
Abstract
School health teams commonly address the needs of students with asthma, which requires specific knowledge and skills. To develop a skilled school health team, a competency-based framework for managing asthma in schools was developed. A modified Delphi with 31 panelists was completed. Consensus (≥80% agreement) was reached for all 148 items regarding the appropriateness as a minimum competency for asthma care in schools. The resultant Colorado Competency Framework for Asthma Care in Schools guided the development and pilot testing of a continuing education curriculum for school nurses. Pre- and postassessments demonstrated significant improvements in knowledge and self-confidence related to asthma care in schools and inhaler technique skills. This work is the first to use a consensus process to identify a framework of minimum competencies for providing asthma care in schools. This framework informed a continuing education curriculum that resulted in improved knowledge, confidence, and skills for school nurses.
Asthma is a significant health concern in school settings. It is a leading cause of school absenteeism and (Centers for Disease Control, 2016; Meng, Babey, & Wolstein, 2012), if left uncontrolled, can lead to educational disparities (Basch, 2011). Several studies and policies recognize and advocate for school nurses playing an important role in improving the health of students with asthma (Engelke, Swanson, & Guttu, 2013). Previous research highlights that many challenges are faced when managing asthma in the school setting (L. Cicutto et al. 2016; L. C. Cicutto et al., 2006; Nadeau & Toronto, 2015). One of these challenges is the limited knowledge and skill of school nurses and the health team (L. Cicutto et al., 2016; Nadeau & Toronto, 2015). Responding to these challenges, there has been a call to action for school nurse leaders to develop strategies to support school health teams’ delivery of evidence-based, best practice, asthma management in school settings (Nadeau & Toronto, 2015; Vought-O’Sullivan, Meehan, Havice, & Pruitt, 2006). A recommended strategy is that school administrators recognize the need for and support of continuing education for school health teams and that providing continuing education opportunities for school health teams is financially and strategically valuable to school districts (Vought-O’Sullivan et al., 2006). Managing complex chronic conditions, like asthma, requires continuing education for the application of evidence-based knowledge, skills, and judgments that culminate in best practices and healthy and engaged learners.
The healthy learner model, developed by Erickson and colleagues (2006), recognizes that addressing the health needs of students with chronic health conditions requires school nurses and other school health team members to develop and sustain a high level of nursing clinical care expertise. The model proposes bridging traditional clinical care settings and health teams in the school environment supporting students. The healthy learner model proposes an integrated, coordinated attempt to optimize student health and support academic success of students affected by chronic health conditions (Erickson et al., 2006). The model is dependent upon two fundamental prerequisites being available in the school setting. The first is a professional school nurse with a baccalaureate degree who displays knowledge, skills, and expertise in school nursing and the second is a key facilitator such as the availability of a chronic disease resource nurse to the school setting. A chronic disease resource nurse has specialized chronic disease expertise and serves as a champion for evidence-based initiatives and mentors other school nurses. In addition, chronic disease resource nurses foster partnerships between community health-care professionals, families, and schools. These partnerships are necessary for making students healthy learners and optimizing students’ academic performance and health status.
Colorado has embraced the healthy learner model. The model for providing supportive health care to students, for most Colorado schools, is to rely on a school health team. Members of these teams typically consist of school nurses, unlicensed assistive personnel (UAP), and secretaries. Very few Colorado schools have a dedicated school nurse in the building 5 days a week (Colorado Department of Education (unpublished report), personal communication, August 25, 2016). In general, most school nurses in Colorado are prepared at the bachelor’s level. UAP are trained to function in an assistive role to the registered professional nurse in the provision of activities of care as delegated by and under the supervision of a registered professional nurse (American Nurses Association, 2010). If permitted by state law, activities UAP can perform with proper training and oversight by the school nurse include screenings, maintaining student health records, noncomplex daily activities, first aid and selected emergency procedures, student-specific nursing tasks, administer medications, and other school health office tasks (Bobo, 2014; Raible, 2012). In Colorado, there are school health consultants and chronic disease specialists who provide support to school health teams in addressing knowledge and skill gaps and implementing evidence-based practices. In general, large school districts have their own chronic disease resource nurses. The Colorado Department of Education’s school health wellness practice model includes regional school health nurse consultants who are assigned to regions across the state to support all school districts in the assigned region. This role supports school nurses related to school health practices and standards and for supporting student with chronic health conditions. For smaller districts, the regional school health nurse consultants are the only source of support for school nurses. For the purposes of our model and this article, we use the broader term school health nurse consultant to also include chronic disease specialist, chronic disease resource nurse, and school health consultant. All of these roles recognize the role as a key leader with specialized knowledge for building capacity and evidence-based care within school settings. Asthma is one of the more common conditions and reasons for requiring school health services in Colorado schools (Colorado Department of Education (unpublished report), personal communication). In Colorado, an informal consortium of the Colorado Department of Education, Colorado Department of Public Health and Environment, school districts, and health-care organizations have collaborated and worked together to achieve the common goal of providing evidence-based best practices for asthma management in school settings to reduce health and educational disparities for students with asthma. To achieve this goal, there is recognition for the need to develop a comprehensive and consolidated competency-based framework for providing evidence-based, best practice, asthma management in schools settings that addresses the varying roles of school health teams. This framework would subsequently be used to inform continuing education curricula and serve as a minimum competency framework for the school health team according to the role, school health consultant/chronic disease specialist, school nurse, UAP, and secretaries. The purpose of this article is to describe the development and application of a competency-based framework, which was subsequently used to develop and pilot a continuing education curriculum for school nurses.
Method
Development of Competency Framework for Asthma Care in Schools
The lens of two conceptual frameworks, the National Asthma Educator Certification Board, Certified Asthma Educator competency framework (National Asthma Educator Certification Board, 2015), and the healthy learner model (Erickson et al., 2006) were used to inform the development of our competency-based asthma care in school settings framework. The competencies of the National Asthma Educator Certification Board, Certified Asthma Educator competency framework were used as a starting point for this project, as it serves as the standardized national framework for asthma care competencies that are not oriented to prescribing practices and written for multiple disciplines and training levels. The healthy learner model provides the focus on bridging traditional clinical asthma care to school settings by a trained and qualified school health team that has a leader to support competency development of the school health team and build capacity for implementing evidence-based practice. A modified Delphi was used to inform the development of the Colorado competency framework. A Delphi technique is a process for consensus building that uses an iterative series of survey questions to collect opinions from a panel of informed participants concerning a specific topic (Hsu & Sandford, 2007).
Three iterative rounds were used to seek information and consensus of opinion among an informed respondent group to develop the Colorado Competency Framework for Asthma Care in Schools. In each round, every participant worked through a questionnaire, which was returned to the coordinator who collected, edited, and returned to every participant a statement of the position of the whole group that was used to compare to individual responses. The feedback process allowed and encouraged participants to reassess their initial judgments about the information provided. The Delphi technique provided anonymity to respondents and a controlled feedback process.
As scoping was previously completed by the National Educator Certification Board, the current study used a modified Delphi survey (Hasson, Keeney, & McKenna, 2000; Hsu & Sandford, 2007; Keeney, Hasson, & McKenna, 2011) to serve as the content of the Delphi survey. For our project, Round 1 used a predefined list of competencies derived from the National Educator Certification Board—an acceptable modification of the Delphi process (Hsu & Sandford, 2007) and all of the competencies identified on the board’s Certified Asthma Educator competency framework were items on the questionnaire. Respondents were asked to identify for each competency item whether or not it was appropriate for each of the following roles of school health teams: school health nurse consultant, school nurse, UAP, and secretaries. A contextual element missing from the National Asthma Educator Certification Board’s Certified Asthma Educator competency framework important for the purpose of this project was the integration of asthma care into the school setting (vs. a traditional clinic setting). To address this gap, we added 6 competency items related to asthma care in schools and tailored the competency where possible and appropriate to reflect the school community context. In total, the first round questionnaire had 148 items. Questions/items were distributed across four domains: the asthma condition, assessment of a student with asthma and family, asthma care, and organizational issues. For Round 2, only items for which there was no consensus were included in the questionnaire. Consensus was defined as 80% or greater agreement assigned for each item among panel members. Each participant received a second questionnaire and was asked to review and rate the items summarized by the coordinator based on the information provided in the first round. In the third round, each panelist received a questionnaire that included the competency items associated with disagreement or lack of consensus and summarized ratings of appropriateness. In addition, prior to submitting their ratings for the third round, panelists were encouraged to participate in a telemeeting held to discuss the remaining areas of disagreement and the reasons.
Since the Delphi technique focuses on eliciting opinions over a short period of time, the selection of panelist members is generally dependent on areas of expertise related to the specific topic and takes into account (1) decision makers who will use the outcome, (2) professional staff members who are the end users, and (3) those whose judgments are being sought for their insight (Hsu & Sandford, 2007). Based on these guidelines, our respondent group included school health leaders (5), regional school health nurse consultants (5), chronic disease school nurse specialists (3), school nurses (6), UAP (8), school secretaries (4), and asthma specialists (7); and nurse practitioner, physician assistant, medical assistants, and certified asthma educators with experience working in school settings. Some individuals are counted more than once as they represent multiple roles and perspectives, for instance, there is an individual who is a school nurse, a certified asthma educator, and a regional school health nurse consultant. In total, there were 31 individuals who formed the respondent panel. Purposive sampling was used to involve those from rural and smaller school districts and for state geographic diversity. School secretaries only provided ratings for the items pertaining to their own school health team role, as this is what they felt most comfortable with in providing expertise and insight.
Analysis involved determining the frequencies for each item on the questionnaire for the three response categories of appropriate, uncertain/unclear, and not appropriate for each of the four school health team roles. We used the cut-point of 80% agreement among respondents for either appropriate or inappropriate to indicate that consensus was reached for each competency criterion for each health team role (Fitch et al., 2011; Hsu & Sandford, 2007). Content analysis was used to analyze and organize data collected from open-ended questions that primarily occurred for ratings of uncertain/unclear or to tweak the wording of individual competencies.
Development and Implementation of Training Curriculum
The end product of the modified Delphi, described above, was the development of the Colorado Competency Framework for Asthma Care in Schools. This framework was used to develop and pilot a curriculum to support the attainment of minimum competencies for school nurses. The curriculum model developed for preparing school nurses was a hybrid model that included successful completion of a professional-community online asthma program and attendance at a local face-to-face, hands-on, problem-based workshop. School nurses successfully completed Asthma and Allergy Foundation of America’s continuing education for health care professionals’ Asthma Management and Education Online course (http://www.aafa.org/page/continuing-education-for-health-care-professionals.aspx) before attending a local, skill-based workshop. The target audience for the online course is health professionals who teach and care for people with asthma. The content follows the National Asthma Education and Prevention Program, National Heart, Lung, and Blood Institute, National Institutes of Health’s (2007) Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma and is covered through 12 units that learners complete at their own speed, usually around 3 hr. In addition, school nurses could earn seven continuing education credits for online course completion. The online course requires completion of a learning outcome assessment (quiz) to determine whether or not learning outcomes were attained. Before attendance at a local face-to-face workshop, school nurses submitted proof of successful completion of Asthma and Allergy Foundation of America’s online course.
The face-to-face workshop was developed to contextualize and operationalize asthma management to the school setting. Specifically, the half-day workshop reviewed the recommended standardized forms and resources of the Colorado Department of Education and consisted of problem-based application of knowledge and skills through case studies and hands-on skill assessment for inhaler technique. School health nurse consultants (typically from the Colorado Department of Education) and community asthma clinicians delivered the face-to-face workshops to school nurses. Prior to serving as the trainers for school nurses, school health nurse consultants were required to successfully complete the Asthma and Allergy Foundation of America’s Asthma Management and Education Online course, attend over 8 hr of face-to-face training regarding best practices of asthma care in the school setting, existing resources to support best practice asthma care, capacity building for evidence-based practice, and a motivational interviewing workshop. For our project, pre- and postlearner assessments were completed for asthma care in schools knowledge, self-confidence, and inhaler technique.
Results
Development of Competency Framework for Asthma Care in Schools
After three rounds, consensus (at least 80% agreement) was reached for each proposed competency, either as an appropriate or inappropriate competency for the school health team roles of school health nurse consultant, school nurse, UAP, and secretary. Participation rates of panelist members for all three rounds were greater than 85% and greater than 80% for attendance at a review meeting held as part of Round 3. Round 1 used a structured questionnaire that included the competencies identified in the national Certified Asthma Educator competency framework plus questions to capture additional areas important to the school setting. Areas of competency disagreement or lack of consensus were noted for all four roles: 10 items (6.8%) for school health nurse consultant, 33 items (22.3%) for school nurses, 26 items (17.6%) for UAP, and 10 (6.8%) for school secretaries. It was most common to have competency item disagreement specific to the individual school health team role. However, some competency items of disagreement overlapped between the two roles. For instance, the competency area of the use and interpretation of objective lung function tests was associated with disagreement for the school health nurse consultant and the school nurse role, and for both the UAP and secretary roles, competency disagreement was noted for identifying asthma control and directing a call for emergency medical care based on the student’s presentation. Refer to Table 1 for results. Round 2 only included items for which there was no consensus. Areas of disagreement persisted for school nurses (10 items, 6.8%), UAP (8 items, 5.4%), and secretaries (3 items, 2.0%). Consensus was reached for all (100%) items for the role of school health nurse consultant role. In Round 3, consensus was reached for all remaining areas of disagreement for school nurses, UAP, and secretaries. Typically, the reason for disagreement was the wording and varying interpretations of the item competency. The meetings held as part of Round 3 were helpful in reaching consensus by clarifying interpretation and wording.
Areas of Competency Disagreement Identified in Round 1 According to Role.
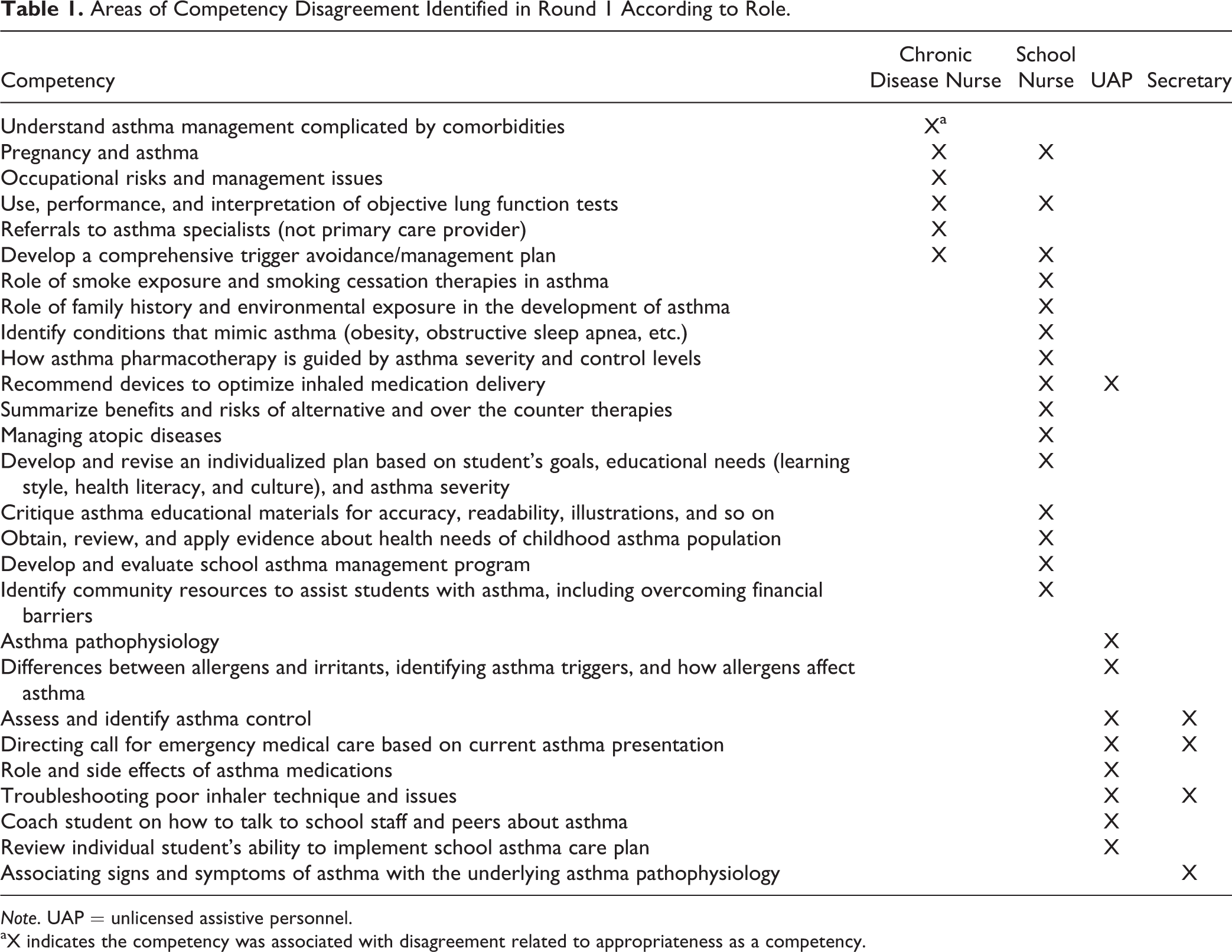
Note. UAP = unlicensed assistive personnel.
aX indicates the competency was associated with disagreement related to appropriateness as a competency.
Based on the results of the three rounds of the modified Delphi, the Colorado Competency Framework for Asthma Care in Schools was developed. This framework is available at the Colorado Department of Education’s website (https://www.cde.state.co.us/healthandwellness/snh_healthissues) and includes the minimum competencies for the four school health team roles: school health nurse consultant, school nurse, UAP, and secretaries. The minimum competencies are also available for review at The Journal of School Nursing website at this link.
Development and Implementation of Training Curriculum
As described above, based on the Colorado Competency Framework for Asthma Care in Schools, a curriculum was developed to support school nurse competency attainment. Five workshops were held and attended by 40 school nurses who had successfully completed the Asthma and Allergy Foundation of America’s continuing education for health care professionals’ Asthma Management and Education Online course prior to their attendance. School nurses reported that it took them from 2 to 10 hr to complete the online course and that it was completed in one session to multiple sessions over 3 weeks. Overall, the school nurses rated the online course favorably. Strengths of the course were that it is free of charge, provides continuing education credits, and could be completed when the learner had the time (any time during any day–night). The comprehensive nature of the course related to asthma management was identified as both a strength and a weakness. Some participants remarked that they were uncertain how they would apply some of the detailed clinical information while others commented that the extensive clinical information would be very helpful in informing their care. Limitations identified included the inability to ask questions as the learner was covering the material and that it was targeted more for the clinical setting. The range reported for time to complete the online course was due to the individual learner’s baseline understanding of asthma management in the clinical setting regarding diagnostics and pharmacologic and nonpharmacological approaches. Those with less understanding took longer to complete the course and those who reported completing the course over multiple weeks reported longer time duration to complete, as they were going back to review topics covered to reorient themselves to the content.
After successful completion of the online course, school nurses attended local workshops that focused on providing asthma care in the school setting. Workshop participants completed pre- and postassessments for knowledge and self-confidence regarding asthma care in the school setting and metered-dose inhaler technique using a standardized tool (L. Cicutto, To, & Murphy, 2013; L. C. Cicutto et al., 2005). At baseline, knowledge assessment related to evidence-based asthma care in schools revealed gaps in identifying and prioritizing students with at-risk asthma and in need of closer monitoring and service provision, some confusion with the ability to share information and communicate with health-care providers (Family Educational Rights and Privacy Act (FERPA) and Health Insurance Portability and Accountability Act (HIPAA)), and identifying important asthma outcomes/indicators to follow and how to assess them. At baseline, self-confidence was lowest for identifying the at-risk status for students with asthma and for providing care and education to support implementation of the Colorado School Asthma Care Plan. Following workshop attendance, statistically significant improvements were noted in knowledge, confidence, and inhaler skills (refer to Table 2). Asthma knowledge almost doubled from pre- to postassessment (45–90%). Self-efficacy was assessed on a scale of 0 (not at all confident) to 4 (completely confident). Scores increased from 2.4 to 3.3 for self-efficacy from pre- to postassessments. Participant inhaler technique also improved following the workshop with improvements in scores from 3.6 at baseline to 4.8 postworkshop. The theoretical score range for inhaler technique was 0 (no steps performed accurately) to 5 (all steps performed accurately). Participants’ overall satisfaction with the workshops was very high (3.8 out of 4). Aspects favored by participants included demonstrations and hands-on practice with feedback for various inhaler device techniques, opportunities to ask lots of questions with discussion, and the practical ideas and standardized approaches provided for managing asthma in school settings.
Pre- and Postscores for School Nurses’ Inhaler Technique and Knowledge and Confidence Related to Asthma Care in Schools.
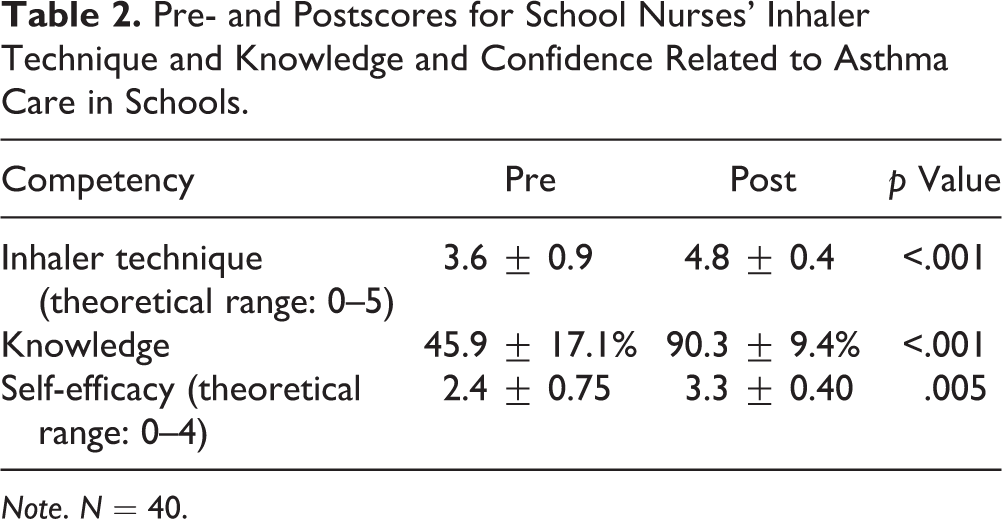
Note. N = 40.
Discussion
In summary, the modified Delphi technique was a useful, fast, and ultimately successful method for attaining consensus among panelists for four school health team roles (school health nurse consultant, school nurse, UAP, and secretaries) regarding the minimum competencies for providing evidence-based asthma care in schools. After three rounds, consensus was reached for all 148 items in terms of the appropriateness or inappropriateness as a competency necessary for providing asthma care in schools for the four school health team roles. Based on the results of the modified Delphi, the Colorado Competency Framework for Asthma Care in Schools was developed and includes all of the minimum competencies for each of the four school health team roles that attained consensus (≥80%) and identified as an appropriate competency. This framework can be accessed through the Colorado Department of Education’s website at https://www.cde.state.co.us/healthandwellness/snh_healthissues
The Colorado Competency Framework for Asthma Care in Schools guided the development of a continuing education curriculum for preparing school nurses to provide asthma care in schools. The developed curriculum uses a hybrid model of an online professional continuing education course for asthma management and a face-to-face workshop that focuses on the application of knowledge and skills to support students with asthma and the provision of evidence-based asthma care in schools. The hybrid model was viewed favorably by school nurses and resulted in improvements in knowledge and self-confidence related to providing asthma care in schools and improved inhaler technique skills.
The modified Delphi worked well for this project. We were able to maintain participation rates greater than 85%, had less than 2% missing data, and were able to complete the data collection process in 3 months. Participation rates suggest that panelists felt motivated and engaged in the project. The number of panelists was on the smaller side but still within the range recommended (Hasson et al., 2000; Hsu & Sandford, 2007; Keeney et al., 2011). Panelists were selected to represent the diverse opinions of the school heath team member roles while having expertise and/or experience with asthma care in school settings. We invited a smaller number of panelists because we felt it was important to keep those participating engaged throughout the entire process. We did not provide incentives for participants. Panelists reported that the quick turnaround time between submitting data and receiving the results and feedback was important to maintaining momentum and engagement in the Delphi process.
This project was novel and innovative in several ways. To our knowledge, this work is the first to use the Delphi consensus approach to develop a minimum competency-based framework that was used to develop a continuing education curriculum for school nurses. Additionally, the work is novel through its identification of minimum competencies for differing roles of the interdisciplinary health team for asthma care in schools. The hybrid continuing education model for school nurses was also innovative through its use of an existing free resource available from a well-respected professional society that is accessible to all school nurses and then extends learning with tailored application to the school setting through face-to-face problem-based workshops.
Our competency framework and continuing education incorporated the healthy learner model (Erickson), the work by Hoyle, Samek, and Valois (2008), for building capacity for schools and the quality and safety education for nurses framework (Cronenwett et al., 2007). The work by Erickson et al. (2006) and Hoyle et al. (2008) support the need for collaborative interagency relationships. Community (health care), schools, and educational sector leadership partners were involved in all aspects of the project (project design, Delphi process, review of results, workshop design, and provision) and will have sustained involvement in implementation across the state. Working together, community asthma experts and school health nurse consultants provided the tailored learning workshops to school nurses. Consistent with the works of Hoyle, Samek, and Valois (2008) and Erickson (2006) was the involvement of community asthma care providers in consultative and technical assistance roles to facilitate and advance schools and districts to move beyond current practice to practice aligned with best available evidence. Community asthma providers were important to provoking critical thinking and the exploration and identification of possibilities that best meet the needs of students and families affected by asthma. Ouellette (2000) suggests that external technical assistance, such as the involvement in community asthma clinicians, often inspires and forces schools and districts to think about how to incorporate best evidence practices. All parties involved in the project acknowledge that the synergies created through collaboration exceeded what anyone entity could have accomplished.
As a result of the pilot work success, our continuing education efforts will continue to target school nurses and will be extended to chronic school health nurse consultants and UAP across the state using a train the trainer model. To support implementation of best asthma practices in the school setting, our train the trainer model will include school health nurse consultants completing the same requirements of those who participated in the pilot project who will serve as school nurse trainers. Those school health nurse consultants who participated in the pilot project will serve as trainers for other school health nurse consultants. Once school nurses have completed the training elements, they will be charged with training school nurses using the curriculum materials described in this article. School nurses will be charged with training UAP. To support school nurse training of UAP, support materials for delivering the competency-based curriculum will be developed. The training of school health nurse consultants, school nurses, and UAP will use the Asthma and Allergy Foundation of America’s online asthma management course. However, due to its comprehensiveness and intended target audience, a separate resource for school secretaries will need to be identified or developed. It is anticipated that school nurses will complete this training with school secretaries. The Colorado Department of Education Office of Health and Wellness will be promoting the framework and curriculum across the state and will be implementing the work through the regional school health nurse consultant roles. In addition, existing school-centered asthma programs in Colorado will be supporting and implementing the framework. Based on the success of this pilot work, the approach may be replicated for managing life-threatening allergies in schools.
There is great diversity in workforce models used in school systems across the United States to meet the health needs of students. As mentioned, most Colorado school districts have UAP as part of their school health teams and/or often rely on secretaries for additional coverage of care. However, several school systems in the United States do not have UAP or school health nurse consultants. In addition, some states do not allow school nurses to delegate medication administration to UAP or school secretaries. The full Colorado Competency Framework for Asthma Care in Schools may not be applicable or generalizable to all school systems because of the variance in school health workforce models. However, at the core of the framework is the school nurse. The school nurse is the most critical role for the provision of evidence-based quality asthma care in schools. This framework is helpful to school nurses through the identification of asthma care competencies and for a training resource that is available free of charge to lay a solid foundation for providing guideline-based asthma care. The Colorado Competency Framework for Asthma Care in Schools provides a structure and resource that is adaptable to a variety of school health workforce models.
Footnotes
Author Contribution
All authors contributed to this work and article in the following ways: (1) contributions to conception and design, or acquisition of data, or analysis or interpretation of data; (2) drafting the article or revising it critically for important intellectual content; and (3) final approval of the version to be published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by funding received by the Colorado Department of Public Health and Environment’s Cancer, Cardiovascular and Pulmonary Disease Program, and the Colorado Kaiser Permanente Foundation.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.