
Abstract

TO THE EDITOR: We read with great interest the study by Kane et al 1 evaluating multiple equations to correct total phenytoin levels in neurointensive care patients. This study is to be commended for its large sample size and focus on critically ill patients, who have multiple reasons for altered phenytoin concentrations. They found the traditional Winter-Tozer (WT) equation significantly underpredicted patients’ actual free phenytoin concentrations and concluded it is not appropriate to use in this population. They found greater correlation between predicted and actual free phenytoin concentrations with a modified WT equation and an equation developed through multivariate analysis.
Previous studies evaluating the WT equation’s predictive ability have shown mixed results.2-4 We conducted an analysis of internal data in our neurointensive patient population to see how patient’s phenytoin binding changes throughout their stay. Our cohort included 100 patients and 556 paired total and free phenytoin concentrations. The average free fraction of phenytoin in our group was 18.8% and the average albumin was 2.7 g/dL.
Following the results from Kane et al, 1 we applied the 3 equations used (WT, multivariate liner regression model, and modified WT coefficient) to our data in an attempt to validate their results. We applied these equations to each patient’s first phenytoin concentrations and albumin level as Kane et al did (group 1, n = 92), then to the patient’s phenytoin concentrations and albumin levels throughout their entire intensive care unit stay (group 2, n = 312). Surprisingly, we found the traditional WT equation had the greatest correlation when compared with the other 2 equations, and overall, all 3 equations correlated poorly with actual free phenytoin concentrations (see Table 1).
Comparison of Free Phenytoin Predictive Equations.
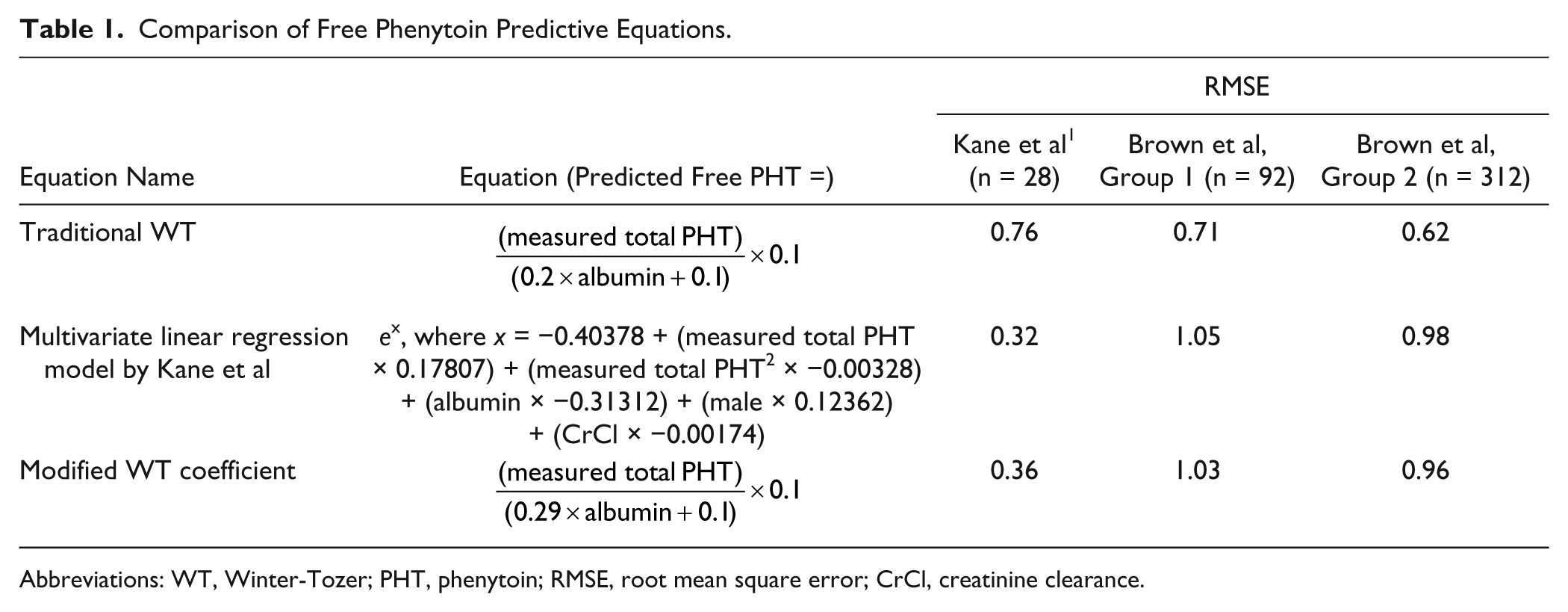
Abbreviations: WT, Winter-Tozer; PHT, phenytoin; RMSE, root mean square error; CrCl, creatinine clearance.
These markedly different results may be because of differences in study design and baseline demographics. Our data are from the patients’ entire stay in the neurointensive care unit (each patient had multiple phenytoin concentrations) versus within the first 24 hours of admission as Kane et al used. Also, our patients had a mean albumin of 2.7 g/dL versus a mean albumin of 3.3 g/dL in Kane et al’s group.
Overall, we agree with Kane et al’s idea of developing new predictive equations accounting for other variables in addition to albumin. Both our results have shown that the WT equation is not reliable in neurointensive patients. Future studies evaluating predictive phenytoin equations should include a variety of variables in their analysis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.