
Abstract
Keywords
Dystonias are intermittent and sustained muscle spasms and abnormal postures that can be acute or chronic. They are most likely to occur in the eye, face, neck, and throat muscles, but can occur in any skeletal muscle group. 1 In 1972 an acute dystonia was described during treatment with methylperone (a butyrophenone related to haloperidol) in 3 elderly women. 2 The dystonia experienced by these women was characterized by a sustained, abnormal posture with flexion of the body and head to one side plus axial rotation of the trunk and is now known as pleurothotonus, or more commonly as Pisa syndrome, so named because the abnormal posture resembles the Leaning Tower of Pisa. 3 This abnormal posture is secondary to persistent dystonia of the cervical or lumbar musculature and worsens during sitting or walking.3,4 The patient is frequently unaware or indifferent to the abnormal posture. This adverse drug reaction is considered relatively uncommon; most of the literature is case reports,5 -14 and a multicenter drug safety project found the rate of Pisa syndrome after treatment with antipsychotics to be 0.06%, caused most frequently by typical antipsychotics. 4 However, a population study examining newly admitted psychogeriatric patients described a prevalence rate of 8.3% (N = 133), suggesting the reaction may be more prevalent in geriatric patients. 15 Various cases of Pisa syndrome have demonstrated that the adverse effect may be a subtype of either acute or tardive dystonia with a mean initial onset of 14.2 years (range 3 months-41 years) after exposure to antipsychotic medications. 16
The pathophysiology of Pisa syndrome is poorly under-stood, but is proposed to involve dopaminergic-cholinergic imbalance, along with serotonergic and/or noradrenergic interactions with dopamine.3,5 Agents reported to cause Pisa syndrome include antipsychotics, tricyclic antidepressants (TCAs), cholinesterase inhibitors, and phenothiazine antiemetic drugs.3 -5 Patients at higher risk for developing Pisa syndrome include those receiving prolonged antipsychotic therapy, females, the elderly, and those with organic brain changes.2 -4
There is no well-defined clinical definition or diagnostic criteria for Pisa syndrome. A diagnosis of Pisa syndrome is presumed when a patient taking a neuroleptic medication develops the characteristic abnormal posture and indifference to the abnormal posture. 3 Causes by other psychiatric conditions (eg, catatonia), neurologic diseases causing dystonia, and other extrapyramidal symptoms must be excluded. In addition, there is no standard treatment recommendation for Pisa syndrome because different strategies have been used with varying success. Some benefits have been observed from the addition of anticholinergic medications with up to 40% (9 of 21) of patients in one report showing improvements; however, only Japanese patients composed the study population and it is possible that other ethnicities may not be as responsive to anticholinergic medications. 13 Other strategies implemented for improvement of Pisa syndrome include discontinuing the offending medication or reducing the dose.
Case Report
Pisa syndrome developed in a 31-year-old, 75.9-kg (body mass index 27 kg/m2), white male with pervasive developmental disorder and multiple sclerosis (MS). The patient had been hospitalized in locked psychiatric facilities since the age of 15 years because of impulsivity, aggression, and severe sexually inappropriate behaviors that made it difficult for him to function appropriately in an outpatient setting. MS was diagnosed when the patient was aged 19 years. MS initially presented with an unsteady gait and declining cognitive function, followed by development of bilateral optic neuritis and generalized muscle weakness, both of which resolved. He had multiple magnetic resonance imaging (MRI) studies and physical therapy sessions for MS that showed no abnormalities in spinal curvature until 2009, when a slight kyphosis was noticed. Early MRIs showed nonspecific white matter changes and later white matter lesions suspicious for MS; a recent MRI showed improvement.
Per available records, the patient had been receiving varying doses of risperidone for most of the past 11 years for disruptive behaviors associated with pervasive developmental disorder. Throughout this time, he was transferred multiple times between psychiatric facilities because of conflicts with peers and sexually inappropriate behavior. Risperidone was initiated at 2 mg at bedtime with variable dosing over 4 years and a maximum total daily dose of 4 mg. The patient was treated concurrently with clomipramine for obsessive-compulsive behaviors for approximately 1 year with a maximum daily dose of 300 mg. After 4 years, the patient had an antipsychotic drug holiday of approximately 14 months. He then had a brief trial of risperidone (<1 week), followed by 17 months of quetiapine. Quetiapine was discontinued and risperidone was restarted at 0.5 mg daily, eventually reaching a maximum total daily dose of 4 mg after 7 months of titration. This dose was maintained for approximately 4 years, and then was increased to 6 mg. Other scheduled medications during this time included atenolol 50 mg daily, divalproex sodium 1250 mg daily, docusate 100 mg daily, glatiramer 20 mg daily, hydrochlorothiazide 25 mg daily, meclizine 12.5 mg 3 times daily, and a multivitamin daily.
Approximately 1 week after the increase in risperidone dose, physical therapy notes described an ataxic gait with a significant lean to the left when the patient was sitting or walking. Physical therapy was not able to continue treatment because the patient’s posture was significantly affecting his safety during the exercises. The patient was referred to neurology for possible worsening of MS. During a neurology appointment 3 weeks later, he was noted to ambulate with his spine concave to the left and his right hip rotated slightly forward. He also leaned to the left during a tandem walk and when sitting in a chair. The patient was indifferent to the lean and did not report pain or discomfort unless he attempted to straighten his posture. There was no evidence of other extrapyramidal symptoms and no medication changes were recommended by neurology. The neurologist noted that the cause of the lean was unclear and ordered an MRI to further evaluate the progression of MS. The results of this MRI were unchanged from previous ones and showed nonspecific white matter changes consistent with MS. His disease progress was noted as “unchanged.” Recommendations from neurology were to continue current treatment, including daily exercise and gait training. Pisa syndrome was not suspected.
After the neurology appointment, clomipramine 25 mg daily at bedtime was prescribed for treatment of obsessive-compulsive symptoms. Over the course of 6 months, the patient’s lean continued to be present, and several medication changes occurred. Atenolol was decreased from 50 mg daily to 25 mg daily, hydrochlorothiazide was increased from 25 mg daily to 50 mg daily, and clomipramine was titrated from 25 mg daily to 100 mg daily. Two months after clomipramine was increased to 100 mg daily and 6 months after the patient’s lean was documented, risperidone was tapered to discontinuation and lurasidone 40 mg daily was started due to lack of improvement in psychiatric symptoms. All other medications remained the same. Five days after discontinuation of risperidone, the neurologist noted the patient’s posture was improving, with only an occasional tendency to lean to his left and improved overall balance. One week after discontinuation of risperidone and within days of an increase in clomipramine to 200 mg daily at bedtime, the patient no longer leaned to the left when standing or walking. At this time, a diagnosis of Pisa syndrome was presumed. Because the adverse event has been associated with both risperidone and clomipramine, the Naranjo probability scale 17 was used to determine the likelihood of causation for each medication. It was determined that risperidone was a probable cause of the patient’s abnormal posture and clomipramine was a possible cause.
After an 11-day trial of lurasidone 40 mg daily, the medication was discontinued due to worsening of the patient’s psychiatric symptoms and chlorpromazine 50 mg twice daily was initiated. Chlorpromazine was chosen due to its multiple daily dosing (thereby ensuring consistent interactions with nursing staff), sedative effects, and lower propensity to cause movement disorders compared to higher potency typical antipsychotics. The chlorpromazine dose was increased after 3 days to 100 mg 3 times daily. Three months later, chlorpromazine was increased further to 200 mg 3 times daily. Approximately 2 months after this dose was achieved, the patient’s leaning had returned and was documented by physical therapy. The only other medication change during this time was a decrease in clomipramine from 200 mg to 150 mg daily at bedtime, secondary to sexual dysfunction, approximately 1 month before the final dose increase in chlorpromazine. On follow-up, physical therapy noted that the patient exhibited winging of his left scapula, had a strong tendency to lean to the left, and walked quickly with a left trunk lean. The Naranjo probability scale 17 determined that chlorpromazine was a probable cause of the patient’s leaning.
At time of writing, chlorpromazine had been continued at 200 mg 3 times daily and the patient continued to exhibit symptoms of Pisa syndrome while sitting and standing. He remained indifferent to the lean and did not report pain or discomfort. Although reduction in dose or discontinuation of the antipsychotic can lead to resolution of Pisa syndrome, continuation of chlorpromazine therapy can be justified because the regimen was controlling the patient’s severe sexually inappropriate and disruptive behaviors. Anticholinergic medications such as trihexyphenidyl and benztropine have been used to treat Pisa syndrome. However, chlorpromazine and clomipramine have a considerable anticholinergic burden and anticholinergic medications have shown mixed results in improving symptoms; therefore, a trial of an anticholinergic medication could increase adverse effects to an unacceptable degree. This had not been attempted in our patient secondary to a history of longstanding constipation and multiple falls. In this patient, the risk of causing additional anticholinergic adverse effects or worsening of impulsivity and sexually inappropriate behaviors must be weighed against the benefit of improving dystonia. The attending psychiatrist had not attempted to reduce the dose of chlorpromazine or switch to an alternative antipsychotic due to concern that the patient’s condition would clinically deteriorate.
Discussion
A search of the literature identified 8 case reports of drug-associated Pisa syndrome: 5 with risperidone,6 -10 1 with paliperidone, 11 and 2 with chlorpromazine12,13 (Table 1). Four patients not presented in Table 1 (aged 20, 26, 29, and 60 years) experiencing chlorpromazine-induced Pisa syndrome were described within a case series. 13 All patients had chlorpromazine added to their current antipsychotic regimen (agents not reported), with 3 of the patients being exposed to a third antipsychotic (levomepromazine, haloperidol, or tiapride). These patients were all initially receiving trihexyphenidyl 6 mg/day; after development of Pisa syndrome, this dose was increased to 12 mg/day. Only one of the patients responded to the increased dose of trihexyphenidyl, with the remainder showing improvement in symptoms after a dose reduction of their antipsychotic.
Pisa Syndrome Cases Involving Risperidone, Paliperidone, and Chlorpromazine.
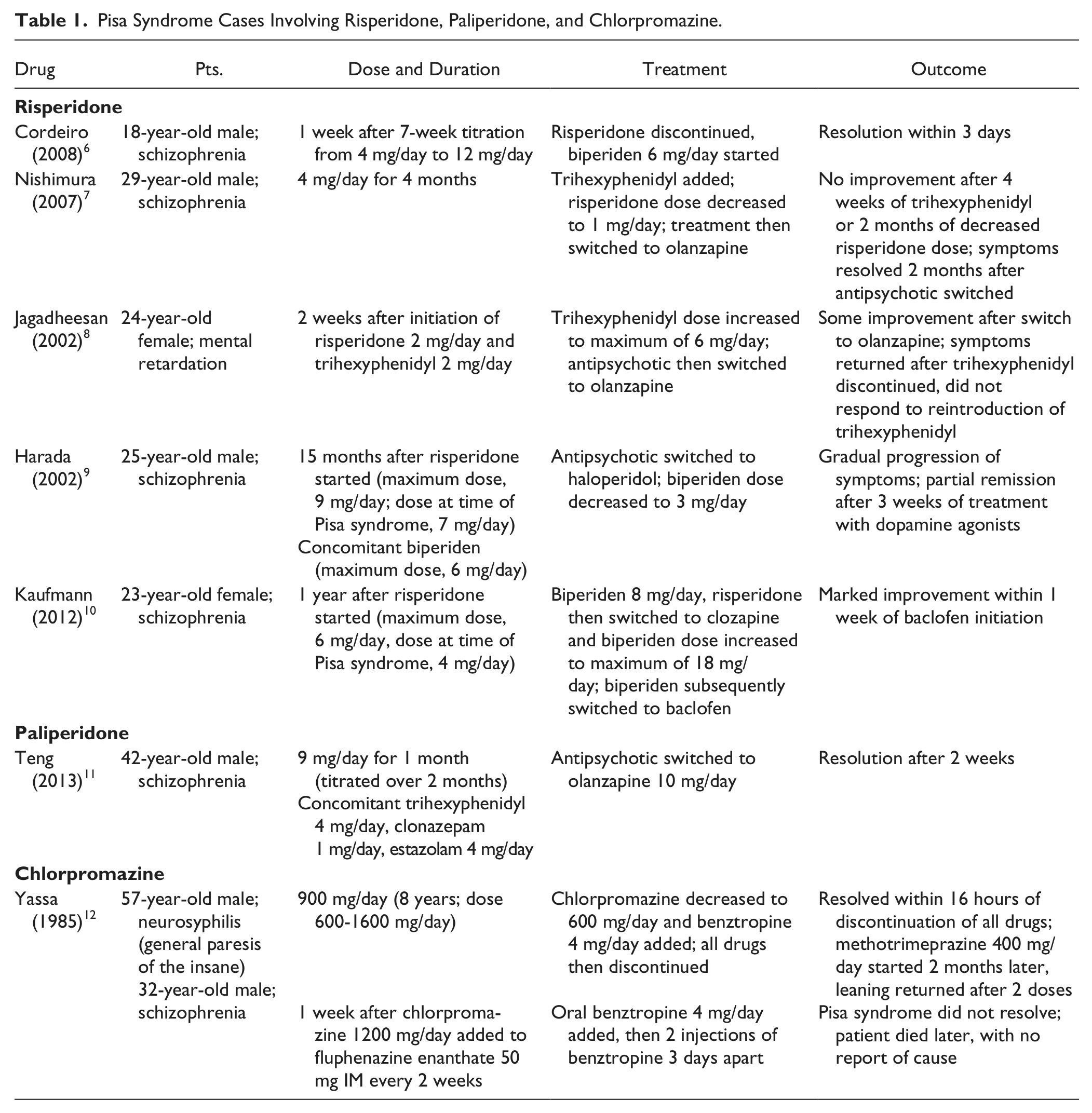
The age range of patients receiving risperidone, paliperidone, or chlorpromazine varied, with most being young adults, in contrast with the population study 15 that suggested Pisa syndrome may be more common in geriatric patients. Duration of therapy and titration schedules also varied, with some cases appearing months after a consistent dose and others appearing 1 week after a dose increase. Our patient was similar to many of the reports because he is a young adult and Pisa syndrome was noticed shortly after an increase in dose. For the risperidone cases, doses at the onset of symptoms ranged from 2 mg to 12 mg, with our patient falling in the middle of this range at 6 mg/day. Treatment strategies often involved switching to a different antipsychotic or adding an anticholinergic. One case noted worsening of Pisa syndrome after treatment was switched from risperidone to haloperidol plus biperiden (an anti-cholinergic medication). 9 A parallel to this case can be seen in our patient, who had a recurrence of Pisa syndrome after treatment was switched from an atypical antipsychotic (lurasidone) to a typical antipsychotic (chlorpromazine).
TCAs, such as clomipramine, also have been reported to cause Pisa syndrome.5,14 Suzuki et al. described a 58-year-old Japanese man with organic brain changes and major depressive disorder who developed Pisa syndrome while receiving 3 TCAs (amitriptyline 150 mg/day, imipramine 150 mg/day, and nortriptyline 150 mg/day). 5 The patient developed an abnormal posture resembling Pisa syndrome 2 days after an increase in the nortriptyline dose from 75 mg/day to 150 mg/day and approximately 3 weeks after initiation of this combination of antidepressants. Biperiden 6 mg/day was added and 4 days later the abnormal posture resolved. The antidepressant doses were not adjusted and the patient showed no signs of Pisa syndrome for the remainder of his hospitalization (~5 months). Clomipramine-induced Pisa syndrome was described in a 56-year-old woman. 14 Two months after beginning clomipramine 225 mg daily the patient developed symptoms of Pisa syndrome. The dose of clomipramine was reduced to 75 mg daily and 2 weeks later the patient’s posture began to improve. Symptoms of Pisa syndrome resolved 1 month after the decrease in the dose. In contrast, our patient was not receiving clomipramine at the initial onset of Pisa syndrome, Pisa syndrome resolved shortly after an increase in clomipramine dose, and the second occurrence developed after a reduction in the clomipramine dose.
Our patient also was receiving divalproex sodium throughout the time reported here. Two case reports linked Pisa syndrome to valproic acid; however, in both cases the patients were receiving other medications that could have led to dystonia.18,19 The first case described a 65-year-old wheelchair-bound man whose condition was stable with valproic acid 750 mg twice daily, carbamazepine 200 mg twice daily, and risperidone 3 mg twice daily for many months. 18 He developed Pisa syndrome, which resolved immediately after discontinuation of valproic acid. The second case described a 67-year-old male with Huntington disease whose condition was stable with olanzapine 10 mg/day and paroxetine for 2 years, after which rivastigmine 3 mg/day and valproic acid 500 mg twice daily were added. 19 Within days of this addition, the patient developed Pisa syndrome, which resolved within 1 week of discontinuation of valproic acid. The lack of case reports with divalproex sodium, as well as the resolution and recurrence of symptoms in our patient while there was no change in the divalproex sodium dose, leads us to believe that this drug was not responsible for Pisa syndrome in our patient (possible association according to the Naranjo probability scale 17 ).
As with other adverse reactions, pharmacokinetic and pharmacodynamic drug interactions may play a role in the development of Pisa syndrome. Our patient was receiving multiple medications that have been reported to cause Pisa syndrome during each occurrence of the adverse drug reaction. A multicenter drug safety project reported that all 20 cases of Pisa syndrome identified by the project involved polypharmacy, leading the authors to list combined pharmacologic treatment as a risk factor for developing Pisa syndrome. 4 These data are limited, however, because they do not provide details on combinations of medications, specifically whether any cases involved polypharmacy with multiple agents reported to cause Pisa syndrome. To our knowledge, there are no published data on whether concomitant use of multiple agents reported to cause Pisa syndrome puts patients at an increased risk, although there are case reports involving more than one causative agent. The authors of the first reported case of valproic acid–induced Pisa syndrome proposed that the adverse drug reaction could have been caused solely by valproic acid or secondary to a pharmacodynamic interaction between valproic acid and risperidone. 18 The use of multiple causative agents as a risk factor for developing Pisa syndrome warrants further investigation. Risperidone, chlorpromazine, and clomipramine are major substrates of the CYP2D6 isoenzyme, whereas divalproex sodium is primarily metabolized through pathways other than cytochrome P450.20 -22 Clomipramine is also an inhibitor of CYP2D6 and could cause an increase in serum concentrations of risperidone or chlorpromazine. 21 It has been reported that chlorpromazine inhibits the metabolism of valproic acid due to an unknown mechanism 23 ; however, our patient’s valproic acid concentration did not increase significantly after the addition of chlorpromazine (109 mg/L at admission, 80 mg/L 5 months after admission, 92 mg/L 12 months after admission and 2 months after the final chlorpromazine dose increase). We did not monitor drug concentrations for the patient’s other medications. Therefore, we cannot rule out the possibility of a pharmacodynamic or pharmacokinetic interaction that led to additive effects or increased concentrations of risperidone, clomipramine, or chlorpromazine, which in turn led to development of Pisa syndrome.
Organic brain changes are associated with an increased risk of development of Pisa syndrome. As seen in multiple MRIs, our patient had white matter changes due to MS that may have put him at higher risk for developing Pisa syndrome. To our knowledge, no case reports of Pisa syndrome in patients with MS have been published. There are case reports of paroxysmal dystonia in patients with MS; however, this dystonia presents differently than that seen in Pisa syndrome. Case reports describe the paroxysmal dystonia in MS as brief (30 seconds-2 minutes) episodes of dystonia that recur multiple times daily.24 -27 This dystonia is also referred to as tonic spasms and often involves multiple muscle groups including the face, neck, elbow, wrist, and leg. It can be triggered by stress, hyperventilation, or voluntary movement.24,27 In comparison, Pisa syndrome involves only the trunk and is not characterized by multiple brief episodes. Pisa syndrome does not recur and remit throughout the day and is not triggered; rather, it remains constant and has a more gradual course of improvement after the offending medication has been discontinued. The presentation of dystonia in our patient more closely resembles that of Pisa syndrome. There is no definitive link between MS and other types of dystonia. 27
It is important to recognize Pisa syndrome at initial presentation to formulate a feasible plan for medication adjustment to reduce progression and social stigmatization. The risk of changing the medication regimen may outweigh the benefit of improving the dystonia in this patient; however, an attempt to resolve the adverse drug reaction would be warranted in the majority of patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.