
Abstract
Schools increasingly face complex medical emergencies, underscoring the need for coordinated, school-based response systems. School nurses are well positioned to lead Medical Emergency Response Teams (MERTs), yet implementation of coordinated medical emergency response in schools can be constrained by contextual and organizational challenges. We examined the effectiveness of a train-the-trainer program designed to build school nurses’ capacity to lead and implement MERTs. Using a mixed-methods design, participants (n = 335) completed a retrospective pre/post-survey immediately after training to assess knowledge across core MERT concepts and a 6-month follow-up survey to examine application in practice. Significant increases in self-reported knowledge were observed across all domains (P < 0.05) and were maintained at 6 months post-training. Follow-up findings indicated active implementation, including MERT formation, staff training, and use of response plans during medical emergencies. Findings demonstrate that professional development can produce sustained improvements in school nurse leadership and medical emergency preparedness.
Keywords
Introduction
Current approaches to emergency preparedness for schools encompass a broad range of threats, including natural hazards, mass violence, public health crises, and complex medical emergencies (National Association of School Nurses (NASN), 2024a; Centers for Disease Control and Prevention (CDC), 2024a). This multi-hazard approach to risk assessment and crisis management recognizes schools as settings where both security-related and health-related emergencies are increasingly likely to occur (CDC, 2024a; NASN, 2024a). Despite progress in school emergency planning, gaps in preparedness remain, particularly in school nurses’ ability to prepare their school environments to respond to medical emergencies (Boudreaux & Broussard, 2020; Murata et al., 2020; Ugalde et al., 2018). The current study seeks to evaluate the efficacy of a training program, SCHOOL NURSES: Enhance Effective Medical Emergency Teams at Each of Your School Sites, in preparing school nurses to lead coordinated support for medical emergencies that occur in the school.
Current Approaches to Emergency Management in Schools
According to the National Association of School Nurses (NASN, 2024a), effective school emergency preparedness requires a collaborative, systems-thinking approach to comprehensive planning and response. This approach includes conducting risk and vulnerability assessments, providing regular staff training, ensuring efficient communication, supporting psychosocial health, and developing emergency plans. Emergency plans should follow an all-hazards framework to address a wide range of incidents, including natural disasters, weather-related emergencies, disease outbreaks, food allergy emergencies, medical emergencies, and acts of violence. NASN further emphasizes that emergency preparedness must encompass all phases of emergencies (e.g., prevention, protection, mitigation, response, and recovery) and remain an ongoing process of coordination, training, and evaluation.
Guidelines for emergency medical care in schools emphasize that schools must anticipate and be prepared to respond to a broad array of medical, behavioral, and traumatic emergencies (Gereige et al., 2022). A review of data using the National Emergency Medical Services (EMS) Information System, a nationally representative dataset of EMS encounters, indicate that between 2018 and 2022, over 500,000 EMS calls originated from school settings, representing 11.3% of all pediatric EMS scene responses during that period, with nearly 70% resulting in hospital transport (Harries et al., 2025). The most common emergencies involved neurologic conditions, psychiatric or substance-use crises, and trauma-related injuries (Harries et al., 2025). The most frequently required interventions included cardiac assessment and vascular access and the most frequently administered medications were analgesics, albuterol, and antiseizure agents (Harries et al., 2025).
In response to the growing complexity of health-related emergencies in schools, various organizations—including the American Heart Association (AHA), the Epilepsy Foundation, and the Allergy and Asthma Network—have advocated for comprehensive emergency response preparedness addressing conditions such as sudden cardiac arrest, seizures, asthma emergencies, and anaphylaxis (AHA, 2023; Allergy & Asthma Network, n.d.; Epilepsy Foundation, 2021). Laws in 25 states require Automated External Defibrillator (AED) placement in schools, and 49 states allow schools to maintain emergency supplies of epinephrine, of which 10 states legally require it (Asthma & Allergy Foundation of America, 2025; CDC, 2024b). These statutes often mandate training for anticipated responders, including school nurses, educators, and coaches (CDC, 2018). Additionally, national and state guidelines have been developed to support timely and appropriate emergency response and medication administration, aiming to create safer school environments through standardized readiness protocols (Food Allergy Research & Education (FARE), n.d.).
To operationalize emergency planning, schools must first establish a planning team to develop a common framework for emergency response (U.S. Department of Education, 2013). School nurses, with their specialized training and knowledge, are ideally positioned to lead these efforts, coordinating with administrators, staff, and community partners to define roles, schedule regular meetings, and ensure ongoing readiness through training and practice drills (NASN, 2024a). A Medical Emergency Response Team (MERT) is a designated group of trained school personnel responsible for providing an organized and coordinated response to medical emergencies in the school setting, as clearly described in one school program (Bittenbender et al., 2009). By leading a MERT, school nurses ensure that response efforts are clinically sound, efficiently coordinated, and integrated into broader school emergency preparedness strategies.
Despite their central role in school health and safety, school nurses’ ability to prepare their school environment for medical emergencies varies due to factors such as financial limitations, lack of information or assistance, low staff participation, and resistance or apprehension from staff (Boudreaux & Broussard, 2020; Murata et al., 2020). Confidence is also influenced by the availability of practice opportunities—nurses in schools without emergency medical plans or where plans were infrequently practiced reported lower confidence in managing emergencies (Ugalde et al., 2018). In contrast, participation in emergency exercises has been shown to improve knowledge, competence, and confidence in responding to health emergencies (Skryabina et al., 2017). Targeted professional development has been shown to improve school nurses’ ability to lead comprehensive emergency preparedness and management of medical emergencies, including asthma attacks, anaphylaxis, seizures, and cardiac events (Chokshi et al., 2015; Elizalde et al., 2024; Latuska et al., 2019; Mattheus et al., 2023). Overall, emergency preparedness activities can contribute to readiness in the immediate and short-term timeframe, but evidence of long-term benefits is limited (Skryabina et al., 2017).
The Current Study
To address the limited evidence on the long-term impact of emergency preparedness activities, we examined a professional development program designed to strengthen school nurses’ ability to establish and lead MERTs. The program, SCHOOL NURSES: Enhance Effective Medical Emergency Teams at Each of Your School Sites, is a train-the-trainer opportunity offered nationwide to equip school nurses with the tools needed to advocate for and implement a MERT plan. The curriculum includes standardized protocols to facilitate effective responses to medical emergencies commonly encountered in schools, such as asthma attacks, anaphylaxis, seizures, and cardiac events. Mental health crises, which are typically addressed by schools’ behavioral health teams, were not included in the training; however, MERT protocols are implemented if these situations escalate to a medical emergency. Virtual resources support the training by guiding application of training concepts, such as securing school and district support, developing response plans for common medical emergencies, providing comprehensive and efficient training for MERT members, and collecting feedback from team members after an emergency response. We evaluated training effectiveness by assessing school nurses’ knowledge of MERT concepts immediately after participation in the training and their application of these skills to support MERT implementation 6 months later. This approach aligns with recommendations that evaluations extend beyond knowledge acquisition to examine whether learning translates into practice change (Bergren, 2023). We hypothesized that the training program would enhance school nurses’ knowledge of MERT concepts immediately following training and that they would apply the knowledge gained to support MERT implementation 6 months after participation.
Methods
We utilized a mixed-methods design to measure participants’ knowledge and execution of MERT activities, and gain deeper insights into perceived barriers, facilitators, and planned practice changes. Quantitative and qualitative data were analyzed separately and then integrated during interpretation to provide a comprehensive understanding of training outcomes. The evaluation protocol was reviewed by the Henry Ford Health Institutional Review Board and was determined to be exempt from full review and oversight. Data were collected anonymously and stored on a secure, password-protected computer accessible only to the evaluation lead.
Intervention
The MERT training consisted of a synchronous virtual professional development session designed to strengthen school nurses’ capacity to develop, implement, and lead MERTs within their schools. Each session was delivered live via Zoom by an experienced certified school nurse trainer who used a structured agenda and presentation to present information on jurisdiction-specific laws that affect school health, the role of the school nurse in emergency planning, the needs of students with chronic health conditions, and importance of MERTs and specific MERT actions to include in trainings. Each training session lasted approximately 6 hours and incorporated brief case examples, opportunities for participant interaction, and a demonstration of the practical resources available to participants in the program's digital binder to support application of the learning content. Between January 2024 and February 2025, 11 virtual training sessions were held with a total of 335 school professionals across the United States.
Procedures
At the beginning of each training session, participants were invited to complete a brief voluntary quiz to provide descriptive information about their professional roles and school settings. At the end of each session, the training facilitator provided participants with an online survey link through the Zoom chat feature and asked participants to complete the voluntary survey. All individuals who completed the virtual trainings were invited to participate, representing a convenience sample. At the end of the survey, participants were asked whether they agreed to be contacted for a follow-up survey. Only individuals who agreed were subsequently invited to complete the follow-up survey.
Participants
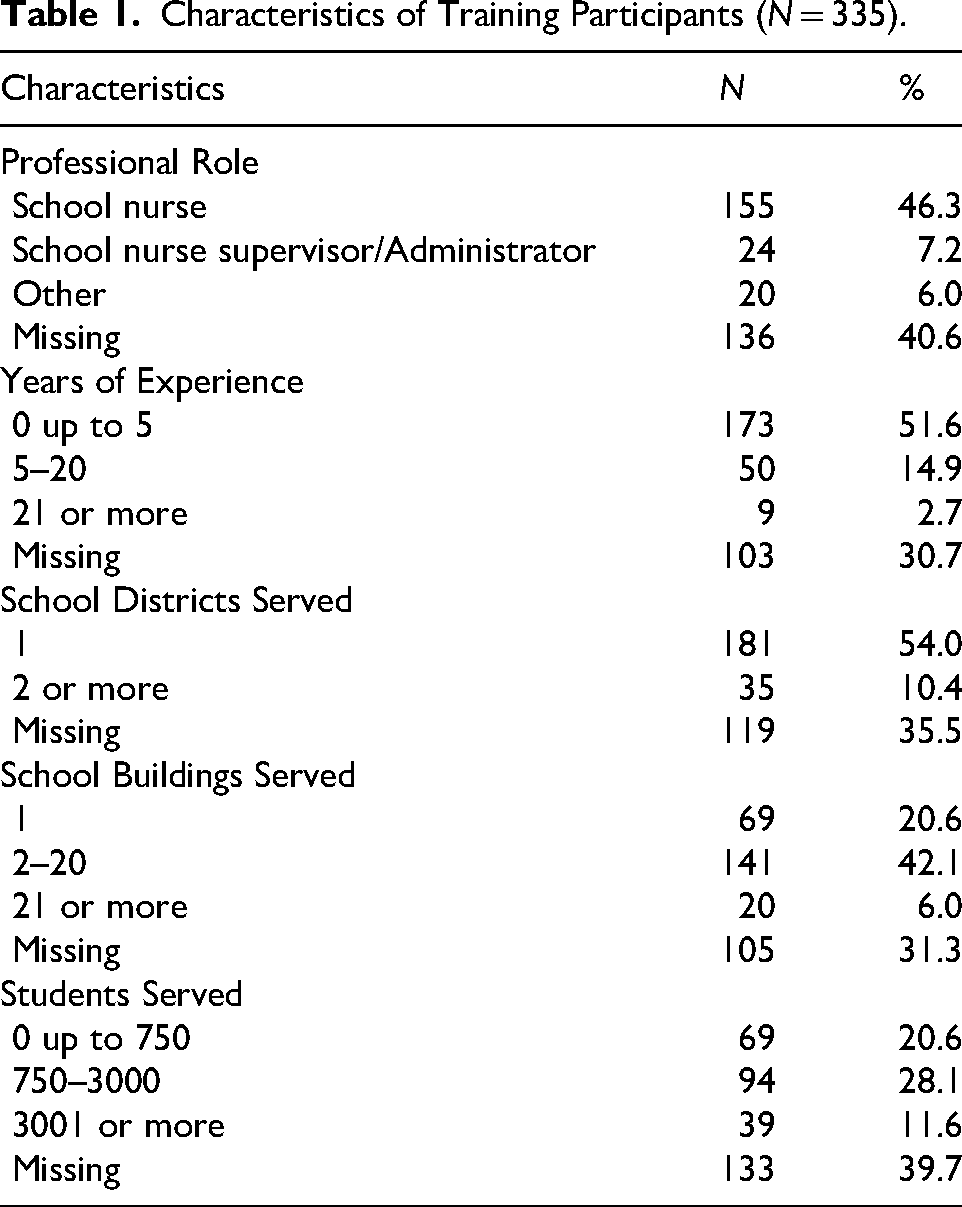
As shown in Table 1, 46.3% of participants were school nurses and 7.2% were school nurse supervisors or administrators. Among participants, 51.6% had fewer than 5 years of experience in their role and 14.9% had between 5 to 20 years of experience. More than half (54.0%) reported serving one school district, and 42.1% reported serving between 2 and 20 school buildings. Nearly half of participants (48.7%) reported serving up to 3,000 students, and 11.6% reported serving more than 3,000 students.
Characteristics of Training Participants (N = 335).
Measures
The NASN School Nursing Practice Framework provides an overarching structure that incorporates concepts integral to school nursing and emphasizes student-centered activities that support student health and safety (NASN, 2024b). It combines Standards of Practice with four overlapping practice principles: Care Coordination, Leadership, Quality Improvement, and Community/Public Health (NASN, 2024b). The framework was used to guide the selection of knowledge areas assessed in the surveys to ensure that outcomes were relevant to professional school nursing practice. Specifically, knowledge of the main components of an effective MERT and securing school or district support reflects the principles of Leadership and Care Coordination; knowledge of the school nurse's role in emergency response aligns with Leadership and Community/Public Health; providing training and drills for MERT members corresponds to Leadership and Quality Improvement; and collecting input from MERT members after an emergency response reflects Care Coordination and Quality Improvement.
Getting to Know You Quiz
At the beginning of each training session, we invited the 335 participants to complete a voluntary “Getting to Know You” quiz administered through the Kahoot platform to gather descriptive information about participants’ professional roles and work contexts, including years of experience and number of school districts, buildings, and students served.
Retrospective Pre/Post-Training Survey
At the end of each training session, a survey link, administered through SurveyMonkey, was provided to all 335 participants through the Zoom chat platform. We used a retrospective pre/post format where participants rated their knowledge before and after the training on the same items. This approach was selected because it is a valid method for measuring self-reported change and can reduce response-shift bias, allowing participants to more accurately assess their pre-training knowledge after gaining a clearer understanding of the content (Pratt et al. 2000). Ratings were based on a 5-point Likert scale (1 = not at all knowledgeable, 5 = extremely knowledgeable) across five core MERT domains: (1) the main components of an effective MERT, (2) the role of the school nurse in emergency response at school, (3) securing school and district support for a MERT, (4) providing training and drills for MERT members, and (5) collecting input from MERT members after an emergency response. Knowledge was assessed via self-report and no formal testing of knowledge or practical skills was conducted. In addition to the knowledge assessment, two open-ended questions were used to collect information on intended practice changes as a result of the training and anticipated barriers to using the training content. The survey was developed explicitly for this training and was not formally tested for reliability or validity.
6-Month Follow-Up Survey
Six months after training completion, the 66 participants who agreed to be contacted for follow-up were emailed a survey link via SurveyMonkey. We asked participants to rate their current knowledge on the same 5-point Likert scale across four core MERT domains (1) securing school and district support for a MERT, (2) creating a response plan for common medical emergencies, (3) providing training and drills for MERT members, and (4) collecting input from MERT members after an emergency response. Participants were asked to report the extent to which they applied what they learned and to identify factors that facilitated its use. Participants were also asked to respond to a series of yes/no questions regarding MERT implementation, including whether they formed a MERT and developed a medical emergency response plan, conducted at least one training session for MERT members, completed at least one emergency drill, and responded to an actual medical emergency in their school. No formal testing of knowledge or practical skills was conducted and the survey was not formally tested for reliability or validity.
Analyses
We imported survey responses from SurveyMonkey into IBM SPSS Statistics (version 30.0) for data cleaning and analysis. Descriptive statistics were used to summarize attendance and implementation outcomes post-training and at follow-up. We compared retrospective pre/post knowledge ratings using the Wilcoxon signed-rank test, a non-parametric test appropriate for paired ordinal data. This test was used to assess statistically significant changes in participants’ self-reported knowledge across the core MERT domains. Statistical significance was set at p < 0.05. Effect sizes were calculated by dividing the standardized test statistic (Z value) by the square root of the sample size.
We analyzed responses to open-ended questions using inductive thematic analysis. Responses were reviewed and coded manually in Microsoft Excel. An initial coding framework was developed through open coding of a sample of responses, and codes were refined through iterative review. Responses were analyzed to identify themes in the following areas: intended practices and perceived barriers to implementation. An initial set of codes was developed by one member of the evaluation team, then refined through discussion and consensus with a second reviewer.
Results
Survey Response
Figure 1 presents participants’ response to post-training and follow-up surveys. Of the 335 training attendees invited to participate after each training, 178 (53.1%) completed the retrospective pre/post-survey. Among the 178 respondents, 66 (37%) agreed to be contacted for a 6-month follow-up survey. All 66 individuals were emailed a follow-up survey, and 10 (15.2%) completed the follow-up survey.
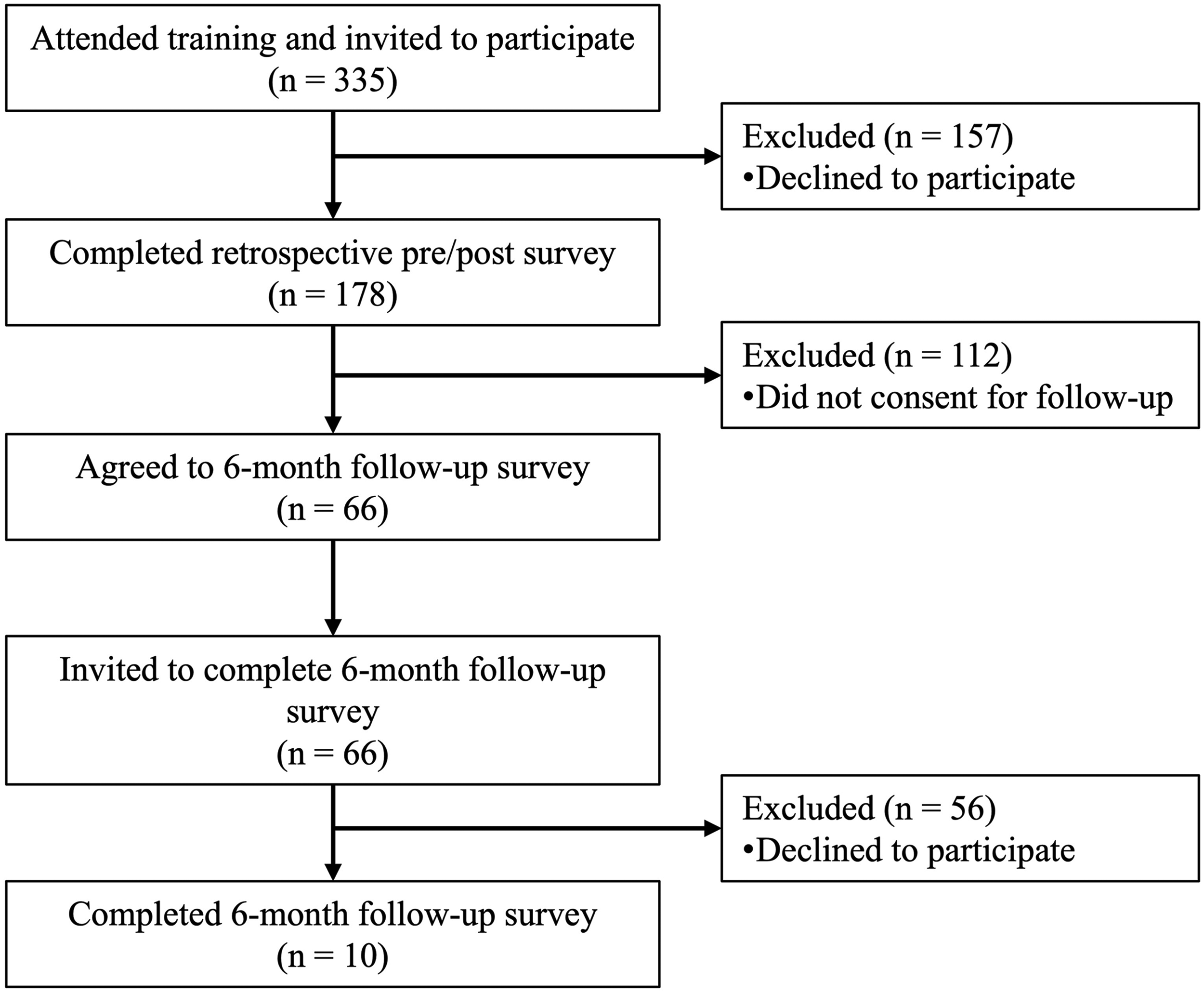
Participant survey response.
Post-Training Knowledge
Participants reported increased knowledge across all five MERT domains (Table 2). For example, knowledge of the main components of an effective MERT increased from 29.2% before training to 86.5% after training, and the knowledge of the role of the school nurse in emergency responses increased from 48.0% to 91.0%. Similar improvements were observed across the other domains, demonstrating a consistent pattern of knowledge gain post-training.
Participant Knowledge Ratings Before and After MERT Training (n = 178).
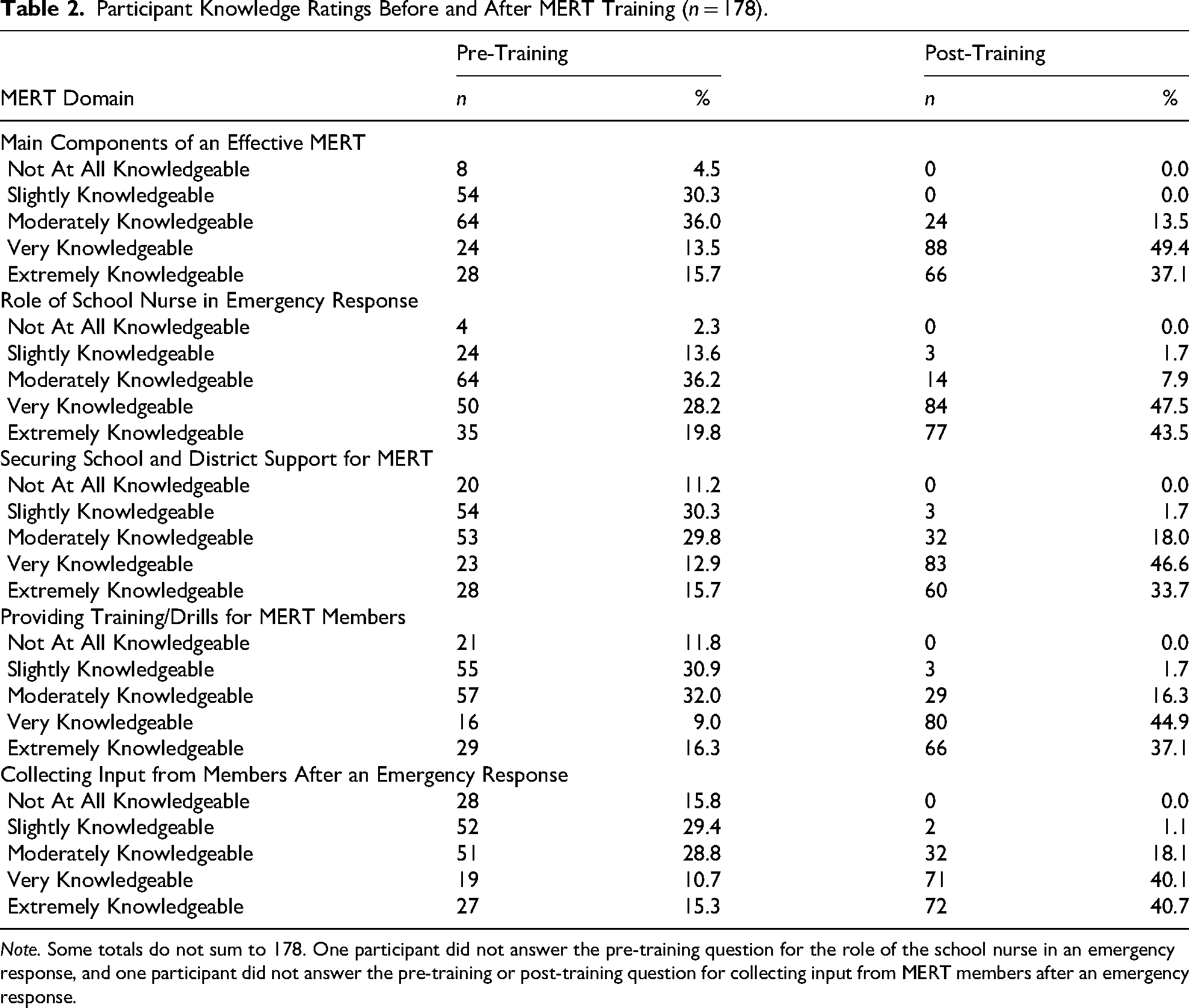
Note. Some totals do not sum to 178. One participant did not answer the pre-training question for the role of the school nurse in an emergency response, and one participant did not answer the pre-training or post-training question for collecting input from MERT members after an emergency response.
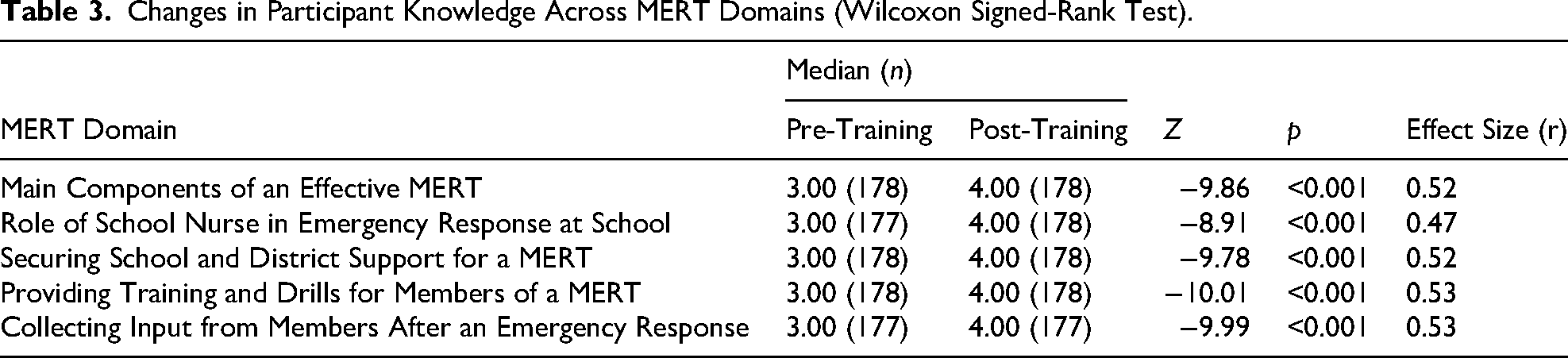
To further assess changes in self-reported knowledge before and after the training, Wilcoxon Signed-Rank tests were conducted for each domain. The results indicated statistically significant increases in median scores in all MERT domains (Table 3). Median pre-training scores for all domains were 3.00 (“moderately knowledgeable”), which increased to 4.00 (“very knowledgeable”) post-training. Effect sizes ranged from 0.47 to 0.53, indicating moderate to large effects.
Changes in Participant Knowledge Across MERT Domains (Wilcoxon Signed-Rank Test).
Intended Practice Change
Of the 178 survey respondents, 157 (88.2%) indicated at least one new practice they will attempt to implement as a result of the training. Six themes were identified: formation or expansion of MERT teams (n = 49 respondents who made comments that pertained to a theme); conducting or improving training and drills (n = 48); having emergency action plans in place (n = 20); garnering administrative or district support (n = 15); improving communication during and after medical emergencies (n = 15); and assigning and clarifying roles within MERTs (n = 13).
Formation or Expansion of MERT Teams
Participants described plans to establish new MERTs or expand existing ones. Many were motivated by the training to take concrete steps and referenced using the resources and organizational tools provided. For example, participants shared: “Since my district does not have a MERT, I plan on implementing one and ensuring [we conduct] a debrief at the end,” and “We don’t have a MERT currently. I am very excited to implement this in my school! Our processes will be much smoother, and our staff will feel more supported in emergencies.”
Conducting or Enhancing Training and Drills
Participants expressed interest in implementing or enhancing training and emergency drills, including conducting tabletop exercises, involving EMS, and increasing drill frequency. Participants shared examples such as: “I will coordinate with our professional development team to insist that we secure time for MERT training on in-service/professional development days,” and “I will be using the presentations for all staff, and I will also be implementing more MERT trainings regarding different health conditions in my district.”
Developing or Maintaining Emergency Action Plans
Many participants recognized the need for structured, accessible emergency response plans, including documenting procedures, creating and posting safety maps, and ensuring emergency medications are readily available. Participants also mentioned aligning plans with state and local guidelines to ensure consistent and effective response. For example, participants noted: “[I will] talk to our admin regarding the need for emergency response teams and putting up emergency maps/school information with addresses around the building,” and “Meeting with admin to see if they already have a plan in place. At this time, I don’t know.”
Garnering Administrative or District Support
Participants noted that administrative or district-level buy-in was essential for establishing and sustaining MERTs. They described plans to schedule meetings, present the program to leadership, and communicate the need and importance of MERTs within their schools. For example, one participant stated: “I will work with my administrators to discuss the importance of MERT and work to get it started in my district.”
Improving Communication During and After Emergency Responses
Participants described plans to enhance internal communication protocols. This included creating more comprehensive communication plans, incorporating portable two-way radios, and holding debriefing meetings after an emergency response. One participant noted: “[I plan to] implement a scheduled meeting with the MERT team, including debriefing meetings.”
Assigning and Clarifying Roles Within MERTs
Participants highlighted the need for documented responsibilities during medical emergencies and emphasized the importance of defining and assigning roles within the MERT. One participant shared: “We have had good general ideas about what should be happening in the event of emergencies, but the lines of who is doing what, particularly the non-medical care elements, are blurry, and I’m excited to firm them up.”
Perceived Barriers to Implementation
Of the 178 survey respondents, 150 (84.3%) indicated at least one factor they believed might impede their ability to apply the training content. Four themes were identified: lack of administrative support (n = 24); limited time (n = 24); limited interest or engagement from staff (n = 12); and limited capacity (n = 9).
Lack of Administrative Support
Participants expressed concern that school or district leadership might resist establishing MERTs or be unable to prioritize MERT development due to competing demands. For example, participants stated: “I am somewhat apprehensive getting the buy-in I need from building and district administration and the teachers” and “The hardest part is having the support at my school from the administration staff.”
Limited Time
Participants noted time constraints, including accessing busy team members, finding time for training, and building time into their own schedules to develop plans and implement changes. One participant noted: “Time constraints, availability of professional development time or time set aside for such training.” Another added: “Time constraints presented during the regular school day due to student needs.”
Limited Interest or Engagement from Staff
Participants expressed concerns of low participation from staff due to lack of interest or availability. For example, one participant stated: “Possibly the buy-in for staff that is already stretched thin with responsibilities.”
Limited Capacity
Participants cited personal limitations, such as feeling overwhelmed or uncomfortable leading the effort, while others mentioned organizational limitations, such as limited resources or a lack of staff able to lead trainings. One participant shared: “I am only one person. Given the daily grind of hands-on-provision of care to students, getting my head above water to pull this content together, establish a team, and train said team is daunting.”
Implementation at Follow-up
Six months after training completion, the ten participants who completed a survey reported a sustained knowledge across MERT domains. For securing school and district support for MERTs, two participants (20.0%) rated themselves as moderately knowledgeable, three (30.0%) as very knowledgeable, and five (50.0%) as extremely knowledgeable. For providing training and drills for MERT members, four participants (40.0%) rated themselves as moderately knowledgeable, five (50.0%) as very knowledgeable, and one (10.0%) as extremely knowledgeable. For creating response plans for common medical emergencies, one participant (10.0%) rated themselves as moderately knowledgeable, four (40.0%) as very knowledgeable, and five (50.0%) as extremely knowledgeable. For collecting input from members after an emergency response, six participants (75.0%) rated themselves as very knowledgeable and two (25.0%) as extremely knowledgeable. No participants reported having no knowledge or being slightly knowledgeable in any domain.
All ten participants reported using what they learned from the training. Eight participants (80.0%) indicated they applied the content to a great extent and two participants (20.0%) reported using it to some extent. When asked what factors facilitated application of the training content, seven participants (70.0%) reported having the necessary resources and opportunities to use what they learned. Six participants (60.0%) indicated having support from their supervisor, and five participants (50.0%) noted support from colleagues, reminders of key learning concepts or skills, and having time to apply what they learned. During the 6 months following training, seven participants (70.0%) assembled a MERT and corresponding response plan in at least one school site. Four participants (40.0%) provided at least one training for MERT members, and one participant (10.0%) conducted at least one drill. Four participants reported experiencing an incident that required an emergency response. Of these participants, three did not yet have a MERT in place, and one did. The participant with an established MERT reported that the MERT process was successfully utilized during the incident.
Discussion
The evaluation demonstrates that a specialized training program for school nurses can improve knowledge of MERT development and implementation. Training outcomes indicate strong immediate knowledge acquisition across MERT domains, particularly in areas where baseline knowledge was lower, suggesting that the intervention effectively targeted gaps in emergency preparedness competencies. These results reflect growth in competencies aligned with the NASN School Nursing Practice Framework, which are central to effective emergency preparedness and response in school settings. These findings also support prior research showing that specialized or skills-based training improves school nurses’ knowledge, confidence, and preparation for managing health emergencies (Chokshi et al., 2015; Elizalde et al., 2024; Latuska et al., 2019; Mattheus et al., 2023).
Qualitative findings further illustrate the practical value of the training. Participants’ intended practice changes suggest early-stage movement toward implementation of structured emergency preparedness systems in school settings, particularly in areas of coordination, planning, and role clarification. Importantly, these behaviors align with framework principles emphasizing Leadership, Care Coordination, and Quality Improvement, suggesting that training may support not only knowledge acquisition but also readiness for organizational change in school emergency response systems. These intended changes are consistent with prior studies demonstrating that structured training programs can prompt improvements in school-based emergency practice and readiness. For example, previous research has shown increased competency in asthma assessment following skills-based training (Francisco et al., 2017), improved ability to respond to life-threatening bleeding emergencies (Latuska et al., 2019), and increased availability of emergency medications in schools (Chokshi et al., 2015). Similarly, a school nurse-led training program motivated school staff to revise emergency response procedures (Elizalde et al., 2024). Although we did not objectively assess skills, participants’ reported intentions to modify practices suggests that structured training may support meaningful practice changes that strengthen emergency preparedness in schools.
Reported barriers highlight structural and organizational challenges that may limit translation of training into practice, particularly related to staffing capacity, leadership engagement, and time allocation. These constraints suggest that successful implementation of MERTs may depend not only on individual knowledge but also on broader system-level support within school environments. These findings are consistent with prior research regarding the importance of adequate staffing, leadership buy-in, and resources to support school nurses in emergency preparedness (Boudreaux and Broussard, 2020; Murata et al., 2020). These barriers are particularly relevant to the NASN Framework for School Nursing Practice principles of Leadership and Quality Improvement, which emphasize nurses’ involvement in decision-making, advocacy for risk-reducing policies, and engagement in system-level improvement efforts (NASN, 2024b). Overall, the findings underscore that effective implementation of MERTs requires not only individual readiness but also organizational infrastructure, including administrative support, interprofessional collaboration, and access to necessary resources, to maintain a healthy and safe school environment.
Six-month follow-up data, although limited by a small sample size of 10 participants, suggest that some participants were able to sustain knowledge gains and begin implementing MERT processes in school settings. Reported facilitators, such as administrative support, available resources, and time to apply newly acquired skills, indicate that continued application of training content may depend on environmental and organizational conditions that support practice change over time. While these findings are preliminary and cannot be generalized to the full population of training participants due to the small sample size, they underscore the potential value of structured MERT training paired with ongoing resources to reinforce knowledge and promote practice change. Although several studies have examined immediate post-training outcomes, to our knowledge, few studies have examined whether these gains persist over time, reflecting a limitation identified in earlier emergency preparedness research (Skryabina et al., 2017).
Overall, findings suggest that structured training can enhance school nurses’ knowledge of the MERT process, encourage meaningful practice change in emergency preparedness, and support competencies emphasized within the NASN School Nursing Practice Framework. In addition to assessing immediate knowledge gains, this study incorporated qualitative data to better understand factors influencing implementation and assessed application of knowledge gained over time, supporting the translation of training into practice. Opportunities for future research include the need for additional longitudinal studies with larger sample sizes that may yield greater insights into barriers and facilitators to implementing MERTs in school settings. Additionally, future qualitative research with administrators at the local, regional, and state level is critical to understand their perspectives on disseminating MERTs and support policy changes that would facilitate implementation.
Limitations
This study has several limitations. All outcome data were self-reported, and knowledge and skills were not objectively assessed, which may overestimate participants’ actual knowledge gains or implementation efforts. The survey instruments were developed for this training and were not formally tested for reliability or validity, which limits confidence in their consistency and accuracy. In addition, the retrospective pre/post format may be influenced by recall bias when participants rated their pre-training knowledge. Reported practice changes and completion of MERT components at the 6-month follow-up were not externally verified, limiting the ability to confirm the extent to which changes occurred in practice. Because this study did not include a control group, it is not possible to attribute observed changes in knowledge or MERT implementation solely to the training intervention and future randomized controlled trials are needed to examine causal changes to MERT participation.
Survey participation was voluntary, and a substantial number of training participants did not complete the surveys, particularly the 6-month follow-up. Competing professional responsibilities and the timing of the follow-up survey may have contributed to non-response. Participants who were more engaged or successful in applying the training content may have been more likely to respond, potentially resulting in an overestimation of implementation progress and overall training effectiveness. In addition, some descriptive information collected through the voluntary participant quiz contained missing responses, limiting the completeness of participant background characteristics. Lastly, the small number of respondents at follow-up limits the generalizability of the sustained knowledge findings.
Conclusion
This study highlights the potential of structured MERT training to strengthen school nurses’ capacity to lead and coordinate school-based emergency preparedness efforts. Findings suggest that training can enhance knowledge of MERT development and implementation, support practice changes aligned with the NASN School Nursing Practice Framework, and facilitate the establishment of coordinated emergency responses processes within schools. As schools continue to address increasingly complex student health needs, equipping school nurses with the knowledge, resources, and organizational support necessary to lead MERTs may strengthen emergency preparedness and contribute to safer school environments.
Footnotes
Author Contribution(s)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author “Evilia Jankowski” declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Evilia Jankowski developed and delivered the training program evaluated in this study and has a financial interest in the company that provides the program. The remaining authors declare no conflicts of interest.