
Abstract
This study investigated the association between school-based health centers (SBHCs) and sexual behavior and contraceptive use among 11th graders. The sample included 134 high schools (27 schools with SBHCs) and 11,840 students who participated in the 2015 Oregon Healthy Teens Survey. Multilevel logistic regressions found positive associations between SBHC presence and healthy sexual behavior (OR = 1.23, p < .05) and contraceptive use (OR = 1.31, p < .01). Associations were stronger at schools with at least 50% of students receiving free or reduced price lunch. Among SBHC schools, prescribing and dispensing contraceptives onsite was positively related to contraceptive use among students who had sex within the past 3 months (OR = 1.77, p < .01). Findings suggest that exposure to SBHCs in general, and availability of specific reproductive health services, may be effective population-based strategies to support healthy sexual behaviors among youth.
School-based health centers (SBHCs) are designed to provide low-cost, easily accessible, and youth-friendly health-care diagnosis, referral, and treatment services. Services may include immunizations, checkups, family planning, mental health care, dental services, and vision care that are delivered by a medical professional such as a doctor or nurse practitioner. Reproductive health visits are among the most common reasons adolescents seek care at SBHCs (Allison et al., 2007; Amaral, Geierstanger, Soleimanpour, & Brindis, 2011; Juszczak, Melinkovich, & Kaplan, 2003; Soleimanpour, Geierstanger, Kaller, McCarter, & Brindis, 2010), suggesting that SBHCs may have the capability to positively impact youth sexual and reproductive health (SRH) behaviors. The current study has the following two overall aims: (1) to examine whether there is a relationship between SBHC exposure and adolescent SRH behavior and whether this is moderated by socioeconomic status, race/ethnicity, and/or gender and (2) to investigate whether the type of contraceptive services offered within schools with SBHCs is associated with reported contraceptive use.
Research suggests that physical availability of and access to family planning clinics may reduce adolescents’ risk for early sexual intercourse and increase the likelihood of effective contraceptive use among those who are sexually active (Bersamin et al., 2011; Bishai et al., 2005; Brewster et al., 1993; Grady et al., 1993; Katende et al., 2003). Yet adolescents often have limited access to health-care services, particularly reproductive health services, due to a wide array of financial and social barriers such as cost, transportation, convenience, availability, and confidentiality concerns (Bender, 2013; Carroll, Lloyd-Jones, Cooke, & Owen, 2012; Lindberg, Lewis-Spruill, & Crownover, 2006). SBHCs address these barriers by providing youth with easily accessible, affordable, and confidential services either directly or indirectly through increased knowledge or referral to another service provider.
Research to date has noted a positive, though equivocal, relationship between access to an SBHC and a range of adolescent reproductive health outcomes. For example, one study comparing youth with and without access to an SBHC on campus found a lower likelihood of engaging in sexual intercourse among those with SBHC access (Hutchinson, Carton, Broussard, Brown, & Chrestman, 2012). Another study found that sexually experienced female students with SBHC access were more likely to have ever used a hormonal birth control method and more likely to have used a hormonal method at first and last intercourse (Minguez, Santelli, Gibson, Orr, & Samant, 2015). The effect was found to extend to males regarding ever having used condoms, with lifetime use significantly higher among males with SBHC access compared to those without. A study of 12 schools in California also found that among females, SBHC access increased the odds of having used hormonal contraceptives or emergency contraception at last sex (Ethier et al., 2011). Other studies have noted that SBHC users were more likely to report higher levels of screening and/or counseling to prevent pregnancy and sexually transmitted diseases (STDs) than nonusers, controlling for demographic variables (Klein et al., 2007) and higher levels of pregnancy or STD prevention care among females (Ethier et al., 2011). Notably, however, results are not consistent across studies, with some research finding significant SBHC effects among males while others did not (Ethier et al., 2011) and some noting an impact of SBHCs on birth control use while others did not (Hutchinson et al., 2012).
Despite substantial growth in the establishment of SBHCs across the United States, empirically investigating their influence on youth SRH behavior (as well as other health outcomes) has been challenging. The lack of definitive findings may be a function of methodological limitations (Bersamin et al., 2016; Keeton, Soleimanpour, & Brindis, 2012; Mason-Jones et al., 2012) including small sample sizes, which reduce statistical power and make it more difficult to detect effects of SBHCs; lack of randomized controlled designs, which help control for selection bias; and the failure to account for the hierarchical structure of multisite data, among others. Additionally, studies using comparison groups have often been conducted between schools with and without an SBHC or among users and nonusers of an SBHC. In most studies, SBHCs have been treated as a single, homogenous entity, with no accounting of the substantial differences that exist across clinics in services offered or other SBHC characteristics (e.g., hours open, staffing, and policies). For example, a recent study noted that these characteristics are critical as clinics that provide more than 10 hr per 100 students of doctor and nursing time had an inverse relationship with number of pregnancies (Denny et al., 2012). More research is needed that examines whether and to what extent (1) SBHCs have differential effects among various student subgroups defined by gender, SES, and race/ethnicity, an evidence gap identified by the Centers for Disease Control (CDC) (Guide to Community Preventive Services, 2015) and (2) unique SBHC services have differential impact on various adolescent health outcomes.
The current study aims to assess SBHC impact on adolescent SRH while also addressing several of the methodological issues associated with this work by (1) using a large statewide data set with a large number of high schools, (2) employing multilevel modeling to adjust for clustering, and (3) controlling for school-level characteristics to address selection issues.
Because SBHCs aim to serve the health needs of low-income underserved youth, we hypothesize that SBHCs will have a larger effect on adolescent SRH (1) in schools with a greater proportion of low-income students and/or a higher percentage of minority youth and (2) at the individual level among lower income youth and/or minority youth. The percentage of young males receiving SRH services is low, estimated at 3–20% (Armitage, Curran, Wright, Lenehan, & Kell, 2004). Therefore, we also expect that the association between SBHCs and SRH behaviors will be stronger for females versus males. In the absence of subgroup differences, given that many SBHCs conduct school-wide outreach (e.g., displaying posters, hosting health events, and supporting and educating teachers and administrators), we hypothesize that young people with access to SBHCs will have more positive and healthy SRH behaviors compared to their peers attending schools without SBHCs. Finally, we hypothesize that SBHCs that provide contraceptive services will have a greater proportion of sexually active students who report contraceptive use.
Method
This study is based on survey data collected in 2015 from a sample of 11th graders in Oregon public high schools and information on SBHCs provided by the Oregon Health Authority Public Health Division. All study procedures were approved by the institutional review board of the Pacific Institute for Research and Evaluation.
Study Sample
The study sample comprises 134 Oregon high schools and 11,840 eleventh graders who participated in the 2015 Oregon Healthy Teens (OHT) survey and provided complete data for study variables. This represents 87% of all 11th graders (N = 13,608) who participated in the OHT in 2015. Of the 134 high schools, 27 (20.1%) had SBHCs. The OHT survey is a self-administered population survey of 8th and 11th graders conducted in odd-numbered years in a representative sample of Oregon middle and high schools. All Oregon public secondary schools were included in the sampling frame. Districts were randomly sampled; in larger districts, schools were also randomly sampled from within those districts. The survey data were weighted to achieve a statewide representative sample based on the probability of students being selected. The survey is voluntary, anonymous, and takes about one class period to complete. Information on SBHCs was provided by the Oregon Health Authority Public Health Division, including which high schools were served and whether they prescribe and/or dispense contraceptives.
Measures
Sexual behavior, lifetime
Students were asked whether they ever had sexual intercourse (1 = yes, 0 = no). If they responded affirmatively, they were asked what type of contraceptive (e.g., IUD, birth control pills, condom, and none) they used the last time they had sexual intercourse with all applicable methods checked. A dichotomous measure for using a contraceptive during last sexual intercourse was created (used contraceptive = 1, didn’t use contraceptive = 0).
Healthy sexual behavior, lifetime
We followed a definition for healthy sexual behavior proposed by the Office of Adolescent Health (Colman, 2012). Specifically, youth who avoided unprotected sex by using contraception at last intercourse and youth who had not reported having sexual intercourse were coded as (1) and those who had sex without protection were coded as (0).
Sexual behavior, past 3 months
Students who reported ever having sex were also asked how many partners they had in the past 3 months. From this item, we created a dichotomous variable indicating whether they had sexual intercourse in the past 3 months. Students who reported having sexual intercourse in the past 3 months were also asked whether they used contraception at last intercourse.
Demographic characteristics
Students reported their age, gender, ethnicity, race, and whether they received free or reduced price lunch (FRPL). Ethnicity was treated as a dichotomy (Hispanic vs. non-Hispanic). Because the majority of students (78.4%) reported their race as White, this was also treated as a dichotomous variable.
School characteristics
School characteristics included presence/absence of an SBHC, total student enrollment, percentage of students who were non-Hispanic and non-White, and percentage of students receiving FRPL. Two school-level dummy variables were created based on median scores for school-level data on FRPL (50% or more of students received FRPL) and percentage of non-Hispanic and non-White (25% or more of students). Within SBHC schools, we also examined whether SBHCs prescribed contraceptives and whether they also dispensed contraceptives. These were treated as dichotomous variables.
Data Analysis
Descriptive analyses were first conducted to examine sample characteristics and compare schools with and without SBHCs among the total sample of 11th graders. Multilevel regression analyses were then conducted to assess the association between SBHC presence and sexual behaviors including healthy sexual behavior among the full sample and contraceptive use and having sexual intercourse in the past 3 months among those who reported ever having sexual intercourse. All analyses controlled for school and student demographic characteristics. Main effects of SBHC presence were examined in initial regression models. Interaction terms were included in subsequent regression models to examine possible moderating effects of socioeconomic status, ethnicity, race, and gender. School-level SBHC Status × Percentage of Students receiving FRPL, SBHC Status × Percentage non-Hispanic and non-White, and corresponding main effects were included in regression models. Cross-level interaction terms for school SBHC status and student characteristics (e.g., SBHC × Gender) were also included in regression models. Nonsignificant interaction terms were dropped from analyses. The nature of significant interactions was investigated in graphical plots. Multilevel regression analyses were also conducted within the subgroup of schools with SBHCs to examine possible associations between family planning services and sexual behaviors. Multilevel regression analyses were conducted with HLM Version 7.01 software to adjust for variance attributable to observations nested within schools (Raudenbush et al., 2011). Sample weights provided with the OHT survey data were applied in descriptive and regression analyses.
Results
Sample Characteristics
As shown in Table 1, 11th graders at schools with and without an SBHC on campus did not differ on several demographic characteristics including age, gender, and race. However, the percentages of students who were Hispanic and receiving FRPL were significantly higher at non-SBHC schools compared to schools with an SBHC. Regarding SRH behaviors, about 41% of the students reported ever having sex. Ninety-two percent reported healthy sexual behavior—either abstaining from sex or using a contraceptive the last time they had sexual intercourse; a higher percentage of 11th graders at schools with SBHCs reported healthy sexual behavior (93%) compared to students at non-SBHC schools (91%). Among youth who ever had sex, about 73% reported having sex within the last 3 months and 79% reported using some type of contraceptive the last time they had sexual intercourse. A higher percentage of sexually active 11th graders at schools with SBHCs reported using a contraceptive the last time they had sex (83%) compared to students at non-SBHC schools (78%).
Student Sample Characteristics, Mean (SD) or Percent.a
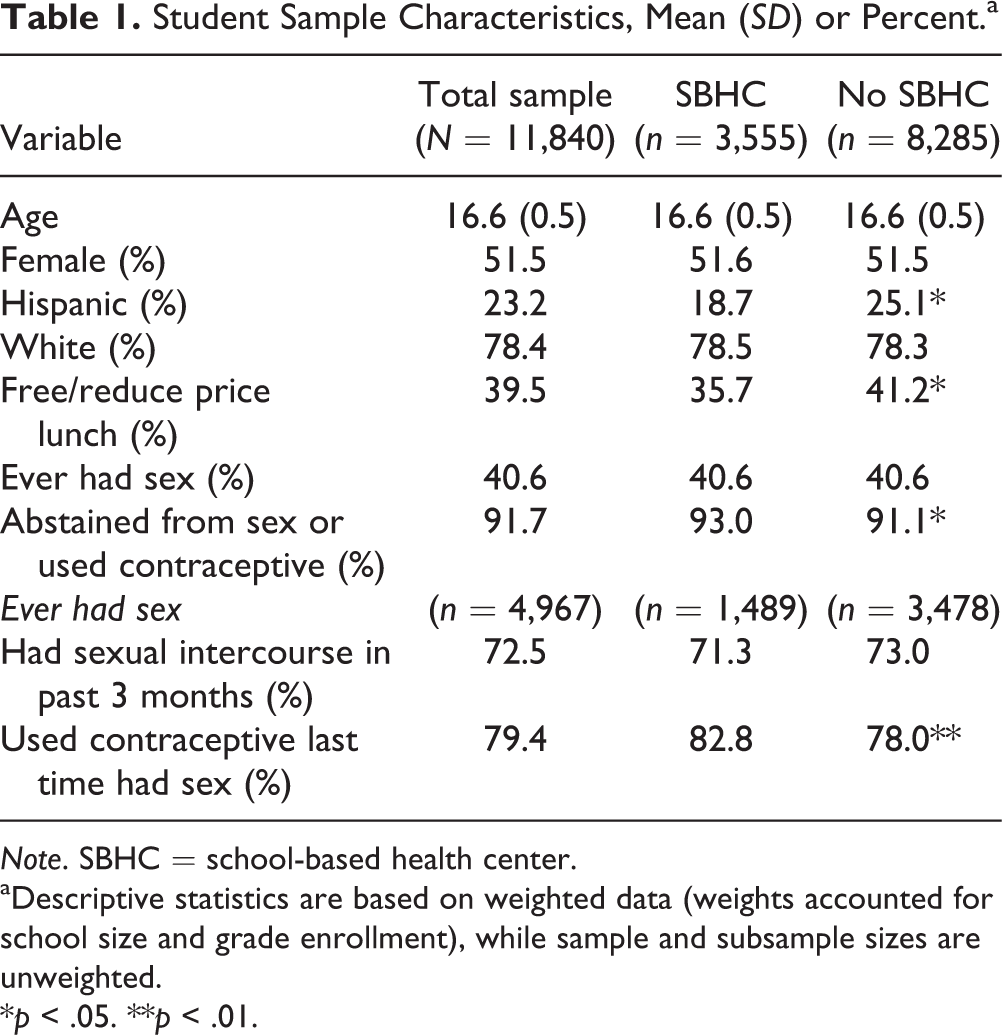
Note. SBHC = school-based health center.
aDescriptive statistics are based on weighted data (weights accounted for school size and grade enrollment), while sample and subsample sizes are unweighted.
*p < .05. **p < .01.
School characteristics are provided in Table 2. Schools with an SBHC had a significantly greater mean student enrollment level than non-SBHC schools, but schools with and without an SBHC were similar with respect to the mean percentages of non-White, non-Hispanic students, and students eligible for FRPL. Of the 27 schools with an SBHC, 74% prescribed contraceptives, while 52% prescribed and dispensed contraceptives.
School Characteristics, Mean (SD) or Percent.
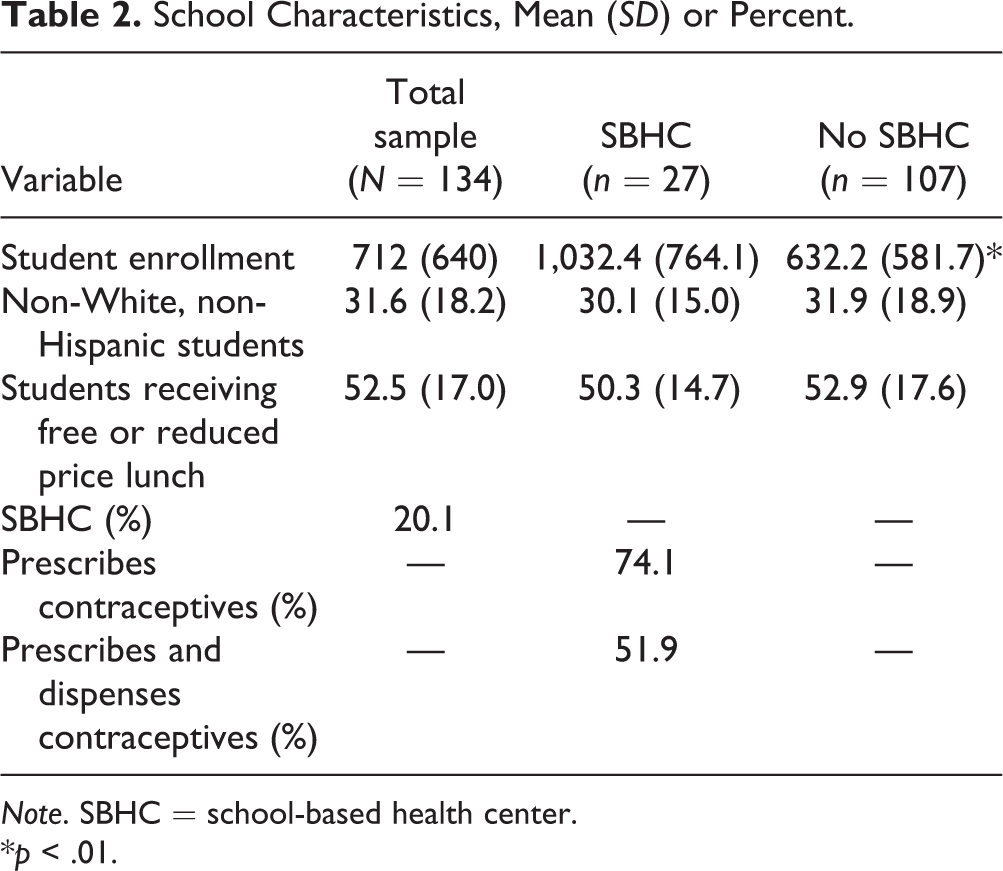
Note. SBHC = school-based health center.
*p < .01.
Multilevel Regression Analyses
Healthy sexual behavior
Results of multilevel logistic regression analyses for healthy sexual behavior with the total sample of 11th graders are reported in Table 3. The initial regression model (Model 1) indicates a positive association between SBHC presence and the likelihood of healthy sexual behavior when controlling for other school and student demographic characteristics. Students at SBHC schools were 23% more likely to report healthy sexual behavior than students at non-SBHC schools. Of the interaction terms included in subsequent regression models, only SBHC × FRPL (school level) was statistically significant, as shown in Model 2. The nature of this interaction is illustrated in Figure 1 and shows a stronger association between SBHC presence and healthy sexual behavior among schools where at least 50% of students were receiving FRPL, compared to schools where less than 50% of students were receiving FRPL. Students’ age and receiving FRPL were inversely associated with healthy sexual behavior, while none of the other student demographic characteristics were associated with healthy sexual behavior. At the school level, a higher percentage of students receiving FRPL was also inversely associated with healthy sexual behavior.
Results of Multilevel Logistic Regression Analyses to Assess the Association Between SBHCs and Healthy Sexual Behaviora for the Total Sample of 11th Graders, Odds Ratio (95% Confidence Interval).
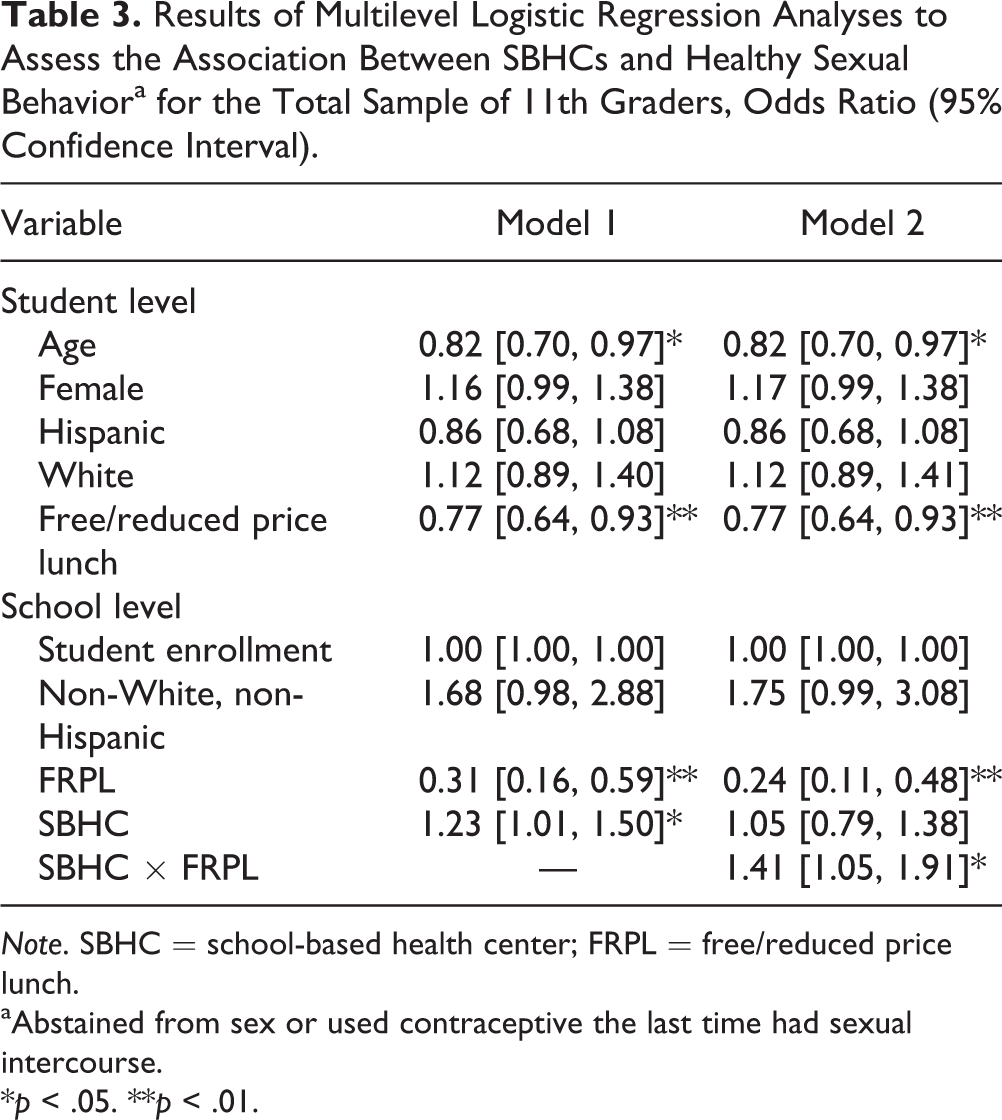
Note. SBHC = school-based health center; FRPL = free/reduced price lunch.
aAbstained from sex or used contraceptive the last time had sexual intercourse.
*p < .05. **p < .01.
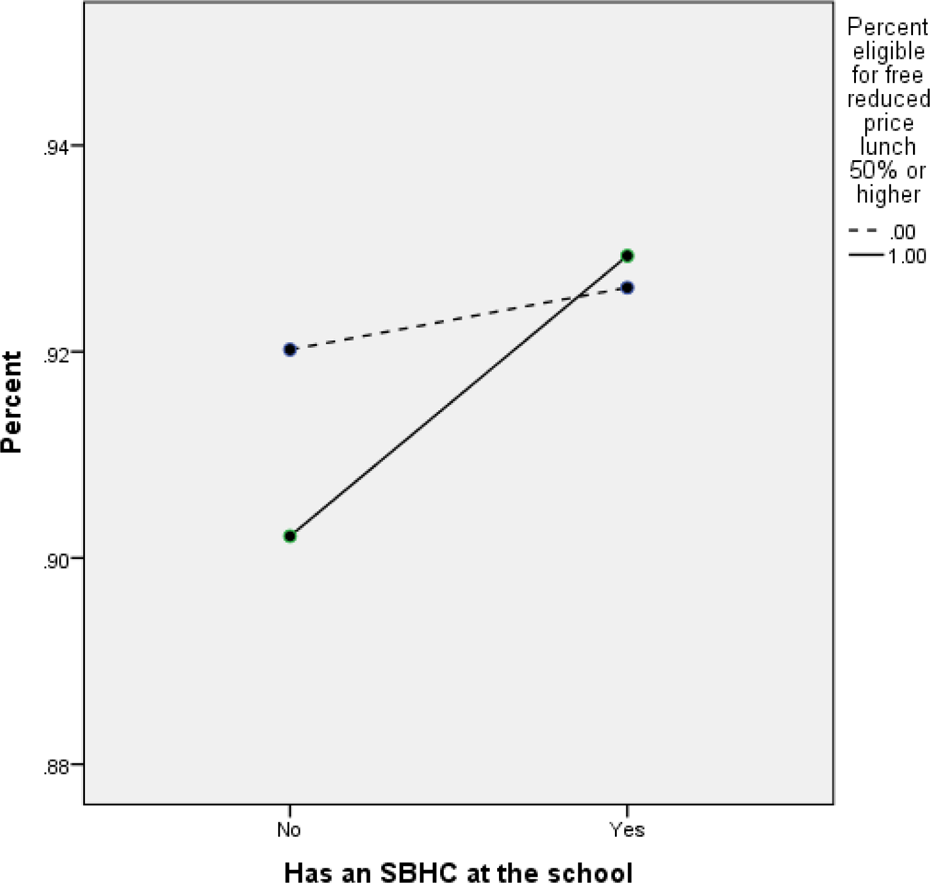
Percentage of students reporting healthy sexual behavior (abstinence or contraceptive use) by school SBHC status and percentage of students receiving free/reduced price lunch. SBHC = school-based health center.
Contraceptive Use
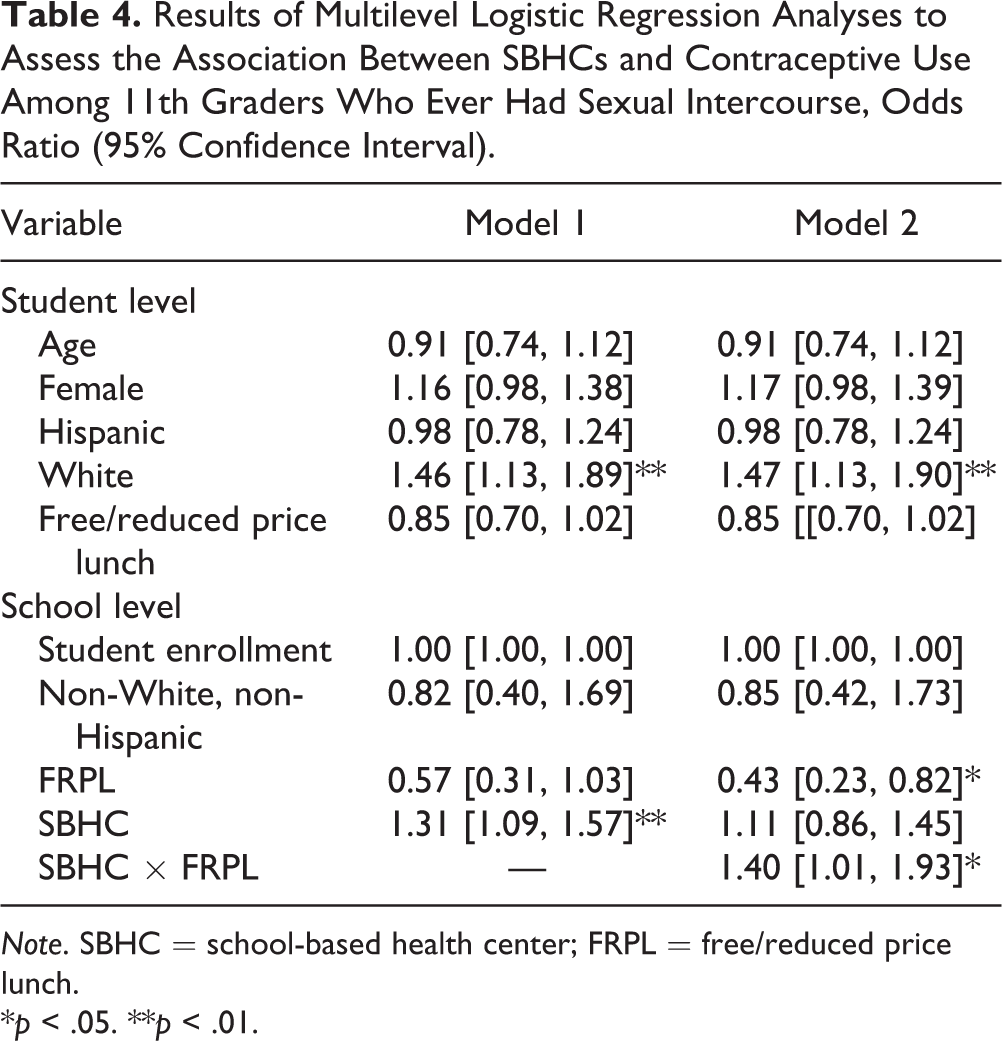
Results of multilevel logistic regression analyses in Table 4 indicate a positive association between SBHC presence and contraceptive use among students who ever had sex the last time they had sexual intercourse. Students at SBHC schools were 31% more likely to report contraceptive use than students at non-SBHC schools. SBHC × FRPL (school level) was again the only statistically significant interaction term, as shown in Model 2. The nature of this interaction is illustrated in Figure 2 and shows a stronger association between SBHC presence and contraceptive use among sexually active students at schools where at least 50% of students were receiving FRPL compared to schools where less than 50% of students were receiving FRPL. White students were more likely than non-Whites to report contraceptive use the last time they had sexual intercourse, while none of the other student demographic characteristics were associated with contraceptive use. The percentage of students receiving FRPL was inversely related to contraceptive use in Model 2.
Results of Multilevel Logistic Regression Analyses to Assess the Association Between SBHCs and Contraceptive Use Among 11th Graders Who Ever Had Sexual Intercourse, Odds Ratio (95% Confidence Interval).
Note. SBHC = school-based health center; FRPL = free/reduced price lunch.
*p < .05. **p < .01.
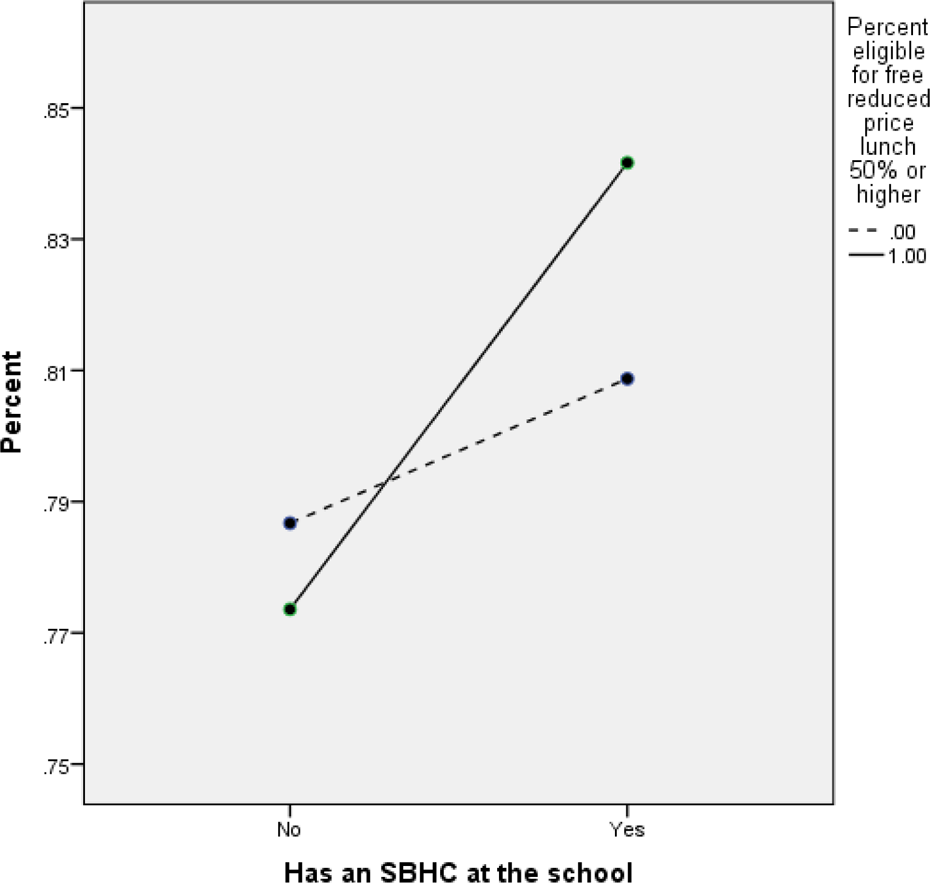
Among students who have ever had sex, percentage who used a contraceptive the last time they had sex by school SBHC status and percentage of students receiving free/reduced price lunch. SBHC = school-based health center.
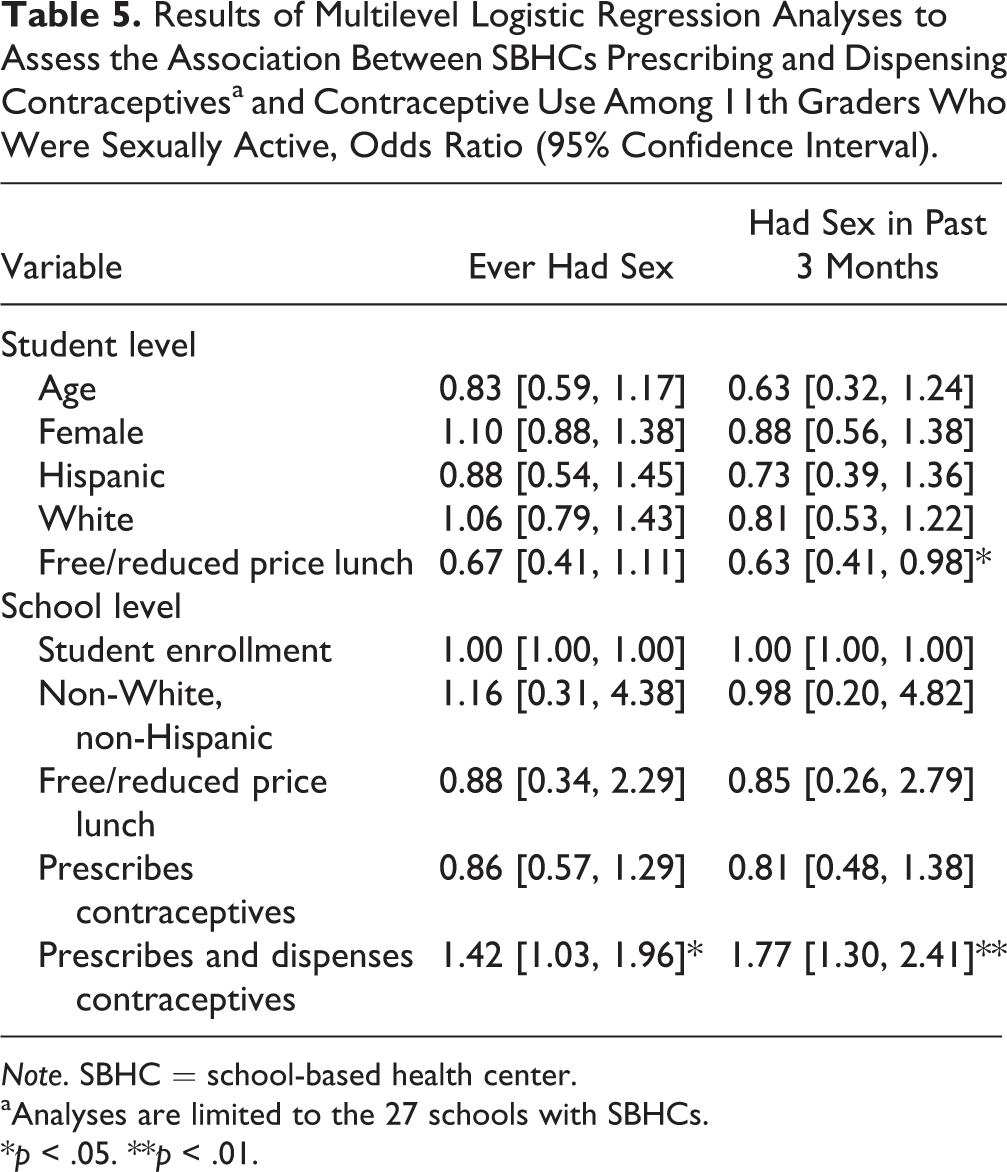
Additional multilevel analyses with the subgroup of 27 schools with an SBHC indicated significant positive associations between prescribing and dispensing contraceptives onsite and contraceptive use among 11th graders who ever had sex and among those who had sex within the past 3 months (Table 5). At SBHC schools that prescribed and dispensed contraceptives, students who ever had sex were 42% more likely to report contraceptive use the last time they had sexual intercourse than students at SBHC schools that did not prescribe and dispense contraceptives. Among students who had sex within the past 3 months, those attending SBHC schools that prescribed and dispensed contraceptives were 77% more likely to report contraceptive use the last time they had sexual intercourse than students at SBHC schools that did not prescribe and dispense contraceptives. Of the student demographic characteristics, receiving FRPL was inversely related to contraceptive use among students who had sex in the past 3 months. None of the other student demographic characteristics were associated with contraceptive use, nor were any of the other school characteristics.
Results of Multilevel Logistic Regression Analyses to Assess the Association Between SBHCs Prescribing and Dispensing Contraceptivesa and Contraceptive Use Among 11th Graders Who Were Sexually Active, Odds Ratio (95% Confidence Interval).
Note. SBHC = school-based health center.
aAnalyses are limited to the 27 schools with SBHCs.
*p < .05. **p < .01.
Discussion
This study investigated the association between SBHC presence in Oregon high schools and healthy sexual behavior among 11th graders and contraceptive use among 11th graders who were sexually active. This study also investigated possible moderating effects of school and student demographic characteristics. Findings suggest that SBHCs are associated with a greater likelihood of healthy sexual behavior among 11th graders and with a greater likelihood of contraceptive use among students who are sexually active. The associations between SBHC presence and healthy sexual behavior and contraceptive use appear to be stronger among schools with a larger percentage of students who are socioeconomically disadvantaged. This study also indicates a greater likelihood of contraceptive use among sexually active students at SBHC schools that prescribe and dispense contraceptives relative to other school with SBHCs that do not prescribe and dispense contraceptives.
These findings suggest that making contraception readily available on-site at SBHCs can support safe sex practices, particularly in economically disadvantaged communities where youth may be at elevated risk for unintended pregnancy and sexually transmitted infections. This may include working closely with school administration, school boards, and the community to support policies that include the provision of contraception at SBHCs. Although some SBHCs can prescribe contraception, if students must then go to a pharmacy or another health-care provider to obtain the prescribed method of birth control, the added burden on youth associated with inconvenience, cost, and transportation may reduce the likelihood of use. It also raises questions regarding SBHC service heterogeneity and the need to parse out whether and to what extent specific services and characteristics of SBHCs (e.g., types of health services, hours open, teacher–clinician relationships) may contribute to contraceptive use and other health-related outcomes.
Support also emerged for our hypothesis that SBHCs can have positive effects on students’ SRH behavior undifferentiated by subgroups as evidenced via significant main effects. SBHC presence was positively associated with healthy sexual behavior in the total sample. Among sexually active youth, SBHC presence was positively associated with contraception at last sexual intercourse. The latter may be a result of SBHC work: targeted outreach, education, and engagement of youth by SBHC staff. Additional research is necessary to better understand what specific strategies are employed that may result in this protective behavior.
Although males tend to become disconnected from health services in adolescence (Armitage et al., 2004), we did not find any support for the hypothesis regarding gender differences in SBHC effects. This finding is encouraging in that Oregon SBHCs may be just as beneficial for males as they are for females with respect to healthy sexual behavior and contraceptive use.
SBHCs also appear to be similarly associated with healthy sexual behavior and contraceptive use among students of different ethnic and racial groups, and students who were and were not receiving FRPL. The latter finding suggests that SBHCs can be beneficial for all students whose families are socioeconomically disadvantaged, even though the positive associations between SBHC presence and healthy sexual behavior and contraceptive use appear to be stronger for schools with a larger percentage of students who are disadvantaged.
Limitations
The current study is limited in several ways, including the cross-sectional nature of the data, which limits our ability to make causal inferences regarding SBHC effects. There is also the possibility of selection effects at the school and student level. Controlling for school-level characteristics and conducting analyses within the subgroup of SBHC schools helped to reduce this threat. There may also be important differences between SBHCs that dispense condoms only, for example, as opposed to a full range of contraceptive services. In particular, this difference may interact with student gender (given males increasing likelihood to obtain condoms vs. long-acting reversible contraceptives). However, we were not able to distinguish among contraceptive types offered by SBHCs. Sample attrition due to nonresponse may have biased our results in unknown ways, and the focus on 11th graders may limit the extent to which our findings generalize beyond the study sample. Additionally, the study sample is based in Oregon, with a relatively small minority population. Future studies are needed to examine whether similar results arise among high school students in other school grade levels and in states that are more ethnically diverse.
Implications
Nonetheless, these findings contain several important implications for SBHCs. The decision about whether or not to prescribe and/or dispense contraceptives in the SBHC, generally a decision made by the school board, is often fraught with controversy and tension for local communities. This study may be useful for SBHCs looking to gain permission to begin providing contraception on-site, particular in school communities with a large percentage of disadvantaged students. SBHCs considering using “prescribing” as a useful stepping stone to increasing access to contraception may also be motivated to wait until they can start dispensing, given the findings that prescribing alone does not appear to be associated with contraceptive use. Additionally, interest in planning new SBHCs in school communities with higher percentages of disadvantaged students may increase, particularly in those where teenage pregnancy rates are a concern, given the data showing increased healthy sexual behaviors among disadvantaged students with access to SBHCs.
A number of additional questions are generated by these findings, leading to some natural next steps for analysis. First, it would be very useful to look specifically at differences between students who utilize the SBHC versus those who simply have access but don’t utilize SBHC services. It would also be useful to replicate this study in other states to see if the observed relationships between SBHCs and student contraceptive use occur in other populations. Lastly, longitudinal studies are needed to provide more definitive evidence regarding hypothesized effects of SBHCs on sexual behavior among adolescents.
Findings of this study support the role of school nurses as partners with SBHCs and community health-care providers. School nurses can work collaboratively with SBHCs to coordinate reproductive and sexual reproductive health and educational services as well as follow-up care for students. At schools without SBHCs, school nurses are also in a position to assist students with reproductive health services through education, counseling, and referrals to primary care or family planning clinics in the community. The current study suggests that health-care visits with high school students that incorporate a discussion on SRH services and resources may serve to increase pregnancy prevention behavior in youth.
Footnotes
Authors’ Note
The contents of this article are solely the responsibility of the authors and do not necessarily represent official views of National Institute of Child Health and Human Development or NIH.
Acknowledgments
The authors wish to thank Xiaoyu Song, PhD, for her technical advice on statistical analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Grant Number 1R01HD073386-01A1 from the National Institute of Child Health and Human Development.