination Behavior
An important aspect of psychological safety is the absence of fear of negative consequences following challenging actions such as speaking up (Kahn, 1990; Nembhard & Edmondson, 2006). Negative consequences of such challenging actions may—on the harmless end of the spectrum—include negative social reactions by team members leading to feelings of embarrassment, up to—on the harmful end—very tangible consequences such as losing one’s job. Accordingly, previous research has found the construct to be positively related to a number of interpersonally risky behaviors such as speaking up within aircrew teams (Bienefeld & Grote, 2014), subordinates’ improvement-oriented voice (Detert & Burris, 2007), reporting of treatment errors in hospitals (Leroy et al., 2012), and negatively related to different types of silence toward supervisors (Brinsfield, 2013). We argue that by giving individuals space for expressing themselves without fear of negative consequences, psychological safety translates into low social pressure to conform to group norms. Punishing members of a social group for not adhering to group norms is one measure to enforce norms (e.g., Fehr & Fischbacher, 2004; Fehr & Gächter, 2002). Even the threat of punishment can make individuals conform to norms (Spitzer, Fischbacher, Herrnberger, Grön, & Fehr, 2007). Therefore, freeing individuals from such fears, signified by a high psychological safety, should reduce pressure exerted by social norms.
Psychological safety is connected to interpersonally risky behavior. For example, in low psychological safety teams, members do not feel safe to admit errors or ask for help (Edmondson, 1999). However, every behavior within a team contains some degree of risk of receiving negative reactions by team members such as social rejection or punishment. In fact, especially behavior which does not correspond to group norms will be interpersonally risky since others will tend to enforce these norms by punishing the deviate (Fehr & Fischbacher, 2004; Fehr & Gächter, 2000). In low psychological safety teams, team members should therefore feel greater social pressure to adhere to the current team norm with regard to individual behaviors compared to team members in high psychological safety teams. This assumption is also compatible with the predictions of uncertainty–identity theory, which states that the more uncertain people are, the more likely they are to identify with a social group (Hogg, 2007). Psychological safety can be construed as an absence of uncertainty about how other team members will react to an individual’s behavior, which is why in low psychological safety teams, members should feel more uncertain and therefore identify more strongly with the team and follow its norms to reduce uncertainty. Hence, we hypothesize that psychological safety has a moderating impact on the effect of perceived norm on intention.
In our context, this means that low psychological safety in the physicians’ team should lead to higher social pressure to conform to the team norm, in order to avoid negative reactions by team members. Therefore, physicians’ vaccination behavior should be more strongly influenced by the perceived team norm with regard to getting vaccinated.
We have argued that in psychologically safe teams, individuals feel less pressure to follow group norms. Psychological safety should reduce the influence of the perceived norm, as we hypothesized above. Individuals should feel more comfortable to be themselves (Kahn, 1990). Thus, they should feel safer to act according to their attitudes—even if these attitudes might not be in line with group norms.
This may be illustrated by the study by Pearsall and Ellis (2011): The authors found that student teams composed of members with high utilitarianism were more likely to cheat and that psychological safety enhanced this relationship. The authors argued that with high psychological safety, members feel safeguarded and are more likely to overcome social constraints such as social norms against unethical behavior. Members thus feel more comfortable to share risky ideas such as cheating. Their results illustrate that psychological safety can weaken the effect of perceived norms and strengthen the effect of attitudes—even if the attitudes go against broader social norms.
Further, according to the RAM, the determinants of intention may vary in their predictive validity between persons, behaviors, or also contexts (Ajzen, 1991; Fishbein & Ajzen, 2010). While one or two of the three determinants may be of little importance for the prediction of a specific behavior, at least one of them must stay predictive. Therefore, moderators which strengthen the influence of one of the determinants on intention may well weaken the influence of the others and vice versa. While social pressure enhances the influence of (perceived) norms on behavior, there is empirical evidence that social pressure has an opposite influence on the impact of attitude on behavior. In a meta-analysis, Wallace, Paulson, Lord, and Bond (2005) have found that social pressure moderates the attitude–behavior relationship—the relationship becomes stronger with decreasing social pressure.
In our context, this means that physicians in psychologically safe teams should pay greater attention to their personal attitude toward influenza vaccination and develop a corresponding behavioral intention also if the team norm dictates otherwise. Thus, we hypothesize a moderating impact of psychological safety on the effect of attitude on intention.
In summary, we postulate a moderated mediation model of psychological safety’s role in the prediction of individual behavior in teams (see Figure 1), spelled out in the final hypothesis.
Method
Participants and Procedure
We gathered data at two measurement points using online questionnaires that we administered in a large Swiss hospital. We contacted all physicians employed at the hospital via e-mail before the hospital started to provide free influenza vaccination at T1. We sent a link to the first questionnaire, which included the measures for attitude toward vaccination, perceived norm on vaccination, psychological safety, and intention to get vaccinated. We also assessed several descriptive variables as well as our control variables. After the end of the influenza vaccination phase, around three months after T1, we sent out the link to the second questionnaire (T2). The second survey included the measure of vaccination behavior and some additional questions about situational aspects of the vaccination (e.g., if they received it in their ward or after an information event). These additional measures were not considered for this study.
We contacted 816 physicians, of which 290 (35.5%) completed the first online questionnaire. Two participants commented they were not able to correctly answer the questions about their teams (perceived norm and psychological safety) and were therefore excluded. Of the remaining 288 participants, 208 (72.2%) completed the second questionnaire. The sample at T1 included 131 females (45.5%) and 146 males (50.7%) with 11 participants not answering the question. On average, the participants were 39.42 years old (SD = 9.35), ranging in age from 25 to 66 years old. They had worked in that particular hospital for an average of 7.12 years (SD = 7.01) and in their job more generally for an average of 12.75 years (SD = 9.19). The physicians worked in different clinics of the hospital including oncology, internal medicine, pathology, surgery, anesthesia, and radiology. In the sample at T2, participants were 43.3% women, had an average age of 40.02 years (SD = 9.63), an average organizational tenure of 7.16 years (SD = 6.78), and an average job tenure of 13.34 years (SD = 9.15). We compared the sample at T2 with the participants who did not fill in the questionnaire at T2. We found no significant differences in age, F(1, 265) = 3.14, p = .078, gender, χ2(1, N = 277) = 1.86, p = .180, organizational tenure, F(1, 239) = 0.02, p = .900, or job tenure, F(1, 262), p = .091.
Measures
RAM variables (i.e., attitude, perceived norm, and intention) were measured with self-generated items. Since items to assess RAM variables are tailored to a very specific behavior and context, generating items to measure these variables conforms to the usual research process, and it was guided by recommendations by Fishbein and Ajzen (2010). These recommendations are very specific and lead to a certain standardization of RAM questionnaires if followed closely. Therefore, looking at other studies that investigated the RAM in context of vaccination behavior, there is considerable overlap of the generated items between studies (e.g., Agarwal, 2014; Godin et al., 2010).
All self-generated items were pretested with 19 physicians of the same hospital. The pretest showed there were no difficulties in answering the items and no problems with internal consistency (all Cronbach’s alpha >.70). For the intention to get vaccinated, the pretest revealed that two items were redundant. For the questionnaire at T1, they were therefore replaced with a newly generated item.
Attitude toward getting vaccinated
We used five items to assess participants’ attitude toward vaccination. The items started with “My getting vaccinated during the upcoming influenza season would be,” followed by semantic differentials with poles such as useful versus useless and important versus unimportant. Answers were assessed on a 7-point scale and ranged from −3 to +3 (α = .87).
Perceived norm on vaccination
We measured participants’ perceived norm on vaccination in their physicians’ team with five items. Sample items were as follows: “Members of my team think one should get vaccinated during the upcoming influenza season” and “Members of my team are getting vaccinated during the upcoming influenza season.” Participants answered on a 7-point scale ranging from 1 (strongly disagree) to 7 (strongly agree) (α = .92).
Intention to get vaccinated
We used four items to assess participants’ intention to get vaccinated. Sample items were as follows: “I will get vaccinated during the upcoming influenza season” and “It is likely that I’m getting vaccinated during the upcoming influenza season.” Reliability analyses showed that one of the four items had a low intercorrelation with the other items. Inspection of the data revealed that a large number of participants did not answer the negatively phrased and reverse coded item consistently with the other items. Therefore, the item was excluded from our analyses. Participants answered on a 7-point scale ranging from 1 (strongly disagree) to 7 (strongly agree) (α = .95).
Psychological safety
Psychological safety was assessed using the seven-item scale by Edmondson (1999). The items were translated into German using the translation by Baer and Frese (2003) as a guideline. Items were back-translated and compared to the original items to ensure that the meaning of all items was the same as in English (Schaffer & Riordan, 2003). The items were slightly adapted to better suit our setting, changing the wording from “on/in this team” to “in my team.” A sample item was, “Members of my team are able to bring up problems and tough issues.” The rating was assessed on a response scale ranging from 1 (strongly disagree) to 7 (strongly agree) (α = .78).
Vaccination behavior
Vaccination behavior was measured with one item: “During the last influenza season, have you got vaccinated?” The answer was assessed in a binary format (0 = no, 1 = yes).
Control variables
We controlled for gender because women have been found to report more adverse effects from influenza vaccination than men (Beyer, Palache, Kerstens, & Masurel, 1996). Therefore, women are more likely to have had unpleasant experiences with vaccination, which might cause them to avoid future vaccinations. Furthermore, we controlled for physicians’ job tenure. Physicians with higher job tenure have more personal experience when it comes to influenza vaccination. Depending on whether negative or positive experiences (e.g., unpleasant side effects vs. never contracting influenza) are predominant, physicians with higher job tenure could tend to develop unfavorable or favorable vaccination intentions.
We compared our results with and without control variables. Since we did not find any differences in the pattern of our results, we are going to report the results without control variables (Becker, 2005; Becker et al., 2016).
Confirmatory Factor Analyses
We conducted confirmatory factor analyses (CFAs) to test if our measurement model fits our data and if alternative models would be a better fit. We conducted the analyses using R version 3.6.1 (R Core Team, 2019) and the package lavaan (Rosseel, 2012). First, we specified a four-factor model including the items used to measure attitude, perceived norm, intention to get vaccinated, and psychological safety. The CFA showed that the model had an acceptable fit to the data, χ2(164) = 350.36, p < .001, comparative fit index = .96, normed fit index = .92, goodness of fit index = .89, root mean square error of approximation = .06, 90% confidence interval (CI) [.05, .07], and standardized root mean square residual = .06. This four-factor model had a significantly better fit than a three-factor model with attitude and perceived norm as a combined factor, Δχ2(3) = 842.72, p < .001, than a three-factor model with attitude and intention to get vaccinated as a combined factor, Δχ2(3) = 393.09, p < .001, and than a one-factor model with all items loading on a single factor, Δχ2(6) = 1918.50, p < .001.
Results
Data Analysis
Before testing our model, we checked our data for different types of outliers, following recommendations by Aguinis, Gottfredson, and Joo (2013). In detail, we used multiple-construct techniques (standardized residuals, scatter plots, studentized deleted residuals, and leverage values), and we checked for model fit outliers as well as prediction outliers (Cook’s distance, standardized difference in fits, and standardized difference in betas). To be conservative, we excluded cases only if they were identified as outliers by at least two of the techniques mentioned above. Seven cases of our sample met these criteria and were excluded from further analyses.
Intercorrelations, Means, and Standard Deviations for Study Variables.
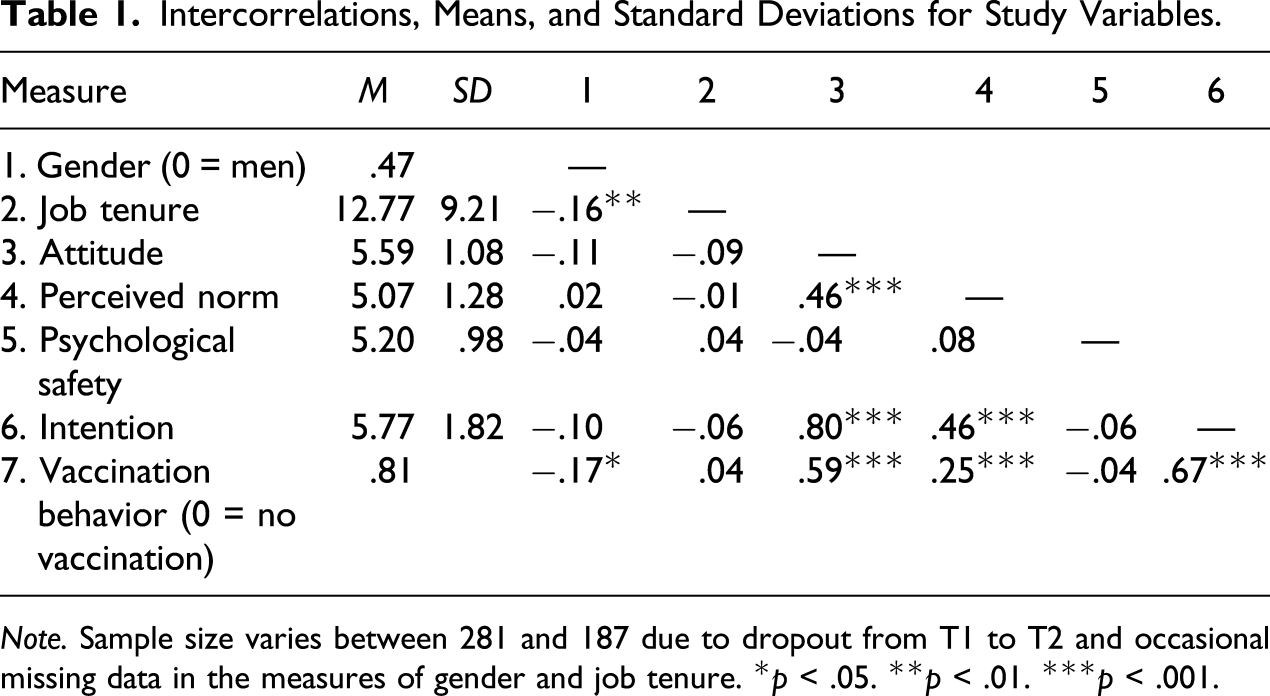
Note. Sample size varies between 281 and 187 due to dropout from T1 to T2 and occasional missing data in the measures of gender and job tenure. *p < .05. **p < .01. ***p < .001.
Testing Hypotheses Based on RAM
Hierarchical Linear Regression Analyses Predicting Intention to Get Vaccinated from Attitude Toward Vaccination, Perceived Norm on Vaccination, and Psychological Safety.
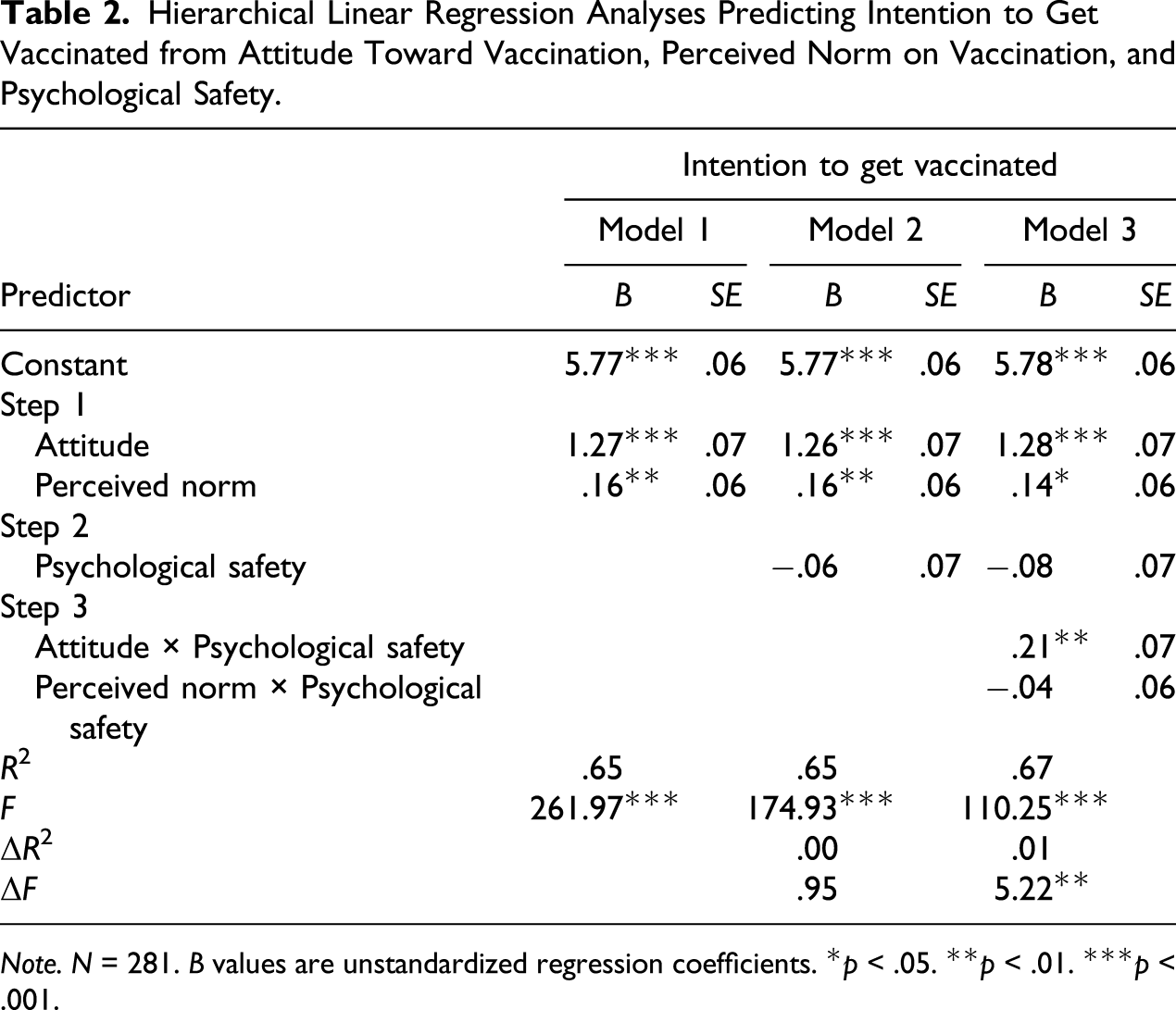
Note. N = 281. B values are unstandardized regression coefficients. *p < .05. **p < .01. ***p < .001.
As shown in Table 2, in Model 1, physicians’ attitude toward vaccination (B = 1.27, p < .001; f2 = 1.28) as well as their perceived norm on vaccination (B = .16, p = .006; f2 = .03) were positively and significantly associated with their intention to get vaccinated. Therefore, Hypotheses 1 and 2 were supported.
Hierarchical Logistic Regression Analyses Predicting Vaccination Behavior from Attitude Toward Vaccination, Perceived Norm on Vaccination, and Intention to Get Vaccinated.
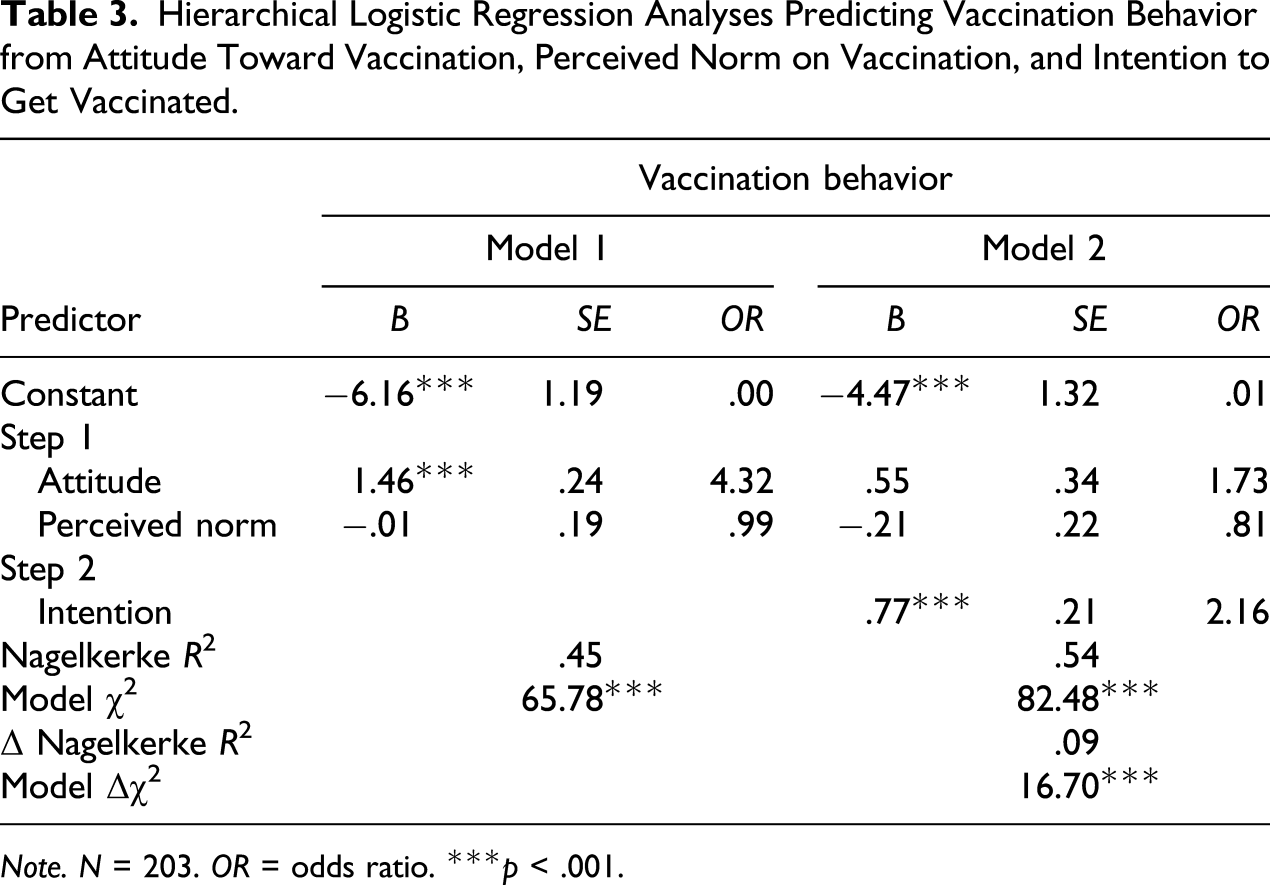
Note. N = 203. OR = odds ratio. ***p < .001.
As shown in Table 3, in Model 2, there was a positive and significant relationship between intention to get vaccinated and vaccination behavior (B = .77, p < .001). The odds ratio for this relationship was 2.16, which indicates that with an increase of physicians’ intention to get vaccinated by one unit, the odds of physicians to actually get vaccinated increases by 2.16. Thus, Hypothesis 3 was supported.
Hypothesis 4 proposed that there are indirect effects from (a) physicians’ attitude toward getting vaccinated and (b) physicians’ perceived norm on vaccination in the physicians’ team through physicians’ intention to their vaccination behavior. To test for mediation in Hypothesis 4, we used PROCESS, a macro for the SPSS software package (Hayes, 2013). To test our model’s mediation effect, we constructed a bootstrap CI for the indirect effect (Preacher & Hayes, 2008) using 10,000 bootstrap samples generated by the PROCESS macro (Model 4).2 The analysis was performed separately for two mediation models, once with attitude toward getting vaccinated as the predictor and once with perceived norm on vaccination as the predictor.
There was a significant indirect effect of .97, 95% CI [.59, 1.53] from physicians’ attitude toward getting vaccinated through intention to get vaccinated to vaccination behavior. There was also a significant indirect effect of .11, 95% CI [.01, .26] from physicians’ perceived norm on vaccination in the physicians’ team through intention to get vaccinated to vaccination behavior. Therefore, Hypotheses 4a and 4b were supported.
Testing Hypotheses on Psychological Safety
Next, we analyzed Hypotheses 5 to 7 which concern psychological safety’s role in the prediction of individual behavior. Hypothesis 5 predicted that psychological safety in the physicians’ team moderates the relationship between physicians’ perceived norm on vaccination in the physicians’ team and their intention to get vaccinated such that psychological safety weakens the relationship. We analyzed the hypotheses using a hierarchical linear regression model. In Step 1, we entered our two predictors, attitude toward vaccination and perceived norm on vaccination. In Step 2, we entered the moderator—psychological safety. In Step 3, the two interaction terms of attitude toward vaccination with psychological safety and perceived norm on vaccination with psychological safety were entered to test for moderation effects. Results of the hierarchical linear regression analyses are depicted in Table 2. Predictors and the moderator were mean-centered prior to analysis.
As shown in Table 2, in Model 3, there was no significant interaction effect between perceived norm on vaccination and psychological safety on intention to get vaccinated (B = −.04, p = .533; f2 = .00). Therefore, Hypothesis 5 was not supported.
Hypothesis 6 predicted that psychological safety in the physicians’ team moderates the relationship between physicians’ attitude toward getting vaccinated and their intention to get vaccinated such that psychological safety strengthens the relationship. As shown in Table 2, in Model 3, there was a significant interaction effect between attitude toward getting vaccinated and psychological safety on intention to get vaccinated (B = .21, p = .003; f2 = .03). As can be seen in the interaction plot in Figure 2, among those high in psychological safety (1 SD above the mean), the relationship between attitude toward vaccination and intention to get vaccinated was stronger than with those low in psychological safety (1 SD below the mean). Thus, Hypothesis 6 was supported. Simple slope analyses showed that both slopes were significant (B = 1.07, p < .001 for low psychological safety and B = 1.48, p < .001 for high psychological safety). We further wanted to see whether there was a significant difference in intention for low versus high psychological safety for physicians with a negative attitude specifically (i.e., whether the two end points on the left in Figure 2 are significantly different from each other). To test this, we performed a simple slope analysis, where the predictor (attitude toward getting vaccinated) and moderator (psychological safety) are switched (see Dawson, 2014). We found that physicians with a negative attitude toward getting vaccinated (1 SD below the mean) had a significantly weaker intention to get vaccinated when psychological safety was high rather than low, B = −.31, p = .003. Interaction effect between attitude toward vaccination and psychological safety on intention to get vaccinated. Note. PS = psychological safety.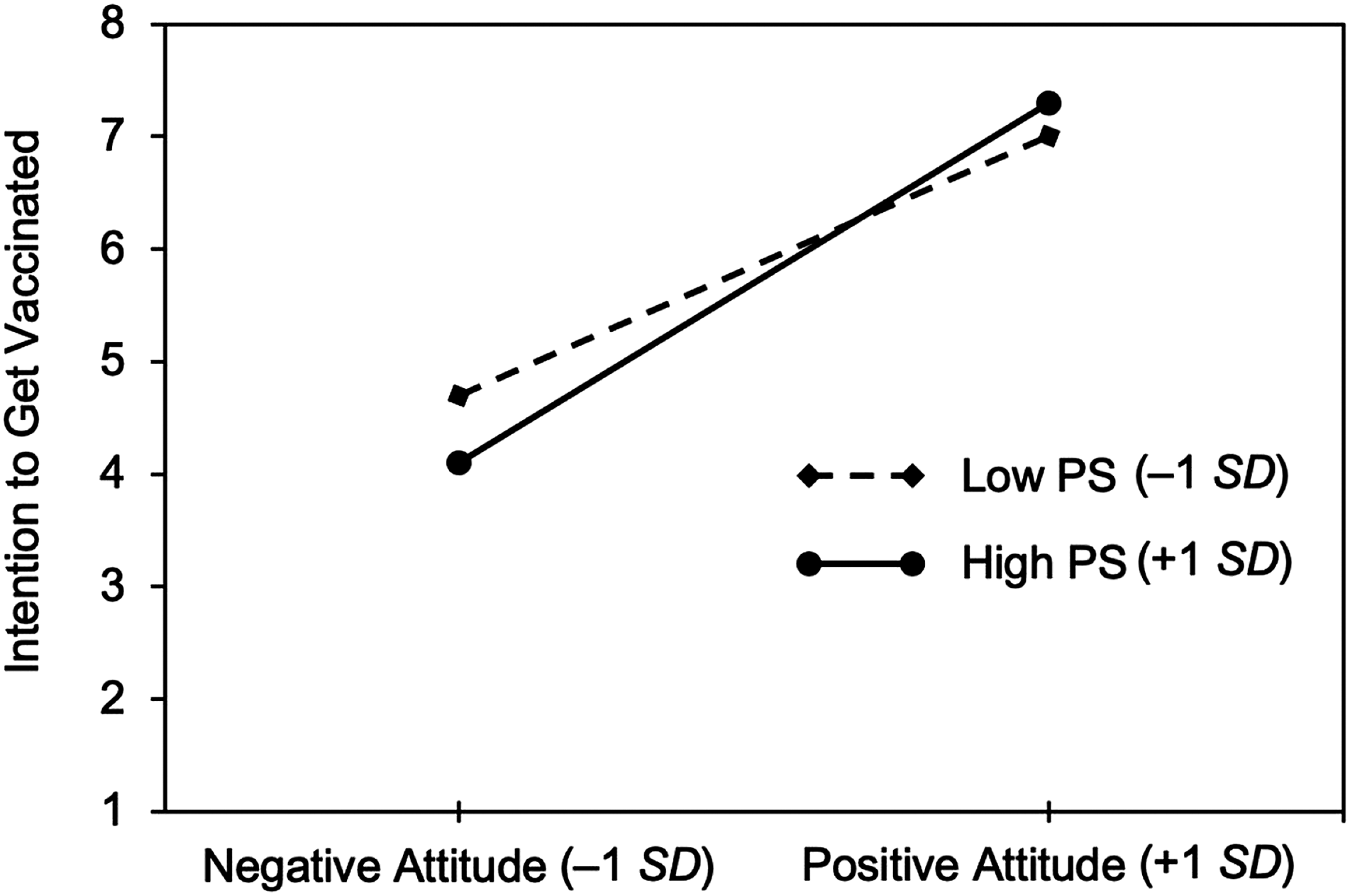
Finally, Hypothesis 7 predicted that there are moderated indirect effects from (a) physicians’ attitude toward getting vaccinated and (b) physicians’ perceived norm on vaccination in the physicians’ team through physicians’ intention to their vaccination behavior. Psychological safety was hypothesized to moderate the indirect effects by strengthening the effect of attitude and weakening the effect of perceived norm. To test this hypothesis, we again used the PROCESS macro (Model 7) for SPSS (Hayes, 2013). Similar to the mediation analysis described above, 10,000 bootstrap samples were generated and used to construct a bootstrap CI for the conditional indirect effect or moderated mediation effect. Again, the analysis was performed for the two model predictors separately.
Conditional Indirect Effects of Attitude Through Intention to Get Vaccinated on Vaccination Behavior.
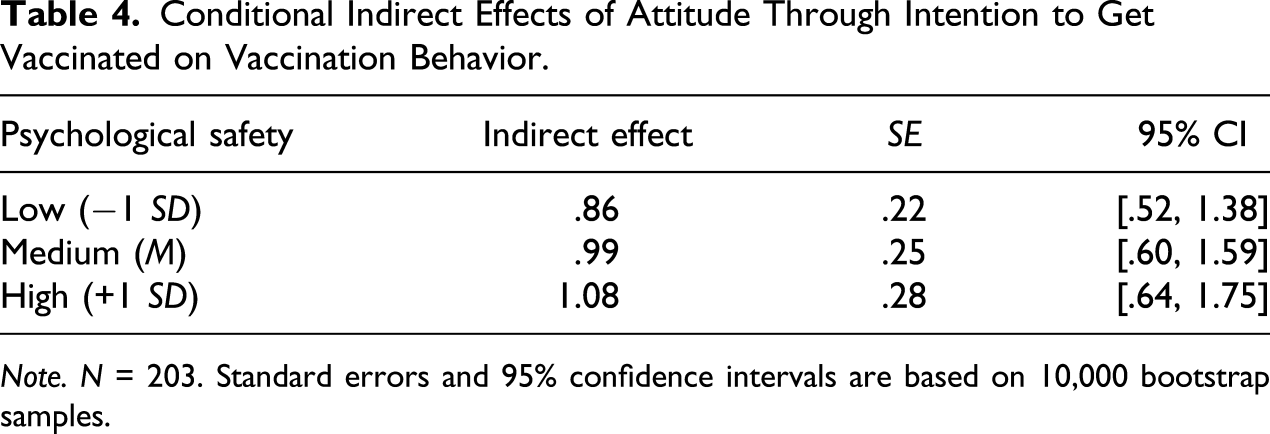
Note. N = 203. Standard errors and 95% confidence intervals are based on 10,000 bootstrap samples.
Discussion
In this study, we argued that it is important to look at psychological safety as a climate variable which exerts contextual influence on individual behavior (see Sanner & Bunderson, 2015). Drawing on the RAM and the concept of social pressure, we suggested a model which specifies the moderating role of psychological safety in the prediction of individual behavior as it occurs in a team context. We hypothesized that psychological safety would strengthen the effect of individuals’ attitude on intention to show a behavior and weaken the effect of their perceived norm on intention to show a behavior. The intention, in turn, should predict the likelihood of the individual to actually perform the behavior. We tested our model in the medical field and focused on physicians’ influenza vaccination behavior.
We found support for the hypothesized relationships based on the RAM: We found significant positive main effects for physicians’ attitude toward getting vaccinated and their perceived norm on vaccination in the physicians’ team on their intention to get vaccinated. Physicians’ intention, in turn, had a positive effect on their vaccination behavior. Regarding our main research question about the moderating effect of psychological safety, we found that the effect of attitude on intention was strengthened by psychological safety experienced by physicians in their team. Physicians with a positive attitude toward getting vaccinated were even more inclined to actually get vaccinated when they worked in a team in which they felt psychologically safe. Thus, psychological safety strengthened the effect of a positive attitude toward a desirable behavior. In the same way, psychological safety also strengthened the effect of a negative attitude toward a desirable behavior: Physicians with a negative attitude toward getting vaccinated were even less inclined to get vaccinated when they worked in a team in which they felt psychologically safe. This illustrates that psychological safety (i.e., the individual’s perception of the climate) enhances the effect of the individual’s attitude—regardless of whether that attitude is positive or negative. In psychologically safe teams, individuals feel comfortable and safe to be who they are (Edmondson, 1999; Kahn, 1990). Our results provide first evidence that in teams with high psychological safety, individuals feel more comfortable and safer to act in accordance with their attitudes than in teams with low psychological safety. Therefore, increasing psychological safety can facilitate both positive and negative consequences, depending on whether the individual’s attitude is in line with an organization’s goals or ethical values.
Our results are less conclusive when it comes to the interaction between individuals’ perceived norm and psychological safety. In our sample, we did not find a significant interaction effect between the two on physicians’ intention to get vaccinated. We see two plausible reasons for this finding. First, attitude and perceived norm are interrelated. If individuals hold a strong positive or negative attitude toward a behavior, they might assume that other individuals who are important to them have a similar attitude, which translates into an attitude-congruent perceived norm (Oliver & Bearden, 1985). Also, if there is a strong positive or negative norm on a behavior in a team, individuals might assimilate their personal attitude to be in line with the perceived norm (Terry & Hogg, 1996). Underlying this effect might be a process of social contagion, where individuals adopt the attitudes or behaviors of others (Bovasso, 1996). These crossover effects—as this phenomenon has been termed in the literature (e.g., Oliver & Bearden, 1985; Terry & Hogg, 1996)—from attitude to perceived norm and vice versa make it difficult to look at interaction effects with psychological safety separately, possibly leading to nonsignificant results. An experimental design with attitude and perceived norm manipulated as independent variables could be used to isolate the two interaction effects.
Second, perceived norm and psychological safety in a team might interact in contradicting ways, which could, in combination, lead to a weak or nonsignificant effect. Following our hypotheses, psychological safety should reduce the effect of perceived norm on intention: with a reduced fear of negative consequences, individuals feel safer to deviate from the norm. However, psychological safety could also coincide with a generally positive team climate and a higher group cohesion. This could lead individuals to more strongly identify with the team and be more willing to accept team norms (Hogg & Reid, 2006). Supporting this notion, initial psychological safety has been found to be positively related to team identification (Johnson & Avolio, 2019). Therefore, in teams with high psychological safety, the effect of perceived norms could actually be enhanced instead of weakened. More research is needed to better understand how psychological safety and perceived norm interact and, for example, test under which conditions psychological safety weakens or strengthens the perceived norm’s effect on intention.
Finally, it is conceivable that psychological safety simply does not have the hypothesized moderation effect on the relationship between perceived norm and intention. What an individual perceives to be the norm in a given team may impact the individual’s intention and subsequent behavior, regardless of the level of psychological safety within the team. Our proposed directions for future research will be instrumental for further clarifying these relationships.
Theoretical Implications
We follow Sanner and Bunderson’s (2015) suggestion that psychological safety might be better conceptualized as a contextual, moderating variable rather than as a causing factor of, for example, learning. With our theoretical model, we illustrate how psychological safety can act as such a moderating variable in the prediction of individual behavior. It can help to better understand psychological safety’s effect mechanisms and provide a new perspective on previous research.
For example, Pearsall and Ellis’s (2011) finding that psychological safety strengthens the positive relationship between utilitarianism and cheating behavior is readily compatible with our model: If students have a utilitarian approach, this should mean that they have a positive attitude toward cheating if this behavior leads to benefits such as a higher grade. Students with high utilitarianism (and thereby positive attitude toward cheating) should therefore be more inclined to and subsequently more likely to cheat in teams with high compared to low psychological safety.
The new perspective can enrich our understanding also in scenarios in which psychological safety has been considered to directly affect behaviors such as employee voice (Walumbwa & Schaubroeck, 2009). According to our model, psychological safety in teams should make individuals feel comfortable to act according to their personal attitudes. Therefore, especially those employees who have a positive attitude toward voice should show voice behavior in the context of high psychological safety. However, employees with a neutral or negative attitude toward voice might be largely unaffected in their voice behavior by the climate or even be encouraged to remain silent. Assuming that the majority of individuals in a group or organization have positive attitudes toward voice, psychological safety will lead to more voice, resulting in a positive relationship between psychological safety and voice behavior. However, the strength of this relationship is expected to vary across teams and organizations since the composition of individuals with positive, neutral, or negative attitudes toward voice will vary. In general, this alternative perspective may provide a possible explanation for differences in findings with regard to psychological safety’s main effects, such as varying effects of psychological safety on learning behavior (Edmondson & Lei, 2014; Sanner & Bunderson, 2015). Of course, future studies will need to investigate if these assumptions hold true.
A reiterated observation in the psychological safety literature is that there is little theorizing on how psychological safety affects behavior (Newman et al., 2017). The proposed theoretical model shows on a very basic level how psychological safety can act as a moderator in the prediction of behavior performed in a social environment. It is therefore applicable to beneficial as well as detrimental behavior, the latter of which is largely absent from the literature (Edmondson & Lei, 2014; Newman et al., 2017). The model can thus be used in future research on possible detrimental effects that might be facilitated by psychological safety. Also, studies investigating psychological safety’s consequences might want to consider potential unintended effects which could counteract or outweigh the beneficial consequences they are focusing on.
Practical Implications
In practice, our model enables the prediction of potential positive and negative consequences facilitated by enhancing psychological safety. An overwhelming majority of the current literature focuses on psychological safety’s beneficial impacts such as increased speaking up or learning behavior (Newman et al., 2017). Therefore, many team leaders may consider increasing psychological safety within their teams. Our theoretical model and empirical findings suggest that while this may have desirable effects, leaders must be cautious of potential unintended, undesirable effects. In a psychologically safe team, individuals will feel safer to act according to their attitudes. Hence, the ultimate behavioral consequences of increasing psychological safety in a team will depend on the individuals’ attitudes. If the latter are not in line with organizational goals or outright detrimental, the individual behaviors may be also. We were able to demonstrate this with our study using real-life data on physicians’ individual beliefs on vaccination and their vaccination behavior. For individuals with deviant attitudes, a high psychological safety facilitated behavior that was not in line with organizational recommendations and represents real health risks for patients.
Team leaders seeking to enhance psychological safety should therefore be cautious of potential unintended consequences. We suggest that one way to mitigate such consequences will be to uncover relevant attitudes and, if necessary, take measures to bring employees’ attitudes in line with organizational goals before enhancing psychological safety. For example, in physicians’ teams, enhancing psychological safety could lead to a decrease in influenza vaccination if a majority of physicians had a negative attitude toward vaccination. Thus, team leaders would have to take measures to make sure physicians’ attitudes are in line with the hospital’s recommendations, which is to increase influenza vaccination of healthcare workers. For example, such encouragement could be achieved by issuing an information campaign or other educational interventions targeted at physicians’ detrimental beliefs about the vaccination (e.g., Heininger, Bächler, & Schaad, 2003; Manuel, Henry, Hockin, & Naus, 2002; Nafziger & Herwaldt, 1994; Qureshi, Hughes, Murphy, & Primrose, 2004).
Moreover, the model suggests that positive effects of psychological safety—like increases in error reporting and speaking up—might be boosted by taking measures to get employees’ attitudes in line with these goals. For example, reducing barriers for speaking up—which is what increasing psychological safety in a team does—is only the first step toward getting employees to speak up. Employees also need to exhibit a positive attitude toward speaking up in order to form an intention to do it and, subsequently, perform the behavior. Therefore, if managers seek to enhance psychological safety in order to improve team performance, for example, by enhancing learning behaviors, they should seek to promote employees’ attitudes toward these behaviors as well. Thereby, increasing psychological safety should be even more effective.
Limitations and Future Research
Our study has several limitations, which we want to discuss in the following. First, we conducted a study in a specific context and on a specific behavior; thus, the generalizability of our results might be limited. Even though this context was particularly suitable to test our model, future studies still need to examine whether our model holds in other contexts and with other behaviors. With regard to the behavior studied, it will be important to better understand what types of behavior our model can be applied to (i.e., with which behaviors does psychological safety exert its moderating effect). For example, it will be interesting to see if our model can only be applied to overt individual behaviors which are easily spotted by other team members or if it also holds for more covert individual behaviors. To give an example, if we were to look at nurses’ hand hygiene when interacting with patients, would psychological safety in the healthcare team only play a role for hand hygiene which is observable by other healthcare workers or would it also affect covert hand hygiene behavior where no one would notice its execution (or omission). It could be argued that the moderating effect of psychological safety would be stronger in overt behaviors because social pressure (in the form of a lack of psychological safety) should be greater and therefore more effective if the behavior occurs in public rather than in private (Argyle, 1957). Whether the model can only be applied to behaviors that are permitted or if it also holds for behaviors which are prohibited is also worth examining. This question could be asked with regard to permission or acceptance in the team, the organization, or society. For example, with an organizational focus, it would be interesting to see whether psychological safety plays a role in counterproductive work behavior. The findings of Pearsall and Ellis (2011) could suggest that psychological safety does not only facilitate permitted but also prohibited behaviors. Future studies could investigate the type of behavior as a moderator of the effect of psychological safety, translating into a three-way interaction between the type of behavior, psychological safety, and attitude or perceived norm for predicting intentions and behavior.
Second, we could not collect objective behavioral measures because the hospital could not provide data on the individual vaccination status of physicians based on ethical reasons. Although self-reported vaccination behavior comes close to actual vaccination behavior, physicians may have answered our question in a socially desirable way. This might be reflected in the higher reported vaccination rate in our study compared to the overall vaccination rate of physicians in the hospital. Then again, these differences could also be due to a sampling bias with physicians who encourage influenza vaccination being more interested in the topic and more inclined to participate in a study about vaccination than physicians who do not encourage influenza vaccination. Since physicians know that the hospital tracks who is getting vaccinated and who is not, the effect of social desirability might be weakened. Also, our study was completely anonymous, and the participating hospital did not receive any individual data that would allow them to identify participants. Nevertheless, future studies could prevent social desirability biases by gathering data on actual, objective behavior.
Third, our study is based on data provided by a single source: All model constructs were measured using self-report ratings by the same individual—the physician. This can lead to a common method bias, which can inflate or deflate associations (Podsakoff, MacKenzie, Lee, & Podsakoff, 2003). Certainly, attitude, perceived norm, and intention are individual and subjective in nature and thereby best captured by self-report. However, psychological safety, actual work team norm, and behavior could also be measured using ratings by other team members or, in the case of behavior, objective data. Future studies could therefore try to incorporate additional data sources to further strengthen the design and assess the relationship between model variables with less common method variance. It would also be interesting to incorporate ratings of all or several members per team, for example, for psychological safety and team norm. This would allow to test a multilevel model, where attitude, intention, and behavior are measured at the individual level and team norm, and psychological safety are measured at the team level. This would provide a better understanding of how individual perceptions of the team and measures on the team level interact and which variables are more important when it comes to predicting individual team members’ behavior.
Fourth, with our field study, we were not able to support our hypothesis regarding the interaction between psychological safety and perceived norm. Further studies need to be conducted in order to either gain evidence for that part of our proposed model or else to gain insights into how to modify the model to accurately predict individual behavior. Given that some of the model’s constructs might be related in intricate ways, as explained above, it could be beneficial to conduct psychological experiments to disentangle the constructs in order to look at their effects separately.
Conclusion
In this study, we proposed and tested a theoretical model of the specific mechanisms through which psychological safety affects individual behavior. Our findings show that psychological safety may not only facilitate beneficial behavior but also enable unintended detrimental behavior—in our study, the omission of influenza vaccination by physicians. We hope that this differentiated model will constitute a starting point for a new research stream within the psychological safety literature. The current, mostly one-sided view on psychological safety needs to be calibrated through a more nuanced understanding of both opportunities and risks that psychological safety might facilitate in teams and organizations. Given that much of the psychological safety research has been conducted in high-risk environments such as health care, this new stream of research might not only help to make organizations a psychologically safer place but also promote physical safety.
Footnotes
Acknowledgments
We thank Matthias Schlegel and Manuela Rasi for their feedback on the questionnaires and their help with data collection.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Notes
Associate Editor: Hannes Leroy