
Abstract
Hand hygiene for children is crucial to keep them healthy. The purpose of the study was to evaluate the effects of two educational initiatives on “handwashing effectiveness (HWE).” A randomized controlled trial was carried out during April/June 2016, and 96 primary school students were randomly assigned to Group I receiving education with fluorescent gel; Group II receiving interactive education or control group continuing its normal education. Evaluation was made by scoring the fluorescent areas on the hands with photographs. There were significant differences in handwashing scores between preprogram and postprogram for all areas in only Group II (p < .05). HWE increased from 17.9% to 18.4% in Group I, from 15.4% to 37.7% in Group II, and from 35.5% to 35.8% in control group. Only concretization with fluorescent gel is not a sufficiently strong motivator for increasing HWE. New techniques should be integrated into the training programs for children.
Keywords
Background
Emerging and reemerging infectious diseases continue to maintain their importance despite the significant changes and advancements that took place in the world during the last three decades (World Health Organization [WHO], 2015). Childhood respiratory diseases and gastrointestinal system infections are still among significant morbidity and mortality burden (Aunger et al., 2016; Ejemot-Nwadiaro, Ehiri, Arikpo, Meremikwu, & Critchley, 2015). High infection rates during childhood indicate a relationship with schools. The school environments are places where children spend an important amount of their daily lives that are suited for direct and indirect infections. Contagious diseases may spread rapidly in school environments—as was the case during the 2009 pandemic H1N1 contamination (Freeman et al., 2014; WHO, 2015).
Hygiene education and handwashing are among the simplest and most cost-effective applications for reducing such contagious diseases significantly (Fewtrell & Kay, 2015). It has been put forth that improving hand hygiene during childhood decreases diarrhea-related diseases by 40% (Ejemot-Nwadiaro et al., 2015), respiratory system diseases by 23% (Aunger et al., 2016), and infection-related school absences by 26% (Chittleborough, Nicholson, Basker, Bell, & Campbell, 2013; Lee, Leung, Tong, Chen, & Lee, 2015; Nandrup-Bus, 2009; Willmott et al., 2016). Proper hand hygiene practices prevent the spreading of secondary infections in the society while also decreasing the health expenses and the burden on the family due to impact on the leave of absence periods as a result of childcare (Chittleborough et al., 2013).
WHO published a hand hygiene directive comprised of nine parts that lasts 40–60 s for an effective decontamination of all hand surfaces and a consensus has been reached in this matter (WHO, 2009). Apart from this, there is no specific instruction prepared for children. When studies on hand hygiene among children are examined, it is observed that handwashing effectiveness (HWE) has been studied less frequently. Despite the individual and social benefits it provides, handwashing is a frequently neglected public health issue (Snow, White, & Kim, 2008; Song, Kim, & Park, 2013).
The purpose of the study was to evaluate the effects of two educational interventions on increasing HWE. It is expected that the study will be a guide for school nurses and teachers to teach a proper handwashing technique to the children.
Method
Design and Setting
The study was carried out as a controlled triple-blind study during the dates of April 1–Jun 7, 2016, at a primary school in the rural region of Turkey with a low socioeconomic level. Approval was obtained from the Mersin University Clinical Research Ethical Committee (78017789/050.01.04/E.65341). The target population of the study was comprised of 552 students at this school. Children display similar development characteristics—even though they have different learning speeds and learning methods individually—at certain age intervals. The childhood period can be divided into two main periods based on development and learning as 4–7 and 8–11 age-groups (Postma, Getkate, & van Wijk, 2004). Children of 4–7 can concentrate on single elements of an object at a time because of short attention span. They have a limited knowledge of other people and their experiences. Children of 8–11 can concentrate for a longer period of time and clean themselves in the correct way. They are able to see things from their point of view. The children at this stage could assist the younger children on how to perform hand hygiene technique (Postma et al., 2004). Therefore, the second, third, and fourth grades that mostly contain the target age-group were chosen for this study. Intervention procedure and details were explained. Informed written consent was taken from all students and their parents at the beginning of the study. School administration and teachers were informed prior to the study. Students who were not allowed by their parents to participate in the study, students who did not wish to take part in the study, and students with dermatologic problems in their hands (eczema, dermatitis, scar, etc.) were not included.
The sample size for the study was found to be 30 individuals in each group (Group I, Group II, and control group) and 90 individuals in total for the effect size of .635 for main hypothesis with .80 power and .05 Type I error (G*Power Version 3.1.9.2 statistical software). The study sample group was comprised of 180 students in total with 60 in each group according to the assumption that there would be losses in the sample groups. The power of the study was found to be .90 based on the mean of “right- and left-hand’s dorsal and palmar surfaces total points” at a confidence interval of .05 by the SPSS program (Version 21, New York, USA).
Randomization occurred by grade level when forming the Group I, Group II, and control group for minimizing the interaction between the students. Three different envelopes were prepared for the second, third, and fourth grades, and the class names in each grade were written down and placed in the envelopes. Three classes were picked up randomly from each envelope. A total of 28 students who did not meet the study criteria along with 56 students who could not receive parental approval were excluded from the study. The classes of the remaining 96 students were appointed to their groups by way of drawing lots. The students and parents were not informed of their groups. They were informed that the effects of different handwashing education strategies would be evaluated. Two students in the control group left the study since they changed their schools and the study was completed with a total of 94 children (Figure 1).
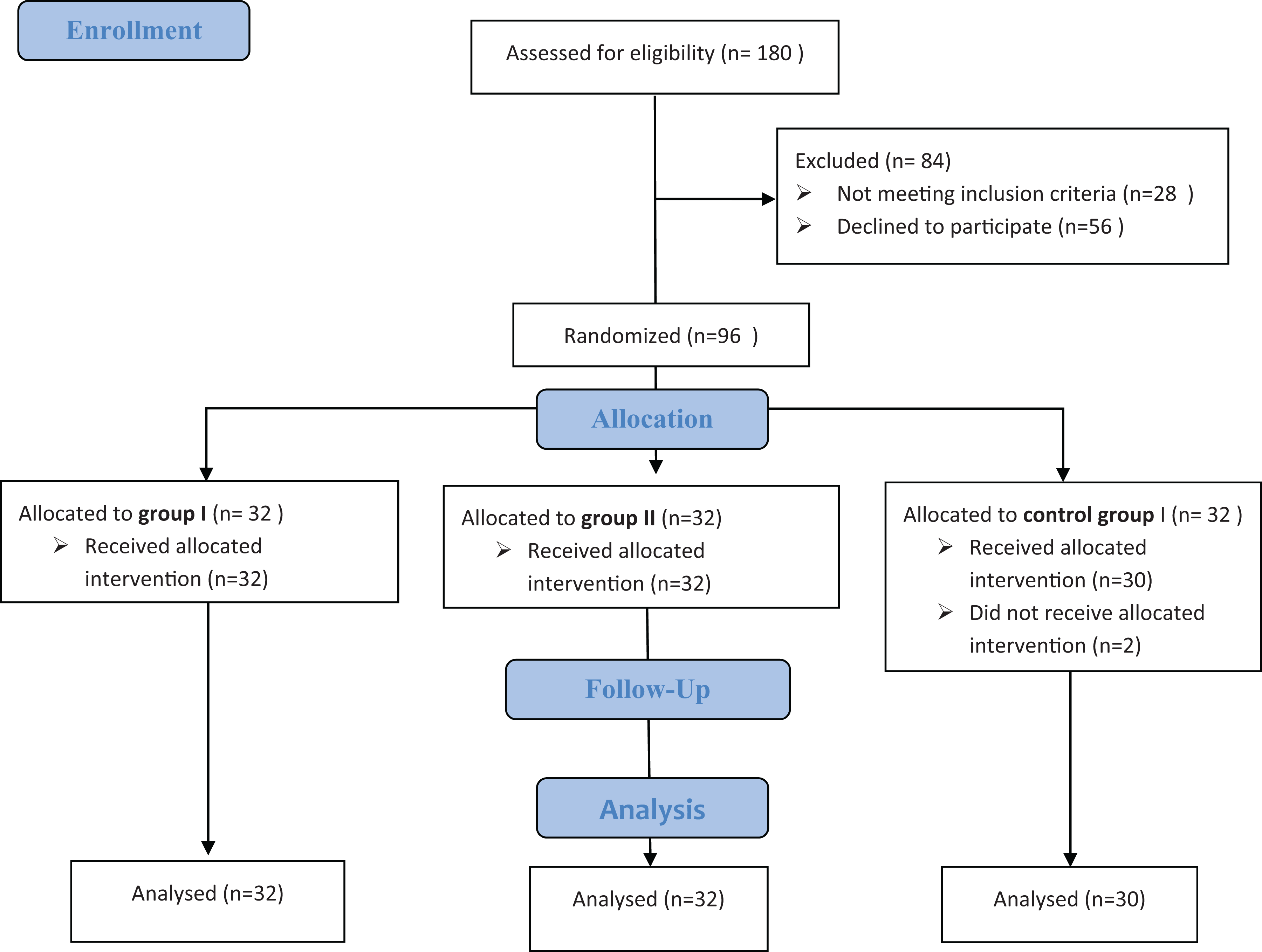
Flow diagram of the study population.
Measurements
The study data were acquired by way of the questionnaire and visual evaluation of handwashing. The questionnaires were prepared by the researchers according to literature (Aslan et al., 2006; Ayhan et al., 2015; Cevizci et al., 2015; Ray, Dobe, Lahiri, & Basu, 2009). This form included 20 questions on the sociodemographic characteristic of the students, their handwashing behaviors, and general hygiene habits. It was completed by the students in classroom environment in 15 min, and the researchers helped those who could not fill out the questionnaire.
Fluorescent containing gel, ultraviolet (UV) lamp, and black box were used for evaluating HWE. The gel that can be seen under UV lamp due to the fluorescent substance was prepared by adding one drop of phosphoric substance to 75 ml hydroalcoholic solution as described in the gel prospectus. Even though the gel amount to be used on adults has been specified as 1.75 ml (Macdonald, McKillop, Trotter, & Gray, 2006), the gel amount was adjusted so that it would cover the hands as a cream due to the variance in the hand sizes of children (on average 1 ml; Lee et al., 2015). UV lamp was used to observe the fluorescent substance remains on the hands. A black box with dimensions of 50 × 40 cm which does not allow light to penetrate inside while enabling the hands to be placed in it for taking pictures was used for better photographs of the fluorescent gel and for decreasing UV exposure, and the curtains in the environment were drawn.
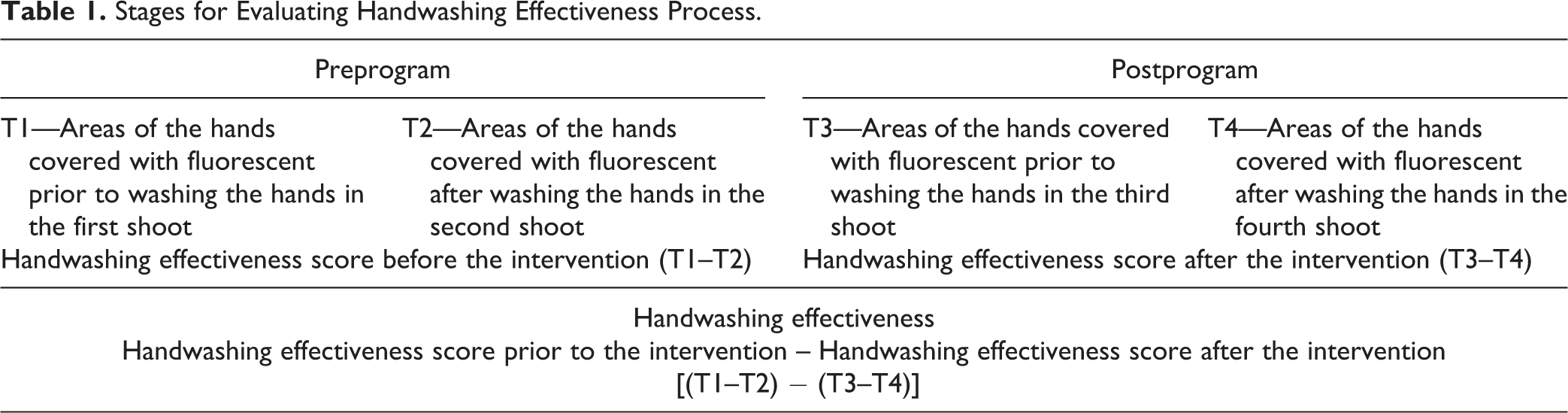
The application stage of the study was carried out in the school laboratory. Soap and paper towels were placed near the sinks prior to the study. The students were taken into the laboratory in groups of five. Each student was given a code number, and the same number was used when taking the photographs. Photographs were taken at four different times for evaluating the HWE (Table 1).
Stages for Evaluating Handwashing Effectiveness Process.
Handwashing procedure applied on the control group
The application consisted of two stages. In the first stage, gels were given to the children and they were asked to apply the gel to all the surfaces of their hands after which the gel was left to dry for 15–20 s. Dorsal and palmar views of the right and left hands were photographed under UV lamp twice in order to determine the level at which the applied gel has covered the hands (T1). The children were then asked to wash their hands. A second photo shoot was made to determine the fluorescent substance remaining on the hands (T2). Third (T3) and fourth (T4) shoots were made as before handwashing (before HW) and after handwashing (after HW) in the second stage about 1 month after the first application (Table 1).
Handwashing procedure applied on Group I
The first stage for the Group I resembled that of the control group. During the second photo shoot, the spots on the hands of the children where fluorescent substance remains can be observed were shown to the children; they were told that these are spots where microbes still remain after which they were informed that they can also get rid of these microbes if they wash their hands properly. The third and fourth photo shoots were carried out in accordance with the control group procedure 1 month after the first application.
Handwashing procedure applied on Group II
All stages took place as they did for Group I. Group II received hand hygiene training, however, between the first and second stages by way of a 30-min PowerPoint slideshow on the definition of a microbe, types of microbes, diseases caused by microbes, and the importance of handwashing in preventing diseases. Afterward, the nine-stage handwashing activity put forth by the WHO (2009) was demonstrated. Each student washed their hands in accordance with the demonstrated technique under the observation of the researchers. The third and fourth shoots were carried out 1 month after the first.
At the end of the study, 30-min hand hygiene training was given to all students in the school, and posters depicting the importance of handwashing were hung on classroom bulletin boards. Teachers received information on the results of the study and the method they can use for teaching the students how to wash their hands.
The practice of handwashing was evaluated with the surface area covered by fluorescent material. The UV photographs of students’ hands were converted to JPEG format for analysis. Measurements taken for each image were made according to blue areas and densities (Figure 2). The photographs taken were examined by three researchers who did not participate in the design of the study in order to prevent bias in evaluations. Percentages were calculated for the area of each hand. In addition, the statistics of the study were done by a statistician who did not participate in the work (triple-blind).
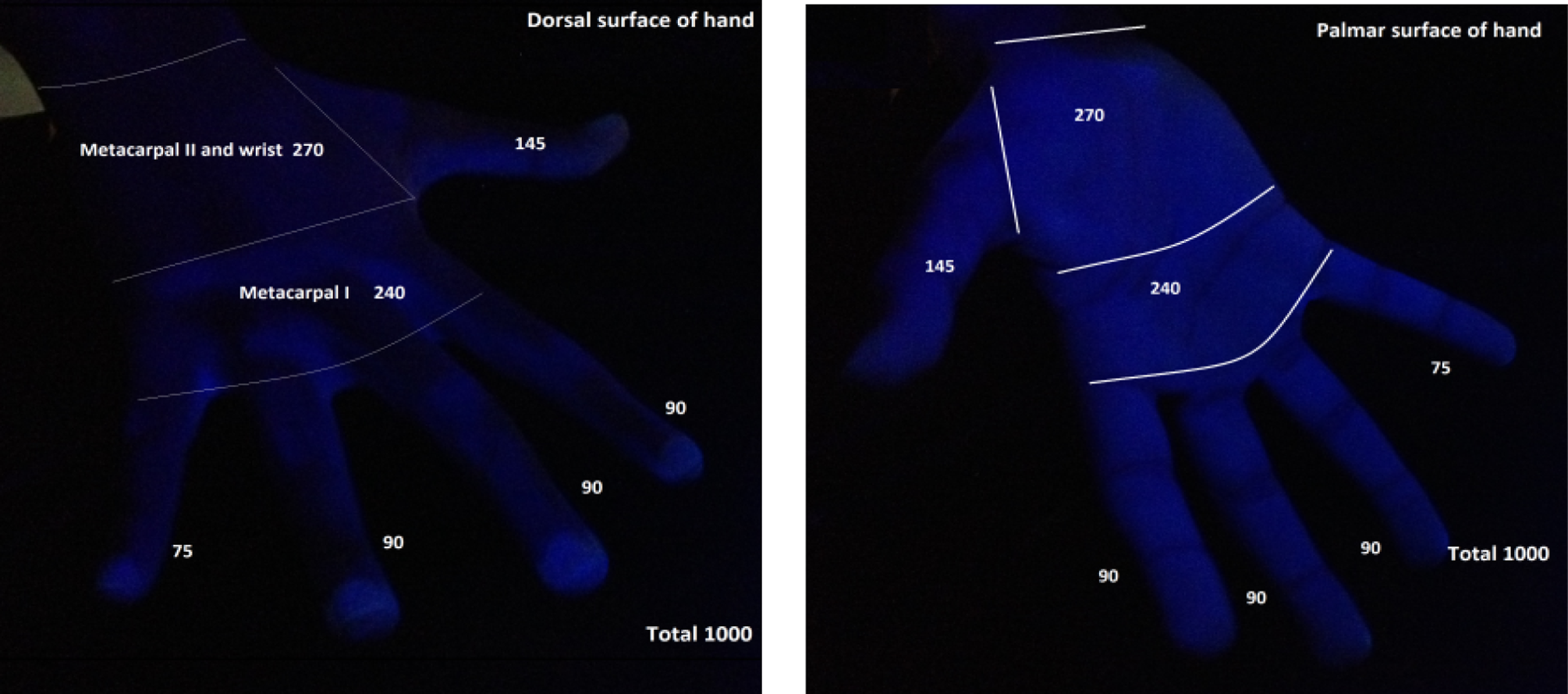
Evaluation of hand points system images.
The hand surface was calculated as follows: Regions where distal phalanges, intermediate phalanges, proximal phalanges, metacarpal, and carpal bones are located were measured using a tape measure for determining the palmar and dorsal surface areas of the right and left hands. Areas of each hand were calculated in cm2 which were then transformed into percentages. Accordingly, dorsal/palmar area and their percentages were determined, 14.5% for the thumbs, 34.5% for the other fingers, 24.0% for the metacarpal area near the fingers, and 27.0% for the metacarpal area away from the fingers and the carpal area for a total of 100%. The display of 100’s was changed into 1,000 to simplify the task of the researchers while evaluating the photographs in the computer environment. The right hand was evaluated over a score of2,000, left hand of 2,000, palmar surfaces of 2,000, and dorsal surfaces of 2,000; both hands were evaluated over a score of 4,000 (Figure 2). The increase in the differences between the fluorescent areas before and after handwashing points to preprogram and postprogram was evaluated as the “increase in HWE.” (Table 1)
Statistical Analysis
The data were analyzed using SPSS statistical package program (Version 21, New York, USA). Analysis of categorical variables was performed with χ2 test, descriptive characteristics expressed in frequency and percentage. One-way analysis of variance was used in the comparison of the multiple group averages for continuous variables. Repeated general linear models (GLMs) were used to evaluate the changes within group and between groups. Post hoc Tukey’s test was used to assess the significance of differences between pairs of groups. p ≤ .05 was accepted as statistically significant.
Results
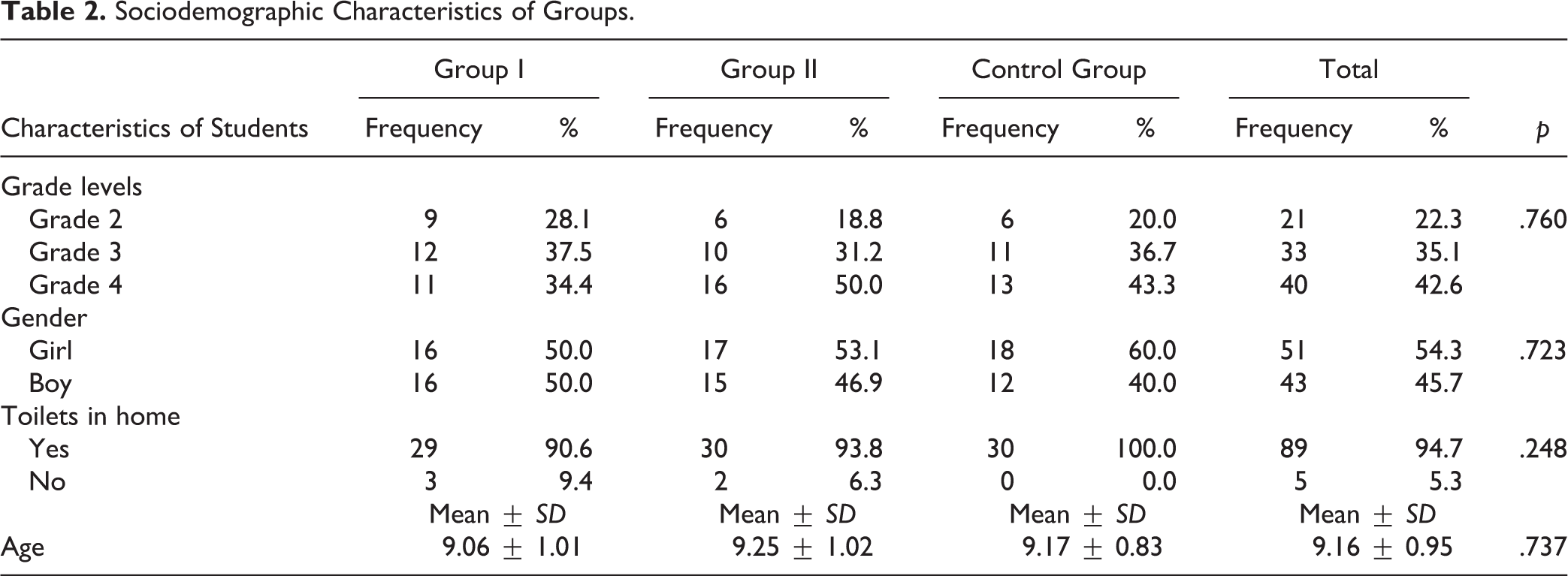
All students excluding two in control group completed the study (Figure 1). Age average of Group I was 9.06 ± 1.01 (8–12) years, Group II was 9.25 ± 1.02 (7–12), and that of control group was 9.17 ± 0.83 (08–11; p > .05; Table 2). Of the students, 54.3% (51 students) were girls and 45.7% (43 students) were boys. There were no differences among the groups with regard to age, class, and gender (Table 2). It was determined that 5.3% of the students do not have a toilet in their homes, 14.9% do not have toilet paper in their toilets, and 13.8% do not brush their teeth and clean their teeth only with water and that the parents of one of every five students do not have a regular teeth-brushing habit. It was determined that 4.3% of the students do not clean their perineum after urination and 2.2% after excretion, whereas it was also determined that only half of the students use toilet paper after urination/excretion and that the remainder clean themselves only using water.
Sociodemographic Characteristics of Groups.
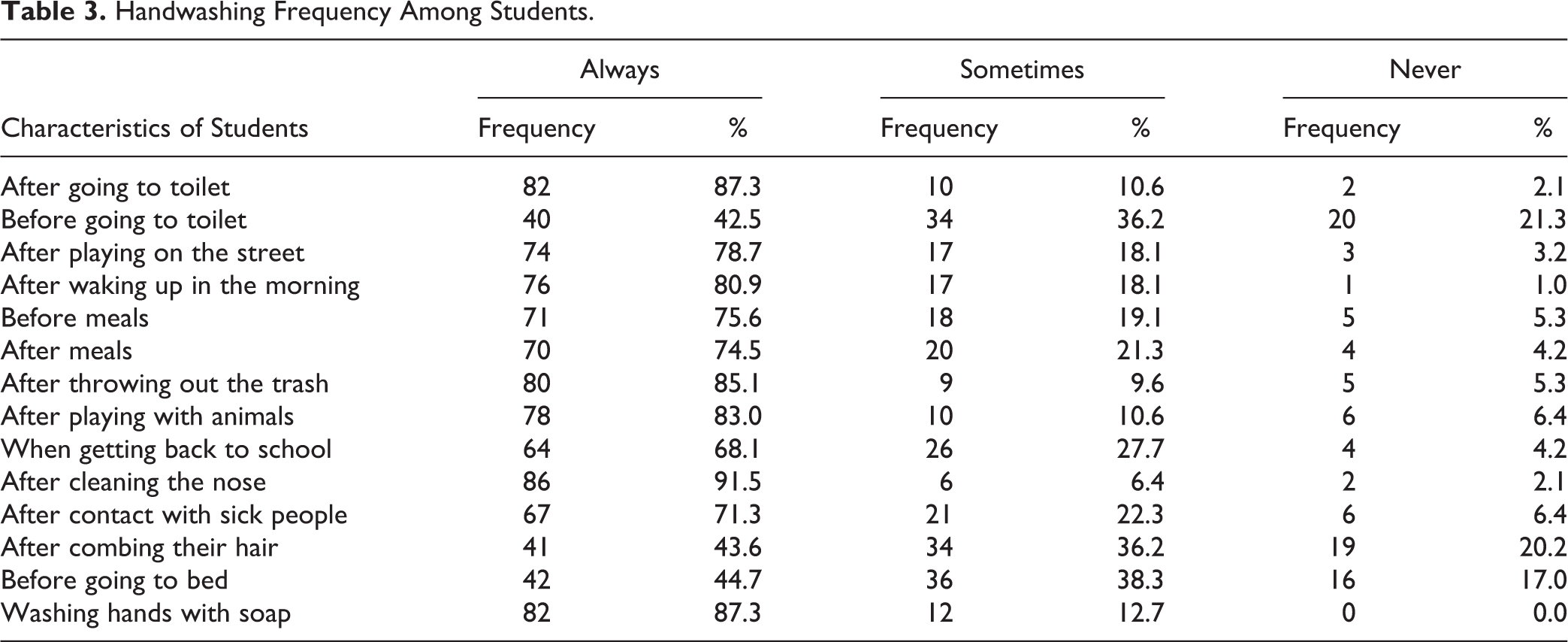
Following the evaluations of handwashing habits, children reported that they always wash their hands after toilet (87.3%), after throwing out the trash (85.1%), after playing with animals (83.0%), and after waking up in the morning (80.9%). The majority of the children presented that they do not wash their hands before going to the toilet (21.3%), after combing their hair (20.2%), before going to bed (17.0%), after contact with sick people (6.4%), and before meals (5.3%; Table 3).
Handwashing Frequency Among Students.
After the handwashing, the total fluorescent-covered areas on the dorsal and palmar surfaces of both hands decreased from 90.4% to 82.1% in Group I, 90.9% to 84.6% in Group II, and 82.7% to 64.5% in the control group before the intervention. After the intervention, it decreased from 91.0% to 81.6 in Group I, 79.5% to 62.3% in Group II, and 85.9% to 64.2% in the control group. Group II had higher HWE scores despite the slight increase in other groups (Figure 3).
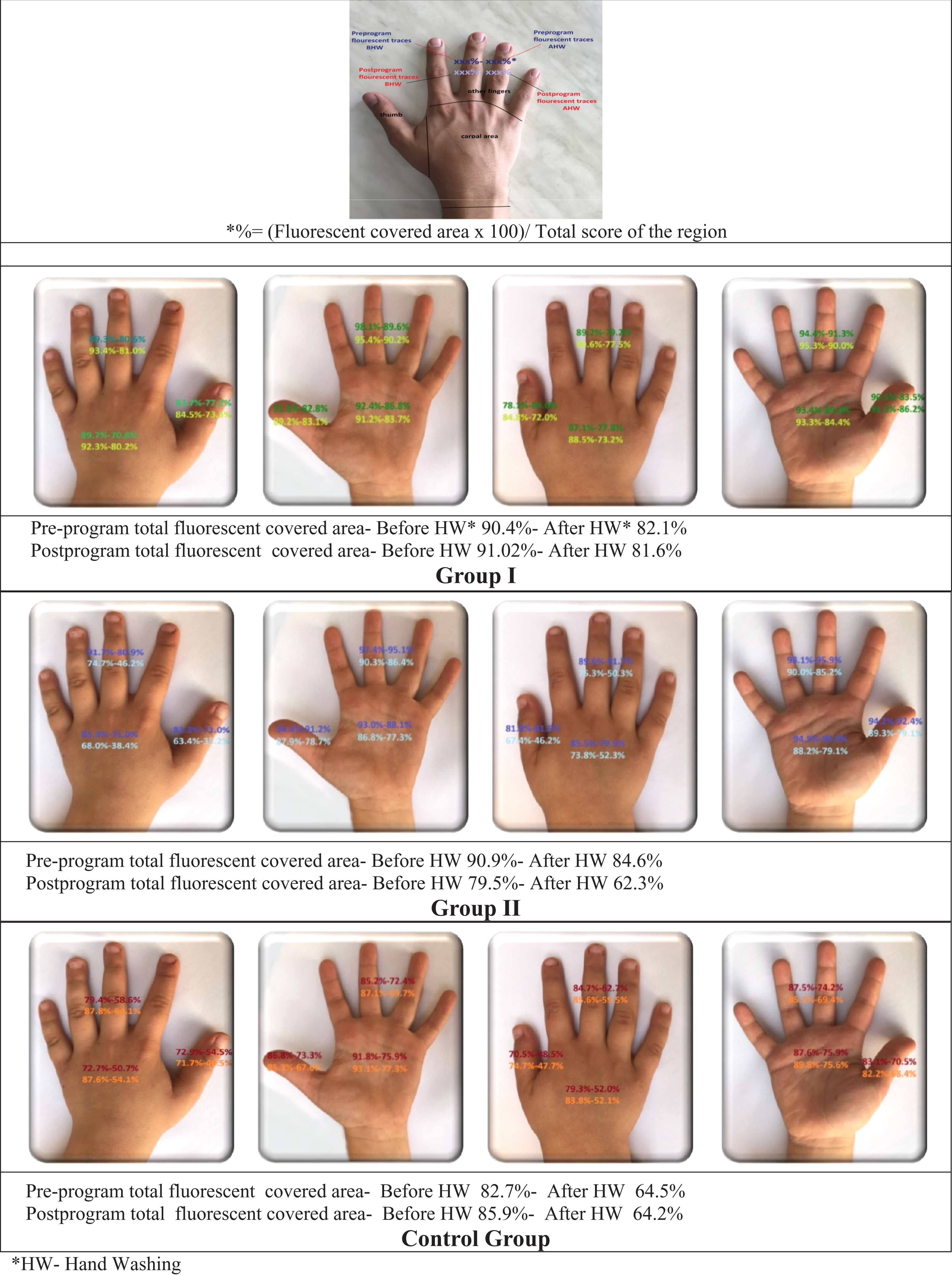
The percentage of distribution of fluorescent traces on hands surfaces before and after handwashing.
It was determined that the postprogram HWE scores of Group II increased at a statistically significant level in all regions of both hands in comparison with the preprogram scores (p < .05). The values did not change within the control group (p > .05; Table 4). In Group I, the HWE scores for the right-hand dorsal and palmar surface, right- and left-hands metacarpal and carpal palmar surface, and other fingers of the right and left hands dorsal and palmar surfaces increased in comparison with the preprogram scores (p < .05). No change was determined between the HWE scores of right- and left-hands dorsal and palmar surface, left-hand dorsal and palmar surface, right- and left-hands’ dorsal surfaces, right- and left-hands’ palmar surfaces, right- and left-hands metacarpal and carpal dorsal surface, and thumb of the right- and left-hands dorsal and palmar surface in comparison with the preprogram scores in Group I (Table 4).
The Point Distribution of Fluorescent-Labeled Hand-Rub on Hands Before and After Handwashing.
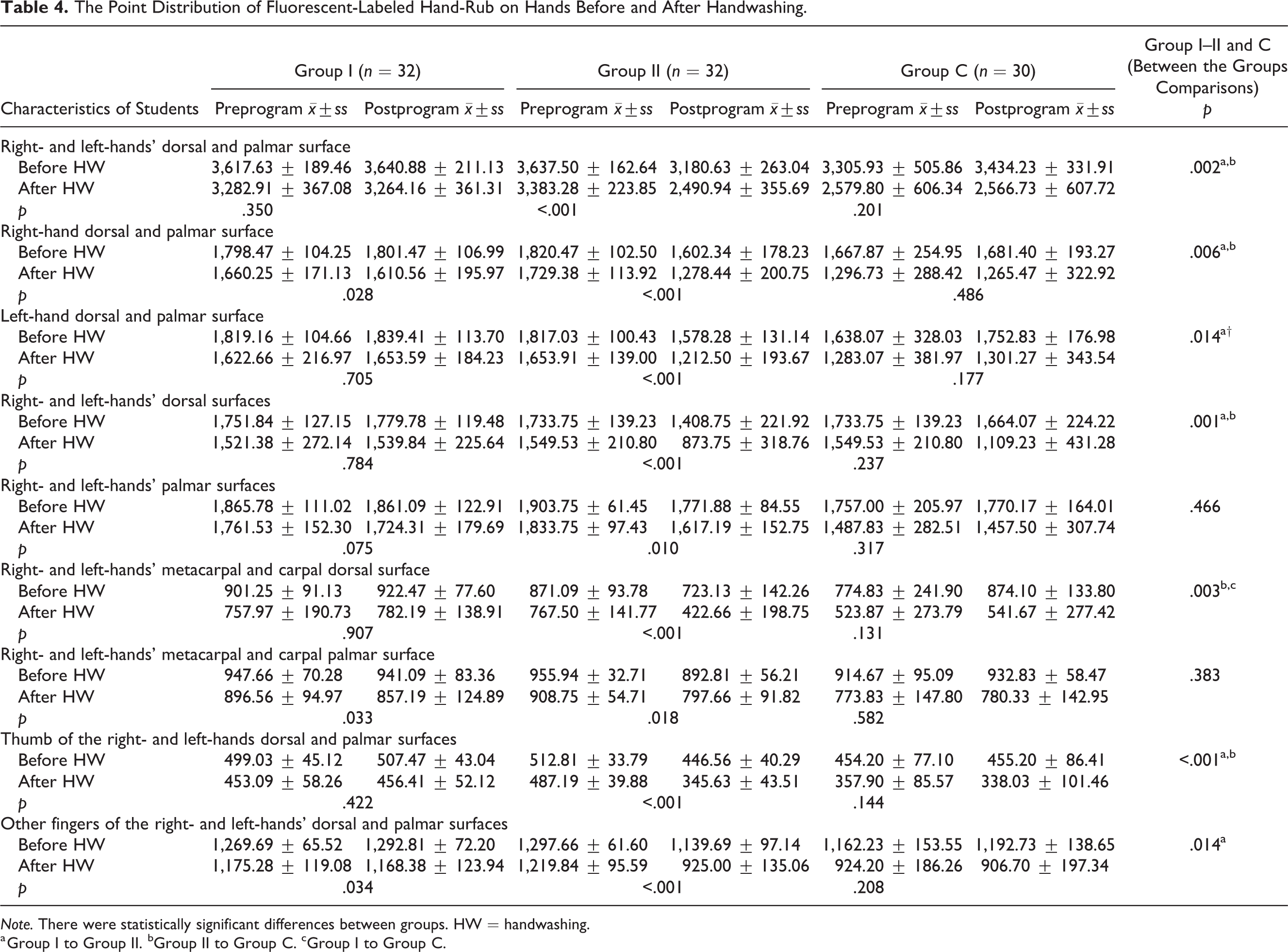
Note. There were statistically significant differences between groups. HW = handwashing.
a Group I to Group II. bGroup II to Group C. cGroup I to Group C.
A statistically significant difference was determined between the changes in the HWE scores of the groups with regard to right and left hands dorsal and palmar surface, right-hand dorsal and palmar surface, left-hand dorsal and palmar surface, right- and left-hands’ dorsal surfaces, right- and left-hands metacarpal and carpal dorsal surface, thumb of the right- and left-hands dorsal and palmar surfaces, and other fingers of the right- and left-hands dorsal and palmar surfaces (p < .05). On the other hand, no statistically significant difference was determined between the groups with regard to the HWE scores for right and left hands’ palmar surfaces and right and left hands metacarpal and carpal palmar surface (p > .05). Table 4 indicates the group that causes the differences observed during intergroup comparisons.
Discussion
HWE is very low despite the fact that effective handwashing is the cheapest, simplest, and easiest application for controlling infections among the society. Similar to those of relevant studies in the literature, this study’s results demonstrated that HWE may be increased in school children by way of education (Ghanim et al., 2016; Shrestha & Angolkar, 2015).
The evaluation of the hand hygiene habits of participating children indicated that they wash their hands more in cases with higher risks of contamination such as after waking up in the morning, throwing out the trash, and before the meals. Participants’ handwashing is still at low rates in critical times such as before and after the toileting (Ghanim et al., 2016; Lopez-Quintero, Freeman, & Neumark, 2009). In Turkish culture, the perineum is cleaned by hand with water after urination and defecation. Thus, this indicates that children are more prone to infection in areas with high probability of fecal oral contagion.
The number of students who pointed out that they always wash their hands after the toilet, after playing in the street, after waking up in the morning, before and after meals was higher in another study carried out in Turkey in comparison with those in our study (Kitiş & Bilgili, 2011). Low hand hygiene effectiveness with hand hygiene of the children may be related with the fact that the study was carried out at a region with low socioeconomic level (Freeman et al., 2014). It is known that low socioeconomic level has an adverse impact on handwashing habit. Indeed, there were some students in the study who do not have a toilet in their homes, who do not have toilet paper for use in perineum cleaning, and who do not have any personal hygiene products. Educational applications on hand hygiene are very important for preventing epidemics, which can affect the school population and which can spread in this risky population (Willmott et al., 2016).
HWE was low according to the study results despite the high ratio of students indicating that they wash their hands during daily activities. Whereas studies generally set forth that handwashing frequencies of people according to self-report are generally higher while also indicating that their adaptations to handwashing are low (Borchgrevink, Cha, & Kim, 2013; Ray et al., 2009; Snow et al., 2008).
The majority of the health issues related with school children may be prevented by way of hygienic applications passed onto the children through education. It is also important how the education activities are carried out. Kitiş and Bilgili (2011) reported that the use of visual–aural tools is important for teaching proper handwashing technique to students in the primary school since they are in the concrete learning period. It was indicated by the researchers at the beginning of the study that strong visual learner students may develop effective handwashing techniques when visually stimulated (Morton & Schultz, 2004). There are examples in literature that support this opinion (Fishbein, Tellez, Lin, Sullıvan, & Groll, 2011; Snow et al., 2008). In the study by Fishbein, Tellez, Lin, Sullıvan, and Groll (2011) on 60 pediatric patients in the 8–18 age-group at the emergency pediatric polyclinic waiting room, the locations of the remainder microbes were shown to the patient group by way of a fluorescent gel. An additional training was given to the other group after which it was expressed at the end of the study that indicating the locations of remainder microbes by way of a fluorescent gel to the children will increase the handwashing skills of the children without any need for special hand hygiene training. The results of our study are different from those of the study by Fishbein et al. (2011). This difference was thought to be due to the differences in the age-groups of the children in addition to the differences in evaluation criteria as well as the fact that the children were sick, thus resulting in a high level of interest on their part. The results of our study were in accordance with those put forth by Randle et al. (2013) indicating that educational approaches integrated with interactive applications may increase the HWE.
In a study that evaluates HWE using the control lists prepared in accordance with the handwashing steps suggested by the WHO, parts that were most frequently overlooked prior to the training were expressed respectively, as wrists, fingertips, and thumb, whereas the overlooked parts were indicated as wrists and fingertips after the intervention (Kitiş & Bilgili, 2011). Another study carried out using a similar technique reported that the most frequently overlooked parts were between the fingers prior to the intervention and wrists following the intervention (Aslan et al., 2006). Cevizci et al. (2015) carried out a study and listed these areas as thumbs (proper washing ratio 15.5%) and palm (25.5%) prior to the intervention and palms (55.3%) along with thumbs (59.2%) after the intervention. Different from other studies, it was observed in our study that the best cleaned parts of the hands were thumbs both before and after the intervention, whereas the least cleaned parts were the remaining fingers and palms. It was understood that the stages of rubbing the palms, cleaning the fingers by interlocking the fingers, and cleaning the fingertips by placing them inside the palm are not carried out effectively. This result may be due to the fact that while the thumb movement is easier to be understood by the children, movements of the other fingers are more difficult and take a longer period of time. It can be stated that developing simpler techniques for washing the hands faster in addition to evaluating the psychomotor skills of children may increase the hand hygiene compliance of children when teaching these movements. While a lower washing effectiveness was expected for the right hand, which is more active in washing hands, it was observed that there is no difference between the right and left hands. Conversely, similar to the study by Škodová et al. (2015), palmar surfaces remained dirtier in comparison with the dorsal surfaces. Avşar, Kaşikçi and Yağci (2015) carried out a study in which it was observed that the students do not use the proper technique when washing the palms. However, the pathogens remaining on the hands of the children may act as reservoirs when the HWE is not sufficient (Randle et al., 2013). All areas of the hands should be washed properly for attaining full decontamination (WHO, 2009).
Limitations of Study
While the data from our research are informative, it should be noted that observations only took place in one school’s low socioeconomic environment. For this reason, care should be taken in generalizing the findings. Some children could share information between classrooms even though randomization was made not according to the students but according to grade level in order to minimize the interaction between the students.
Even though “observation” is accepted as the golden standard when evaluating HWE, it is indicated to be a costly and time-consuming method (Haas & Larson, 2007). Conversely, evaluations were carried out in this study only on the areas covered with fluorescent gel, and it was assumed that the fluorescent-covered parts on the hands after washing will potentially indicate remaining pathogens. Microbiological validity was not used in the study. It is aimed with an effective washing of the hands to remove the microbial flora without any impact on the permanent skin flora. The microorganisms determined on the permanent flora during microbiological analyses may affect the results (Ayhan et al., 2015; Szilágyi et al., 2013). Hence, the methodology used in this study was a simpler and less costly form of evaluation in comparison with the observation method and culture technique used by Szilágyi et al.
Despite the fact that the requirement of experienced observers in addition to the lack of three-dimensional evaluations for the photographs has brought about various limitations, handwashing activity with fluorescent gel added demonstration is a cheap method that can easily be understood by the children.
Implication for School Nurses
Although sanitation infrastructure varies from country to country (i.e., running water and toilets in the homes), handwashing practices may be similar across all populations/countries. The improving handwashing practices among children is not only important for themselves but also for their families and society. Trained children can show the siblings and their families on how to perform hand hygiene technique.
Handwashing practices could be improved with interactive training program by the school nurses and teachers. Using fluorescent gel with interactive education may improve hand hygiene effectiveness for children. Faster and simpler techniques for handwashing taking into account the frequently omitted areas of the hands should be developed in future studies.
Footnotes
Author Contribution
Study conception and design: Emine Öncü, Sümbüle Köksoy Vayısoğlu; Acquisition of data: Esra Peker, Dilek Yurtsever; Analysis and interpretation of data: Diğdem Lafcı, Ebru Ravlı Bulut; Drafting of manuscript: Emine Öncü, Sümbüle Köksoy Vayısoğlu, Diğdem Lafcı, Dilek Yurtsever, Ebru Ravlı Bulut, Esra Peker; Critical revision: Emine Öncü, Sümbüle Köksoy Vayısoğlu, Diğdem Lafcı, Dilek Yurtsever,Ebru Ravlı Bulut, Esra Peker.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.