
Abstract
Bullying is a prevalent form of interpersonal violence in childhood. Sleep disruption may represent a modifiable factor linking bullying exposure to school outcomes, yet population-level evidence remains limited. Using pooled 2022–2024 National Survey of Children's Health data, we examined associations between bullying exposure, sleep health (short sleep, <9 h; bedtime consistency), and chronic absenteeism due to illness or injury (≥11 missed school days) among U.S. children aged 6–11 years (up to n = 45,118). Approximately 45% of children experienced bullying in the past year. Bullying exposure was associated with higher odds of short sleep, with graded increases for occasional and frequent bullying. Bullying was also strongly associated with chronic absenteeism. In sequential models, bedtime consistency remained independently associated with chronic absenteeism, whereas short sleep was not significant after accounting for bedtime consistency. Findings identify bedtime consistency as the sleep indicator most consistently associated with absenteeism risk in middle childhood.
Introduction
Bullying is a prevalent and harmful form of interpersonal violence often experienced during childhood and early adolescence (Burr et al., 2024). As a manifestation of peer violence, bullying involves repeated aggressive physical, verbal, relational, or social behaviors characterized by a power imbalance and intent to harm (Smith, 2016). Bullying can occur through in-person interactions and digital contexts, including cyber-based victimization that has increased alongside social media and online communication. Surveillance efforts indicate that a substantial proportion of U.S. children experience bullying each year, underscoring its population-level relevance (Gladden et al., 2014). Bullying exposure has been associated with adverse mental health, emotional, and academic outcomes, including internalizing symptoms, behavioral difficulties, and impaired school functioning (Farrington & Baldry, 2010; Fekkes et al., 2004). Accordingly, bullying is recognized as a public health concern and a priority target within violence prevention research and policy (Arseneault, 2018).
Although the association between bullying exposure and psychosocial maladjustment is well documented, less attention has focused on potentially modifiable behavioral factors that may link bullying exposure to functional school outcomes. Sleep health is one plausible factor that remains understudied in population-based research (Levková et al., 2025). Adequate and consistent sleep supports children's cognitive performance, emotional regulation, and physical health, and insufficient or irregular sleep has been linked to deficits in attention, mood regulation, and academic functioning (El-Sheikh & Kelly, 2017; Mindell & Williamson, 2018). Sleep disruption may represent one behavioral factor through which exposure to interpersonal stressors, including bullying, influences children's health and school functioning (El-Sheikh & Kelly, 2017; van Geel et al., 2016).
Emerging evidence suggests that psychosocial stressors and victimization can adversely affect children's sleep duration and sleep routines (Zhao, 2023). Stress-related hyperarousal, anxiety, and emotional dysregulation may interfere with sleep initiation and maintenance, increasing the likelihood of short sleep and inconsistent bedtimes among victimized children (Sadeh et al., 2014). In turn, insufficient or irregular sleep is associated with poorer academic functioning and increased school absenteeism (Dahl, 1996; Dewald et al., 2010). Despite these links, relatively few nationally representative studies have examined whether sleep characteristics partially explain associations between bullying exposure and school absenteeism in middle childhood (van Geel et al., 2016).
This gap is relevant to school nursing practice because school nurses often encounter students with bullying-related somatic complaints, sleep-related concerns, and attendance problems that require coordinated school and family response (Lineberry & Ickes, 2015). School nurses work at the intersection of student health, school attendance, and psychosocial well-being, and therefore, play a critical role in identifying and responding to both bullying exposure and sleep-related concerns. As frontline providers within school settings, school nurses frequently encounter students presenting with somatic complaints, fatigue, or recurrent absenteeism, which may reflect underlying psychosocial stressors such as bullying or insufficient sleep (Fekkes et al., 2004; Dewald et al., 2010). In addition to supporting school-based bullying prevention initiatives, school nurses are equipped to assess sleep behaviors, provide anticipatory guidance to families, and reinforce consistent sleep routines as part of routine care (Mindell & Williamson, 2018; Owens & Weiss, 2017). Integrating sleep health promotion into school nursing practice may represent a feasible and complementary strategy to mitigate the downstream functional consequences of bullying exposure, including school absenteeism (Dewald et al., 2010; El-Sheikh & Kelly, 2017). Accordingly, examining sleep as a potentially modifiable behavioral factor linking bullying exposure to school attendance outcomes has direct relevance for school nursing practice and school health policy.
Using pooled, nationally representative data from the National Survey of Children's Health (NSCH), this study examined associations among bullying exposure, sleep health, and illness- or injury-related school absenteeism among U.S. children aged 6–11 years (U.S. Census Bureau, 2025a, 2025b, 2025c, 2025d). This age range aligns with pediatric sleep duration recommendations and captures a developmental period in which both bullying exposure and school engagement are highly salient (Paruthi et al., 2016). By integrating bullying frequency, sleep duration, bedtime consistency, and absenteeism, the study sought to identify potentially modifiable behavioral factors that may inform school-based violence prevention and student support strategies. Given the central role of school nurses in identifying bullying, monitoring student attendance, and addressing health-related barriers to learning, understanding potentially modifiable behavioral factors such as sleep that may link bullying exposure to absenteeism has direct relevance for school nursing practice and school-based interventions. To address current gaps in the literature, the following research questions were addressed for U.S. children aged 6–11 years:
Methods
Study Design and Data Source
This study used a cross-sectional analytic design with pooled data from the 2022–2024 NSCH, a nationally representative survey of child health in the United States. The NSCH employs a complex, multistage probability sampling design using address-based sampling from the U.S. Census Bureau's Master Address File to generate population-level estimates of physical, behavioral, familial, and social environmental health among children and adolescents. Households are randomly selected and mailed a screener questionnaire to identify children ages 0–17 years residing in the home. Based on screener responses, one child per household is randomly selected, and a knowledgeable caregiver (typically a parent or legal guardian) completes an age-specific topical questionnaire corresponding to one of three mutually exclusive age groups: 0–5 years, 6–11 years, or 12–17 years.
Survey weights are applied to account for selection probability, nonresponse, and demographic distributions, allowing for nationally representative estimates. Data from the 2022, 2023, and 2024 NSCH cross-sectional surveys were combined into a single analytic dataset using pooled weights, consistent with NSCH guidance for multiyear analyses (U.S. Census Bureau, 2025a). The 2022–2024 survey cycles were selected to provide the most recent nationally representative estimates of child health while maximizing sample size and statistical power through pooled analysis. Detailed NSCH sampling, weighting, and data collection procedures are described elsewhere (U.S. Census Bureau, 2025a, 2025b, 2025c, 2025d). Public-use NSCH data contain no personally identifiable information. Accordingly, this study was classified as nonhuman subjects research and deemed exempt from review by the University of Alabama Institutional Review Board (IRB #: 26-02-9399).
Study Sample
The analytic sample was restricted to children ages 6–11 years to align with both the NSCH age-specific questionnaire structure and established pediatric sleep duration recommendations. This age range corresponds to the American Academy of Sleep Medicine (AASM) guideline that children ages 6–12 years should obtain 9–12 h of sleep per 24-h period (Paruthi et al., 2016). Adolescents have lower recommended sleep durations due to developmental shifts in circadian timing and sleep regulation, and including children who completed the adolescent questionnaire would require different sleep duration thresholds and introduce developmental heterogeneity.
Because the NSCH assigns children to mutually exclusive topical questionnaires, inclusion of children outside the 6–11-year module would complicate the interpretation of sleep duration, bedtime consistency, and school attendance measures. Therefore, children from the 0–5-year and 12–17-year topical questionnaires were excluded to preserve developmental consistency and ensure a uniform operational definition of short sleep. Children with missing data on bullying exposure, sleep duration, bedtime consistency, school absenteeism, child age, or other covariates included in a given model were excluded using listwise deletion, consistent with prior NSCH-based analyses (Lebrun-Harris, Ghandour, Kogan, Warren, 2022). After applying inclusion criteria and accounting for missing data, the unweighted analytic sample included 46,149 U.S. children ages 6–11 years. This represents the unweighted number of children ages 6–11 years included across the pooled 2022–2024 NSCH cycles and reflects the subset of respondents meeting inclusion criteria within the publicly available dataset. Complete-case sample sizes varied by model due to listwise deletion (range: 45,383–44,852; see Appendix A for missingness analyses).
Measures
Bullying Exposure
Bullying exposure was assessed using a caregiver-reported item asking how often, during the past 12 months, the child was bullied, picked on, or excluded by other children, excluding siblings or dating partners. Response options ranged from never to almost every day. Consistent with prior NSCH research and to reduce sparse cell counts, responses were collapsed into a three-category bullying frequency variable: never bullied, occasional bullying (1–2 times in the past year or 1–2 times per month), and frequent bullying (1–2 times per week or almost every day). In regression models, never bullied served as the reference category.
Short Sleep Duration
Sleep duration was assessed using a caregiver-reported item asking how many hours of sleep the child obtains on most weeknights, with ordinal response options ranging from <6 h to ≥11 h. Consistent with AASM recommendations for this age group (Paruthi et al., 2016), weeknight sleep duration was dichotomized. Children obtaining <9 h of sleep were classified as experiencing short sleep, whereas children obtaining ≥9 h were classified as obtaining adequate sleep. In regression models, short sleep (<9 h) was coded as the event, and adequate sleep (9–11+ hours) served as the reference category.
Bedtime Consistency
Bedtime consistency was measured using a caregiver-reported item asking how often the child went to bed at about the same time on weeknights, with response options ranging from always to never. To align with pediatric sleep hygiene recommendations, improve interpretability, and maintain consistency with previous NSCH analyses (Lebrun-Harris, Ghandour, Kogan & Warren, 2022), responses were collapsed into three categories: consistent bedtimes (always or usually), variable bedtimes (sometimes), and inconsistent bedtimes (rarely or never). Consistent bedtimes (always or usually) served as the reference category in the models. Although bedtime consistency is inherently ordinal, categories were collapsed to improve interpretability and model stability, given sparse observations in higher-risk response categories.
Chronic School Absenteeism
School absenteeism was assessed using a caregiver-reported item asking how many days during the past 12 months the child missed school due to illness or injury. Consistent with chronic absenteeism thresholds, responses were dichotomized as 0–10 missed days versus 11 or more missed days. In regression models, chronic absenteeism (11+ missed days) was coded as the event, and 0–10 missed days served as the reference category.
Covariate
Child age in years was included as a continuous covariate in all models to account for developmental variation within the 6–11-year age range. Child age was included as a continuous variable without transformation or centering to preserve the interpretability of model estimates.
Statistical Analyses
All analyses accounted for the complex sampling design of the NSCH, including stratification, clustering, and survey weights, using the Complex Samples module in IBM SPSS Statistics, Version 31.0.0.0 (IBM Corp., Armonk, NY). Weighted descriptive statistics characterized the study population and estimated the prevalence of bullying exposure, sleep behaviors, and chronic absenteeism. Missingness across study variables was low (1.2%–1.7%; Appendix A). Given the minimal missingness and large sample size, complete-case (listwise deletion) estimation was used, consistent with recommended practice for complex survey analyses (Heeringa et al., 2017; Little & Rubin, 2019).
To address RQ1, complex samples logistic regression models examined associations between bullying exposure and short sleep duration (Model 1), bullying exposure and bedtime consistency (Model 2a), and bedtime consistency and short sleep duration (Model 2b). To address RQ2–RQ4, sequential logistic regression models estimated associations between bullying exposure and chronic absenteeism, first without sleep variables (Model A), then with short sleep (Model B), bedtime consistency (Model C), and both sleep variables simultaneously (Model D). Child age was included as a continuous covariate in all models.
Model explanatory power was evaluated using Nagelkerke pseudo-R2 statistics, and changes in bullying coefficients (ΔB) were examined following inclusion of sleep variables. Because pseudo-R2 values in logistic regression are not directly comparable to R2 in linear models and do not have universally accepted interpretive thresholds, changes were evaluated comparatively across nested models alongside consistency of parameter estimates. Even modest increases in pseudo-R2 may reflect meaningful improvements in explanatory value when accompanied by stable or theoretically consistent parameter estimates (Menard, 2002). This comparative approach is consistent with recommendations for logistic regression and complex survey data analysis, emphasizing parameter stability and incremental model improvement rather than reliance on standardized cut points (Heeringa et al., 2017). Sensitivity analyses using multinomial models evaluated whether preserving the ordinal structure of bedtime consistency altered the interpretation of findings (Appendix B).
Given the cross-sectional design, sleep factors were evaluated as explanatory factors using sequential design-based logistic regression models, with changes in coefficients interpreted as attenuation rather than evidence of causal mediation. Adjusted odds ratios (aORs) with 95% confidence intervals are reported. Statistical significance was defined as p < .05, and interpretation emphasized effect sizes and practical relevance in addition to statistical significance. Odds ratios were interpreted using conventional benchmarks for epidemiologic research (e.g., OR ≈ 1.2–1.5 = small, 1.5–2.5 = moderate, >2.5 = large). Changes in coefficients (ΔB) and model explanatory power (ΔR2) were evaluated comparatively across nested models, consistent with recommended practices for logistic regression and complex survey data analysis (Hosmer et al., 2013; Heeringa et al., 2017).
Results
Data Properties
Missingness analyses indicated low levels of item nonresponse across all study variables (range: 1.2%–1.7%; Appendix A). Analytic sample sizes varied modestly across models due to outcome-specific missingness under listwise deletion, with complete-case sample sizes ranging from 45,383 to 44,852. These differences reflect variable-specific nonresponse rather than systematic exclusion based on predictors.
Sensitivity analyses using multinomial models (Appendix B: Model 2a, RQ1) yielded results consistent with the primary analyses (Table 2: Model 2b). Specifically, bullying exposure was associated with increased odds of less consistent bedtime routines, with stronger associations observed for the most irregular category (inconsistent bedtime) relative to the intermediate category (variable bedtime), indicating a graded relationship. These multinomial results support the decision to collapse bedtime consistency categories in the primary analyses, demonstrating that associations between bullying exposure and bedtime consistency follow a graded pattern across levels of irregularity.
Characteristics of Children Aged 6–11 Years Overall and by Bullying Exposure, NSCH 2022–2024 (Pooled).
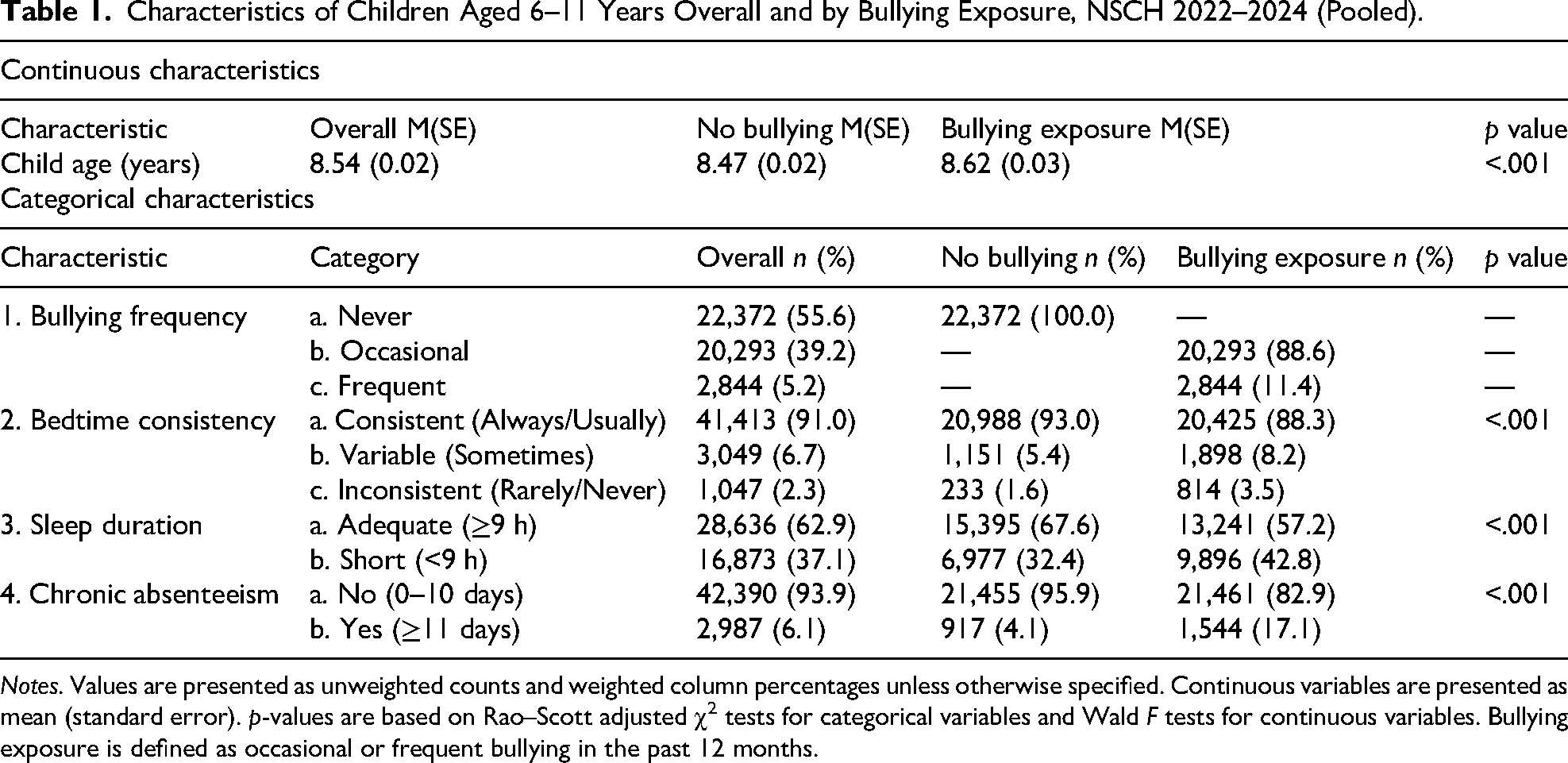
Notes. Values are presented as unweighted counts and weighted column percentages unless otherwise specified. Continuous variables are presented as mean (standard error). p-values are based on Rao–Scott adjusted χ2 tests for categorical variables and Wald F tests for continuous variables. Bullying exposure is defined as occasional or frequent bullying in the past 12 months.
Sample Characteristics
Among the U.S. children included in the analytic sample, 44.5% experienced bullying in the past 12 months, whereas 55.5% were not bullied. Of those exposed, most experienced occasional bullying (39.2%), while a smaller proportion experienced frequent bullying (5.2%). The mean child age was 8.54 years (SE = 0.02), and bullied children were slightly older than nonbullied children (8.62 vs. 8.47 years, p < .001). Bullying exposure varied modestly by child sex and more noticeably by race/ethnicity. Boys and girls were similarly represented in the analytic sample (51.1% boys, 48.9% girls), and the distribution of bullying frequency was largely comparable across sex categories. Occasional bullying was reported by 19.9% of boys and 19.2% of girls, while frequent bullying was reported by 2.9% of boys and 2.3% of girls, indicating only minor differences in exposure prevalence based on descriptive comparisons; formal statistical testing of sex differences was not conducted.
In contrast, bullying exposure differed across racial and ethnic groups when examining the distribution of cases within the overall sample. Non-Hispanic White children comprised the largest proportion of the sample (69.8%) and accounted for the largest share of bullying exposure, including 28.6% experiencing occasional bullying and 3.7% experiencing frequent bullying. Non-Hispanic Black children represented 13.1% of the sample, with 4.4% reporting occasional bullying and 0.8% reporting frequent bullying. Children identified as Hispanic, multiracial, or other racial groups collectively accounted for smaller proportions of bullying exposure within the total sample. These percentages reflect the distribution of bullying exposure across the overall sample rather than within-group prevalence estimates. Together, these findings indicate that bullying exposure is common within the overall sample of children ages 6–11 years.
Sleep characteristics differed significantly by bullying exposure. Short sleep (<9 h) was more prevalent among bullied children than nonbullied children (42.8% vs. 32.4%, p < .001), representing an absolute difference of approximately 10 percentage points, indicating a meaningful difference in prevalence at the population level. Bedtime consistency also differed by bullying exposure (p < .001), with bullied children more likely to have inconsistent bedtimes (3.5% vs. 1.6%) and less likely to have consistent bedtimes (88.3% vs. 93.0%). Chronic absenteeism due to illness or injury (11 or more missed school days in the past 12 months) was reported for 6.1% of children overall and varied markedly by bullying exposure (4.1% among children never bullied, 7.6% among children experiencing occasional bullying, and 17.1% among children experiencing frequent bullying; p < .001). Table 1 summarizes weighted percentages and unweighted sample counts overall, stratified by bullying exposure.
RQ1 (Models 1–2): Bullying, Short Sleep, and Bedtime Consistency
Models 1–2 (RQ1) examined associations between bullying exposure and sleep health indicators, as well as the association between bedtime consistency and short sleep duration. Model 1 (RQ1) estimated the association between bullying exposure and short sleep duration, adjusting for child age. Relative to children who were not bullied, children experiencing occasional bullying had higher odds of short sleep (aOR = 1.34, 95% CI: 1.18–1.52), and those experiencing frequent bullying had still higher odds (aOR = 1.43, 95% CI: 1.19–1.71). Older age was independently associated with increased odds of short sleep (aOR per year = 1.19, 95% CI: 1.15–1.24). Model explanatory power was modest (Nagelkerke R2 = 0.029), consistent with expectations for logistic regression models of behavioral outcomes.
Model 2a (RQ1) estimated the association between bullying exposure and bedtime consistency. Bullying exposure was associated with a greater likelihood of less consistent bedtime routines, with stronger associations observed for higher levels of bullying frequency (see Appendix B for multinomial sensitivity results demonstrating graded associations across bedtime categories). Model 2b (RQ1) examined the association between bedtime consistency and short sleep duration. Bedtime consistency demonstrated a strong graded association with short sleep. Compared with children with consistent bedtimes, children with variable bedtimes had nearly threefold higher odds of short sleep (aOR = 2.97, 95% CI: 2.44–3.60), and children with inconsistent bedtimes had more than fourfold higher odds (aOR = 4.29, 95% CI: 3.12–5.90). Model explanatory power increased (Nagelkerke R2 = 0.076), representing a relative improvement in explanatory value following inclusion of bedtime consistency, indicating that bedtime regularity is strongly associated with sleep duration.
RQ2 (Model A): Bullying and Chronic Absenteeism
RQ2 examined whether bullying exposure was associated with chronic absenteeism. Complex samples logistic regression models were estimated with chronic absenteeism as the dependent variable, adjusting for child age. Relative to children who were never bullied, children experiencing occasional bullying had higher odds of chronic absenteeism (aOR = 1.94, 95% CI: 1.62–2.31), and children experiencing frequent bullying had substantially higher odds (aOR = 4.93, 95% CI: 3.78–6.44). Older age was independently associated with lower odds of chronic absenteeism (aOR per year = 0.94, 95% CI: 0.89–0.99). Model explanatory power was modest (Nagelkerke R2 = 0.038), consistent with expectations for logistic regression models in population-based data (Table 2).
Complex-Samples Logistic Regression Models Predicting Short Sleep (<9 Hours) (RQ1, Models 1–2b; See Appendix B for Model 2a).
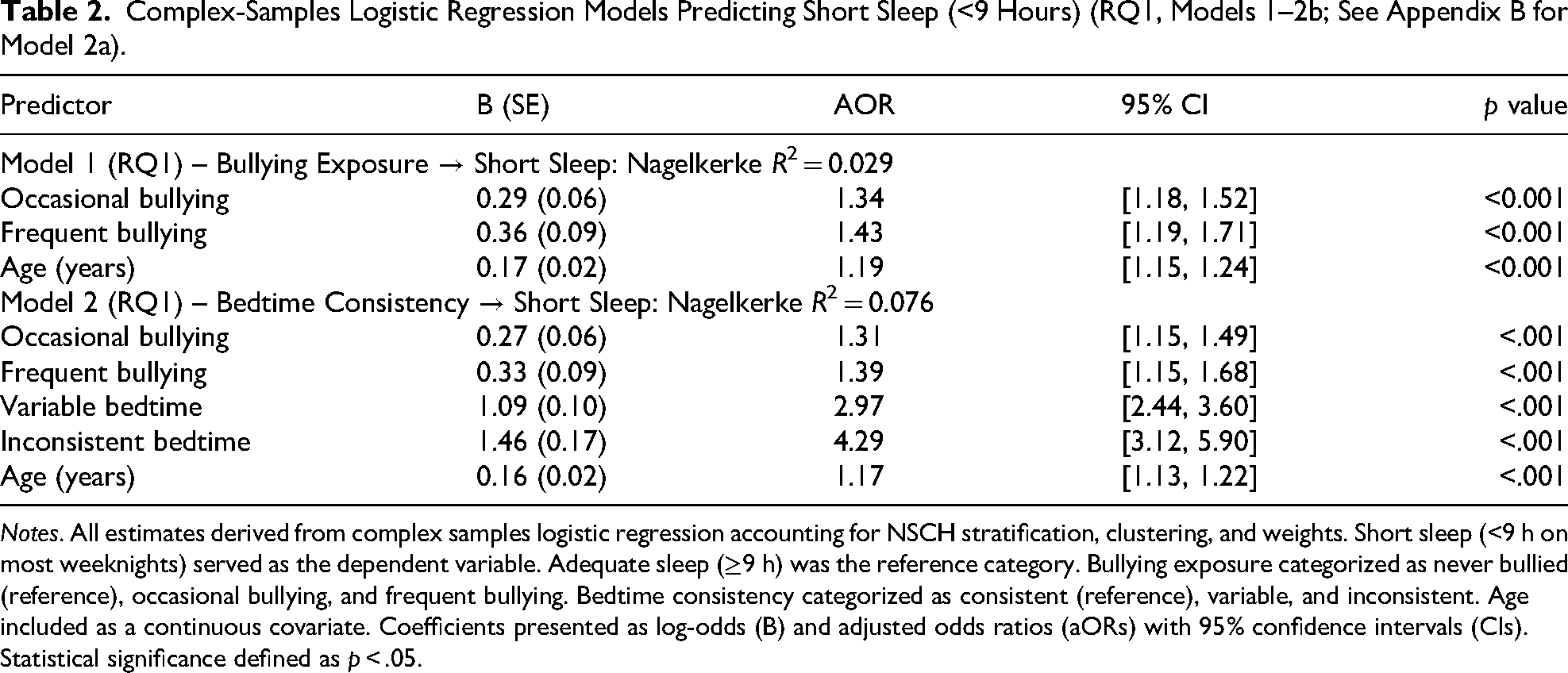
Notes. All estimates derived from complex samples logistic regression accounting for NSCH stratification, clustering, and weights. Short sleep (<9 h on most weeknights) served as the dependent variable. Adequate sleep (≥9 h) was the reference category. Bullying exposure categorized as never bullied (reference), occasional bullying, and frequent bullying. Bedtime consistency categorized as consistent (reference), variable, and inconsistent. Age included as a continuous covariate. Coefficients presented as log-odds (B) and adjusted odds ratios (aORs) with 95% confidence intervals (CIs). Statistical significance defined as p < .05.
RQ3 (Models B–C): Sleep Characteristics and Chronic Absenteeism
Models B–C (RQ3) evaluated whether short sleep and bedtime consistency were independently associated with chronic absenteeism after accounting for bullying exposure and age. Model B (RQ3) added short sleep to Model A. Short sleep was independently associated with higher odds of chronic absenteeism (aOR = 1.24, 95% CI: 1.04–1.48). Bullying exposure remained strongly associated with chronic absenteeism (occasional bullying: aOR = 1.95, 95% CI: 1.64–2.33; frequent bullying: aOR = 4.88, 95% CI: 3.73–6.37). Model explanatory power increased slightly (Nagelkerke R2 = 0.040), indicating minimal incremental explanatory value associated with short sleep.
Model C (RQ3) replaced short sleep with bedtime consistency. Bedtime consistency was independently associated with chronic absenteeism. Compared with children with consistent bedtimes, children with variable bedtimes had higher odds of chronic absenteeism (aOR = 1.76, 95% CI: 1.28–2.43), and children with inconsistent bedtimes had higher odds (aOR = 2.48, 95% CI: 1.72–3.60). Bullying exposure remained strongly associated with chronic absenteeism (occasional bullying: aOR = 2.00, 95% CI: 1.69–2.38; frequent bullying: aOR = 4.84, 95% CI: 3.69–6.33). Model explanatory power increased more substantially (Nagelkerke R2 = 0.049), indicating additional explanatory value associated with bedtime consistency relative to short sleep.
RQ4 (Model D): Changes in the Bullying–Chronic Absenteeism Association After Adjustment for Sleep
Model D (RQ4) estimated a fully adjusted model including bullying exposure, short sleep, bedtime consistency, and age. Bedtime consistency remained independently associated with chronic absenteeism (variable bedtime: aOR = 1.71, 95% CI: 1.24–2.35; inconsistent bedtime: aOR = 2.38, 95% CI: 1.64–3.48), whereas the association between short sleep and absenteeism was reduced and no longer statistically significant (aOR = 1.12, 95% CI: 0.94–1.34; p = .198). Bullying exposure remained strongly associated with chronic absenteeism (occasional bullying: aOR = 2.01, 95% CI: 1.69–2.39; frequent bullying: aOR = 4.81, 95% CI: 3.67–6.30). Model explanatory power increased slightly further (Nagelkerke R2 = 0.050), indicating incremental improvement in model fit relative to prior models (Table 3).
Sequential Complex-Samples Logistic Regression Models Predicting Chronic Absenteeism (≥11 Days Missed) (RQ2–RQ4, Models A–D).
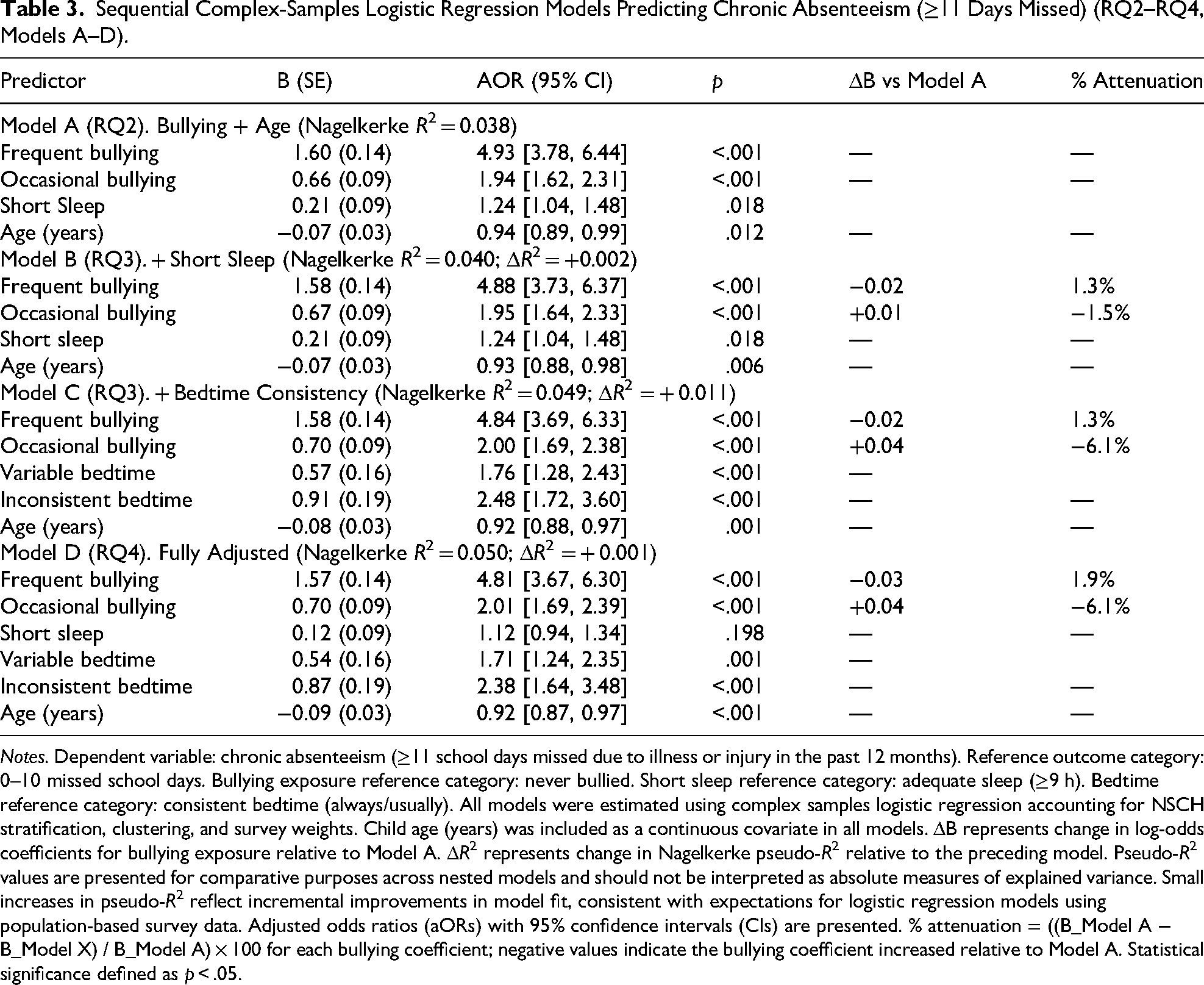
Notes. Dependent variable: chronic absenteeism (≥11 school days missed due to illness or injury in the past 12 months). Reference outcome category: 0–10 missed school days. Bullying exposure reference category: never bullied. Short sleep reference category: adequate sleep (≥9 h). Bedtime reference category: consistent bedtime (always/usually). All models were estimated using complex samples logistic regression accounting for NSCH stratification, clustering, and survey weights. Child age (years) was included as a continuous covariate in all models. ΔB represents change in log-odds coefficients for bullying exposure relative to Model A. ΔR2 represents change in Nagelkerke pseudo-R2 relative to the preceding model. Pseudo-R2 values are presented for comparative purposes across nested models and should not be interpreted as absolute measures of explained variance. Small increases in pseudo-R2 reflect incremental improvements in model fit, consistent with expectations for logistic regression models using population-based survey data. Adjusted odds ratios (aORs) with 95% confidence intervals (CIs) are presented. % attenuation = ((B_Model A − B_Model X) / B_Model A) × 100 for each bullying coefficient; negative values indicate the bullying coefficient increased relative to Model A. Statistical significance defined as p < .05.
Sequential adjustment for short sleep and bedtime consistency resulted in minimal changes in the magnitude of the bullying–absenteeism association. For frequent bullying, the log-odds coefficient decreased from 1.60 to 1.57, corresponding to 1.9% change after inclusion of both sleep indicators. In contrast, the coefficient for occasional bullying increased from 0.66 to 0.70 across models. The addition of short sleep (Model B) resulted in a small increase in model explanatory power (Nagelkerke R2: 0.038–0.040), corresponding to a minimal change in the bullying coefficient (ΔB ≈ 0.02). In contrast, inclusion of bedtime consistency (Model C) produced a larger increase in model explanatory power (Nagelkerke R2: 0.038–0.049), corresponding to an approximate 29% relative increase in explanatory value, although absolute values remained small as expected in logistic regression models. Consistent with the recommended interpretation of pseudo-R2 statistics, these changes were evaluated in relation to shifts in model coefficients and overall pattern of results rather than against fixed thresholds for magnitude. In the fully adjusted model (Model D), explanatory power increased slightly further (Nagelkerke R2 = 0.050), indicating incremental improvement in model fit. Overall, attenuation of bullying coefficients remained minimal across all models, indicating that sleep characteristics explain only a small proportion of the association between bullying exposure and chronic absenteeism.
Discussion
This study examined associations between bullying exposure, sleep characteristics, and school absenteeism among U.S. children ages 6–11 years using pooled, nationally representative data. Fully adjusted models indicated that bedtime consistency remained independently associated with chronic absenteeism after accounting for bullying exposure and age, such that children with variable or inconsistent bedtimes had higher odds of chronic absenteeism compared with children with consistent bedtimes. Short sleep did not retain an independent association with chronic absenteeism after inclusion of bedtime consistency, suggesting that bedtime regularity may represent the more proximal sleep-related correlate of chronic absenteeism in this age group. Bullying exposure remained associated with chronic absenteeism across all model specifications.
Interpretation of racial and ethnic patterns in bullying exposure warrants caution. The descriptive percentages presented in the current study reflect the distribution of bullying exposure across the overall sample rather than within-group prevalence estimates. Because racial and ethnic groups differ substantially in size within the NSCH sample, these values primarily reflect group composition rather than differences in risk. As such, the present findings do not permit conclusions regarding disparities in bullying exposure across racial or ethnic groups. Future research should examine within-group prevalence and adjusted models to better characterize potential differences in bullying exposure across demographic subgroups.
Bullying, Short Sleep, and Bedtime Consistency
In regard to RQ1, findings indicated that bullying exposure was associated with both short sleep and bedtime consistency, and that bedtime consistency was strongly associated with short sleep duration. The graded association between bedtime consistency and short sleep suggests that increasing irregularity in sleep routines corresponds to progressively higher likelihood of insufficient sleep. These findings are consistent with prior research indicating that regular sleep routines represent a key upstream correlate of sleep duration in children (Table 2).
Bullying and Chronic School Absenteeism
In response to RQ2 (Table 2), bullying exposure demonstrated a strong and consistent association with chronic school absenteeism. Children experiencing occasional bullying, and particularly frequent bullying, had substantially higher odds of missing 11 or more school days in the past year compared with children who were never bullied, even after adjustment for age. The magnitude of this association exceeded that observed for sleep characteristics, indicating that bullying represents a salient and independently associated factor for chronic absenteeism during middle childhood. These findings are consistent with prior literature linking bullying exposure to somatic complaints, emotional distress, and school avoidance behaviors (Farrington & Baldry, 2010; Fekkes et al., 2004; Moore et al., 2017). Subsequently, chronic absenteeism represents a functional outcome that may reflect both physical symptoms and psychosocial distress. From a population health perspective, the strength and consistency of this association suggest that bullying exposure may serve as an important upstream correlate of sustained attendance disruption.
Sleep Characteristics and Chronic Absenteeism Risk
Addressing RQ3 (Table 3), short sleep and bedtime consistency were each associated with higher odds of chronic absenteeism in sequential models. However, in the fully adjusted model, bedtime consistency retained an independent association with chronic absenteeism, whereas short sleep was attenuated and no longer statistically significant after accounting for bedtime consistency. This pattern suggests that bedtime regularity may represent a more proximal sleep-related correlate of illness- or injury-related absenteeism than sleep duration alone (Dewald et al., 2010; Dahl, 1996).
Although sleep variables improved model explanatory power modestly and were independently associated with absenteeism, inclusion of sleep indicators did not substantively diminish the magnitude of the bullying exposure and absenteeism association on the log-odds scale. In practical terms, sleep-focused strategies alone are unlikely to offset the attendance-related consequences associated with bullying exposure, although addressing sleep routines may support overall functioning and complement broader prevention and attendance efforts (Blunden & Rigney, 2015; Dewald et al., 2010). These findings from Models B–C indicate that bedtime consistency, rather than sleep duration alone, may represent the more proximal sleep-related correlate of chronic absenteeism in this age group.
Sleep as an Explanatory Factor
In terms of RQ4 (Table 3), sequential models (Models A–D) indicated that inclusion of sleep characteristics added modest explanatory value, but attenuation of the bullying–absenteeism association was minimal. For frequent bullying, inclusion of both sleep indicators was associated with approximately 1.9% attenuation of the bullying coefficient. The persistence of a strong bullying association across all models suggests that bullying exposure may relate to chronic absenteeism through multiple mechanisms beyond sleep, including somatic complaints, psychological distress, fear-based school avoidance, and caregiver decisions related to health and safety (Fekkes et al., 2004; Moore et al., 2017).
Implications for Intervention and Policy
The present findings build on literature demonstrating that bullying exposure in middle childhood is associated with adverse health and educational outcomes, reinforcing bullying as a consequential form of interpersonal violence rather than a normative developmental experience (Arseneault, 2018; Moore et al., 2017). While prior studies have linked bullying victimization to emotional distress, somatic complaints, and academic disengagement, fewer population-based investigations have examined sleep behaviors alongside school attendance outcomes among younger children (Fekkes et al., 2004; Levková et al., 2025). By integrating sleep duration and bedtime consistency into a design-based analytic framework, the current study identifies a practical and potentially modifiable behavioral correlate, namely bedtime regularity, that is independently associated with absenteeism risk (El-Sheikh & Kelly, 2017; van Geel et al., 2016).
From a policy perspective, these findings support a complementary approach to bullying prevention and response. Established school-based antibullying interventions remain essential given the strength and persistence of the bullying exposure association with chronic absenteeism (Freeman et al., 2015). At the same time, adjunctive strategies that promote consistent bedtime routines may be feasible to integrate into student support services and parent engagement initiatives (Mindell & Williamson, 2018; Kearney & Graczyk, 2014). At the public health level, the findings reinforce the importance of integrated approaches to child well-being that transcend traditional silos (Dewald et al., 2010). Bullying, sleep, and school attendance are often addressed independently despite likely interconnections. Pediatric and school-based health providers may consider routine assessment of bedtime regularity when evaluating children presenting with bullying exposure, frequent illness-related absences, or school avoidance (Blunden & Rigney, 2015).
Implications for School Nursing Practice
School nurses are well positioned to identify students experiencing bullying and to assess sleep duration and bedtime regularity during routine health encounters. Given the robust association between bullying exposure and chronic absenteeism, routine screening for bullying among students with repeated absences is likely warranted. In practice, this may include integrating brief, structured screening questions related to peer victimization and sleep behaviors into existing health assessments, particularly for students presenting with frequent visits, fatigue, or attendance concerns (National Association of School Nurses, 2021).
Findings also indicate that variable or inconsistent bedtimes, rather than short sleep duration alone, were independently associated with absenteeism risk. Incorporating brief sleep hygiene counseling and caregiver education focused on consistent bedtime routines may represent a feasible adjunct to existing bullying response protocols and tiered student support services and may support student functioning in the context of comprehensive violence prevention and attendance interventions (Dewald et al., 2010; Kearney & Graczyk, 2014). School nurses can reinforce the importance of consistent sleep routines through developmentally appropriate education for students and caregivers, emphasizing regular bedtimes, reduced evening screen exposure, and alignment with school schedules (Williamson, Mindell, Hiscock & Quach, 2019).
These findings also support the integration of sleep health into multi-tiered systems of support, where school nurses contribute to Tier 1 universal education, Tier 2 targeted interventions for at-risk students (e.g., those experiencing bullying or attendance problems), and Tier 3 individualized care coordination (National Center on Intensive Intervention, 2020; National Association of School Nurses, 2021). In collaboration with school counselors, psychologists, and administrators, school nurses may play a central role in identifying students at risk for absenteeism and facilitating referrals to appropriate behavioral health or family support services (Centers for Disease Control and Prevention, 2021). At a systems level, incorporating sleep-related indicators into school health surveillance and attendance monitoring processes may enhance early identification of students experiencing compounding risks related to bullying and sleep disruption (Centers for Disease Control and Prevention, 2021). Together, these approaches position school nurses as key contributors to interdisciplinary efforts aimed at improving student well-being, school engagement, and attendance outcomes.
Limitations and Future Directions
Several limitations warrant consideration. First, the cross-sectional design precludes causal inference and limits conclusions regarding temporal ordering among bullying exposure, sleep characteristics, and absenteeism. Accordingly, findings should be interpreted as associative rather than causal. Future longitudinal studies are needed to clarify directionality and evaluate whether improvements in bedtime routines prospectively reduce absenteeism risk among children exposed to bullying. Second, all measures were caregiver-reported and therefore subject to recall and reporting bias. Reliance on a single informant may not fully capture children's experiences across settings. In addition, bullying exposure was assessed using a frequency-based item that did not capture bullying type, duration, or context. Future research should examine whether specific forms of bullying, including online versus in-person victimization, demonstrate differential associations with sleep and attendance outcomes (Levková et al., 2025; van Geel et al., 2016).
Third, although the large NSCH sample increases statistical power such that small differences may achieve statistical significance, interpretation emphasized effect sizes and practical relevance rather than p-values alone. Sleep indicators accounted for only a small proportion of the bullying–absenteeism association, suggesting that additional mechanisms, including mental health symptoms, school climate, and family context, warrant further investigation (VanderWeele, 2015). Finally, descriptive racial and ethnic comparisons reflected distributions within the overall sample rather than within-group prevalence estimates and therefore should not be interpreted as disparities in bullying exposure. In addition, findings may not generalize to adolescents, whose sleep regulation, peer dynamics, and school engagement differ developmentally from middle childhood. Future studies should evaluate these associations across broader developmental stages.
Conclusions
This study provides nationally representative evidence that bullying exposure in middle childhood is associated with short sleep and increased chronic school absenteeism, and that bedtime consistency is independently associated with absenteeism risk after accounting for bullying exposure and age. Although inclusion of sleep indicators minimally attenuated the bullying exposure association, bedtime regularity represents a feasible adjunctive target that may support student functioning when implemented alongside established bullying prevention and attendance interventions.
Supplemental Material
sj-docx-1-jsn-10.1177_10598405261455901 - Supplemental material for Bullying Exposure, Sleep Duration, Bedtime Consistency, and Chronic School Absenteeism Among U.S. Children Ages 6–11 Years
Supplemental material, sj-docx-1-jsn-10.1177_10598405261455901 for Bullying Exposure, Sleep Duration, Bedtime Consistency, and Chronic School Absenteeism Among U.S. Children Ages 6–11 Years by Adam P. Knowlden and Sarah M. Flora in The Journal of School Nursing
Supplemental Material
sj-docx-2-jsn-10.1177_10598405261455901 - Supplemental material for Bullying Exposure, Sleep Duration, Bedtime Consistency, and Chronic School Absenteeism Among U.S. Children Ages 6–11 Years
Supplemental material, sj-docx-2-jsn-10.1177_10598405261455901 for Bullying Exposure, Sleep Duration, Bedtime Consistency, and Chronic School Absenteeism Among U.S. Children Ages 6–11 Years by Adam P. Knowlden and Sarah M. Flora in The Journal of School Nursing
Footnotes
Acknowledgments
The authors acknowledge the U.S. Census Bureau for the collection and dissemination of the National Survey of Children's Health, which made this analysis possible.
Authors’ Note
Declaration of AI-Assisted Technologies: During manuscript preparation, the primary author used ChatGPT to assist with language refinement and formatting in accordance with journal guidelines. All content was reviewed and verified by the author, who assumes full responsibility for the final manuscript.
Author Contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Heart, Lung, & Blood Institute, National Institutes of Health, Bethesda, MD, Grant/Award Number: K01HL145128.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Institutional Board Approval
This study was determined to be nonhuman subject research by The University of Alabama Institutional Review Board (IRB # 26-02-9399) and was exempted from review due to the lack of identifying information in the National Survey on Children's Health public use data set.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.