
Abstract
The school environment is an ideal setting for healthy weight programming with adolescents. The federal government has reinforced the importance of school-based health promotion. The current study examined the preliminary influence of the 2006 school wellness policy requirement of the Child Nutrition and WIC Reauthorization Act (CNWICRA) on adolescent Body Mass Index (BMI) and physical education participation. Nationally representative data from the 2003 and 2007 Youth Risk Behavior Surveillance Survey (YRBSS) were used. The authors examined BMI percentile and physical education participation based on survey year and geographic region. Results suggest a slight decrease in BMI with no changes in physical education participation. A main effect for geographic region was found for both physical education participation and BMI percentile, while a geographic region-by-survey year interaction was discovered when analyzing BMI percentiles. Results suggest a need for continued investigation and may inform future healthy weight programming and geographically tailored wellness policies.
Obesity is a rapidly growing problem in the United States affecting approximately 12.5 million children and teens (Ogden, Carroll, Curtin, Lamb, & Flegal, 2010). Nearly one in three school-age children is overweight or obese (Ogden, Carroll, & Flegal, 2008).
The school environment is a crucial target within a comprehensive plan promoting healthy weight in children and adolescents. The federal government has reinforced the importance of the schools through recent legislation addressing school nutrition, physical activity, and wellness policies (Child Nutrition and WIC Reauthorization Act [CNWICRA] PL 108-265, 2004).
School-based practitioners will be increasingly responsible for evaluating local school wellness policies. School nurses, social workers, school psychologists, administrators, and others may take part in program evaluation efforts. Analysis of wellness policy effectiveness will be challenging within the current culture of high-stakes academic accountability. How can we effectively integrate and measure physical activity, for example? Feasible wellness policy implementation and measurement must capitalize on elements of the school culture that already exist.
Physical education is one area with great promise when discussing school wellness policy and potential implications for public health. For example, refinement of physical education programs can influence childhood overweight and obesity (Datar & Sturm, 2004). Furthermore, preliminary assessments of school wellness policy may include quantified physical education requirements as a metric (Datar & Sturm, 2004).
Taking the above rationale into account, the current study examined the preliminary influence of school wellness policy on childhood overweight and obesity by examining adolescent self-report data. Specifically, we examined physical education participation and body mass index (BMI) in two cohorts of nationally representative adolescents. One cohort was surveyed before and the second was surveyed after the federal government required schools to implement wellness policies.
Overweight Children: Correlates and Consequences
Obesity and overweight statistics are based on BMI, an indirect measure of body fat (Institute of Medicine [IOM], 2007) calculated by dividing weight in kilograms by height in meters square (Pyle et al., 2006). Adults follow universal BMI scales whereas child and adolescent (e.g., through age 19) classifications are based on age- and sex-based scales to account for normal development. BMI-for-age percentiles allow us, then, to make more standardized comparisons. As such, recent experts note that children and adolescents with a BMI-for-age percentile between 85 and 95 are classified as overweight, while those above the 95th percentile are considered obese (Krebs et al., 2007; Ogden et al., 2010).
Rates of childhood obesity have nearly tripled since the 1960s in certain age groups (Ogden et al., 2006). According to the National Health and Nutrition Examination Survey (NHANES), BMI measurements from 4,207 children and adolescents aged 2 to 19 years showed that 10.9% of those surveyed in 2005/2006 were at or above the 97th percentile of the 2000 BMI-for-age growth charts (Ogden et al., 2008).
Childhood obesity is a comprehensive problem with short- and long-term physical, emotional, and economic consequences (Freedman, Dietz, Srinivasan, & Berenson, 1999; Reilly, 2005; Ribeiro, Guerra, Pinto, Oliveira, & Mota, 2003). Some of the most commonly cited health problems include increased threat of cardiovascular risk factors, asthma, high blood pressure, and premature mortality (Freedman et al., 1999; Reilly, 2005; Ribeiro et al., 2003). Further, children who are treated for obesity generally can expect to have lifetime medical costs 3 times higher than their normal weight counterparts. According to the IOM (2007), annual health care spending for U.S. children with overweight diagnosis is roughly $280 million for private insurance and $470 million for Medicaid (IOM, 2007).
Psychological consequences of obesity cannot be ignored. Obese children may experience more teasing and bullying than normal weight peers, and obsession with body size can also affect overweight children (Dietz, 1998). Not surprisingly, then, the potential for development of eating disorders may be higher in obese girls (Reilly, 2005).
Socioeconomic factors are also relevant when examining the childhood obesity epidemic (Delva, Johnston, & O’Malley, 2007). Low socioeconomic status (SES) has been associated with lower levels of physical activity and, subsequently, higher incidence of overweight (Delva et al., 2007). Low SES children have been found to consume fewer nutrient-rich foods, watch more television, and engage in fewer physically active behaviors than children from other SES brackets (Delva et al., 2007; Hanson & Chen, 2007).
Further, obesity prevalence is disproportionate across ethnic groups (Ogden et al., 2008). Results of an analysis of the NHANES in 2005–2006 indicated that Hispanic and African American children ages 2 to 19 years are at greater risk for and have a higher prevalence of obesity than their non-Hispanic, Caucasian peers (Ogden et al., 2008). The 1994–1996 National Longitudinal Survey of Adolescent Health found combined overweight and obese prevalence rates to be 39.9%, 35.4%, and 28.2% for Mexican American, African American, and non-Hispanic Caucasian Americans, respectively (Wang & Beydoun, 2007).
Disproportionate rates of obesity have emerged across different geographic regions of the United States as well (Singh, Kogan, & van Dyck, 2008). In terms of regional differences, prevalence of childhood and adolescent overweight has been found to be highest in the East South-central region (including Kentucky, Tennessee, Alabama, and Mississippi) and lowest in the Mountain region (including Montana, Idaho, Wyoming, Colorado, New Mexico, Arizona, Utah, and Nevada; Singh et al., 2008). While obesity is a national problem, perhaps some areas are more susceptible to an imbalance of energy resulting in overweight.
Healthy Weight Promotion Through Physical Activity
Understanding energy balance and its relationship with body weight is essential in facilitating healthy weight promotion. The amount of energy consumed must be in careful balance with physical activity expended in order to achieve a healthy weight (Peters, Wyatt, Donahoo, & Hill, 2002). Children and adolescents who are overweight or obese should reduce caloric intake and increase physical activity to obtain a healthy weight while also maintaining healthy growth and development (Kumanyika et al., 2008). Although seemingly simple, this balance is difficult to measure: physiological processes and biological composition vary from child to child.
While a strong emphasis on reducing caloric intake may be punitive and restrictive, the promotion of healthy eating and physical activity builds competencies and health in children of all ages and sizes. Physical activity has been associated with positive psychological outcomes such as increased positive mood, increased concentration, stress reduction, and multiple healthy physical outcomes (Burgeson, Wechsler, Brener, Young, & Spain, 2001; Centers for Disease Control and Prevention [CDC], 1997; Taylor, Sallis, & Needle, 1985).
Many professional organizations have established recommendations for the ideal amount of time children and adolescents should spend engaged in physical activity. The United States Department for Health and Human Services (USDHHS) introduced Healthy People 2010 to promote healthy living in the United States. By targeting physical activity in many of its objectives, this initiative aimed, in part, to eliminate health disparities and increase enjoyable years of healthy living (2000). The National Association for Sport and Physical Education (NASPE) and the Council on Physical Education (2000) also advocate for increased activity in children and adolescents. They recommend children engage in at least 60 min of age-appropriate physical activity each day.
In general, children and adolescents do not meet these activity recommendations in their daily lives. Among adolescents, for example, 65% of students in Grades 9 through 12 have reported insufficient levels of moderate activity (NASPE & American Heart Association [AHA], 2010).
Just as NASPE and AHA (2010) report that overall adolescent physical activity is declining, this drop in activity is disproportionately apparent in certain populations. Caucasian adolescent males were most likely to meet recommended levels of physical activity, while African American and Hispanic females were least active (Eaton et al. 2006). Parenting styles, lifestyle choices, fewer opportunities, and access to physical activity may contribute to the disparity (Delva et al., 2007; Eaton et al., 2006; Hanson & Chen, 2007).
Physical activity in the school environment
Not surprisingly, factors associated with the decline in physical activity are multifaceted and require interventions that target multiple individuals, contexts, and environments (IOM, 2007). The school setting is one such environment wherein specific policies have the potential to influence physical activity patterns of children (IOM, 2007).
One nationwide survey indicated that 65% of parents believed schools to be a major change agent in the childhood obesity epidemic (Kropski, Keckley, & Jensen, 2008). The schools offer a structured environment where children can learn about healthy energy balance at an early age (Budd & Volpe, 2006; CDC, 1997; NASPE & AHA, 2010; Pate et al., 2006; Pyle et al., 2006; Segal & Gadola, 2008; Story, Kaphingst, & French, 2006). By targeting school systems, interventions will reach a large and captive audience in a cost-effective manner (Pyle et al., 2006).
Although schools offer an ideal opportunity for healthy weight promotion strategies, there are challenges associated with using this system. For example, teachers report rigid time constraints along with financial concerns as primary barriers to implementing healthy weight program elements (IOM, 2007; Schumacher & Queen, 2007). In addition, administrators, educators, and local boards of education may find the academic guidelines asserted in the 2001 reauthorization of the Elementary and Secondary Education Act, or No Child Left Behind, overwhelming to incorporate. No Child Left Behind (2001), notably, placed more emphasis on and linked financial support to the results of standardized tests within major academic subject areas. Many believe that this high-stakes testing culture is not necessarily compatible with daily physical education (Schumacher & Queen, 2007).
Recent research has suggested that high-stakes testing preparation may, indeed, be compatible with regular, daily physical activity (Mahar et al., 2006; Opitz, 2011). For example, third and fourth graders who participated in physical activity breaks during intensive academic instruction exhibited increased time on task compared to those who did not participate (Mahar et al., 2006). Physical activities were tied to academic content whenever feasible. Perhaps, then, creative physical education could permeate the cross-curricular landscape, thereby helping to facilitate the implementation of academic achievement mandates (Opitz, 2011; Schumacher & Queen, 2007).
What about legislation associated with physical education? Traditionally, physical education has been the most common outlet for physical activity needs in schools, but no federal mandates on physical education requirements have existed, to date (NASPE & AHA, 2010). While national organizations can make recommendations for quality physical education programs, each state is independently responsible for setting specific physical education guidelines. As reported in 2010, 46 states required physical education at the high school level, while 40 and 43 states required the same of middle and elementary schools, respectively (NASPE & AHA, 2010). Only five states require physical education in all grades, K–12.
Objectives 22-8 and 22-9 of the Healthy People 2010 initiative recommended specific participation requirements for physical education in the United States (USDHHS, 2000). Very few states have met these requirements (IOM, 2007). Only one state, for example, aligns with the nationally recommended 150 min per week of physical education in elementary school and 225 min per week in middle and high school (NASPE & AHA, 2010).
The U.S. Department of Health and Human Services has also recommended daily physical education as an ideal way to meet recommended daily physical activity guidelines. Daily physical education has been linked with more optimal BMIs across students. One study, for example, discovered that extending kindergarten physical education time by 5 hr weekly resulted in a decrease in the prevalence of obese and overweight females the following year by 4.2 and 9.2 percentage points, respectively (Datar & Sturm, 2004). Furthermore, routine physical education participation has been linked to positive long-term outcomes in older students as well. That is, adolescents who participated in a regular physical education program were less likely to become overweight adults (Menschik, Ahmed, Alexander, & Blum, 2008).
Mandating Wellness Through School-Based Health Promotion
The federal government responded to the health needs of children, in part, by enacting the CNWICRA (Public Law 108-265) in 2004. This reauthorization increased the accountability of school systems participating in the National School Lunch and School Breakfast programs, requiring them to provide nutritious meals and physical activity (CNWICRA, 2004). The Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) was originally developed to provide women and children with nutrition, health care referrals, and health education free of charge (United States Department of Agriculture [USDA], 2009). Historically, WIC legislation initially included in the National School Lunch Act of 1946 (i.e., renamed the Richard B. Russell National School Lunch in 1999), the Child Nutrition Act of 1966, and Section 32 of the Act of August 25, 1935 (Richardson, 2006). The 2004 Reauthorization amended original legislation and sought to improve children’s overall health, especially among families of lower SES.
One of the most relevant elements of the 2004 Act required schools to develop local wellness policies to be implemented by July 1, 2006 (Metos & Nanney, 2007). These policies targeted nutrition and physical activity in the schools and required goals, evaluations, and parent involvement in the dissemination of information on healthy eating and activity. Specifically, the legislation outlined five major components to be covered in the wellness policies including (1) goals for all programs associated with the wellness policies, (2) nutritional guidelines to be followed when serving food in the school, (3) assurance that meals served in schools would meet USDA guidelines and recommendations, (4) the establishment of progress monitoring tools, and (5) collaborative wellness policy development by parents, school nutrition personnel, students, school administrators and personnel, and community members (CNWICRA, 2004). Wellness policies were to be implemented in all areas of the country, rural and urban, without any additional funding (Moag-Stahlberg, Howley, & Luscri, 2008).
To assist schools in implementing these mandates, model wellness policies were developed by professional organizations, such as the National Alliance for Nutrition and Activity (NANA). In addition to nutritional guideline recommendations, these model policies suggested that all students in grades kindergarten through 12th receive daily physical education as taught by a qualified physical education teacher as well as daily recess in elementary schools (NANA, 2006).
Certain states have done a more thorough job of implementing the mandates than others. In Utah, for example, wellness policy compliance was highest in school districts with high participation in free- and reduced-price programs (Metos & Nanney, 2007). Overall, 77% of Utah’s school districts complied with all five components outlined in federal legislation. In South Carolina, the legislature and governor enacted South Carolina’s Students’ Health and Fitness Act of 2005 requiring specific changes to physical education and food service requirements, parent involvement in student health assessments, and evaluation of physical fitness in the schools (IOM, 2007). Most recently, lawmakers in Virginia passed a bill in February 2011—which will be in effect by 2014—requiring all public elementary and middle school students to receive at least 150 min of physical activity per week.
State-level wellness initiatives increase awareness of and participation in healthy eating and physical activity. Thus far, few studies have assessed the results of the CNWICRA changes, likely related to the delay in policy implementation (i.e., see below). Moag-Stahlberg, Howley, and Luscri (2008) evaluated the effectiveness of wellness policies across the United States. Sample policies were compared to mandates outlined in the Act and policies outlined in Action for Healthy Kids’ Wellness Policy Fundamentals (2008). The researchers found that 68% of the policies reviewed met mandate requirements outlined in the Act (Moag-Stahlberg et al., 2008). On the other hand, in the area of physical activity, none of the policies assessed met best practices standards set forth in the Wellness Policy Fundamentals (Moag-Stahlberg et al., 2008). A notable gap in policies was that only 45% of those assessed included specific requirements on time or intensity of physical education. Direct outcomes and implications associated with the 2004 mandate need to be understood to guide future, school-based healthy weight programming and legislation.
The CNWICRA was set to expire on September 30, 2009, but was given a 1-year extension through September 2010. In August 2010, the Senate approved the Healthy, Hunger-Free Kids Act of 2010 (e.g., Public Law No: 111-296) with the goal to provide significant changes to school nutrition and WIC programs. The House had approved a similar bill in July (2010) that aimed to further expand child nutrition programs. Scheduled to be in effect by October 2012, these bills—as one example—require increases in federal funding (i.e., 6 cents per lunch) for schools that provide nutritionally optimal lunches. In addition, requirements for school wellness policies will be updated, and $40 million of federal funds will be provided in order to subsidize farm-to-school programs. Despite significant federal funds being dedicated to school wellness policy development, very few studies in the extant literature have examined whether or not schools and children are any healthier now than they were before these policies were required.
Study Objectives
This study sought to examine a few key, obesity-related variables before and after the school wellness policy implementation date of July 2006. Data from a nationally, biennially administered survey of adolescents provided information about student physical education participation and BMI before (e.g., 2003) and after (e.g., 2007) the July 2006 implementation date. Further, we examined whether there may have been regional differences in physical education participation and/or BMI before and after the 2006 school wellness policy implementation date.
Given the preliminary nature of the mandate and likely variability in its implementation, we did not predict changes in BMI from 2003 to 2007. We did, however—especially given the original lack of funding provided by the CNWICRA —predict that there would be BMI and physical education differences based on geographic region (Moag-Stahlberg et al., 2008).
Method
Study Design
This study was a secondary data analysis of cross-sectional, national survey data. Data from two adolescent cohorts (e.g., 2003 and 2007) who completed the Youth Risk Behavior Surveillance System (YRBSS) survey were used in this study.
Measures and Procedures
Data Sources
YRBSS is a self-report, school-based survey conducted biennially by the CDC since 1991. The survey monitors six health risk behaviors: physical activity, sexual behaviors, behaviors associated with violence and injury, tobacco use, alcohol and drug use, and dietary behaviors. Additional information on race, height, and weight are also surveyed within the instrument.
The YRBSS is updated to reflect national topics and concerns before each biennial distribution. In general, the YRBSS consists of 87 core multiple choice questions pertaining to health-related behaviors. The 2007 survey included 11 additional questions. Responses were weighted (a) to ensure representativeness of the sample from which they were drawn and (b) to adjust for nonresponse.
Participants
Participants consisted of a national sample of students in Grades 9 through 12 from public, private, and Catholic schools across the United States. A total of 83,253 surveys were analyzed. The 2003 sample (N = 37,717) included 50.7% females (n = 19,230) and 48.3% males (n = 18,305), while the 2007 sample (N = 45,536) contained 50.6% females (n = 23,025) and 48.7% males (n = 22,159). Participants in 2003 included 30.5%, 27.3%, 21.8%, and 18.6% of students in Grades 9, 10, 11, and 12, respectively. The 2007 participants consisted of 28.7%, 26.8%, 24.4%, and 18.8% of 9th, 10th, 11th, and 12th graders, respectively.
Variables
The variables used in this study were defined by the CDC. They are noted below.
BMI. BMI was calculated by using self-report height and weight data. Students answered the questions “How tall are you without your shoes on?” and “How much do you weigh without your shoes on?” (CDC & USDHHS, 2007). Height was reported in feet and inches and was converted to meters using the following formula: [(feet × 12) + inches] ×0.0254 m/in (CDC & USDHHS, 2008). As aforementioned, child and adolescent BMI is based on percentile ranks, so comparisons across age and gender can be made.
Data from the 2007 YRBSS included BMI percentiles, while the 2003 data only provided height, weight, and the former child BMI classifications of overweight (e.g., current obese classification) and at risk of becoming overweight (e.g., current overweight classification). Therefore, using a program provided by the CDC (2009), researchers transformed the height and weight data into BMI percentiles in order to make 2003 and 2007 comparable.
Physical education participation. Physical education participation was measured by student response to the question “In an average week when you are in school, on how many days do you go to physical education (PE) classes?” Responses included 0, 1, 2, 3, 4, or 5 days (CDC & USDHHS, 2007).
Geographic location. Geographic location for the YRBSS data was categorized by U.S. Census Bureau classifications and available data. State data were included only for those states that collected data in 2003 and 2007 for the questions of interest (United States Census Bureau, 2007). Results were organized according to four regions: (a) Northeast: Maine, Massachusetts, New York; (b) Midwest: Indiana (i.e., the only state from the Centers for Disease Control that had data for all variables across both years); (c) South: Delaware, Kentucky, Mississippi, North Carolina, Tennessee, West Virginia; and (c) West: Alaska, Arizona, Montana, Utah, Idaho.
Analysis of Data
Analyses were conducted using the SPSS Complex Samples module (version 18, IBM SPSS Inc, Chicago, IL). This allowed for (a) the results to reflect a nationally representative sample, using a CDC-generated sampling weight and (b) the production of sample-based standard errors for statistical testing. Data analyses included descriptive procedures and analyses of variance (ANOVA).
Results
Physical Education Participation: 2003 Versus 2007
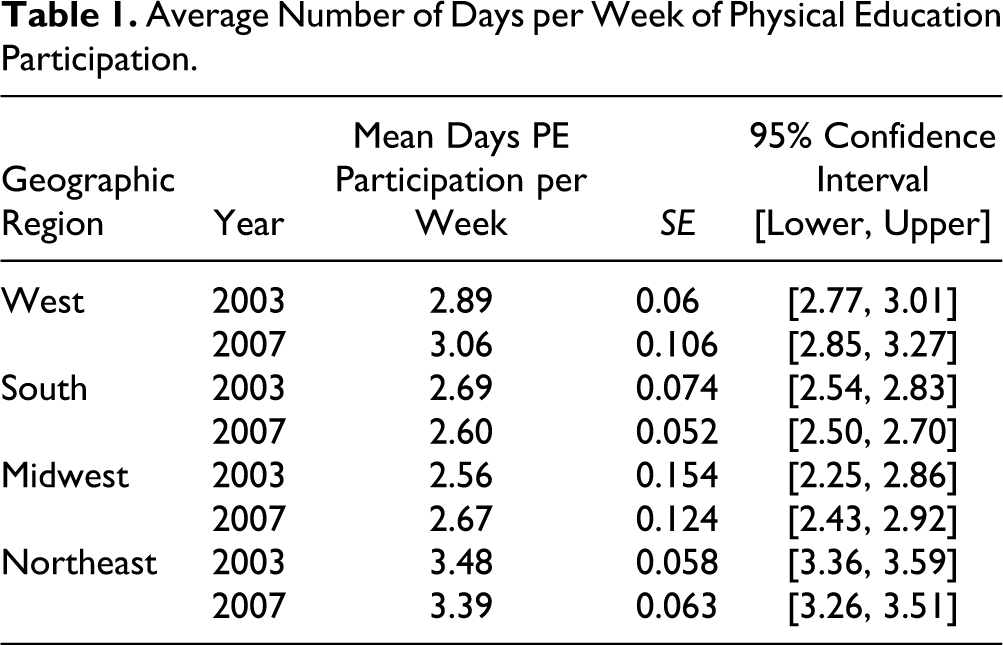
The one-way ANOVA indicated that the self-reported average number of physical education days was not significantly different from 2003 to 2007, F(1, 365) = .519, p = .472. The average number of days of physical education in 2003 and 2007 were 2.91 and 2.93, respectively. See Table 1.
Average Number of Days per Week of Physical Education Participation.
BMI: 2003 Versus 2007
ANOVA results for BMI percentiles in 2003 versus 2007 indicated a significant difference in BMI between the two cohorts of adolescents, F(1, 363) = 5.69, p = .018. The effect size was minimal (d = .04), as the average BMI percentile rank in 2003 was 63.07 compared to 62.18 in 2007. While results were statistically significant, the clinical significance of this difference is negligible.
Geographic Differences: Physical Education Participation and BMI
Physical education participation was found to vary based on geographic region. The results of the Year (2003 vs. 2007) × Region ANOVA indicated a significant main effect for region, F(3,363) = 63.801, p ≤ .001 (i.e., students from the Northeast reported significantly more days of physical education than other regions) but not for year F(1, 365) = .132, p = .717. Finally, there was not a statistically significant interaction for Year (2003 vs. 2007) × Region, F(3, 363) = 1.875, p = .133.
A Year (2003 vs. 2007) × Region ANOVA for BMI percentiles yielded a significant main effect for geographic region, F(3, 361) = 17.50, p ≤ .001, but not year, F(1, 363) = 3.19, p = .075. See Table 2. Adolescents in Southern states, for instance, reported the highest BMI percentiles. A significant interaction between year and region was found, F(3, 361) = 3.66, p = .013. While the effect was minimal (partial η2 = .01), the survey year was differentially influential on BMI percentiles depending on the geographic region of the students.
Average Adolescent BMI Percentile.
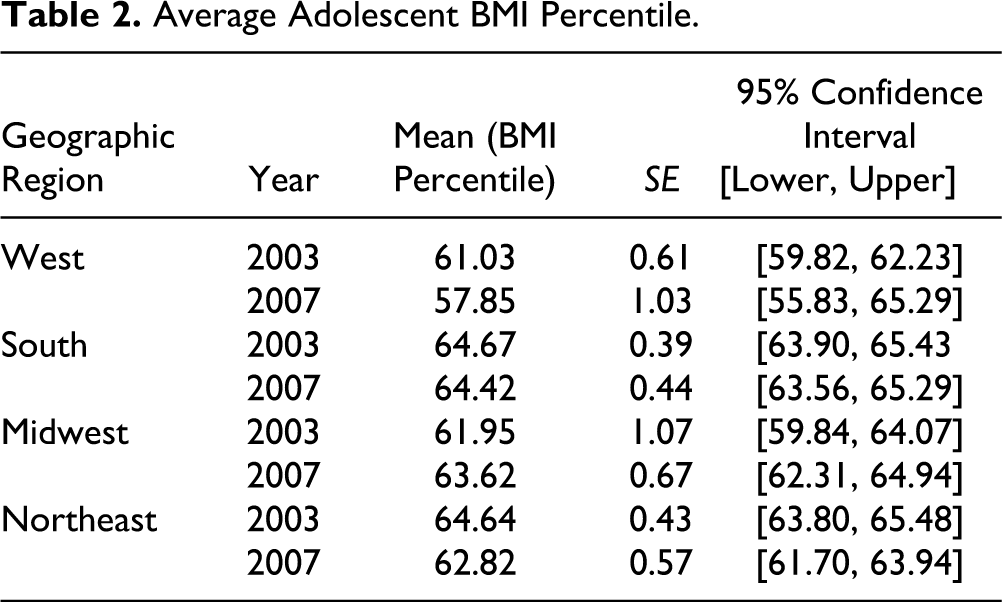
Post hoc analyses were conducted in order to detect specific differences in regional BMI percentiles. Results for the West region indicate a significant decrease in BMI percentiles between 2003 and 2007, F(1, 363) = 7.26, p = .007 (d = .12). Self-reported BMI percentile means in the West were 61.03 (SE = .61) and 57.85 (SE = 1.03) in 2003 and 2007, respectively. Participants in 2003 from the South, Midwest, and Northeast were compared with 2007 participants in these regions: no significant differences were detected.
Discussion
Obesity prevalence among U.S. adolescents has become a national epidemic with far-reaching consequences. In order to reverse this trend, national initiatives to combat the obesity epidemic have been implemented. In 2004, Congress enacted the CNWICRA to direct attention to the important role schools play in the fight against obesity. The legislation required schools participating in the National School Lunch and School Breakfast programs to implement school wellness policies (i.e., by July of 2006) targeting, among other areas, nutrition and physical activity (CNWICRA, 2004).
This study sought to analyze the preliminary influence of the CNWICRA by utilizing self-report data from the CDC’s YRBSS—both pre- and postlegislation. This study was the first to analyze the possible influence of this legislation in these areas.
Legislative Influence on Physical Education Participation?
One objective of school wellness policies addressed physical activity needs and recommendations, but specific guidelines did not accompany this objective. In this study, physical education participation was used as a gauge of legislative compliance in the area of physical activity. As expected, the number of days of physical education participation between 2003 and 2007 was indistinguishable. Adolescents did not report greater participation in physical education in 2007 after the required implementation of the wellness policy portion of the CNWICRA.
Legislative Influence on BMI?
In 2003, the YRBSS revealed an average adolescent BMI percentile rank of 63.59 according to sex- and age-related adolescent categorization. Wellness policies were required to be enacted at the start of the 2006 school year, at the latest, though some were initiated in the 2005 school year. According to the Spring 2007 YRBSS results, the average adolescent BMI percentile rank was 62.57—a statistically significant decline from 2003. The BMI percentile rank of 62.57 still falls within the upper limits of the normal range of BMI percentiles and is not necessarily clinically meaningful relative to 63.59. Ongoing investigation of future YRBSS results will be important.
Geographic Variations in Results
Without specific policy language, many local school districts created wellness policies targeting their own needs. Although this approach allowed the policies to be more individualized, it also led to differential implementation procedures and requirements across various regions of the country.
Results indicated significant differences in physical education participation and adolescent BMI between the four regions of the United States including the West, South, Midwest, and Northeast. Promising results (i.e., significant and meaningful reductions in BMI percentiles as well as an increase in average physical education participation) were found only in the West region, which included the states of Alaska, Arizona, Montana, Utah, and Idaho.
Utah appears to be a model state for school wellness policies since 78% of Utah’s schools complied with guidelines set forth in the CNWICRA (Metos & Nanney, 2007). In this analysis, Utah was part of the geographic region that showed the most significant positive changes in BMI and physical education participation.
Interestingly, participants in the West reported significantly lower BMI percentiles after the implementation of the legislation even when childhood obesity is at epidemic proportions. These findings are consistent with regional research that analyzed adolescent BMI percentiles according to state and regional data (Singh et al., 2008).
The overall goal of the CNWICRA was to provide a way in which schools could combat the growing number of overweight and obese children in the United States. Although consistent results were not detected across regions, the results of the West region may provide preliminary support for the school wellness policies as a preventive tool in the fight against the obesity epidemic when addressed and implemented with integrity.
Limitations and Directions for Future Research
One limitation of this research is the reliability and validity of the self-reported data in the YRBSS. The CDC regularly assesses the validity of YRBSS results, however, reporting confidence in their findings (CDC, 2007). Furthermore, it is difficult to match the breadth of coverage of the YRBSS: The YRBSS included nationally representative data presenting a comprehensive picture of adolescents in high school. This study analyzed data from 86,253 participants. Without the YRBSS, this would not have been feasible. No other tool of this magnitude exists.
Additionally, other variables such as sex, race, and SES may have influenced results in this study and were not controlled in these analyses. SES is of particular concern because the CNWICRA applies to schools receiving federal funding. Unfortunately, a metric for SES was not included in the YRBSS questionnaire. Future research should control for these extraneous variables in order to obtain a clearer understanding of legislation effects.
Within the YRBSS domains, physical education was only measured by days of participation and not actual moderate to vigorous physical activity during class time. In order to better understand the relationship between physical education and possible, associated BMI, physical exertion levels should be measured. Future research may target quantity and quality in order to consider physical education as a tool in preventing obesity.
This study was dependent on the availability of state YRBSS data via the CDC. A more comprehensive understanding may have emerged if more states published health-related data such as YRBSS results. The Midwest, for example, only included one state because of lack of participation or publication of data. Therefore, Midwest results are not likely to be truly representative of the region and should be interpreted with caution.
Finally, the present study analyzed the potential influence of recent federal legislation on physical education and BMI. Nutrition was not addressed. Guidelines outlined in model school wellness policies address nutrition in addition to physical activity. Future research should assess current progress in nutrition and physical activity compliance (Moag-Stahlberg et al., 2008).
Implications
To our knowledge, this was the first published study to analyze whether wellness policy guidelines of the CNWICRA may have been associated with immediate changes in adolescent physical education participation and/or BMI percentiles. Preliminary findings may suggest that some areas of the country have made greater strides than others. Positive patterns in physical education participation and lower BMI percentiles in the Western region, for instance, may imply that meaningful outcomes are associated with previously measured adherence to school wellness policy guidelines (Metos & Nanney, 2007).
Overall, the results of this study suggest that school-based health promotion has legitimate value in the complex and multileveled response to the obesity epidemic. We must take better advantage of this environment to bring about meaningful, lasting change. School nurses and other school-based practitioners can facilitate the development and measurement of meaningful school wellness policies. We must continue advocating for school-based healthy weight promotion, related legislation, and ongoing research evaluating the effectiveness of our efforts.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.