
Abstract
OBJECTIVE:
To determine whether there was an increased incidence of nephrotoxicity in elderly patients (≥65 y) prescribed single-dose (SD) versus multiple-dose (MD) aminoglycosides and whether aminoglycoside-induced nephrotoxicity was associated with length of therapy and other risk factors.
METHODS:
A prospective, observational audit at a university teaching hospital was conducted. Physician prescribing was used to stratify subjects according to dosing regimen: MD (n = 60) or SD (n = 26). Nephrotoxicity was defined as an increase in the serum creatinine level of 0.5 mg/dL sustained over 2 days.
RESULTS:
Eighty-six patients were included; 9.3% developed nephrotoxicity, of whom 62.5% received SD therapy. The incidence of nephrotoxicity did not differ between regimens (p = 0.051). There was an increased length of therapy in those who developed nephrotoxicity (mean ± SD 6.1 ± 6.2 vs. 3.7 ± 2.8 d; p = 0.044). Additionally, patients who developed nephrotoxicity had an increased length of hospitalization (20.3 ± 16.1 vs. 8.4 ± 5.4 d; p < 0.001). Nephrotoxicity correlated with a diagnosis of diabetes mellitus (OR 15.1; 95% CI 1.11 to 205), concomitant angiotensin-converting enzyme (ACE) inhibitor therapy (OR 28.0; 95% CI 2.15 to 365), and SD therapy (OR 20.7; 95% CI 1.45 to 297).
CONCLUSIONS:
Our overall incidence of nephrotoxicity is consistent with that reported in the literature. A diagnosis of diabetes mellitus, concomitant use of ACE inhibitors, and SD regimens were risk factors for the development of nephrotoxicity. An adequately powered, randomized trial is needed to assess whether a difference in the incidence of nephrotoxicity exists between SD and MD therapy in the elderly.
To our knowledge, there have been 5 published studies evaluating single-dose (SD) or multiple-dose (MD) aminoglycoside therapy specifically in the elderly. One compared the efficacy and safety of amikacin given either once or twice daily in 27 elderly patients. 1 There was no difference between the groups in comparison with dosage (mean 12.8 mg/kg/d), duration of therapy (mean 9.9 d), concomitant treatment, or toxicity.
Another trial 2 evaluated the safety and clinical efficacy in a randomized manner of either tobramycin or gentamicin 4 mg/kg/d versus 2 mg/kg every 12 hours in 70 elderly men who received the drug for ≥72 hours. The mean duration of therapy was 8.3 days. There was no difference between the groups with respect to clinical and bacteriologic efficacy. The incidence of nephrotoxicity was 24% in the SD versus 14% in the twice-daily group; this difference was not statistically significant. In the SD group, a correlation was noted between high peak serum concentrations (>12.0 μg/mL) and nephrotoxicity.
Segarra-Newnham 3 performed a retrospective 2-year review of 111 men >65 years of age (average 73) who received large doses of gentamicin (based on a nomogram) for at least 2 days. The mean dose was 5 mg/kg and duration of therapy was 5.7 days. The majority (59%) of patients received 24-hour dosing, while 41% had every 36-to 48-hour dosing. Eighty-nine percent of the patients had an aminoglycoside concentration drawn; 95% were within the therapeutic range. Only 6 (5.4%) patients had an increase in serum creatinine of 0.5 mg/dL. These men had risk factors for changes in renal function, such as a prolonged duration of therapy.
Risk factors for toxicity in 88 elderly patients aged ≥70 years given SD aminoglycosides were prospectively evaluated. 4 Eighty-two percent of the patients were men and 34% had received aminoglycosides in the past year. The development of nephrotoxicity (15%) and otovestibular (3.4%) toxicity was associated with increasing duration of therapy. The incidence of nephrotoxicity for patients receiving an aminoglycoside for <7 days, between 8 and 14 days, and >14 days was 3.9%, 30%, and 50%, respectively. Specific risk factors for aminoglycoside nephrotoxicity were an elevated baseline serum creatinine level and the use of allopurinol.
A recent prospective, surveillance study assessed the safety of once- daily aminoglycoside dosing in 249 patients (84% ≥65 y) over 4 months. 5 An increase of ≥50% in the serum creatinine level was noted in 12.4% of patients. Univariate analysis statistically linked renal damage with aminoglycoside trough concentrations >1.1 μg/mL, hemoglobin <10 g/dL, hospital admission >7 days prior to aminoglycoside therapy, aminoglycoside treatment ≥11 days, and concomitant use of diuretics (p < 0.05 for each). The authors concluded that once-daily aminoglycosides for <11 days with routine trough drug concentrations rarely cause oliguric or chronic renal toxicity.
Several meta-analyses have been published that evaluated SD versus MD aminoglycoside prescribing. 6 12 The heterogeneity of the studies in each analysis was brought to light when evaluating drug selection and dosage, method of administration, dosing regimens employed, variability in patient age, concurrent antibiotics prescribed, type of infection, and concomitant disease states. These studies also varied in their collection of data, definitions of nephrotoxicity/ototoxicity, and the collection/timing (peak, trough, midpoint) of aminoglycoside serum concentrations.
Munckhof et al. 6 reviewed 19 articles on the safety and efficacy of aminoglycosides in 2881 patients. They observed a small, statistically significant difference (p = 0.027) for clinical efficacy in favor of SD aminoglycosides, but no difference between bacterial efficacy and nephrotoxicity compared with MD aminoglycosides. Another meta-analysis evaluated 18 studies with 2317 patients. 7 SD aminoglycosides were found to be more effective, less nephrotoxic, and equally ototoxic as MD aminoglycosides. Hatala et al. 8 investigated 13 studies using SD aminoglycoside dosing in immunocompetent adults. They noted a trend toward reduced nephrotoxicity, ototoxicity, and mortality with SD compared with MD administration. Nineteen studies totaling 3091 patients comparing SD or MD aminoglycosides were assessed. 9 The authors found no differences in mortality, ototoxicity, or clinical efficacy other than with Pseudomonas aeruginosa infections. They observed a decreased incidence of nephrotoxicity with SD aminoglycosides. A review of 16 studies with 1200 patients noted no difference between SD and MD aminoglycosides with respect to efficacy, nephrotoxicity, or ototoxicity. 10 Bailey et al. 11 reviewed 20 trials that had >2500 patients. These authors noted that SD was at least as effective as MD, with similar rates of nephrotoxicity and ototoxicity. Ali and Goetz 12 evaluated 21 studies and noted that clinical outcomes favored the use of SD versus MD aminoglycoside administration. They observed no difference in the occurrence of ototoxicity and nephrotoxicity.
Collectively, the meta-analyses showed no difference between SD and MD aminoglycoside therapy for clinical efficacy or ototoxicity. There may be some suggestion of a reduced incidence of nephrotoxicity with SD administration. If clinical efficacy and drug toxicity are not clinically and statistically different, then SD aminoglycoside administration has practical, cost-effective benefits. Some advantages include reduced preparation, administration, and nursing time; lower consumable cost; and less wastage.13,14 Additionally, there may be a reduction in monitoring of serum aminoglycoside concentrations, especially in patients with normal kidney function.
Our primary objective was to determine whether there was an increased incidence of nephrotoxicity in elderly patients (≥65 y) prescribed SD versus MD aminoglycoside therapy. Secondarily, we wanted to determine whether aminoglycoside-induced nephrotoxicity was associated with length of therapy, and also whether nephrotoxicity with SD versus MD aminoglycosides was associated with other risk factors, such as concurrent diseases or drug therapy.
Methods
This prospective, observational audit evaluated the physician prescribing of SD and MD aminoglycosides in elderly patients (≥65 y) at University Hospitals of Cleveland, a 1009-bed nonprofit teaching hospital with 457 adult medical/surgical beds. Gentamicin and tobramycin were the 2 aminoglycosides most commonly prescribed. Elderly patients with physician orders for either agent were identified through the hospital-wide computer system. Our institution does not have a pharmacokinetic monitoring program, so each physician determines the aminoglycoside regimen. The audit group consisted of patients who received SD aminoglycosides while the control group received MD aminoglycosides. Exclusion criteria included patients who were admitted to an intensive care unit, had a diagnosis of endocarditis, febrile neutropenia, ascites, were receiving dialysis, received <1 day of aminoglycoside therapy, or had the dosing interval changed from SD to MD or vice versa.
Two clinical pharmacy specialists enrolled all elderly patients meeting eligibility criteria Monday through Friday for a 10-month period: July 12, 1999, to May 15, 2000. To diminish variations in measurement, all parameters were defined a priori. The data collection form included demographics, weight, serum creatinine, service, location, dosing regimen, indication and duration of therapy, and type and number of serum concentrations drawn, as well as concurrent antiinfective and nephrotoxic agents. Potentially nephrotoxic agents included amphotericin B, vancomycin, intravenous furosemide, angiotensin-converting enzyme (ACE) inhibitors, cyclosporine, nonsteroidal antiinflammatory drugs, and radiographic contrast agents. Additionally, select disease states such as diabetes mellitus, coronary artery disease, hypertension, and malignancy were noted. Nephrotoxicity was defined as a sustained increase (2 d) of serum creatinine of 0.5 mg/dL from that determined prior to initiating aminoglycoside therapy.
The difference in nephrotoxicity between SD and MD therapies was evaluated by χ2 analysis. A p value ≤0.05 was considered significant. ANOVA was used to analyze the length of therapy and length of hospitalization data. Additionally, regression analysis was performed to determine whether any factor(s) significantly influenced nephrotoxicity associated with SD or MD aminoglycoside therapy.
Results
A total of 230 patients were assessed, of whom 144 (62.6%) were excluded because they did not meet eligibility criteria. Data were collected on 86 patients. The average age was 76.9 years including 53 women (61.6%) and 67 white patients (77.9%). Fifty-nine patients (68.6%) were prescribed gentamicin and 27 patients (31.4%) received tobramycin; SD therapy was prescribed to 26 patients (30.2%) and MD to 60 patients (69.8%). Internal medicine, surgery, and other disciplines were the prescribing services in 48 (55.8%), 31 (36%), and 7 (8.1%) patients, respectively.
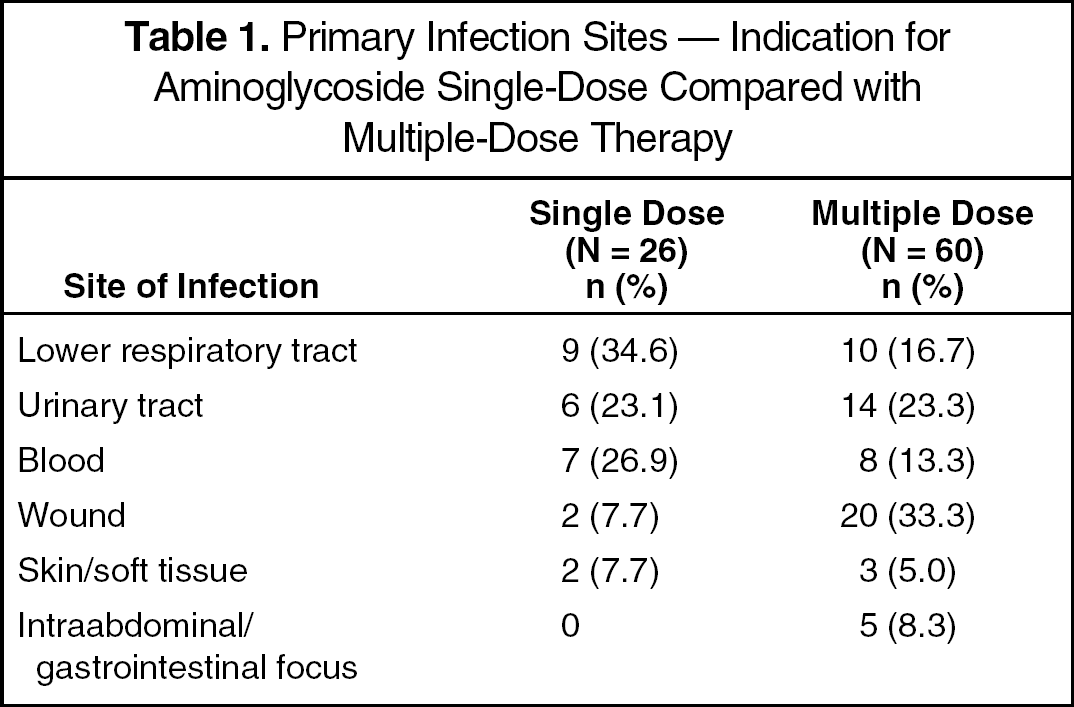
For the 86 patients evaluated, the length of aminoglycoside therapy was 4.0 ± 2.9 days (mean ± SD) and the length of stay was 9.5 ± 7.7 days. The indication for the aminoglycoside is noted in Table 1. All patients received concomitant antiinfectives, mainly β-lactams (81.3%).
Primary Infection Sites — Indication for Aminoglycoside Single-Dose Compared with Multiple-Dose Therapy
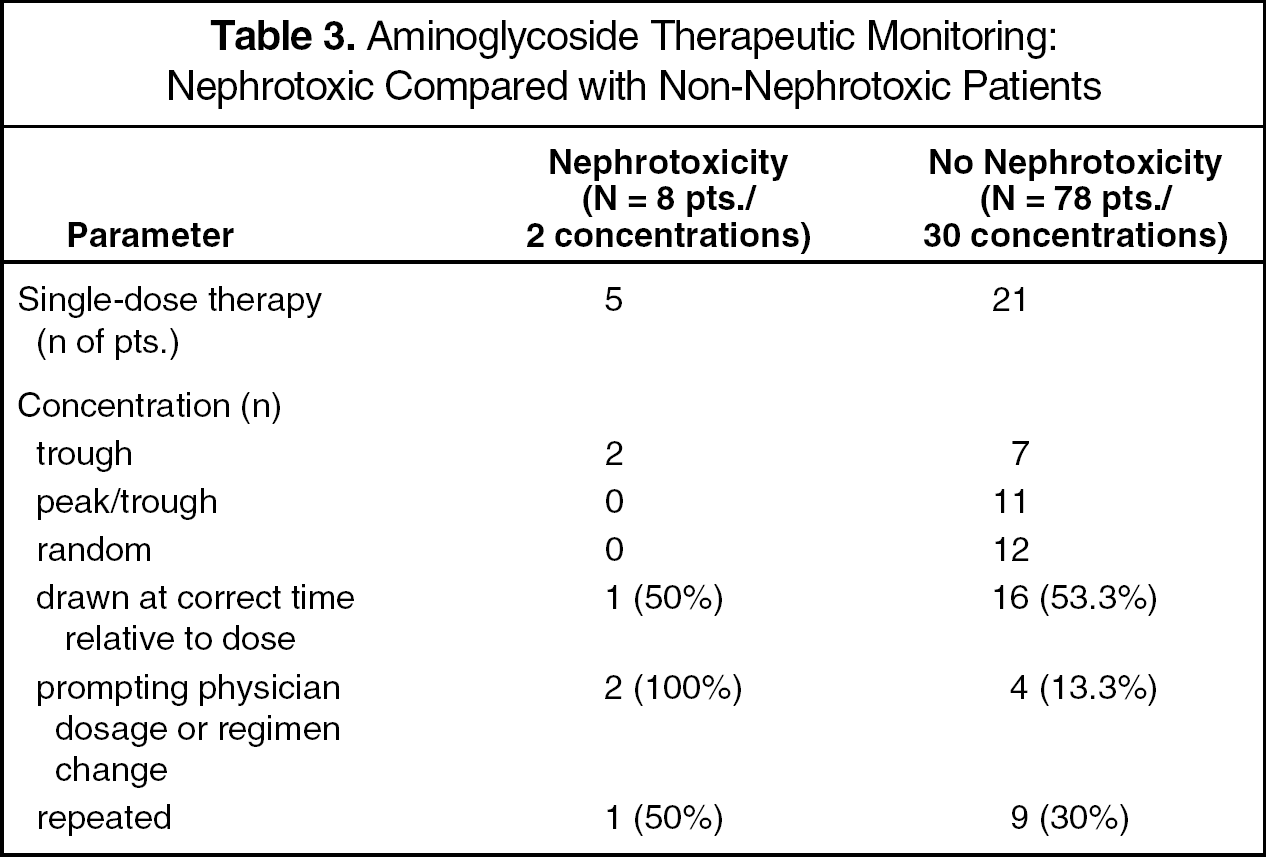
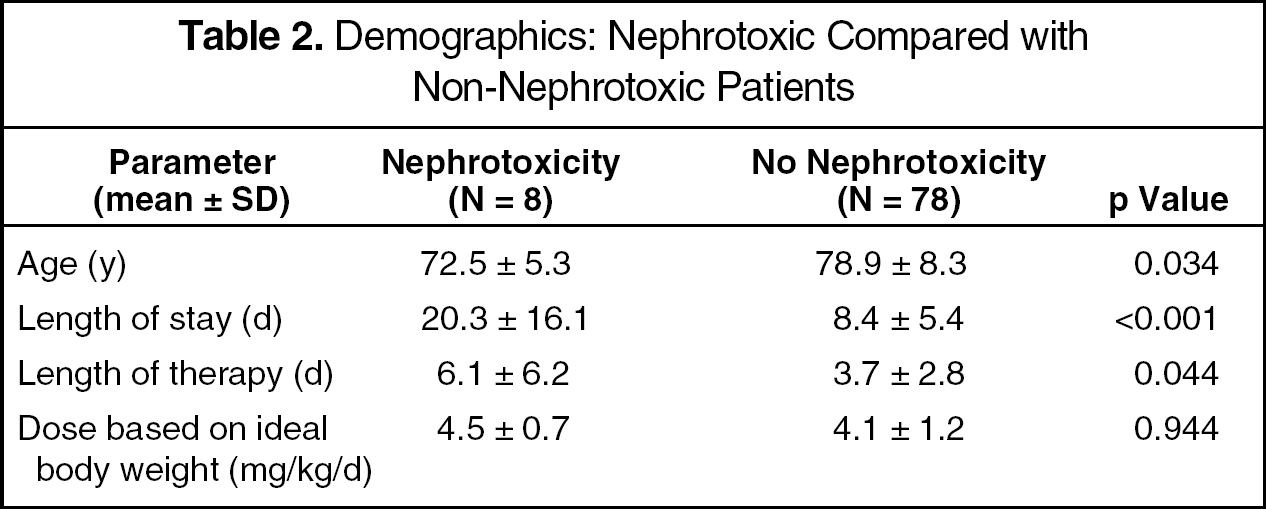
Eight patients (9.3%), of whom 5 (62.5%) were receiving SD therapy, developed nephrotoxicity. Statistical significance was not reached for the incidence of nephrotoxicity between SD and MD therapy (p = 0.051); however, a strong trend was noted. Table 2 compares the 8 patients who developed nephrotoxicity with the 78 patients who did not. Two patients who developed nephrotoxicity required dialysis: 1 died and the other continued on dialysis throughout the data collection period. Initial serum creatinine ranged between 0.5 and 1.2 mg/dL and 0.4 and 2.4 mg/dL for nephrotoxic and non-nephrotoxic patients, respectively. A description of the types of aminoglycoside serum concentrations between the nephrotoxic and non-nephrotoxic patients is provided in Table 3.
Demographics: Nephrotoxic Compared with Non-Nephrotoxic Patients
Aminoglycoside Therapeutic Monitoring: Nephrotoxic Compared with Non-Nephrotoxic Patients
Based on 1-way ANOVA, there was an increased length of therapy in the patients who developed nephrotoxicity compared with the other patients. Additionally, the patients who developed nephrotoxicity had an increased length of hospitalization and were younger than those without the nephrotoxicity. No other adverse effects associated with aminoglycoside therapy were documented.
Possible risk factors for aminoglycoside-induced nephrotoxicity are noted in Table 4. Patients developing nephrotoxicity had a higher prevalence of concurrent ACE inhibitors and vancomycin and were more likely to have diabetes mellitus compared with patients not developing toxicity. Using logistic regression analysis, nephrotoxicity was correlated with the combination of a diagnosis of diabetes mellitus (OR 15.1; 95% CI 1.11 to 205), concomitant ACE inhibitors (OR 28.0; 95% CI 2.15 to 365), and SD therapy (OR 20.7; 95% CI 1.45 to 297). In our review, concurrent vancomycin use was statistically associated with nephrotoxicity in the univariate analysis, but not in the logistic regression analysis.
Possible Risk Factors for Aminoglycoside Nephrotoxicity: Nephrotoxic Compared with Non-Nephrotoxic Patients
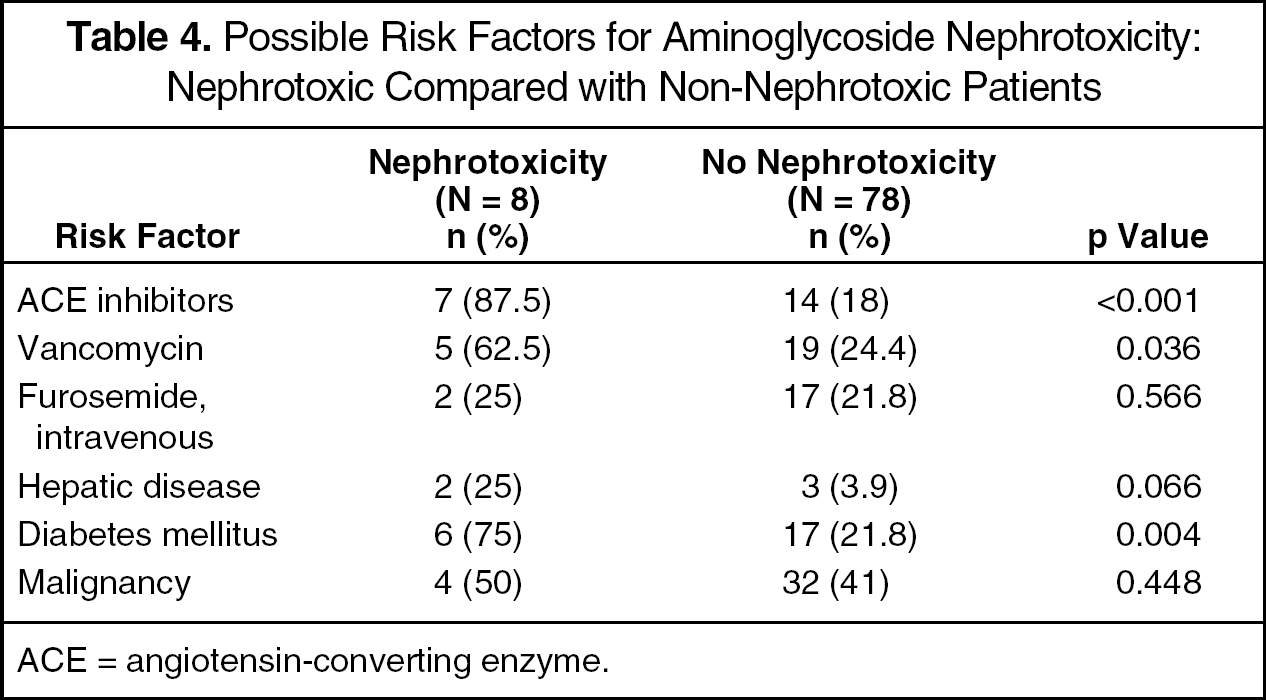
ACE = angiotensin-converting enzyme.
Discussion
Our methods and findings differ from those of other studies evaluating the use of aminoglycosides in the elderly. Unlike the studies by Vanhaeverbeek et al. 1 and Koo et al., 2 our audit was observational, had an average duration of therapy of 4 days, and included patients in whom >24 hours of therapy was administered. Vanhaeverbeek et al. assessed amikacin over a mean duration of therapy of 9.9 days. In the Koo et al. study, patients received an aminoglycoside for at least 3 days (average 8.3).
Our review was similar to that of Segarra-Newnham. 3 However, unlike that study, our institution does not have aminoglycoside dosing guidelines and patients were evaluated if they received at least 1 day versus a minimum of 2 days of aminoglycoside therapy. In the Segarra-Newnham study, all of the patients were men, were given an average dose of 5 mg/kg, and received therapy for an average duration of 5.7 days. Our study included approximately 38% male patients, an average dose of 4.1 mg/kg, and mean therapy duration of 4 days.
Our audit has several weaknesses. Potential candidates may not have been evaluated because the investigators screened patients only on weekdays. The review was not adequately powered, increasing the likelihood of a type II error. To detect a 10% difference in the incidence of nephrotoxicity between groups using a 2-tailed test and a significance level of 0.05, 553 patients would have been needed. Time constraints and manpower did not allow for such an extensive evaluation. As this was an observational audit, it is unknown what sources physicians were using to choose aminoglycoside doses and regimens. Ototoxicity was not evaluated due to the difficulty in assessing this parameter through physician notes. At our institution, vestibular and auditory testing are not routinely performed. Other risk factors for nephrotoxicity, such as hydration status and hypotension, were not evaluated. Additionally, no patient received contrast dye; therefore, it is unknown what effect this could have on a patient's renal function in combination with aminoglycoside therapy.
Summary
The overall incidence of aminoglycoside-induced nephrotoxicity in our audit is consistent with that reported in the literature. The majority of patients who developed nephrotoxicity were receiving SD therapy; however, it would be inappropriate to draw conclusions based on so few patients. We did note several risk factors for the development of aminoglycoside nephrotoxicity in elderly patients. Those who had diabetes mellitus, were prescribed ACE inhibitors, and received an SD regimen had a higher risk of nephrotoxicity.
We advise practitioners to closely monitor elderly patients receiving aminoglycosides who possess the above risk factors. An adequately powered, randomized trial would help to assess whether a difference in the incidence of aminoglycoside-induced nephrotoxicity exists between SD and traditional MD regimens in this patient population.
Footnotes
Acknowledgements
We thank Irene Orynchak MS BSPharm, Clinical Education Consultant, and Ambaris Ambegaonkar PhD, Senior Manager, Clinical Applications Team of Pfizer Inc., for their assistance with developing our data storage and analysis tool (Multiple Disease Risk Assessment 2000).