Short-Term Oral Cobalamin Therapy for Food-Related Cobalamin Malabsorption
TO THE EDITOR: Oral cobalamin (vitamin B12) therapy may be effective for treating patients with cobalamin deficiency, especially those with food–cobalamin malabsorption (FCM).1 We have established that 3 months of oral cobalamin therapy is beneficial.2 To date, however, the duration of treatment has not been determined.3
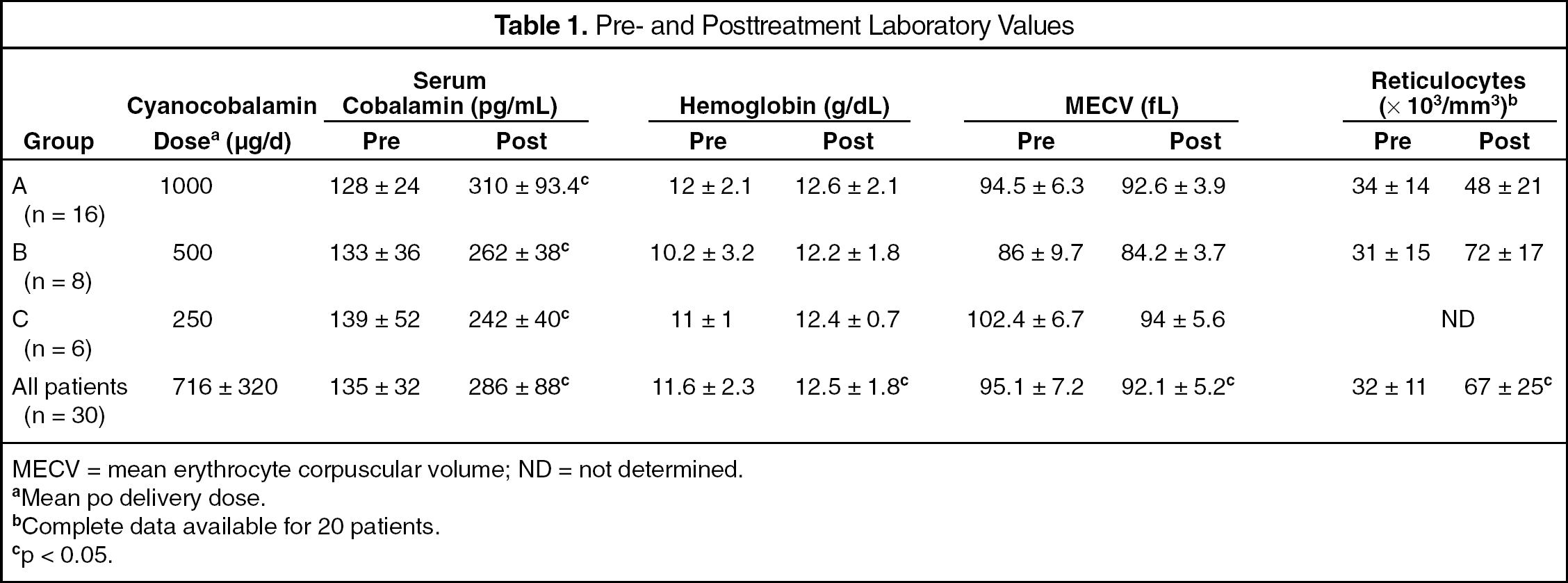
We report preliminary results of an open-label, non–placebo-controlled study on 30 patients with established cobalamin deficiency (serum vitamin B12 <200 pg/mL ± homocysteine >13 μmol/L) related to FCM4 who received between 250 and 1000 μg of oral crystalline cyanocobalamin per day for at least 1 month.
Methods. All patients were white (mean age 72 ± 13 y); 20 were women. Clinical findings included alteration of cognitive function (impaired concentration, memory loss, disorientation) (n = 9), sensitive peripheral neuropathy (n = 7), and ischemic stroke (n = 2). The mean pretreatment vitamin B12 and total homocysteine levels were 135 ± 32 pg/dL (range 82–192) and 20.2 ± 4.6 μmol/L (range 14–35), respectively (Table 1). All patients met the criteria for cobalamin deficiency related to FCM. No serum antibodies to intrinsic factor were detected. Schilling's test results were normal in 10 of 10 patients who were tested (mean ± SD 57Co/58Co ratio 0.95 ± 0.1). Two patients also had mild deficiency due to low vitamin B12 intake.
MECV = mean erythrocyte corpuscular volume; ND = not determined.
Mean po delivery dose.
Complete data available for 20 patients.
p < 0.05.
All the patients were treated with oral crystalline cyanocobalamin for ≥1 month. Oral cobalamin 250–1000 μg/d was administered. Compliance with therapy was good and no adverse events were reported.
Results. Response to treatment is indicated in Table 1. During the first month of treatment, 87% of the patients achieved normal serum cobalamin levels; all had increased serum cobalamin levels (mean 167 pg/dL; p < 0.001 compared with baseline), evidence of medullar regeneration, and corrected initial macrocytosis. Anemia was corrected in 54%. All patients had increased hemoglobin levels (mean 0.6 g/dL), reticulocyte count (mean 35 × 103/mm3), and decreased erythrocyte cell volume (mean 3 fL) (all p < 0.05).
Discussion. These findings suggest that patients with cobalamin deficiency related to FCM promptly benefit from oral crystalline cyanocobalamin. In fact, during the first month of therapy, most patients had significant improvement in serum cobalamin levels as well as in blood cell counts. These results are consistent with those observed in larger studies that used long-term (3–6 mo) or higher doses (>2000 μg/d) parenteral cyanocobalamin.2,3,5 We observed a dose–response effect of oral cyanocobalamin treatment.
Limitations of our study include the small population and lack of a control group. However, because of the apparent effectiveness of oral therapy and its possible benefits compared with intramuscular treatment (e.g., better compliance, lower cost), further studies with larger sample sizes that use different cyanocobalamin doses and duration are warranted.
References
1.
EliaM. Oral or parenteral therapy for B12 deficiency. Lancet1998; 352: 1721-2.
2.
AndrèsE, KurtzJE, PerrinAE, MaloiselF, DemangeatC, GoichotB, et al. Oral cobalamin therapy for the treatment of patients with food–cobalamin malabsorption. Am J Med2001; 111: 126-9.
3.
LaneLA, Rojas-FernandezC.Treatment of vitamin B12 deficiency anemia: oral versus parenteral therapy. Ann Pharmacother2002; 36: 1268-72.
4.
CarmelR. Malabsorption of food cobalamin. Baillière's Clinical Haematol1995; 8: 639-55.
5.
KuzminskiAM, Del GiaccoEJ, AllenRH, StablerSP, LindenbaumJ.Effective treatment of cobalamin deficiency with oral cobalamin. Blood1998; 92: 191-8.