
Abstract
Parents’ recognition of adolescents’ emotional distress is a significant determinant of early detection and treatment of mental disorders. However, there is dearth of research exploring parent–adolescent agreement regarding adolescents’ emotional distress. This cross-sectional, school-based study compared parents’ proxy reports and self-reports of adolescent’s emotional distress among 289 parent–adolescent dyads in Korea. Findings revealed low agreement between adolescents’ and parents’ reports of depression, anxiety, and anger, with an average polychoric r of .25 to .27. The agreement was particularly low for high school students, boys, and father–adolescent dyads. Additionally, parents tended to underestimate adolescents’ emotional distress symptoms; a significant percentage of adolescents experiencing symptoms were rated in the normal range by parents, particularly high school students experiencing anger. Interventions are needed to help adolescents learn to manage and express their negative emotions. Moreover, parent education programs that improve parents’ recognition of emotional distress and appropriate help-seeking behaviors are needed.
Adolescents are vulnerable to mental health problems as they experience a wide range of emotions associated with substantial changes in their behavior, cognitive abilities, and identity in the course of their development (Carr, 2015). Serious and persistent emotional distress affects adolescents’ academic achievement, interpersonal relationships, physical health, and psychosocial development, and may progress to various mental disorders and even suicidal behaviors (Carr, 2015; Lee, Jung, Park, & Hong, 2018). In a national study in Korea, 37.2% of adolescents experienced high levels of stress and 25.1% suffered from depressive symptoms (Korea Centers for Disease Control and Prevention, 2016). Meanwhile, suicide remains the leading cause of death among adolescents although the recent suicide rate has been slightly reduced in Korea (Korean National Statistical Office, 2017). Specifically, 12.9–14.7% of Korean boys and 17.1–23.2% of girls exhibited suicidal ideation (Lee et al., 2018). Emotional distress, such as depression, anxiety, and anger, has been found to have the greatest impact on suicidal ideation risk (Miranda, Ortin, Polanco-Roman, & Valderrama, 2017; O’Connor & Nock, 2014).
About half of mental disorders emerge in adolescence; these disorders are often undetected until later in life (Kessler et al., 2007). In the United States, less than half of all adolescents with mental disorders receive any kind of treatment (Lipari, Hedden, Blau, & Rubenstein, 2013). In Korea, only 17.2% of Korean adolescents who needed psychiatric services actually sought treatment (Shin et al., 2011). Another study painted a grimmer picture: Among adolescents who perceived a need for mental health service, only 3.3% actually utilized the services available (N. Kim et al., 2012). Barriers to mental health service utilization identified in previous studies are inaccessibility to care, lack of health insurance, stigma of mental disorders, and lack of knowledge and understanding of mental disorders (Reardon et al., 2017; Shin et al., 2011).
As adolescents depend on their parents and caregivers to make the judgment for their referral, parents’ ability to recognize adolescents’ emotional distress symptoms is critical (Reardon et al., 2017). A recent meta-analysis (De Los Reyes et al., 2015) indicated low to medium levels of agreement between adolescents’ and their parents’ reports regarding adolescents’ mental health. However, few studies have systematically analyzed parent–adolescent agreement regarding adolescents’ emotional distress symptoms in Korea. Research exploring how the agreement differs by the age and gender of adolescents remains limited.
This study compared parent proxy reports and adolescent self-reports of adolescents’ emotional distress symptoms (namely, depression, anxiety, and anger). The specific aims of the study were to (1) assess the level of agreement between parent proxy reports and adolescent self-reports of adolescents’ emotional distress symptoms and (2) identify the differences in the level of agreement depending on the age and gender of adolescents.
Method
Population/Setting
To examine the agreement between Korean parent proxy reports and adolescent self-reports of emotional distress symptoms, this study recruited a convenience sample of adolescents aged 12–17 years and their parents from two middle schools and three high schools located in Seoul and Gyeonggi Province in Korea.
Study Procedure
This study was reviewed and approved by the institutional review board of the Seoul National University in South Korea. After obtaining permission from the principals and school nurses of the five selected schools, a recruitment letter informing the parents and students about the purposes and procedures of the study was sent to the students’ homes. When both the adolescent and his or her parent expressed interest in participating in this study, separate envelopes containing consent forms and paper questionnaires for the adolescent and parent were sent home with the student. Then, the student returned the completed consent forms and questionnaires to the school in the sealed envelopes to ensure participant confidentiality. Separate envelopes were used so that the adolescents and parents would not see each other’s questionnaires. Study data were collected from June through December 2016.
Measurements
The Korean versions of the Patient-Reported Outcomes Measurements Information System (PROMIS®) pediatric and parent proxy emotional distress measures (i.e., depression, anxiety, and anger) were employed in the study. The PROMIS was developed by the National Institutes of Health initiative to engender progress in the assessment of patient-reported outcomes. The original English pediatric and parent-proxy PROMIS emotional distress measures were designed to evaluate depression, anxiety, and anger for children under the age of 17 years (Irwin, Gross, et al., 2012; Irwin, Stucky, et al., 2012; Varni et al., 2012). Between 2015 and 2016, the original measures of PROMIS Pediatric Item Bank Version 1.1 for Depressive Symptoms (13 items), Anxiety (13 items), and Anger (5 items); Parent Proxy Item Bank Version 1.1 for Depressive Symptoms (13 items) and Anxiety (13 items); and PROMIS Parent Proxy Short form Version 1.0 for Anger (5 items) were translated into Korean in accordance with the Functional Assessment of Chronic Illness Therapy translation methodology: forward translation, reconciliation, back translation, expert reviews, harmonization and quality assurance, and cognitive interviews, successively (Choi, Ko, & Kim, 2017).
The participants were asked to respond to the measures based on recall of the last 7 days. The pediatric and parent-proxy measures for depression and anxiety consisted of 13 items each, and the anger measure had 5 items. The measures employed a 5-point Likert-type scale, on which 0 = never, 1 = almost never, 2 = sometimes, 3 = often, and 4 = almost always. Higher scores indicated higher levels of emotional distress. The completed measures were uploaded to the PROMIS Assessment Center, which assigned them a T-score. PROMIS measures were reported as T-scores (0–100) having a mean of 50 and a standard deviation (SD) of 10. Specifically, T-scores below 55 were considered to reflect a normal range of emotional distress symptoms (T-score < 55). T-scores that were 0.5 to <1.0 SD higher than the mean indicated mild symptoms (T-scores ≥ 55 and <60); scores that were 1.0 to <2.0 SD higher, moderate symptoms (T-scores ≥ 60 and <70); and scores that were ≥2.0 SD higher, severe symptoms (T-score ≥ 70; Cella, Gershon, Bass, & Rothrock, 2016). In this study, Cronbach’s α for the PROMIS pediatric depression, anxiety, and anger measures were .91, .91, and .88, respectively. Cronbach’s α for the PROMIS parent proxy depression, anxiety, and anger measures were .90, .91, and .86, respectively.
Data Analysis
Data were analyzed using SAS 9.2 (SAS Institute, 2008) and STATA 11 (Stata Corp, 2009). First, the characteristics of the adolescents and their parents were summarized using descriptive statistics. Second, the polychoric correlation coefficient and weighted k were used to assess agreement between parent proxy reports and adolescent self-reports for individual items. We also calculated the differences between parents’ and adolescents’ reports and the SD of those differences as a measure of response variability. Third, the χ2 test was used for examining differences in the normal range and symptomatic groups for emotional distress based on parents’ and adolescents’ reports. Based on PROMIS symptom severity levels, normal range (T-score < 55) and symptomatic (T-score ≥ 55) groups for emotional distress (depression, anxiety, and anger) were identified. Adolescents were divided into two age groups: younger (13–15 years old; middle school students) and older (16–17 years old; high school students).
Results
A total of 307 adolescents and 303 parents participated in the study; the final sample of 289 parent–adolescent dyads was used for data analysis. The ages of the adolescent participants ranged from 12 to 17 years, with a mean of 15.11 years (SD 1.28). The ages of their parents ranged from 35 to 64 years, with a mean of 45.51 years (SD 3.75). Of 289 adolescents, 152 (52.6%) were girls. Most of the parents (85.1%) were mothers.
As shown in Table 1, the mean scores of the parents’ and adolescents’ self-reports were 49.54 and 49.79 for depression, 45.64 and 46.02 for anxiety, and 42.95 and 44.13 for anger, respectively. The highest mean score of both parents and adolescents was for depression, followed by anxiety and anger. In terms of age and gender differences in mean scores for depression, anxiety, and anger, the mean scores for girls were higher than those for boys, whereas scores for older adolescents (high school students) were higher than those for younger adolescents (middle school students). High school girls had the highest mean scores for all three emotional distress measures, with the highest score of 52.22 for depression.
Descriptive Statistics of Emotional Distress Measures.
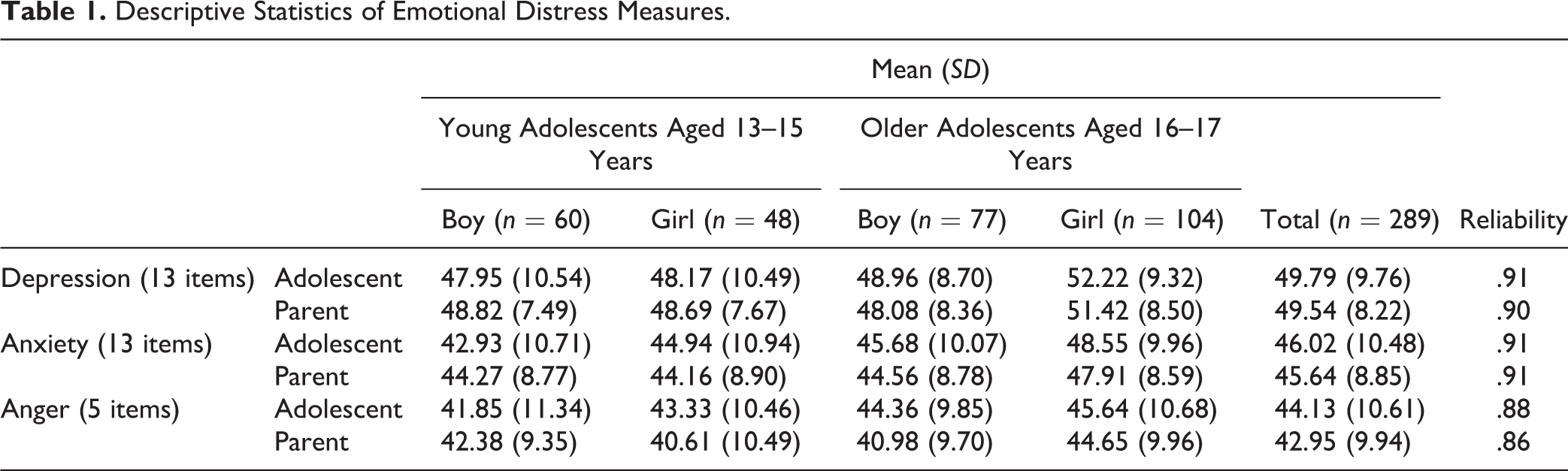
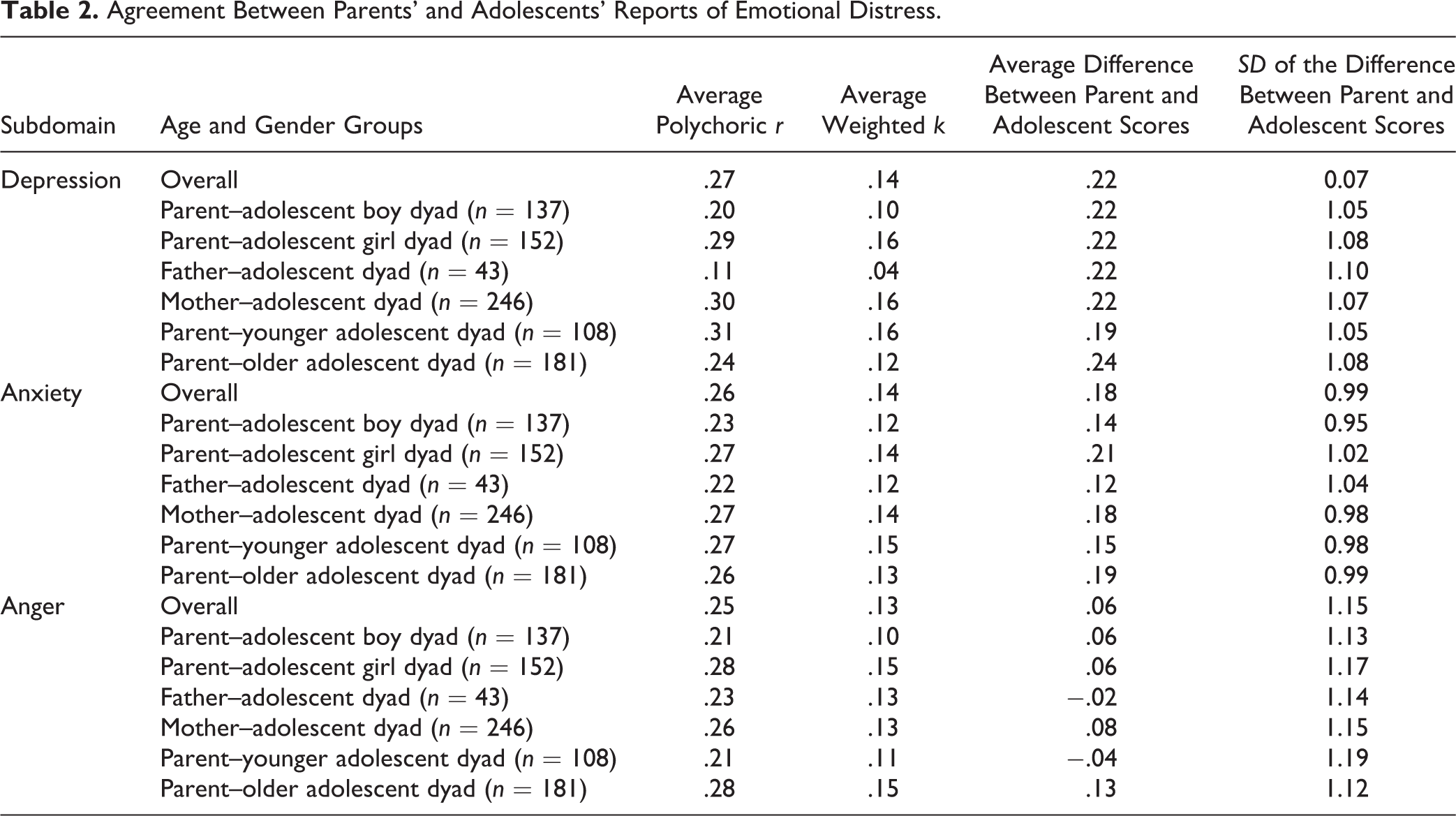
Table 2 shows the average agreement between the parent proxy reports and adolescent self-reports. Overall, the emotional distress measures showed low levels of agreement (average polychoric r: .25 to .27) between parents’ and adolescents’ reports. The average agreement was slightly higher for the depression scores, followed by the anxiety and anger scores. Agreement in parent–adolescent boy dyads was lower compared with parent–adolescent girl dyads. Agreement in father–adolescent dyads for all three emotional distress symptoms was lower than that of mother–adolescent dyads, particularly for depression. The parent–older adolescent dyads showed a lower level of agreement than parent–younger adolescent dyads for all emotional distress measures, except for anger.
Agreement Between Parents’ and Adolescents’ Reports of Emotional Distress.
The item-level agreement results for depression, anxiety, and anger items are presented in the adolescent item forms in the Online Appendix A–C. Specifically, for the depression measure, the agreement between parents and adolescents at the individual item level ranged from .19 to .37. The items “I could not stop feeling sad” and “I felt too sad to eat” showed the lowest level of agreement (r = .19). Meanwhile, the item “It was hard for me to have fun” showed the highest level of agreement (r = .37). In terms of parent–adolescent dyad agreement on the anxiety measure, the range of agreement for individual items was from .13 to .47. The item “I worried when I was at home” had the lowest agreement (r = .13), and the item “I was afraid of going to school” had the highest (r = .47). On the anger measure, the level of item agreement ranged from .16 to .32. The item “I felt mad” showed the lowest agreement (r = .16), whereas “I was so angry I felt like yelling at somebody” showed the highest (r = .32).
Next, emotional distress symptom scores were categorized into normal range (T-score < 55) and symptomatic (T-score ≥ 55) groups based on the parent proxy reports and adolescent self-reports. The cross-tabulated results of the analysis are presented in Table 3. The differences between parent and adolescent reports were statistically significant for all three emotional distress measures. Overall, parents consistently underestimated their children’s depression, anxiety, and anger: a high percentage of adolescents experiencing symptoms were rated in the normal range by their parents. Specifically, 49 of 101 adolescents (48.51%) with depressive symptoms and 52 of 99 adolescents (52.53%) with anxiety symptoms were rated in the normal range by the parents. The tendency to underestimate adolescents’ symptoms was more prominent for anger. Of 52 adolescents experiencing anger, 38 (73.08%) were rated in the normal range by the parents. In contrast, of 188 adolescents with normal-range depression scores, 47 (25%) were rated as symptomatic by parents, meaning that their symptoms were overestimated by their parents.
Cross Tabulation of Normal-Range and Symptomatic Groups for Emotional Distress.
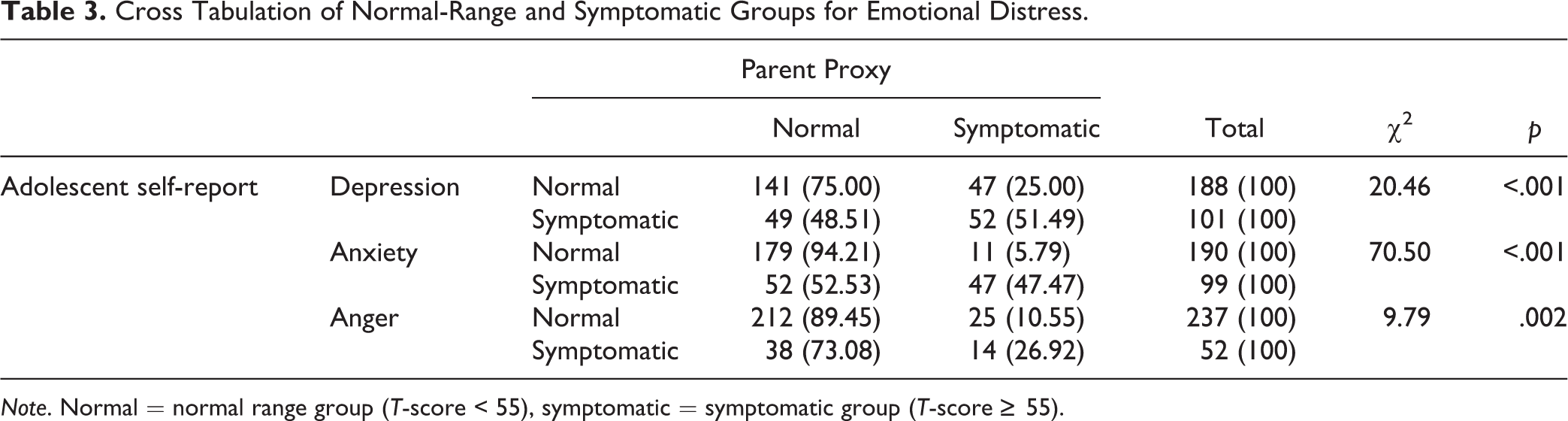
Note. Normal = normal range group (T-score < 55), symptomatic = symptomatic group (T-score ≥ 55).
On examining the degrees of discrepancy by adolescent age and gender (see Table 4), the study found that the discrepancy was particularly prominent for high school students experiencing anger. Specifically, 12 of 13 (92.31%) of the high school boys with anger were rated in the normal range by their parents. In addition, 19 of 25 (76%) of the high school boys with depressive symptoms, 17 of 25 (68%) of high school girls with anger, and 6 of 9 (66.67%) of middle school boys with anger were rated in the normal range by their parents. Meanwhile, 17 of 52 (32.69%) of the high school boys and 19 of 64 (29.69%) of the high school girls who reported normal-range depression scores were rated as being symptomatic by parents, meaning that their symptoms tended to be overestimated by their parents.
Percentage of Normal Range and Symptomatic Groups on Emotional Distress by Age and Gender.
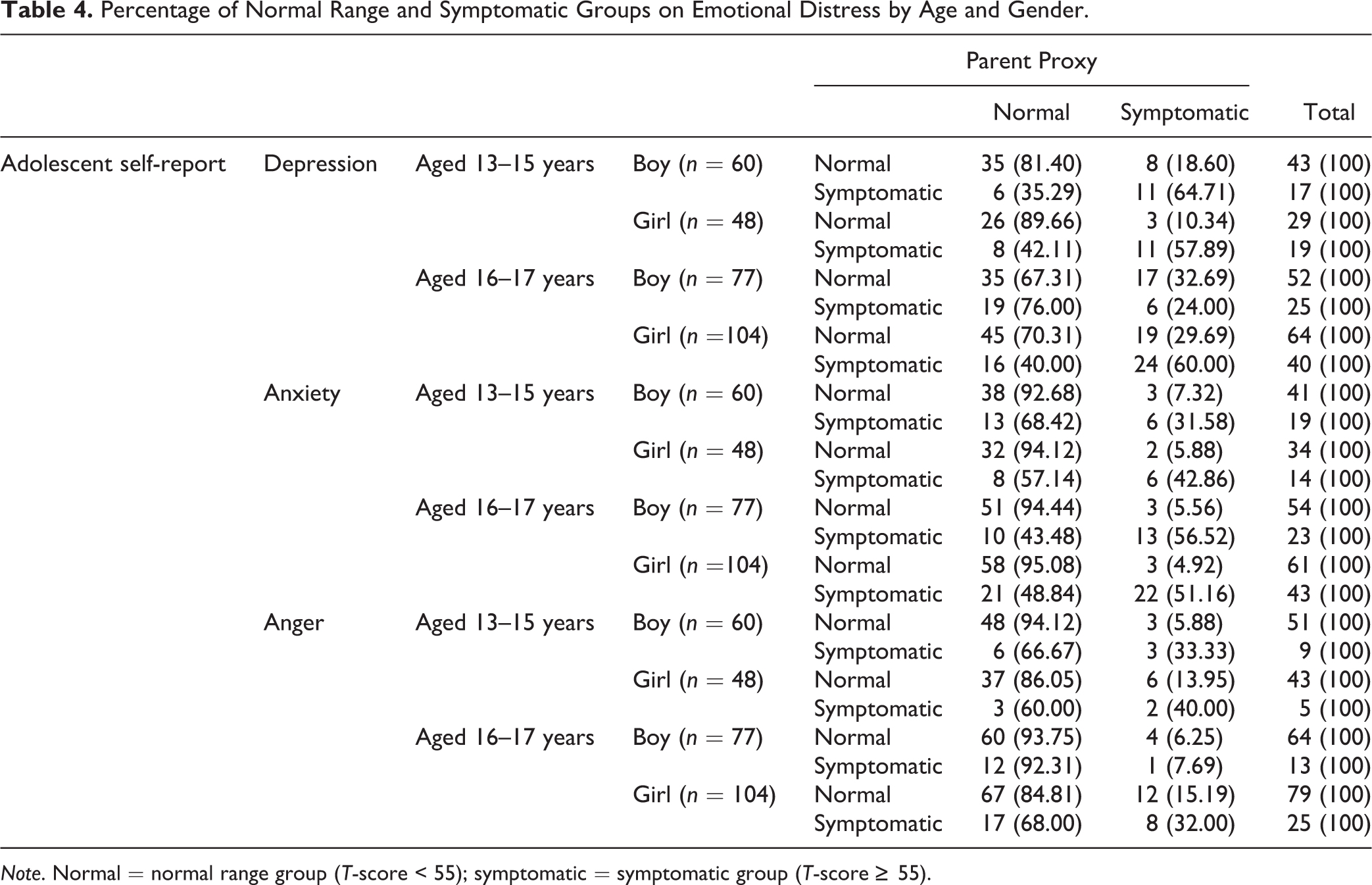
Note. Normal = normal range group (T-score < 55); symptomatic = symptomatic group (T-score ≥ 55).
Discussion
The school-based study was conducted to compare parent proxy reports and adolescent self-reports of adolescents’ emotional distress symptoms (depression, anxiety, and anger). The study had three main findings. First, the level of agreement between parent and adolescent reports was low, overall. Second, the level of agreement between parent and adolescent reports was particularly low for high school students, boys, and father–adolescent dyads. Finally, parents tended to underestimate the severity of their children’s emotional distress symptoms, particularly for high school students with anger.
Overall, in this school-based sample, the level of agreement between parent and adolescent reports of emotional distress symptoms was low, particularly for less observable symptoms. Our findings are consistent with those of a meta-analysis of 341 studies conducted in various countries, including the United States and Norway (De Los Reyes et al., 2015). In their study, adolescents’ and parents’ reports of adolescents’ mental health symptoms were correlated at low to moderate magnitudes, and a higher level of discrepancy was found for less observable and more internalized symptoms, such as emotional distress, compared with externalized behaviors and physical problems. In a Korean study, evaluating mental health literacy among parents of adolescents, only 32.5% were able to recognize adolescents’ depression (Ko & Choi, 2015). Varni et al. (2015) examined the agreement between pediatric patients aged 8–17 years and their parents using the PROMIS pediatric and parent proxy measures. These researchers also found that parent–child agreement was lower for emotional distress (average polychoric r: .26 to .28) than for physical symptoms (average polychoric r ranged from .40 to .68). In Varni et al.’s study, the level of agreement between parent proxy reports and adolescent self-reports of adolescents’ emotional distress (.26 to .28) was similar to that observed in our study. Thus, parents of adolescents may not be able to recognize fully the symptoms of emotional distress in their children.
With respect to the age and gender differences in the level of agreement between parent proxy reports and adolescent self-reports, agreement was particularly low for boys, high school students, and father–adolescent dyads. According to a meta-analysis on gender differences in emotional expression in children (Chaplin & Aldao, 2013), girls tend to display more internalized emotions (e.g., depression and anxiety) whereas boys, more externalized emotions (e.g., anger) until middle childhood aged 6– 12 years. However, as boys enter adolescence, they tend to show fewer externalized emotions than girls. In this regard, adolescent boys are less likely to express their emotional distress symptoms than adolescent girls, and thus, boys’ symptoms may not be easily recognizable to their parents. As adolescents make the transition from childhood to adulthood, conflicts with parents tend to become more intense (Noller & Callan, 2015); such conflict makes it difficult for parents to recognize adolescents’ emotional cues.
Moreover, given the academic pressure experienced by Korean high school students, they may have little time to share their emotional issues with their parents. Korean high school students spend an average of about 12 hr a day in school to prepare for their college entrance examination (G. Kim, 2015); thus, they have limited time to spend with their parents at home. According to national data, 84.7% of Korean adolescents spend less than an hour a day in conversation with their parents (Ministry of Gender Equality and Family, 2017).
In our study, father–adolescent dyads showed lower agreement than mother–adolescent dyads. Fathers have been found to be less engaged in parenting than mothers and to tend to avoid their adolescent children’s expressions of negative emotions (Elster & Lamb, 2013; Phares, Fields, & Kamboukos, 2009). As for Korean fathers, they tend to have much less time than mothers to spend in conversation with their adolescent children. Specifically, 52.5% of Korean adolescents reported having spent less than half an hour a day having conversations with their fathers (Ministry of Gender Equality and Family, 2017). As fathers play a critical role in their children’s emotional, physical, and social development, programs to improve fathers’ communication skills and emotional responsiveness are beneficial. Parental emotional responsiveness refers to a parent’s ability to respond emotionally to a child’s needs and to be supportive of a child’s uniqueness through verbal and nonverbal communication (Babylon Online Dictionary, 2018; Haverfield & Theiss, 2017). This ability leads to comfortable, warm, intimate, and nondefensive attachments with children. Moreover, it has been associated positively with adolescent regulation of emotion and negatively with adolescent impulsiveness; positive influences of parental responsiveness remain significant during both happy and unhappy parent–child interactions (Haverfield & Theiss, 2017).
The final finding that deserves special attention is that parents tended to underestimate their children’s emotional distress symptoms, particularly where older adolescents and adolescents experiencing anger were involved. As a result, a substantial number of adolescents with symptoms of emotional distress may be at risk of their symptoms not being recognized by their parents. This lack of parental recognition of emotional distress symptoms may lead to inadequate treatment for adolescents. Bullying and school violence are now recognized as posing serious social and health problems for adolescents (Bhang et al., 2012; Jennings, Song, Kim, Fenimore, & Piquero, 2017; Song, Hong, Yook, Kim, & Lee, 2016). Internalized anger is a significant predictor of violent behavior toward the self and others (Ammerman, Kleiman, Uyeji, Knorr, & McCloskey, 2015), and as such, it is critical that high levels of anger in adolescents be recognized early. In Korea, adolescents face overwhelming academic pressure and have limited skills and opportunities to vent their anger in healthy ways. They often struggle with the negative consequences of unresolved anger. Given our findings, it is altogether possible that parents of Korean adolescents with symptoms of anger and other negative emotions will not fully recognize the severity of their children’s symptoms.
The lack of agreement between parents’ and adolescents’ reports on matters of consequence is not about right or wrong parenting (Sweeting & West, 1998). Rather, it may point to the different perspectives between parents and adolescents on such matters. Our study showed that parents may not be sensitive and knowledgeable enough to detect emotional distress symptoms in their adolescent children. However, parent proxy reports remain valuable, and parents are still important informants who can provide information to complement adolescent self-reports. Thus, school nurses should consider providing programs that will enlighten Korean parents on the cues that signal emotional distress in their adolescent children and on the potential negative outcomes of untreated distress. Such programs could also promote parent–child communication regarding adolescent emotional distress. In addition, school nurses should address such distress in adolescent students by helping the latter learn to articulate and properly manage their negative emotions.
Limitations and Suggestions for Future Research
This study has several limitations. Parental and familial factors explain the level of agreement between parent and adolescent reports (Montgomery, 2008). These characteristics, including parent education level, family socioeconomic status, family relationships, and parent mental health, may impact the degree of agreement between parent proxy reports and adolescent self-reports. The measurement of these characteristics is recommended for future research. Also, the findings may have limited generalizability owing to the nature of the convenience sampling used in this study. In addition, our study’s school-based adolescent sample was not subjected to clinical examinations for mental health. Objective assessment of adolescent mental health symptoms remained unexplored although mental health assessment by means of adolescent self-reporting has been shown to be valid and reliable (Verhulst, Prince, Vervuurt-Poot, & Jong, 1989). Finally, additional qualitative studies are needed to explore the reasons for the lack of agreement between parent and adolescent reports regarding adolescent emotional distress symptoms in particular areas. Such studies would provide useful insights for future nursing research and practice.
School Nursing Implications
Early recognition and treatment of adolescent emotional distress are crucial, given the negative consequences of untreated distress on adolescent development. Our findings revealed gaps between parent and adolescent reports on adolescents’ emotional distress. The specific age and gender groups, as well as areas of distress where the gaps were prominent, were identified as well. Based on the understanding gained, we believe it is important for school nurses to intervene in such a way as to narrow those gaps.
School nurses, especially in Korea, are ideally positioned to approach both adolescent students and their parents to improve understanding of adolescent emotional distress symptoms, given that Korean adolescents spend most of their waking time in school. School nurses need to provide tailored parent education programs that aim at improving parents’ knowledge and awareness of adolescents’ emotional distress as well as programs that promote adolescents’ ability to express their emotions. It is important that parents and adolescents are assisted in engaging in open and responsive parent–child communications that may lead to understanding each other’s perspective on emotional issues and mental health service utilization. Considering the growing diversity in schools, it would also be important for school nurses to observe the parent–adolescent agreement regarding mental health and well-being. For school nurses to be educationally and experientially prepared for taking on this responsibility, the Ministry of Education and the regional offices of education need to recognize and support the criticality of the school nurses’ role; furthermore, they should incorporate the appropriate education programs into the already established vocational training that school nurses mandatorily take.
Supplemental Material
Supplemental Material, Supplementary_documents_Revision_FINAL_06July2018 - Agreement Between Parent Proxy Reports and Self-Reports of Adolescent Emotional Distress
Supplemental Material, Supplementary_documents_Revision_FINAL_06July2018 for Agreement Between Parent Proxy Reports and Self-Reports of Adolescent Emotional Distress by Chanhee Kim, Heeseung Choi, Heesung Ko and Chang Gi Park in The Journal of School Nursing
Footnotes
Authors’ Note
Appendices A, B, and C in supplementary material show the agreement (polychoric correlations, weighed k) for individual items of the three measures.
Acknowledgments
The authors acknowledge the adolescents and their parents who participated in this study. They also gratefully acknowledge the help of school nurses in collecting the study data. Thanks are also due to Mr. Jon Mann of the University of Illinois at Chicago for his editorial support.
Author Contributions
HC conceived the study; HC, CK, and HK conducted the data collection; CK and HC conducted statistical analyses and drafted the manuscript; CGP provided the statistical consultation; CK, HC, HK, and CGP participated in the interpretation of the study findings and reviewed all manuscript drafts. All authors have read and approved the final manuscript.
Declaration of Conflicts of Interests
The authors(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Promising-Pioneering Researcher Program of Seoul National University.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.