
Abstract
Background
Rasburicase is a recombinant form of urate oxidase and facilitates the renal clearance of uric acid in patients with hyperuricemia from tumor lysis syndrome (TLS). Rasburicase converts uric acid to allantoin, a highly water-soluble compound, allowing it to be excreted in urine.1,2 Rasburicase was initially approved by the Food and Drug Administration in July 2002 for the treatment of hyperuricemia in pediatric patients at risk for the development of TLS; however, the approval was expanded in 2009 to include the adult population. Rasburicase has been shown to be more efficacious than allopurinol in treating patients with TLS and hyperuricemia 3 and is recommended by the Guidelines for the Management of Pediatric and Adult Tumor Lysis Syndrome published by the American Society of Clinical Oncology in 2008. 4 The approved dose is 0.2 mg/kg daily for a maximum of 5 days; however many institutions are using 1-time doses and fixed low doses with similar efficacy.5,6 Rasburicase is generally well tolerated, with most adverse effects lasting less than 2 days. Hematologic events, including hemolytic anemia and methemoglobinemia, were reported in less than 1% of patients in a 703-patient pooled analysis of the premarketing data. 7
Several cases of rasburicase-induced methemoglobinemia are reported in the literature.8-16 Most of these cases involved patients who were positive for glucose-6 phosphate dehydrogenase (G6PD) deficiency, a known contraindication to the use of this medication. All patients in these reports recovered quickly and survived to hospital discharge. Although the hemolytic effects of rasburicase are rare, it is recommended that patients be screened for G6PD deficiency prior to its administration. 4 Our case describes a patient who developed rasburicase-induced methemoglobinemia despite a negative G6PD screen and ultimately died after 16 hospital days and several complications. A calculated score of 7 on the Naranjo probability scale indicated that the association between rasburicase and the development of methemoglobinemia was probable. 17
Case Report
A 62-year-old man was admitted to the oncology service from the oncology clinic, where he presented after experiencing continued abdominal and back pain, hiccups, shortness of breath, and difficulty urinating. He had a 13-year history of chronic lymphocytic leukemia and small lymphocytic lymphoma, which had been treated with several chemotherapy regimens. He was started on lenalidomide and prednisone, 6 days prior to admission, for back pain that was thought to be caused by progressing intra-abdominal lymphadenopathy seen on computed tomography scan. Also, 2 days prior to admission, he was seen in the emergency department for persistent back pain that was not responsive to increased doses of oxycodone.
On the day of admission, the patient continued to experience back pain as well as abdominal pain and hiccups. He was also experiencing shortness of breath, cough, sputum production, vomiting, decreased oral intake, smaller bowel movements, and decreased urine output. The patient appeared uncomfortable, diaphoretic, tachypnic, and was maintaining an oxygen saturation of 95% on 2 L through nasal cannula. The abdominal exam was notable for hypoactive bowel sounds and pain in the left upper quadrant that radiated to the right upper quadrant. Neurologically, he was alert and oriented but slow to respond when questioned. His past medical history also included myocardial infarction with stent placement 7 years prior to admission. Medications prior to admission included amlodipine 5 mg daily, atorvastatin 80 mg daily, lenalidomide 5 mg daily, metoprolol succinate 25 mg daily, omeprazole 20 mg daily, prednisone 60 mg daily, hydromorphone 4 mg every 4 to 6 hours as needed for pain, and ondansetron 4 mg, 3 times daily as needed for nausea. His admission labs were notable for hemoglobin 11.4 g/dL, white blood cell count 49 000/µL (89% lymphocytes), platelets 42 000/µL, sodium 119 mmol/L, chloride 78 mmol/L, anion gap 24, serum creatinine 5.19 mg/dL, uric acid 12.5 mg/dL, total bilirubin 0.8 mg/dL, and methemoglobin 0.3%.
A single dose of rasburicase 3 mg (0.038 mg/kg) was given intravenously on the evening of admission for his elevated uric acid level. Overnight, he continued to decline and became more hypoxic, tachypnic, hypotensive, and oliguric. The following day, his uric acid remained elevated at 9.5 mg/dL, and a second dose of rasburicase of 3 mg was ordered and given. On the evening of hospital day 2, he was transferred to the intensive care unit (ICU) for worsening tachypnea, increasing oxygen requirements, hypotension, and increasing somnolence. The patient was started on vancomycin and piperacillin/tazobactam for possible pneumonia and developing neutropenia. He was started on bilevel positive airway pressure (BiPAP) without improvement in oxygenation, and his arterial blood gas was notable for a methemoglobin concentration of 19.3%. He was emergently intubated by anesthesia late in the evening of hospital day 2 after a short trial of BiPAP. A medical toxicologist was consulted and recommended methylene blue 1 mg/kg if his methemoglobinemia and respiratory status did not improve. He was given 2 units of packed red blood cells (PRBCs), and his methemoglobin level improved to 18%, but his hypoxia continued to worsen. Therefore, he was given a reduced dose of methylene blue 0.75 mg/kg by the medical ICU team, just prior to midnight on hospital day 2. The dose was reduced because of concern for delayed clearance of the drug as a result of his poor renal function.
Hospital day 3 was notable for worsening hypotension, leukocytosis, and renal function from presumed septic shock, for which norepinephrine and continuous renal replacement therapy was initiated. Stool cultures were notable for Clostridium difficile toxin. A G6PD deficiency screen was sent to the laboratory. His methemoglobin level remained unchanged after 1 dose of methylene blue the night before and 2 additional units of PRBCs throughout the day. The decision was made to give a second dose of methylene blue 0.75 mg/kg the evening of hospital day 3.
Throughout the next few hospital days the methemoglobin level fell slowly. By hospital day 8, it was less than 1% and remained there throughout the remainder of his stay (Figure 1). Hemolytic anemia also occurred during hospital days 3 to 8, for which he was transfused a total of 12 units of PRBCs (Figure 2). The remainder of his course was significant for worsening septic shock, which was thought to be secondary to C difficile colitis and health care–associated pneumonia. He was treated with intravenous immunoglobulin for his C difficile colitis. He had multiple endotracheal aspirate cultures that grew both Pseudomonas aeruginosa and Aspergillus fumigates, for which he was treated with cefepime and voriconazole, respectively. He continued on continuous renal replacement therapy as well as norepinephrine and vasopressin until hospital day 15. On hospital day 15, he required increasing vasopressors, including significant doses of norepinephrine, vasopressin, phenylephrine, and dobutamine with only temporary improvement in blood pressure. A Do-Not-Resuscitate order was signed in the early morning of hospital day 16, and the patient died shortly thereafter.
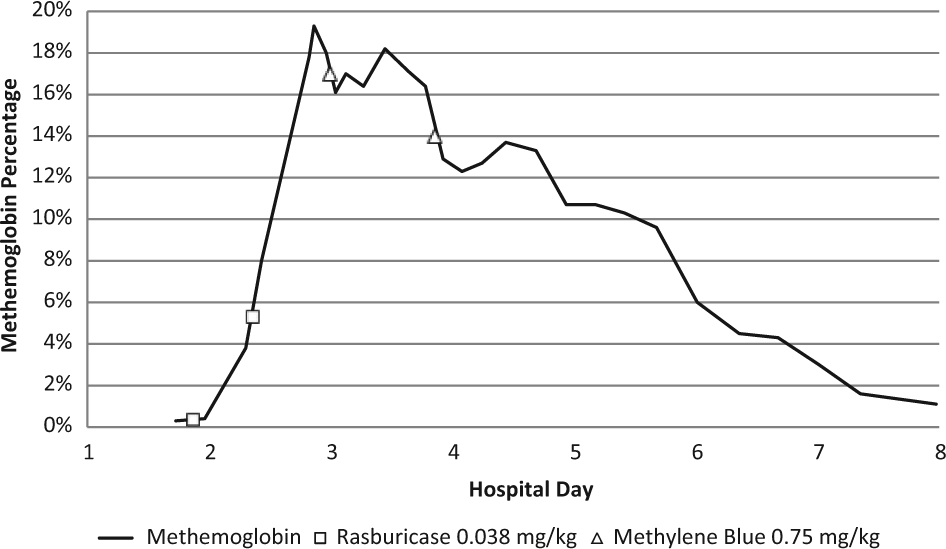
Methemoglobin concentration with timing of rasburicase and methylene blue: this figure illustrates the timing of the administration of rasburicase, the subsequent methemoglobinemia, and the administration of methylene blue.
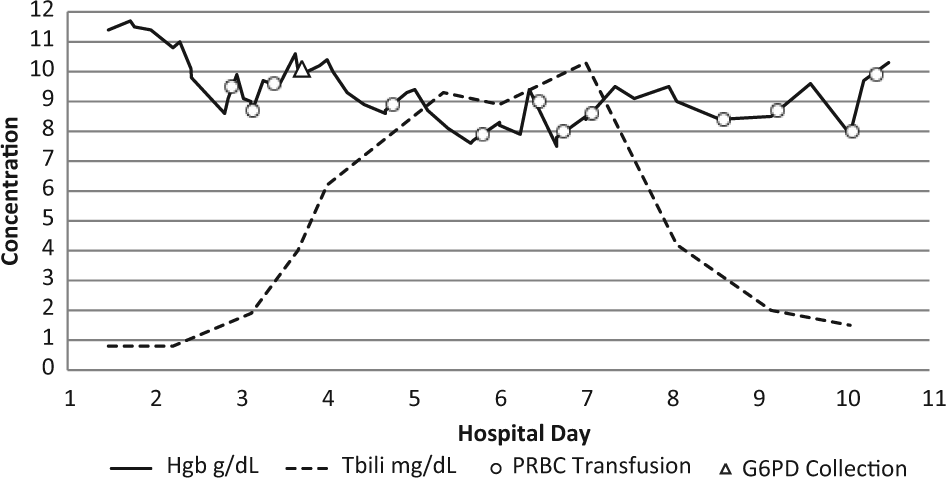
Hemoglobin, bilirubin, PRBC transfusions, and G6PD screen collection: this figure illustrates the collection of the G6PD screen after the recent infusion of 3 units of PRBCs. It also shows a rise in total bilirubin, which signifies hemolysis, which could have been exacerbated by the use of methylene blue in this patient who was likely G6PD deficient.
Discussion
Methemoglobinemia occurs when the iron moiety in hemoglobin is oxidized from the ferrous (Fe2+) to the ferric (Fe3+) state. 18 Methemoglobin is not able to bind oxygen, increasing the risk of tissue hypoxia and ischemia. Significant methemoglobinemia is typically circumvented by cytochrome b5 reductase using nicotinamide adenine dinucleotide (NADH) as a cofactor to reduce methemoglobin to hemoglobin. This pathway accounts for 95% of methemoglobin reduction. 19 A second pathway uses nicotinamide adenine dinucleotide phosphate (NADPH) as a cofactor. NADPH is the reduced form of NADH, which requires G6PD as a cofactor during production. This pathway normally accounts for 5% of methemoglobin reduction; however, it can be activated by exogenous factors such as methylene blue to increase its activity. Patients with G6PD deficiency cannot use this pathway because they are unable to produce NADPH (Figure 3).
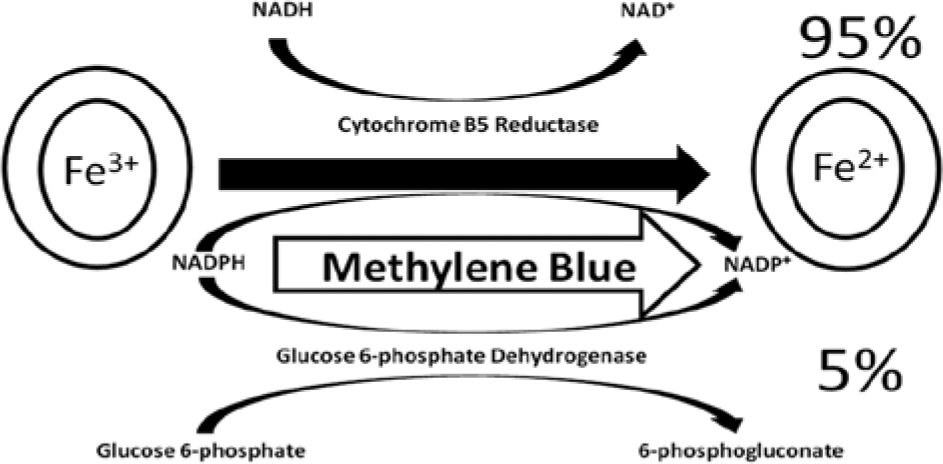
Two pathways to reduce methemoglobin: this figure illustrates the primary and secondary pathways for the reduction of methemoglobin. The cytochrome B5 reductase pathway accounts for 95% of normal methemoglobin production. The G6PD-mediated pathway only accounts for 5% of normal methemoglobin reduction, but its productivity can be increased with the use of methylene blue. Methylene blue is not effective in those with G6PD deficiency because this pathway does not exist without G6PD.
Methylene blue is typically recommended when the methemoglobin concentration is >20% and the patient is exhibiting symptoms of hypoxia. However, if the concentration is >30%, the patient should be treated regardless of symptoms. The typical dose is 1 to 2 mg/kg given intravenously. Additional doses can be given after an hour if there is no improvement in oxygenation; however, doses of more than 7 mg/kg have been shown to paradoxically worsen hypoxia. Furthermore, methylene blue is not effective as an antidote in patients with G6PD deficiency because the NADPH pathway is effectively absent. Methylene blue may act as an oxidizing agent itself in these patients and worsen methemoglobinemia. 20
Most commonly, acquired methemoglobinemia occurs after exposure to an exogenous oxidizing agent such as rasburicase. When rasburicase reduces uric acid to allantoin, hydrogen peroxide is formed as a by-product. 1 Humans do not have endogenous urate oxidase, and therefore, this represents a step in the catabolic pathway that does not normally occur in humans. 21 The catalyst for the reduction of hydrogen peroxide to water is dependent on glutathione. Glutathione is generated by NADPH, and the synthesis of NADPH is dependent on G6PD. Therefore, those with G6PD deficiency have decreased defense against free radicals and are at increased risk of developing rasburicase-induced hemolytic anemia and methemoglobinemia. 22
G6PD deficiency is the most common enzyme deficiency in the world and is common among males of African, Mediterranean, or Southeast Asian descent. This distribution mimics the endemicity of malaria and is thought by some scientists to be an evolutionary strategy to resist the disease. 23
The gene that codes for G6PD is located on the X chromosome; therefore, males are either hemizygotes and deficient or have normal G6PD because they carry a single X chromosome. 24 Women may be homozygotes for abnormal G6PD and express deficiency, but this is quite rare. More often, women are heterozygotes and, phenotypically, will have a mix of G6PD-deficient and normal erythrocytes because of random X chromosome inactivation. Using quantitative laboratory testing, most heterozygous women will test in the intermediate range. Clinically, heterozygous women may experience mild hemolytic anemia; however, most will be asymptomatic. 25 Testing for G6PD deficiency can be done with a qualitative or quantitative test. The qualitative test will not detect those with intermediate deficiency. 24
Although our patient had a negative G6PD deficiency screen, we feel that there is a high probability that he in fact was deficient and that this occurrence of methemoglobinemia and subsequent hemolytic anemia was induced by an overwhelming amount of hydrogen peroxide from the oxidation of uric acid. This reaction also may have been exacerbated by 2 doses of methylene blue. Unfortunately, our patient was tested during active hemolysis, which is not recommended primarily because the immature erythrocytes being generated contain more G6PD than mature erythrocytes. 24 Our patient also received 3 units of PRBCs in the previous 24 hours prior to the collection of the sample, and these units of PRBCs would most likely have normal G6PD activity. Finally, the test used was a qualitative test, which would not detect an intermediate result, which may have been present as a result of exogenous and young red blood cells. 25
To better understand this adverse drug reaction and its association with G6PD deficiency, we performed a literature search (MEDLINE 1990-June 2013) using the search terms rasburicase and methemoglobinemia. A total of 10 published cases between 1997 and 2012 were collected and are summarized in Table 1. They were all in male patients who were 6 to 62 years of age who received rasburicase for hyperuricemia. There were 7 cases that reported race of the patient, and 4 out of 7 patients were African American. It was noted that 7 patients were being treated for hematologic malignancies and developed TLS from chemotherapy, but 2 patients developed hyperuricemia for other reasons.10,11 Out of 8 patients who were tested, 6 were G6PD deficient. All but 2 patients received the approved dose of 0.2 mg/kg of rasburicase. Peak methemoglobin levels ranged from 8.0% to 21.5%, and hemolytic anemia developed concurrently in 5 out of 8 cases. The treatment of these patients was generally supportive with oxygen and PRBCs. Only 2 patients received methylene blue,11,12 and 1 received ascorbic acid. 15 Most patients recovered quickly and had mild symptoms from methemoglobinemia and hemolysis. All survived to hospital discharge.
Identified Published Cases of Rasburicase-Induced Methemoglobinemia.
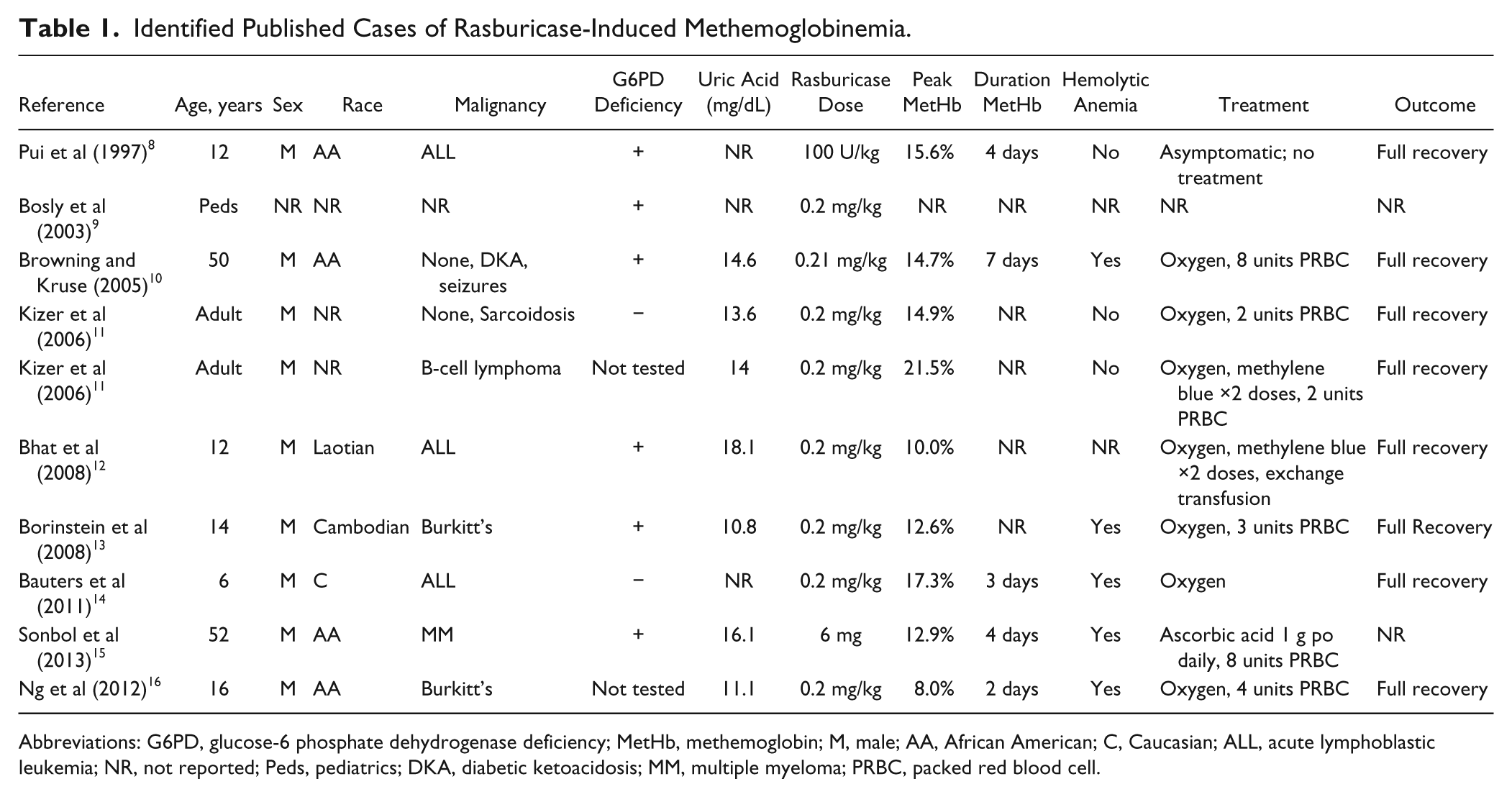
Abbreviations: G6PD, glucose-6 phosphate dehydrogenase deficiency; MetHb, methemoglobin; M, male; AA, African American; C, Caucasian; ALL, acute lymphoblastic leukemia; NR, not reported; Peds, pediatrics; DKA, diabetic ketoacidosis; MM, multiple myeloma; PRBC, packed red blood cell.
Our case was unique compared with most of the reported cases of rasburicase-induced methemoglobinemia. Our patient received a much smaller dose of rasburicase compared with patients in other cases because our institution has had good results with limiting the dose to 3 mg in adult and pediatric patients. It is common for a repeat dose to be given if the uric acid has not improved within 12 to 24 hours. Our patient tested negative for G6PD deficiency, although he was tested during active hemolysis and had received 3 units of PRBCs within 24 hours of the sample collection. Both these can result in false-negative results. Our patient developed several complications during his stay, including acute renal failure, health care–associated pneumonia, and C difficile–associated diarrhea along with his methemoglobinemia and hemolytic anemia. He eventually died from these complications. It is difficult to discern if this adverse drug reaction played a large role in the patient’s hospital course and ultimate death, although it did make his course more complicated. Direct consequences of this adverse drug reaction included intubation, methylene blue administration, and blood transfusion. All of these interventions could have contributed to his further decompensation.
It is important for clinicians to be aware of how to test appropriately for G6PD deficiency and when it is appropriate to administer methylene blue in cases of methemoglobinemia. Patients who test positive for G6PD deficiency should not be treated with rasburicase for TLS. Allopurinol is a logical choice for these patients. African American men who have not been tested for G6PD deficiency and experience rasburicase-induced methemoglobinemia should be considered G6PD deficient until they can be appropriately tested. Methylene blue should not be administered to G6PD-deficient patients or those with a high pretest probability.
Conclusion
Rasburicase-induced methemoglobinemia is a rare adverse drug reaction seen most often in G6PD-deficient patients. Our patient is the first reported mortality following this reaction in an adult patient. G6PD testing should not be ordered during active hemolysis or after blood transfusion because this may lead to false-negative results. Treatment is generally supportive with oxygen and blood transfusion. Methylene blue should not be used as an antidote because it may cause hemolytic anemia in patients with G6PD deficiency.
Footnotes
Authors’ Note
This article has not been presented in another forum at a meeting.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.