
Abstract
OBJECTIVE:
To review information on desloratadine, a nonsedating antihistamine.
DATA SOURCES:
An English-language MEDLINE search was conducted (1966–July 2002). References of identified articles were subsequently reviewed for additional data. Schering Corporation provided unpublished information.
STUDY SELECTION/DATA EXTRACTION:
Articles and abstracts pertaining to desloratadine were considered for inclusion, with emphasis on randomized, placebo-controlled, double-blind trials.
DATA SYNTHESIS:
Desloratadine is approved for the treatment of symptoms associated with seasonal allergic rhinitis (SAR), perennial allergic rhinitis (PAR), and chronic idiopathic urticaria (CIU) in patients aged ≥12 years. In placebo-controlled trials, desloratadine demonstrated superior efficacy as a once-daily treatment of SAR, PAR, and CIU. Data suggest that desloratadine has antiinflammatory and decongestant activity.
CONCLUSIONS:
Desloratadine appears to be a “me-too” agent, with no major differences compared with other second-generation antihistamines.
Peripherally acting, nonsedating oral antihistamines were developed because earlier antihistamines (e.g., chlorpheniramine, diphenhydramine), while effective in controlling allergy, urticarial, and related symptoms, also penetrate the central nervous system (CNS) and interact with cholinergic receptors, causing undesirable sedative and anticholinergic adverse effects.1,2 Terfenadine and astemizole were the first receptor-specific, second-generation nonsedating antihistamines available in the US, coming to the market in the 1980s. Despite their increased cost, they rapidly became widely used agents primarily due to their improved adverse effect profile.1,2 Both agents were withdrawn because of cardiac toxicity, particularly increased risk of QT interval prolongation and the risk of torsade de pointes.3–6
Desloratadine, approved by the Food and Drug Administration (FDA) in late 2001, is the primary active metabolite of loratadine. It is indicated for relief of the nasal and non-nasal symptoms of seasonal allergic rhinitis (SAR) and perennial allergic rhinitis (PAR), and for relief of the symptoms of chronic idiopathic urticaria (CIU) in patients aged ≥1 2 years.
Desloratadine and other second-generation, oral nonsedating antihistamines are shown in Table 1, along with their FDA-labeled indications. Cetirizine, included as well in this category, might be better classified as a low-sedating agent, since it is more sedating than the other agents in this class.1,2
Comparison of Second-Generation Oral Antihistamines
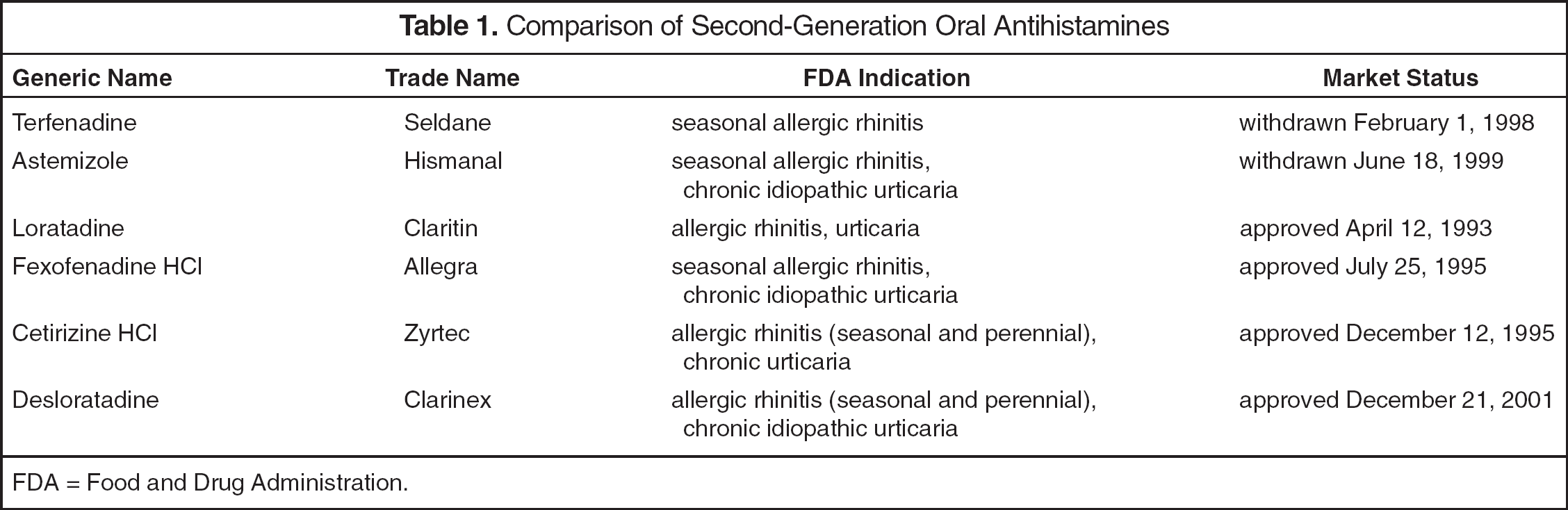
FDA = Food and Drug Administration.
Pharmacology
Antihistamines, histamine1 (H1)-antagonists, are recognized as blockers of the H1 histamine receptor, resulting in decreased capillary permeability, reduced mucus production, relaxation of smooth muscle, and reduced vasodilation, thus lessening allergy-related symptoms (e.g., sneezing, rhinorrhea, nasal pruritus, and itchy, watery eyes). 7 While histamine is still considered an important factor in the pathogenesis of allergic rhinitis and urticaria, better understanding of the allergic cascade suggests a more complicated systemic immune condition. Thus, histamine is just 1 mediator that along with others, including leukotrienes, cytokines (e.g., interleukins, tumor necrosis factor-alfa [TNF-α]), chemokines (e.g., eotaxins, regulated-on-activation normal T-cell expressed and secreted [RANTES]), and adhesion molecules (e.g., selectins, intercellular adhesion molecule [ICAM-1]) regulate complex interactions among effector cells (i.e., mast cells, basophils, eosinophils, T cells).8,9
Inhaled allergens ligate immunoglobulin E (IgE) on the surface of mast cells, causing degranulation. Symptoms such as sneezing, itching, and rhinorrhea are caused by the release of histamine, bradykinin, and leukotrienes. In this early-phase response, in susceptible individuals, these mediators cause bronchial smooth-muscle constriction and increase secretory activity. Four to 8 hours after allergen exposure, as the late-phase response occurs, cytokines and chemokines trigger the release of inflammatory mediators, perpetuating symptomatology, particularly congestion.8,9 Thus, in addition to blockade of histamine, other mediators and effector cells offer potential prevention and treatment targets.
Desloratadine exhibited potent inhibition of H-labeled pyrilamine H1-receptor binding with a mean affinity constant value of 0.87 nmol/L in human H1-receptors cloned in Chinese hamster ovary cells. The rank order of potency was desloratadine > chorpheniramine (2.0), hydroxyzine (10) > terfenadine (40) > cetirizine (47.2) > loratadine (138) > fexofenadine (175). 10 The superior potency of desloratadine is supported by a similar study. 11
Inhibition of histamine release by desloratadine occurred in both human and rodent cell cultures in both IgE-dependent and -independent release of histamine from mixed peripheral leukocyte preparations. 12 In a series of animal studies, Kreutner et al. 13 evaluated the H1-receptor antagonism of desloratadine, demonstrating increased potency compared with loratadine and terfenadine and similar potency compared with astemizole and chlorpheniramine. Desloratadine has more affinity for the H1-receptor subtype compared with the H2-receptor subtype and muscarinic receptors (15–50 times less than the H1 affinity). 13 Desloratadine is also a potent antagonist of calcium influx compared with cetirizine, fexofenadine, or loratadine. Calcium influx is needed for IgE-mediated degranulation and subsequent release of histamine and other proinflammatory mediators from mast cells and basophils.14,15
Desloratadine has effects on effector cells and mediators other than histamine. The release of histamine, tryptase, leukotriene (LTC4), and prostaglandin (PGD2) from mast cells and basophils was attenuated by desloratadine.12,16 Stimulated mast-cell release of the cytokines interleukin (IL)-3, IL-6, TNF, and granulocyte macrophage colony-stimulating factor was reduced by desloratadine to a greater extent than by dexamethasone, ranitidine, and cetirizine. 17 IL-8 release was inhibited by desloratadine in mast cells, basophils, and endothelial cells. 18 Inhibition of in vitro generation of the cytokines IL- 4 and IL-13 from basophils was shown with desloratadine 19 as was the release of the chemokine RANTES from nasal polyp epithelial preparations. 10 Dose-dependent down regulation of the adhesion molecule ICAM-1 has also been documented.20,21 Finally, desloratadine attenuated in vitro chemotaxis, activation, and superoxide generation of eosinophils. 10
The wide range of antiinflammatory effects demonstrated by desloratadine is not unique. A substantial body of published data on other second-generation antihistamines documents their effects on the mediators and effector cells involved in the allergic cascade,1,22–29 although a few researchers found contradictory data.30–36 The clinical implications of potential antiinflammatory effects of antihistamines are unknown. In many of the in vitro studies, concentrations of the drugs that were used were supratherapeutic. Further, it is not known which specific effect or effects would be most critical in differentiating one antihistamine from another. Finally, any antiinflammatory properties of antihistamines are not as great as those of intranasal corticosteroids, as demonstrated in clinical studies and recognized in treatment guidelines.37–41
Pharmacokinetics
Following oral administration of desloratadine 5 mg, the mean time to maximum plasma concentration is about 3 hours, the mean steady-state peak plasma concentration (Cmax) is 4 ng/mL, and AUC is 56.9 ng • h/mL. 42 The bioavailability of desloratadine 7.5 mg given with or without food was evaluated in 18 healthy volunteers. Desloratadine was given after a 10-hour fast and after a high-fat, high-calorie meal. The plasma concentration–time curves were similar and no significant difference was found between the groups.
Desloratadine pharmacokinetics are linear, as demonstrated in 20 male volunteers in a single-dose crossover study 44 and in another group of 49 volunteers in a multi-dose evaluation. 45 Data collected showed a mean Cmax ranging from 2.18 to 8.08 ng/mL over a dosage range of 5–20 mg/d and an AUC ranging from 78 to 290 ng • h/mL. 45 Similar results were observed in children (aged 2–5 and 6–11 y). 46
Desloratadine, which is itself an active major metabolite of loratadine, is metabolized to the active metabolite 3-hydroxydesloratadine (3-OH-desloratadine), which is, in turn, glucuronidated. Desloratadine (82–87%) and 3-OH-desloratadine (85–89%) are bound to plasma proteins. 42 At therapeutic concentrations, desloratadine demonstrates little or no inhibition for CYP1A2, CYP3A4, CYP2C19, CYP2C9, or CYP2D6, suggesting little potential for clinically significant drug interactions. 47
The mean elimination half-life of desloratadine is 27 hours. Approximately 87% of the parent drug is equally distributed between urine and feces as metabolite. 42 By comparison, loratadine has a half-life of 12–15 hours, with similar metabolism. 48
With the exception of the absorption data reviewed above, no data are available on the use of desloratadine in children <12 years old. For patients ≥65 years old, female, or African American, no dosage adjustments are necessary. 49 A subset of the population are slow metabolizers of desloratadine, demonstrating a half-life >50 hours. 42 The clinical significance of this finding is unknown.
Plasma concentrations of desloratadine increased in patients with renal impairment. For those with liver impairment, AUCs increased compared with subjects with normal liver function. The mean elimination half-life of desloratadine was increased; that of the 3-OH metabolite was not. 42
Clinical Studies
Discussed below and further summarized in Table 2 are published and unpublished clinical studies of desloratadine for the treatment of SAR (with and without asthma), PAR, and CIU.50–64
Efficacy of Desloratadine in Clinical Studies for SAR, PAR, and CIU
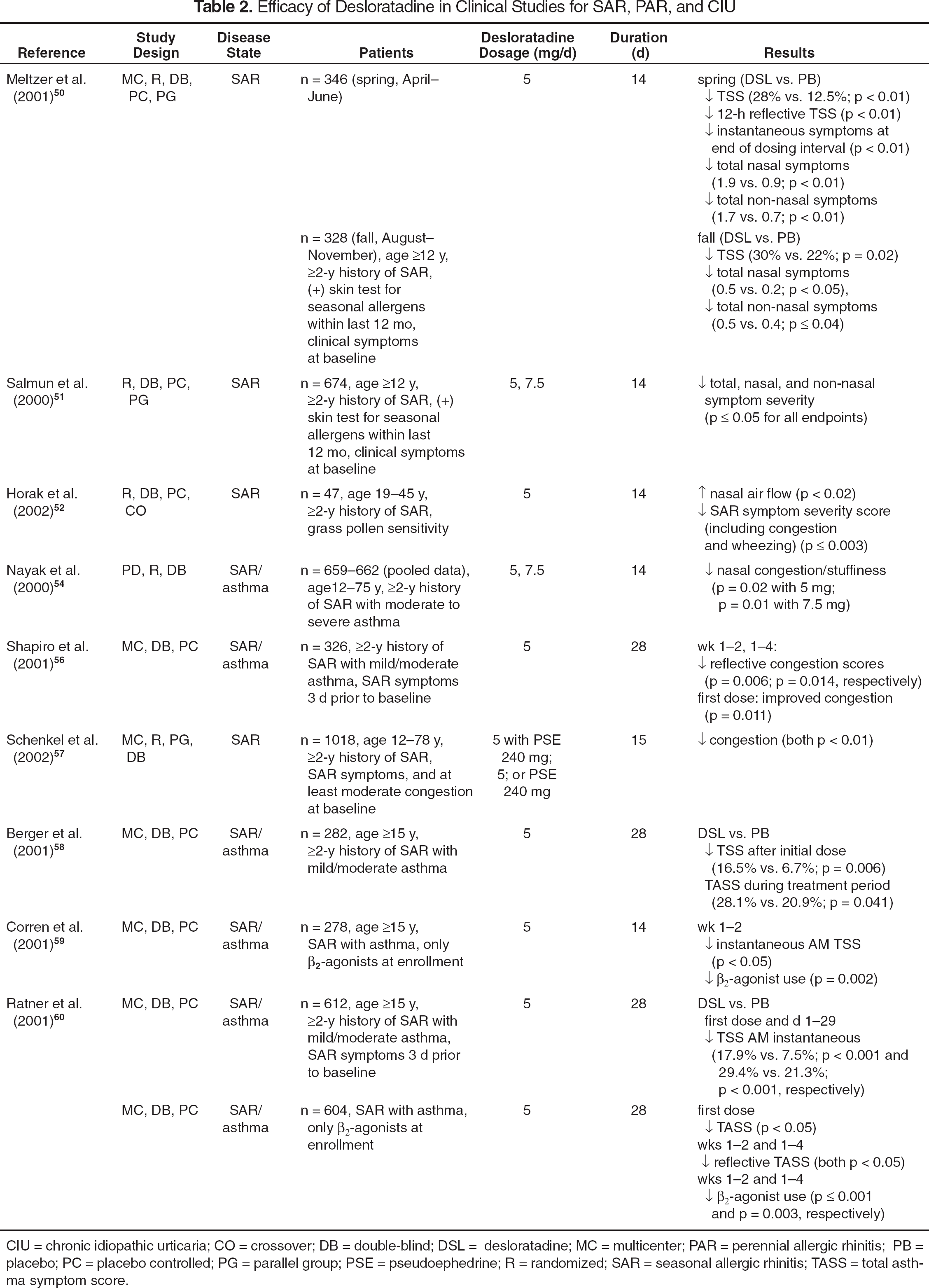
CIU = chronic idiopathic urticaria; CO = crossover; DB = double-blind; DSL = desloratadine; MC = multicenter; PAR = perennial allergic rhinitis; PB = placebo; PC = placebo controlled; PG = parallel group; PSE = pseudoephedrine; R = randomized; SAR = seasonal allergic rhinitis; TASS = total asthma symptom score.
SEASONAL ALLERGIC RHINITIS
Two placebo-controlled studies, published as a single article, evaluated the efficacy of desloratadine for the treatment of patients with SAR during spring and fall allergy seasons. 50 Patients were randomized to receive desloratadine 5 mg or placebo once daily for 14 days. Symptoms were scored by the patients in the morning (AM) and evening (PM) by using a 4-point scale (0 = none, 1 = mild, 2 = moderate, 3 = severe). The initial AM score was a measure of desloratadine's duration of effect, while the 2 reflective daily ratings (AM/PM) for symptom severity were summed to calculate a total symptom severity score (TSS). The primary efficacy endpoint was the mean change from baseline for the averaged TSS during the 2-week treatment periods. Secondary efficacy endpoints included changes from baseline for initial AM scores, total nasal and non-nasal symptom scores, and onset of symptom relief. A reduction in TSS from baseline for desloratadine when compared with placebo during the spring and fall allergy seasons was reported: desloratadine was superior to placebo for secondary efficacy endpoints. Another study evaluating the efficacy of desloratadine for SAR found comparable results for reductions in TSS, total nasal and non-nasal symptom severity, and first- dose TSS. 49
The decongestant effects of desloratadine were evaluated in patients (SAR history) with grass/pollen-induced allergic rhinitis. 52 Nasal obstruction was measured by nasal airflow; desloratadine was more effective than placebo in improving airflow. Nasal congestion symptom severity scores were also improved for desloratadine compared with placebo (p < 0.001 for both time points measured). A few clinical studies evaluated desloratadine's ability to relieve nasal congestion in patients with SAR53–55 and SAR with asthma.54,56 All used similar methodology, where desloratadine 5 mg (1 study also used 7.5 mg) was compared with placebo. Twice-daily reflective congestion scores (assessing severity of nasal congestion over the previous 12 h), were significantly improved for the active treatment groups compared with placebo at all time points. Another study compared desloratadine combined with pseudoephedrine with monotherapy with either agent. 57 The combination was significantly better in relieving nasal congestion than either agent alone, with each agent on its own providing similar congestion relief.
Two 4-week, placebo-controlled studies evaluated the efficacy of once-daily desloratadine 5 mg for treatment of patients with SAR and concurrent mild to moderate asthma.58,59 Patients had to have SAR and asthma symptoms 3 days prior to baseline assessment, a forced expiratory volume in 1 second ≥70%, and only using intermittent inhaled β2-agonists for asthma treatment. SAR and asthma symptoms were scored twice daily. Patients also recorded daily β2-agonist use. A pooled analysis of both studies suggested that desloratadine, when compared with placebo, resulted in a significant reduction from baseline for TSS after the first dose (p < 0.025) that was maintained throughout the study period. 60 Additionally, a reduction in β2-agonist use for the desloratadine group was reported during weeks 1–2 and 1– 4 (p < 0.001, p = 0.003, respectively).
PERENNIAL ALLERGIC RHINITIS
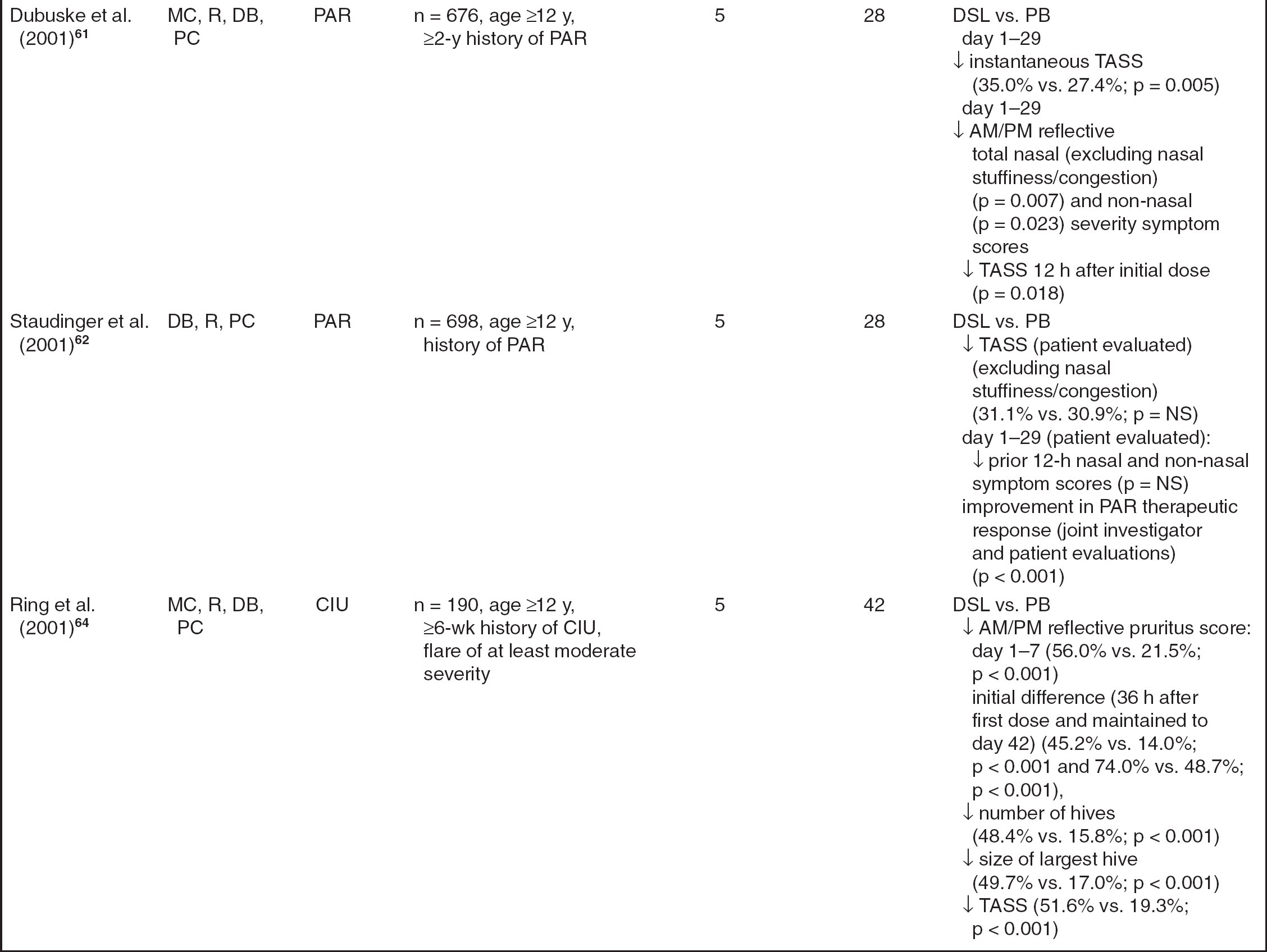
Dubuske et al. 61 conducted a 4-week, placebo-controlled trial, evaluating the efficacy of once-daily desloratadine 5 mg for the relief of symptoms associated with PAR. Patients with a ≥2-year PAR history (confirmed by a positive allergen skin test) were included. The severity of nasal (rhinorrhea, postnasal drip/drainage, itching, sneezing) and non-nasal (itching, burning, tearing, watering of the eyes and itching of the ears or palate) symptoms were self-evaluated and scored. Instantaneous (at the time of assessment) and reflective (during the prior 12 h) scores were recorded daily and then summed to determine TSS. The primary efficacy variable was the mean change from baseline in AM/PM instantaneous TSS during the study period. Secondary efficacy variables included total nasal and non-nasal symptom scores, onset of symptom relief after the initial dose, and 24-hour efficacy. Mean AM/PM instantaneous TSS throughout the study period was significantly reduced from baseline for desloratadine when compared with placebo-treated patients. Improvements in AM/PM reflective total nasal and non-nasal symptom scores were reported throughout the study period for desloratadine-treated patients. Also, improvements in TSS from baseline values were noted 12 hours after the initial desloratadine dose was administered.
A similarly designed, unpublished trial enrolled patients with PAR; no significant difference was found for mean reduction in TSS (as scored by the patient) when desloratadine was compared with placebo. 62 Nor was there a difference in efficacy between desloratadine and placebo for patient-rated evaluations for TSS and total nasal and non-nasal symptom scores for days 1–29. Moreover, patients reported no difference for nasal itching, postnasal drainage, or itching of the ears or palate. However, desloratadine was more effective than placebo for improvement in PAR based on joint investigator and patient evaluation of therapeutic response.
CHRONIC IDIOPATHIC URTICARIA
A 6-week, placebo-controlled study compared desloratadine with placebo for the treatment of CIU. 64 Eligible patients were randomized to receive desloratadine 5 mg or placebo daily. The severity of CIU symptoms (pruritus, number of hives, size of the largest hive) was evaluated and rated twice daily by the patients. Additionally, patients assessed interference with sleep and daily activities. Desloratadine was significantly more effective than placebo for the average AM/PM reflective pruritus score during the first week of treatment. A reduction in the AM/PM reflective pruritus score for desloratadine- and placebo-treated patients was first noted approximately 36 hours (day 2) after initial administration and was maintained throughout the study period. Similar score reductions for desloratadine when compared with placebo were reported for number of hives, size of the largest hive, TSS after the first dose, and TSS during week 1. Desloratadine-treated patients also reported significant improvements in sleep and daily activities.
Safety and Tolerability
Desloratadine is generally well tolerated, with the majority of adverse events rated as mild to moderate in severity, and similar to those of placebo.50–64 In 2 studies comparing desloratadine with placebo for treatment of SAR, headache was the most frequently reported adverse event (16% vs. 14% and 24% vs. 27%, respectively). 50 Other adverse events reported in ≥2% of desloratadine- or placebo-treated patients were pharyngitis, dry mouth, dysmenorrhea, and somnolence. Across clinical trials, there was no difference in the percentage of desloratadine- or placebo-treated patients who prematurely withdrew from the trials because of adverse events.50–64
Previously marketed second-generation antihistamines (terfenadine, astemizole) are known to block cardiac potassium channels, resulting in serious cardiovascular conduction adverse events characterized by a prolonged QT interval and the development of torsade de pointes. 6 To date, this has not been observed with desloratadine. Banfield et al. 65 compared a high dose of desloratadine (45 mg/d) with placebo in healthy volunteers to determine whether desloratadine had any significant effects on cardiovascular parameters. Results indicated that desloratadine had no significant effect on QTc, PR, and QRS intervals. However, the ventricular rate was elevated by 9.4 beats/min during desloratadine administration. The significance of this report has been minimized because the elevation was related to an isolated rapid heart rate in a single patient (117 beats/min with desloratadine vs. 112 beats/min with placebo). Additional studies and reports using lower doses of desloratadine (5 mg) support the conclusion that this agent has no clinically relevant effects on cardiovascular conduction parameters.50,64
The first-generation antihistamines have a high incidence of CNS adverse events, particularly sedation. There is less sedation with second-generation antihistamines, except for cetirizine. In animal studies, desloratadine did not cross the blood-brain barrier.66,67 Scharf et al. 68 reported that CNS effects (i.e., wakefulness, psychomotor impairment) did not differ significantly from those of placebo when desloratadine 7.5 mg was administered to healthy volunteers, but desloratadine did cause significantly less sedation and performance impairment than diphenhydramine 50 mg (p < 0.01 vs. desloratadine and placebo). Desloratadine's nonsedating profile was further confirmed in a placebo-controlled trial evaluating the psychomotor effects of desloratadine 7.5 mg when given concomitantly with alcohol. 69 It was concluded that desloratadine does not augment the psychomotor effects of alcohol.
Drug Interactions
Drug interactions caused by alterations in drug metabolism and subsequent elevations of serum drug concentrations may lead to serious adverse events. Potentially fatal cardiovascular adverse events (torsade de pointes) due to drug-drug interactions between formerly marketed H1-receptor antagonists (terfenadine, astemizole) and potent CYP3A4 inhibitors (erythromycin, ketoconazole) have been documented. 70 Because of the severity of these events, consideration of potential drug- drug interactions with investigational H1-receptor antagonists has become imperative.
Desloratadine and its active metabolite are unlikely to affect the oxidative metabolism and intrinsic clearance of coadministered agents that undergo metabolism by CYP1A2, CYP2C9, CYP2C19, CYP2D6, or CYP3A4. 47 In vitro investigations 47 and studies in healthy volunteers71,72 have explored these potential interactions with desloratadine. A study in healthy volunteers evaluated the safety of desloratadine 7.5 mg/d in conjunction with oral erythromycin or placebo. 72 Coadministration of these agents showed no clinically or statistically significant electrocardiographic (ECG) changes with respect to ventricular rate and QT, PR, QRS, or QTc intervals. Results of a similarly designed trial also suggested no significant changes to ECG parameters during concomitant administration of desloratadine and ketoconazole. 73 Other studies evaluated the coadministration of desloratadine with fluoxetine (CYP2D6, CYP3A4), cimetidine (CYP2D6, CYP3A4), and azithromycin in healthy volunteers to determine possible interactions.74–76 Results of these trials showed no clinically relevant changes in ECG parameters, although increased plasma concentrations of desloratadine and 3-OH- desloratadine were noted.
Other drug–drug interactions may occur from altered bioavailability. Mediators of CYP450 or other active transport systems (P-glycoprotein, organic anion transporting polypeptides), such as grapefruit juice, have been shown to significantly alter the bioavailability of certain medications. 77 Cayen et al. 78 reported that desloratadine is a weak inhibitor of P-glycoprotein in vitro and, therefore, has a decreased potential for causing these types of interactions. In 1 non-blinded, crossover study evaluating the effects of grapefruit juice on desloratadine pharmacokinetics, healthy adults received desloratadine 5 mg or fexofenadine 60 mg administered with and without grapefruit juice. 79 Results showed that coadministration of grapefruit juice did not affect the rate or extent of absorption of desloratadine, but did cause a reduction in bioavailability of fexofenadine.
Dosage and Administration
Desloratadine is available as film-coated and rapidly disintegrating 5-mg tablets for oral administration. Both dosage forms may be taken without regard to food.42,43,80 For all FDA-approved indications, the recommended dosage of desloratadine for adults and children ≥12 years old is 5 mg/d. Safety and efficacy in patients <12 years old have not been established. If patients have hepatic or renal insufficiency, the recommended starting dosage is 5 mg every other day. 42
Formulary Recommendations
Desloratadine has demonstrated efficacy and safety as a once-daily treatment of SAR, PAR, and CIU when it was compared with placebo. It is the only marketed nonsedating antihistamine that has labeling for all of these indications (cetirizine has the 3 indications, but is not labeled as a nonsedating antihistamine). Although there are some differences among the second-generation antihistamines, nothing sets 1 apart from another. Physician and patient preferences play a large role in the choice of individual agents. None of these agents is inexpensive; Table 3 shows monthly costs. 81
Monthly Drug Costs for Second-Generation Oral Antihistamines
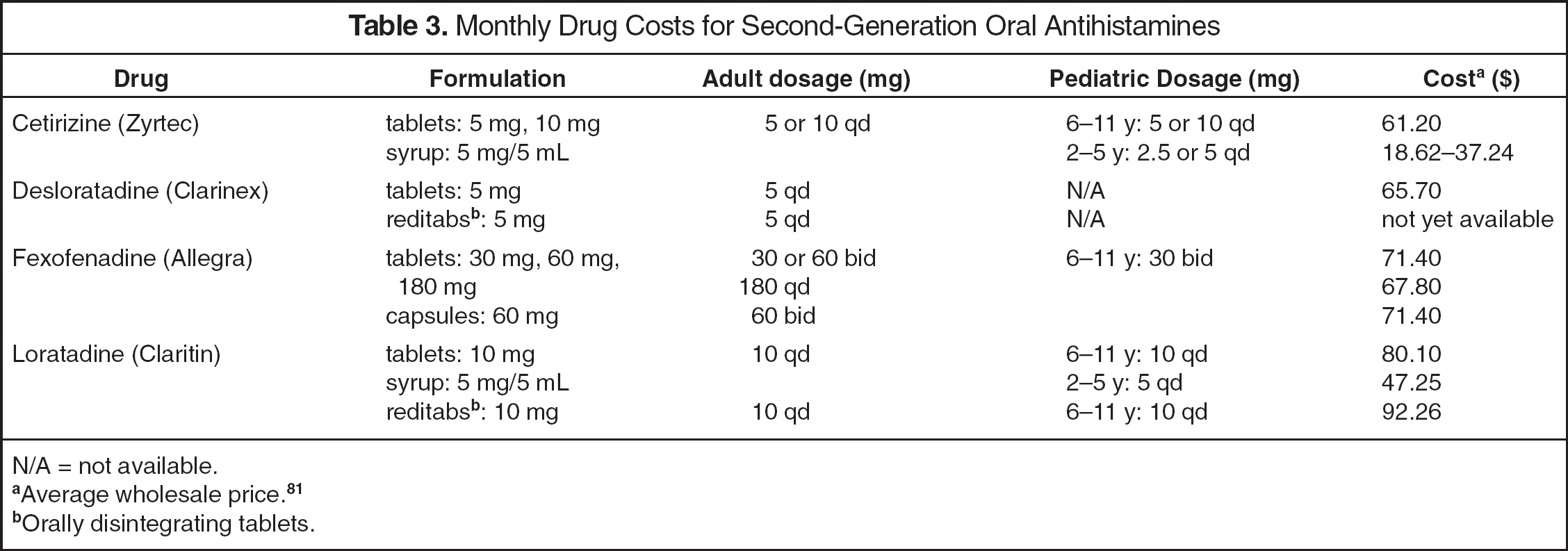
N/A = not available.
Average wholesale price. 81
Orally disintegrating tablets.
The costs of treating allergic rhinitis are considerable. An estimated 20–40 million Americans suffer from allergic rhinitis. Patients with SAR, commonly known as hay fever, usually have more acute symptoms in the spring or fall. Those with PAR suffer year-round from inhaled non-seasonal allergens such as house dust, mite, and animal dander. 82 Fineman 83 compiled data on direct and indirect costs: in year 2000 dollars, total costs ranged from $1.58 billion to $2.2 billion, with prescription drugs accounting for $0.35–1.07 billion of those totals. The cost of nonprescription medications is not included in these numbers. Direct costs include the drugs as well as physician visits; indirect factors include quality-of-life issues, such as work productivity, learning, cognitive functioning, decision-making, and self-perception. Substantial research supports the negative effects of this chronic problem in adults and children. With an increasing prevalence, the economic burden of allergic rhinitis will continue to grow.83,84
A controversial issue with this class of drugs is a possible forced switch from prescription to nonprescription status of all the second-generation antihistamines, a potential FDA action without legal precedent. The burden of cost covered by insurers would be transferred to consumers. In May 2001, the FDA's Nonprescription and Pulmonary Allergy Drugs Advisory Committees discussed a 1998 Blue Cross of California/WellPoint Health Network citizen petition asking to relabel loratadine, cetirizine, and fexofenadine as nonprescription medications (desloratadine had not yet received FDA approval). Although both advisory committees recommended that all 3 agents were suitable for nonprescription status, to date, the FDA has taken no action. 85 Although the focus of the discussion was on cost, an important potential safety benefit of a switch is that the first-generation antihistamines have well-documented cognitive impairment effects that the newer agents do not share. 86
At the time of the May 2001 FDA advisory board meetings, Schering argued against the move, saying that there were not enough postmarketing safety data to support the change. In January 2002, Schering itself submitted a supplemental New Drug Application to switch all indications and formulations of loratadine. It is unknown whether the aforementioned postmarketing safety data were included with the submission. Contributing factors for Schering's submission probably include loratadine patent expiration in December 2002 and manufacturing issues delaying the approval and launch of its successor.85,87
Desloratadine appears to be a “me-too” agent and any decision on formulary inclusion will be based on its price to a particular organization versus other agents. One disadvantage of desloratadine is its approval only for those patients aged ≥12 years, with no liquid dosage form available; however, it is expected that desloratadine will have pediatric options in the near future.
Many institutions do not include (or have limited numbers of) nonprescription medications on the formulary. With the coming of nonprescription loratadine and, potentially, the other agents, many institutions and managed-care plans may discontinue any remaining prescription versions of nonsedating antihistamines as a cost-saving measure. 88
Summary
The coming of nonprescription loratadine may have an impact on the formulary status of all of the second-generation oral antihistamines.