
Abstract
To maximize treatment outcomes, patients receiving warfarin therapy must maintain the intensity of their anticoagulation in a narrow therapeutic range. Deviations outside this range increase the risk of either thromboembolic or hemorrhagic complications. 1 Time in therapeutic range (TTR) is used as a correlate for the quality of anticoagulation control and has been shown to predict both thromboembolic and hemorrhagic events. 1 Despite more than 50 years of clinical use and subsequent related research, most patients are out of their optimal therapeutic range a third of the time, with both system- and patient-specific factors having been identified as having an influence on TTR. 2
Patients in whom chronic warfarin therapy is indicated often have multiple chronic medical conditions (eg, atrial fibrillation, hypertension, heart disease, and stroke), which have been shown to increase the risk of developing depressive disorders.3-7 For example, major depression occurs in approximately 1 in 5 patients hospitalized for acute myocardial infarction. 8 In addition, patients with severe mental illness (bipolar disorder, schizophrenia, etc) have an elevated risk for cardiovascular mortality. 9 The reasons for this increased risk are multifaceted and involve interactions between physiological, behavioral, and psychosocial domains. 10
Patients with depression or other forms of psychiatric disorders often struggle with adherence and may self-discontinue medications without consulting their health care providers.11-14 To our knowledge only 1 study to date has specifically addressed the use of warfarin in patients with any form of psychiatric disorder. 15 This relatively small study (n = 62) of patients who had recently undergone aortic valve replacement showed that patients with depression had statistically significantly lower rates of adherence to scheduled clinic appointments and prescribed drug therapy. There were several limitations to this study, including its relatively small sample size and poor external validity because it only included patients who had recently undergone heart valve replacement surgery. Because of the paucity of generalizable data in this patient population, we chose to further examine these relationships. The purpose of our study is to examine the effects of depression and/or other psychiatric disorders on anticoagulation control in a pharmacist-managed clinic setting, where patients receive anticoagulation for a variety of indications. We hypothesize that patients with a history of depression or other psychiatric disorders have decreased anticoagulation control and thus are at higher risk for complications.
Methods
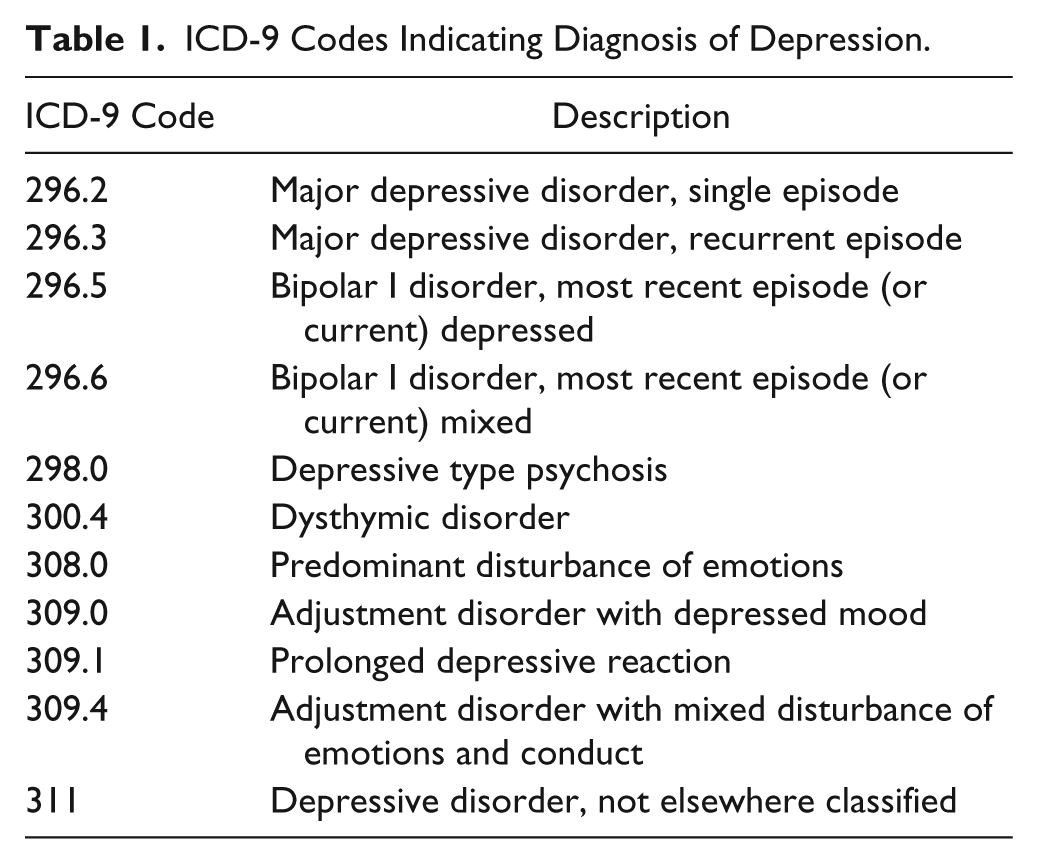
All anticoagulation clinic records of adult patients (19 years or older) receiving warfarin therapy who were referred to the pharmacist-managed anticoagulation clinics at Broadlawns Medical Center in Des Moines, Iowa, over a 24-month period (ending September 1, 2009) were retrospectively reviewed. Records were excluded if patients did not have at least 2 INR measurements during the study period or were referred but not managed by the clinic (eg, did not present to the clinic following referral). Records were screened via the electronic medical record (MEDITECH, Circle Westwood, MA) for the diagnosis of depression or other psychiatric disorders using both ICD-9-CM codes and through confirmatory documentation in the medical record. A diagnosis of depression included diagnostic codes of 296.2 to 296.3, 296.5 to 296.6, 298.0, 300.4, 308.0, 309.0 to 309.1, 309.4, and 311 (see Table 1). Psychiatric disorders excluded from the control group include any ICD-9-CM diagnostic code from 290 to 319, with the exception of tobacco use disorder (305.1).
ICD-9 Codes Indicating Diagnosis of Depression.
Data elements extracted from the medical record for each patient included basic demographic information, indication for anticoagulation, INR goal range, planned duration of therapy, documentation of a diagnosis of depression or any form of psychiatric disorders, use of psychiatric medications prescribed, duration of warfarin use prior to study period, documentation of thromboembolic or bleeding events, and all INR values over the study period. Bleeding events were defined as “major” or “minor.” Major bleeds were defined by the investigators as those events that required hospitalization, transfusion, or surgical intervention. Any other bleeding event reported to the clinic pharmacists or hospital staff was considered minor.
Statistical Analysis
The primary outcome measure was TTR, which was calculated using 3 methods. Three methods were chosen because each method has its own limitations and strengths, and reporting multiple outcome measures provides a more robust assessment of anticoagulation control.16,17 In addition, using 3 methods may allow for greater external comparison. The 3 methods that we chose included the proportion of INRs in goal range, a modified Rosendaal’s linear interpolation, and the percentage of patients with a mean INR (∑INR/Total number of INRs) in their goal range. Because the Rosendaal method assumes a straight line between 2 consecutive INRs it may under- or overestimate TTR when large gaps of time occur between INR measurements. 18 Thus, for our analysis, we modified the Rosendaal method for patients who had a time gap of greater than 60 days between any 2 INR measurements. These patients were considered to have “inconsistent” visits. Patients who had inconsistent visits had their blocks of uninterrupted INR visits (those that did not include 60 days between any 2 INRs) calculated separately and then weight averaged based on the proportion of total days in each block.
When calculating TTR, INRs measured during the first 30 days of therapy were excluded to account for the initial time it typically takes to find a consistent maintenance dose for most patients. Additionally, we excluded INRs that occurred around known planned interruptions (for procedures, etc) and other periods where discontinuation was intentional through 14 days after the day warfarin was restarted. We also excluded INRs taken during hospitalizations and up to 14 days after, if warfarin was held during hospitalization.
Continuous variables were analyzed using the Student t test. Nominal data were analyzed using the χ2 or Fisher’s exact test where appropriate. For the primary TTR outcomes, P values were adjusted using the Bonferroni method for multiple comparisons as well as presented as unadjusted. All TTR calculations were performed using a Microsoft Excel database, except Rosendaal’s method. Rosendaal’s method was carried out with the assistance of the online anticoagulation Web site ClotFree (www.clotfree.com). Statistical analyses were performed using Minitab, version 16 (Minitab Inc, State College, Pennsylvania) and Excel, version 14 (Microsoft Office 2010, Microsoft Corp, Redmond, WA). The study protocol was approved by the institutional review board at Drake University.
Results
Over the index period, a total of 203 patients were referred to the pharmacist-managed anticoagulation clinic. Of these, 151 patients met the inclusion criteria, and 52 patients were excluded for a variety of reasons (see Figure 1). We included 79 patients (52.3%) in the control group because they carried no depressive or other psychiatric disorders (other than tobacco abuse). Among the rest, 72 patients (47.7%) had been diagnosed with at least 1 depressive or psychiatric disorder, and 45 patients (29.8%) had a depression diagnosis, of whom only 14 had a depression diagnosis with no additional psychiatric diagnoses. Overall, 3139 INRs were evaluated, and the total treatment time considered was 145 patient-years. The majority of patients were male (62.5%) and Caucasian (85.4%), with a mean age of 51.6 years. Patient characteristics were similar between groups (see Table 2); however, there was a larger proportion of black patients in the control group (16.5%) than in the group with psychiatric disorders (5.5%, P = .041). Indications for anticoagulation therapy included atrial fibrillation (31.1%), prior venous thromboembolic events (VTEs; 39.7%), mechanical valve replacement (9.3%), or other reasons (including embolic stroke, left ventricular thrombus, VTE prophylaxis, and arterial embolism; 28.5%). Also, 13 patients (8.6%) had multiple indications for anticoagulation therapy. Patients in the depressive (P = .004) and psychiatric disorder (P = .003) groups were significantly more likely to have a history of VTE than the control group. Most patients (73.6%) were prescribed long-term therapy, and nearly half (49.5%) had their therapy initiated during the study period. Complete demographic details can be found in Table 2.
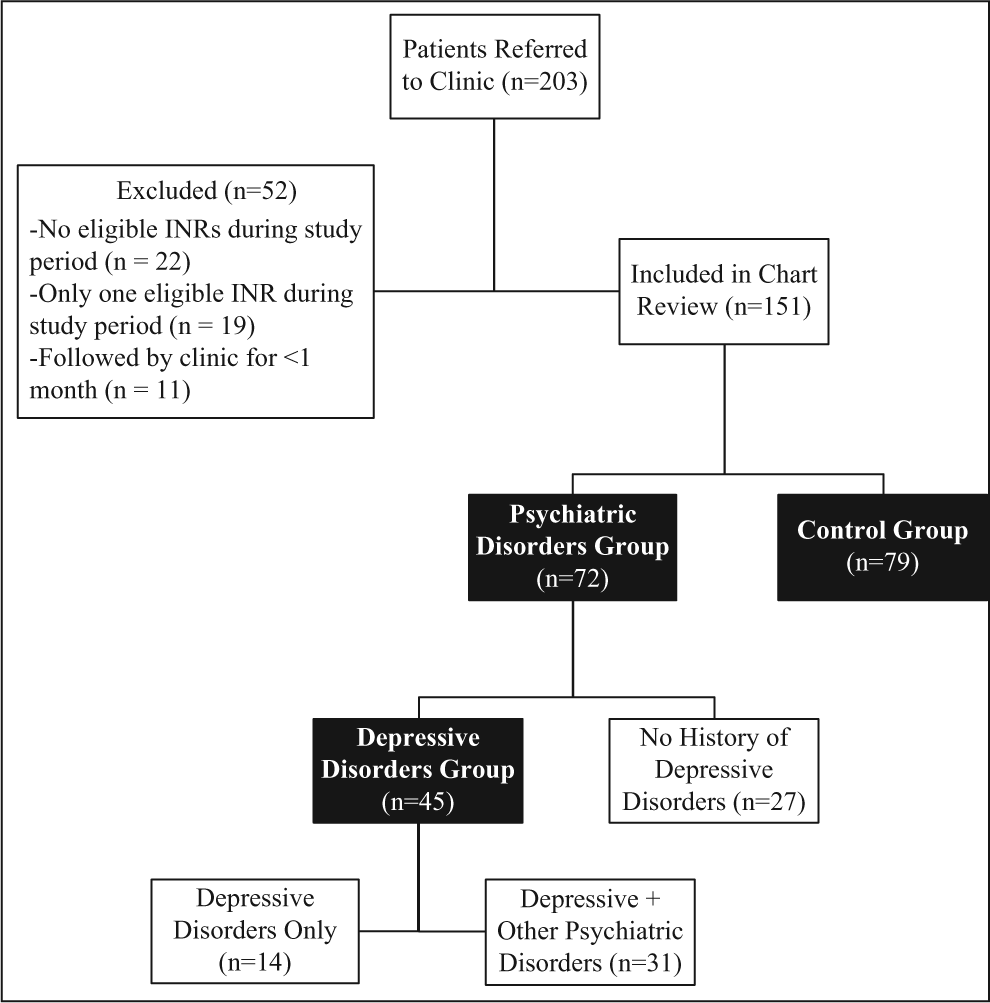
Study inclusion process.
Demographics. a .
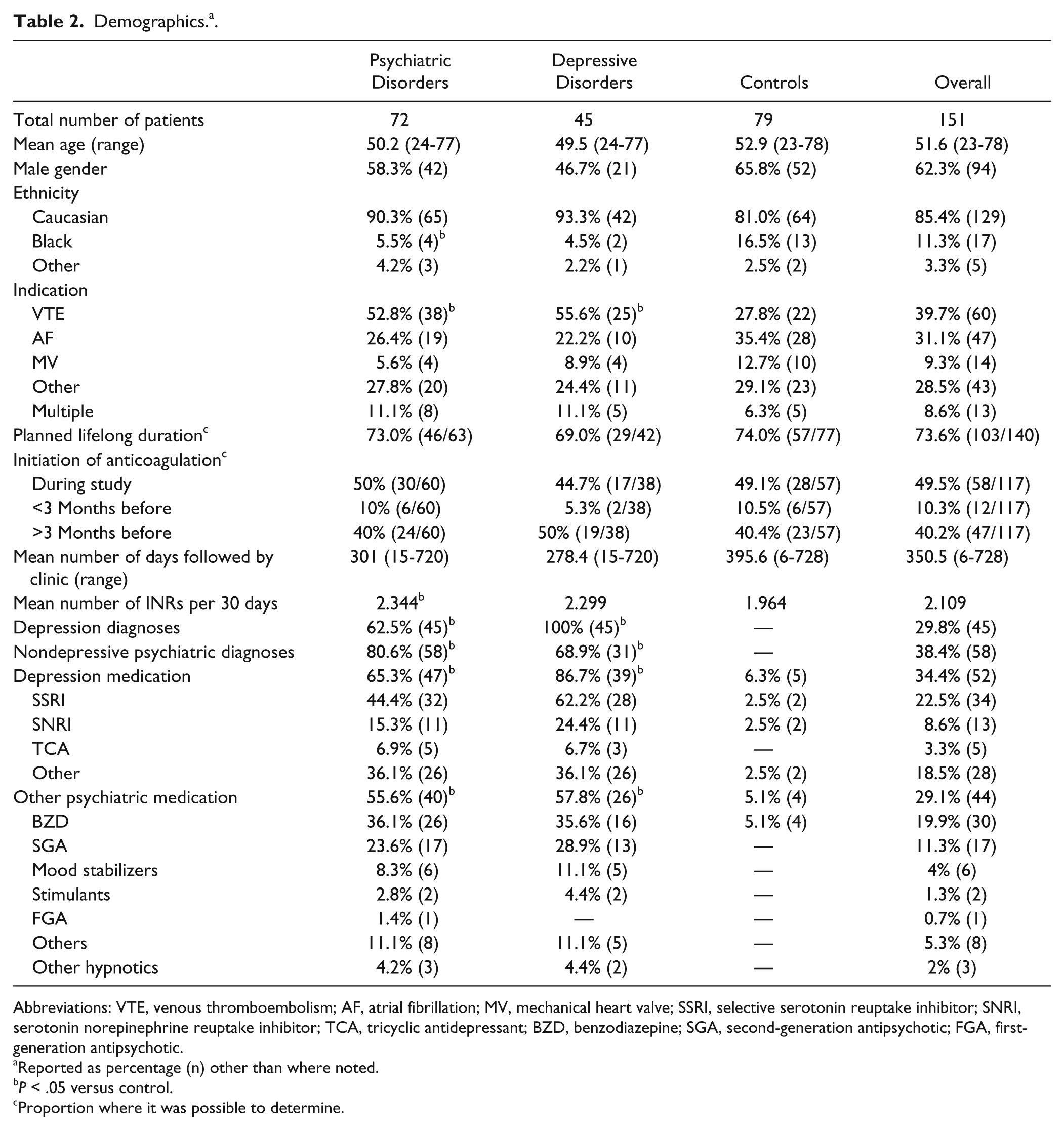
Abbreviations: VTE, venous thromboembolism; AF, atrial fibrillation; MV, mechanical heart valve; SSRI, selective serotonin reuptake inhibitor; SNRI, serotonin norepinephrine reuptake inhibitor; TCA, tricyclic antidepressant; BZD, benzodiazepine; SGA, second-generation antipsychotic; FGA, first-generation antipsychotic.
Reported as percentage (n) other than where noted.
P < .05 versus control.
Proportion where it was possible to determine.
Antidepressant use was common among those with depression and those with psychiatric disorders (86.7% and 65.3%, respectively) and relatively rare within the control group (6.3%). Similar patterns could be seen with other psychiatric medications (see Table 2). More than half of the patients in the groups with depression and psychiatric disorders were taking psychiatric medications (57.8% and 55.6%, respectively), whereas only 5.1% of the control group took any form of psychiatric medications other than antidepressants. Diagnoses of the psychiatric disorders group can be found in Table 3.
Diagnoses in the Psychiatric Disorders Group. a .
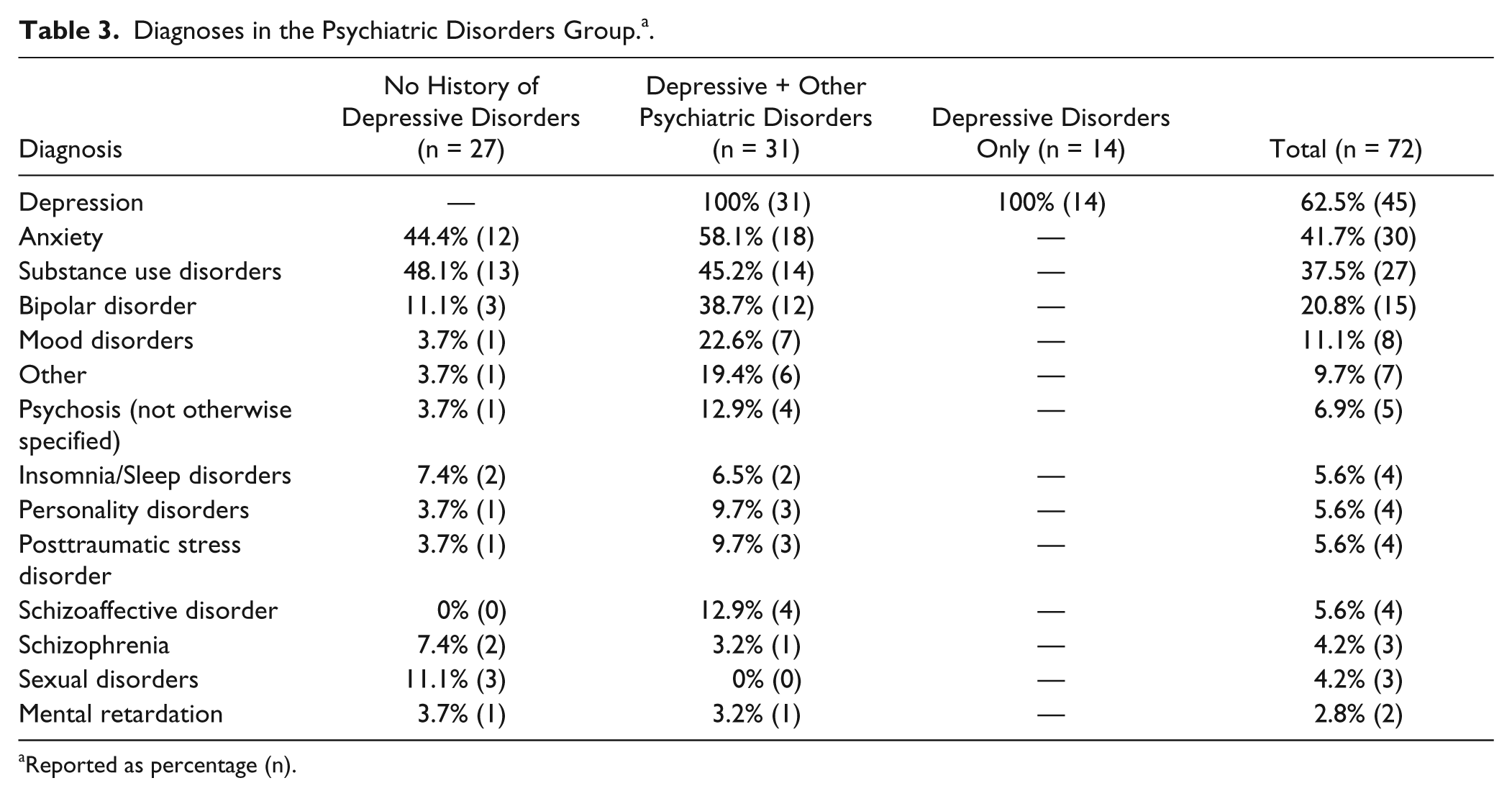
Reported as percentage (n).
Overall, 51.2% of the INRs taken were in the goal range. This increased to 66.9% when considering a variance of ±0.2 INR units. Using the modified Rosendaal’s linear interpolation, patients were in their goal range 57.4% of the time (147 calculable patient cases), and 84.1% of the patients had a mean INR within their goal range. The most common adverse event was minor
bleeding (reported by 38.4% of patients); 10 experienced a major bleeding event (n = 12; 8.3% per patient-year), and 7 experienced an embolic event (n = 7; 4.6% per patient-year). Because of a low number of major bleeds and embolic events, we chose to analyze all INR values that were reported as “critical” (defined at our institution as any INR value equal to or greater than 5.0) or “significantly low” (defined as any INR value equal to or less than 0.5 units below goal range). It was found that 27 patients (17.9%) experienced a critical INR during their therapy (78 events of 3139 evaluated INRs), and 99 patients (65.6%) experienced a significantly low INR (346 events of 3139 evaluated INRs).
When evaluating our primary outcome, both unadjusted and adjusted comparisons were made. The Bonferroni method was utilized to adjust the P value outcomes for multiple comparisons. Control patients had a significantly greater proportion of INRs in the goal range compared with either the depression or psychiatric disorders groups (controls, 55.7% vs depression, 43.5%, adjusted and unadjusted P < .001; vs psychiatric disorders, 45.8%, adjusted and unadjusted P < .001). Utilizing the modified Rosendaal’s linear interpolation, patients with psychiatric disorders were in the goal range significantly less often than the control group (53.0% vs 61.3%, respectively, unadjusted P = .034); however, this difference was not statistically significant when adjusting for multiple comparisons (P = .06). There was also no difference when comparing the control and depression groups (54.5% vs 61.3%, respectively, adjusted P = .24, unadjusted P = .121). There was no difference between the groups when evaluating the percentage of patients with a mean INR in their goal range. Patients in the depressive and psychiatric disorders groups experienced more critically high (P < .001 and P = .003, respectively) and significantly low (P < .001 for both) INR values than those in the control group. Further details on the comparison of anticoagulation control can be found in Table 4.
Anticoagulation Control. a .
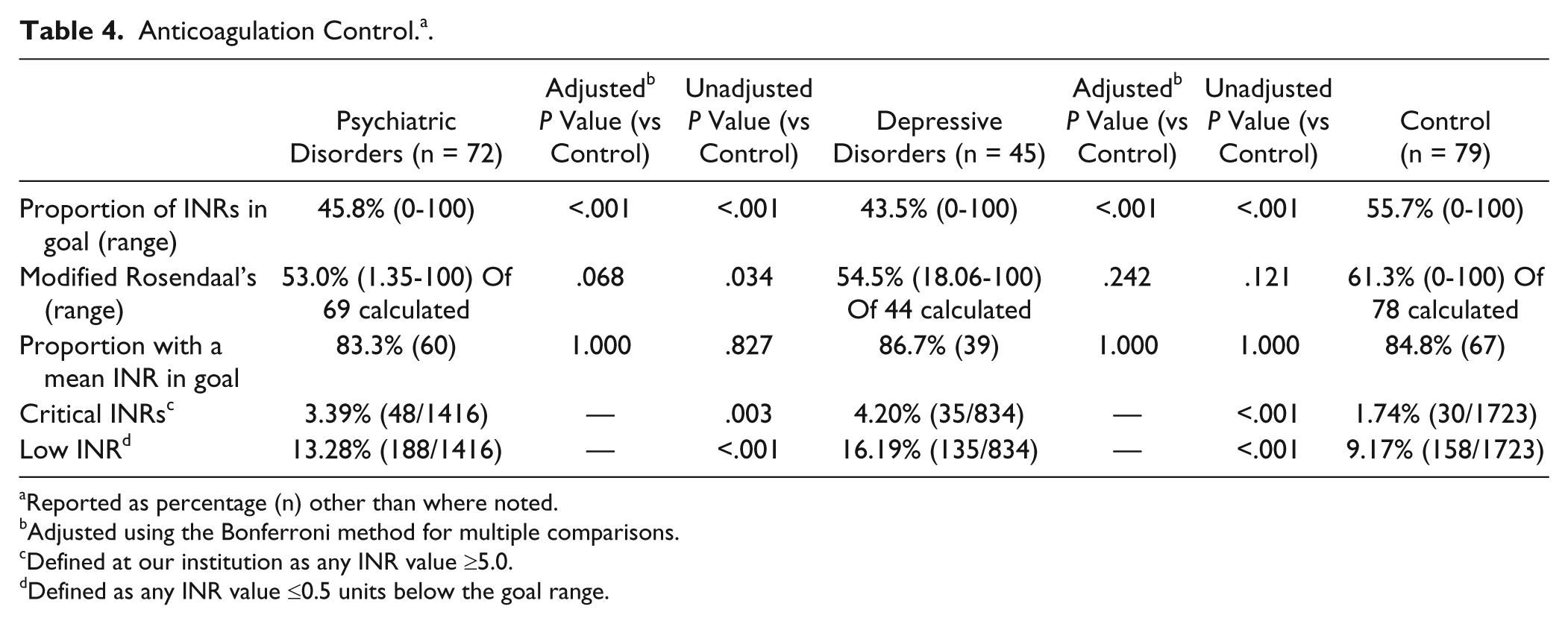
Reported as percentage (n) other than where noted.
Adjusted using the Bonferroni method for multiple comparisons.
Defined at our institution as any INR value ≥5.0.
Defined as any INR value ≤0.5 units below the goal range.
When evaluating clinically significant events, there were no differences in embolic events (P = 1.00 for both psychiatric and depressive vs control) or major bleeds (P = .332, psychiatric vs control; P = .256, depressive vs control). Minor bleeds were reported by more patients with psychiatric disorders than those in the control group (P = .006). This difference was not statistically significant when comparing the group with depressive disorders and the control group (P = .133). Further details can be found in Table 5.
Clinical End Points. a .
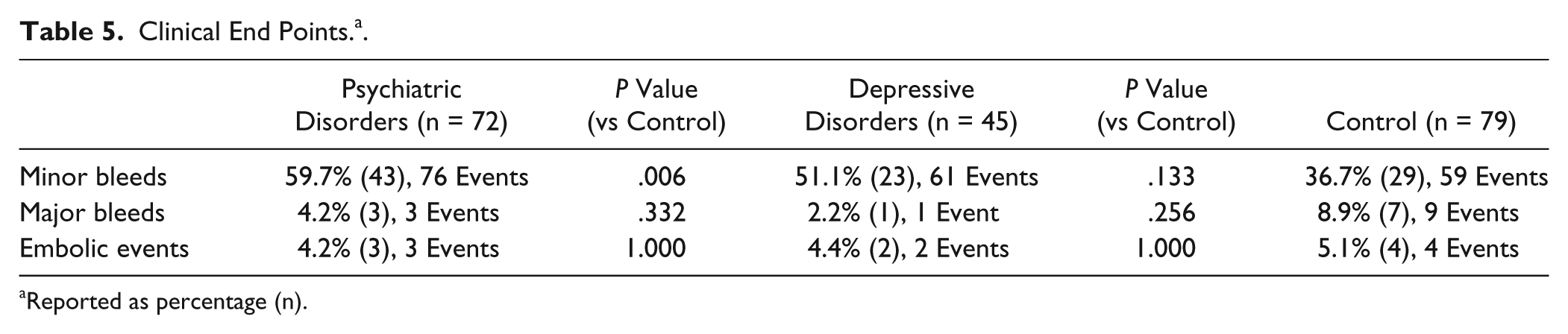
Reported as percentage (n).
Discussion
Our overall TTR findings are consistent with the experience of other coordinated anticoagulation clinics.2,19 For example, in a retrospective review of 12 897 INRs, Wittkowsky and Devine 19 found that 51.5% of their INRs were in the therapeutic range, and this increased to 66.1% when the range was expanded by 0.2 INR units. 19 In our clinic, using a similar measure, our patients had 51.2% of their INRs in the therapeutic range, and this increased to 66.9% when the range was expanded by 0.2 INR units. Because the clinic in this study was in a public safety-net hospital, the socioeconomic and patient disease state mix may be very different from that in other clinic settings.
It is well documented that patients with depression and other psychiatric conditions have difficulty with adherence to prescribed medication regimens.20-23 Patients taking warfarin must maintain not only the prescribed dose of medication but be consistently adherent with other directions specific to warfarin (eg, dietary instructions and follow-up monitoring visits). Therefore, it is not surprising that these patients may struggle with a medication regimen whose successful use is highly dependent on strict adherence. There are, however, multiple factors beyond dosage and visit persistence that may play a role in anticoagulation control for patients with psychiatric disorders. For instance, alcohol abuse and illicit substance use may be more common among patients with schizophrenia and may be a comorbidity among people with depression.24,25 In addition, patients with depression may have appetite disturbances as a symptom of their condition. Variations in vitamin K intake because of inconsistent eating patterns would further contribute to INR instability. It is also likely that patients with psychiatric disorders may experience issues with polypharmacy and, thus, would be more likely to experience drug interactions with warfarin, especially because numerous psychiatric medications have been associated with increases and decreases in the INR.26,27
In our study, we found that patients with psychiatric disorders have lower TTRs compared with those without. In our unadjusted analysis, this result was demonstrated with 2 of the 3 methods (percentage INRs in range and modified Rosendaal’s linear interpolation) used to calculate TTR. When using a conservative statistical adjustment for multiple comparisons, only 1 of these (percentage INRs in range) remained significant; however, this adjustment may also increase the risk of a type II error.
When comparing TTR using mean INR, we found no difference between the groups. There may have been no difference using mean INR because patients experiencing multiple subtherapeutic and supratherapeutic values may still have a mean value within their goal range. Thus, utilizing the percentage of patients with a mean INR within goal range may not be the most sensitive marker of INR control. It is possible that INR sample variability explains this effect and is consistent with our finding that patients with a history of psychiatric disorders also had significantly more critically elevated and significantly low INR values (see Table 4). For example, only 9% (7/79) of control patients experienced a critical INR compared with nearly 28% (20/72) in the group with psychiatric conditions. This effect may be explained by increased psychosocial instabilities and associated behaviors, including concomitant alcohol misuse, episodic medication adherence, variable diets, substance abuse, and even drug interactions with an ever-changing medication profile. Interestingly, patients with a history of depression had a statistically lower TTR than controls when considering the proportion of INRs in range but not with the modified Rosendaal’s linear interpolation. Although the modified Rosendaal’s was numerically lower than that of controls, it is likely that there were not enough patients in the depression group to show a statistical difference.
In addition, the number of individuals reporting minor bleeds in this study was higher in the group with psychiatric condition compared with the control group. The potential reasons for this difference are numerous, but one possibility may be attributed to the fact that some antidepressants, particularly selective serotonin reuptake inhibitors and selective serotonin and norepinephrine reuptake inhibitors, may increase bleeding risk regardless of anticoagulation control.28,29 For instance, 1 study found an increased risk of nongastrointestinal bleeding (odds ratio = 1.7; 95% confidence interval = 1.1-2.5) in patients taking concurrent coumarins and serotonergic agents. 29 Although our study did not have enough event numbers to detect this level of difference, patients maintained on warfarin and receiving pharmacotherapy for psychiatric disorders may still be vulnerable to these adverse events beyond nuisance bleeding.
A previous study by El-Gatit et al 15 analyzed the relationship between depression (excluding those with known major psychiatric disorders) and nonadherence to anticoagulant therapy after valve replacement. 15 This 9-week prospective study enrolled 62 study participants, all of whom had undergone aortic valve replacement therapy within 18 months of study entry. El-Gatit et al showed both a greater percentage of adherent days using a microprocessor installed in the cap of the pill bottles (depression, 86.2%, vs control, 97.0%; P < .0001) and percentage of appointments attended in those who did not meet the diagnostic criteria for depression (depressed, 53.1%, vs control, 96.7%; P < .0001). However, this study does provide a proof of concept that medication and appointment adherence may be reduced in patients on warfarin who have a diagnosis of depression.
In contrast, our study included all patients who were referred to our clinic of whom only 9.3% had undergone valve replacement. In addition, we included patients with all forms of psychiatric disorders in our study population. Interestingly, the participants indicating depressive symptoms in the study by El-Gatit et al 15 were not prescribed antidepressants. In our population, a majority of depressed patients (86.7%) and those with psychiatric disorders (65.3%) used antidepressant medications. These differences demonstrate the limitation of the external validity of the El-Gatit study, and we believe that our study may be more representative of practice in the United States.
Our study is certainly not without some limitations. First and foremost, it is of retrospective design. In a prospective design, inconsistencies in monitoring could be better controlled to decrease the chance of confounding the results. For example, in our study, patients with psychiatric disorders were seen more frequently than those in the control group (2.34 vs 1.96 INRs per 30 days, P = .04). It is possible that the pharmacists in this clinic attempted to follow these patients more closely to minimize this instability, thus making it more difficult to show differences in TTR. Second, our sample size limits our ability to detect statistical differences in clinical outcomes; thus, we relied on the surrogate marker of TTR to test our hypothesis. In addition, when utilizing the Bonferroni adjustment, the modified Rosendaal method was no longer statistically significant. We feel that this comparison would have likely been significantly different if more patients could have been included in our sample. Third, this study did not determine adherence (to clinic visits or medications) or severity of psychiatric disease during the defined study period. In a retrospective study, adherence and psychiatric disease fluctuation are very difficult to objectively assess given the limitations of documentation. Fluctuation in psychiatric disease severity may indirectly affect one’s ability to attend anticoagulation appointments and to remain on prescribed warfarin regimens. Fourth, a small number of participants in the control group were prescribed antidepressants and benzodiazepines. It is certainly possible that some, if not all, were taking these medications for nonpsychiatric purposes (eg, neuropathic pain); however, this could also represent a bias in endogeneity. Fifth, the study investigators did not track other nonpsychiatric disease states and medications that may have greatly affected INR levels (such as antibiotics) because it was assumed that the incidence between the groups would be similar. To minimize these limitations, we attempted to strengthen our retrospective design in several ways. All psychiatric diagnostic codes were verified with other medical documentation, and time frames of known instability (eg, hospitalization, first month of therapy, and planned procedures) were removed to isolate the chronic anticoagulation control measure of these patients. As mentioned previously, we modified Rosendaal’s linear interpolation to reduce the potential bias from prolonged absences in clinic visits. Finally, because patients with depression often have multiple concomitant psychiatric disorders, we feel that including these patients expands the external validity of our sample.
Moving forward, health care providers who manage anticoagulation of patients with psychiatric and depressive disorders should consider utilizing evidence-based techniques outlined by Bucci et al. 30 The authors of this article emphasize educating patients regarding adherence, motivating them to follow their prescribed treatment regimens, and reinforcing the importance of taking medications as prescribed at each patient encounter. The authors also suggest improving communication strategies with our patients, simplifying their treatment regimen, anticipating barriers to medication adherence, providing oral and written instructions, suggesting the use of medication reminders, tailoring the treatment to fit the patient’s lifestyle, and recognizing that not every strategy works in all patients.
Finally, it is important to consider these findings in the context of an evolving anticoagulation landscape. Several new oral anticoagulants are now available in the United States and in Europe. These agents are advantageous because they offer more predictable pharmacokinetic and pharmacodynamic properties, which allow patients to have less frequent laboratory and clinic visits. The impact of reducing the number and frequency of encounters on adherence in clinic practice is yet unknown. It would not be unrealistic to assume that patients may be less adherent to these regimens than was seen in clinical trials, especially those with a history of psychiatric disorders. Therefore, practitioners should consider a patient’s history of psychiatric disorders as they consider the risks and benefits of starting or switching patients to one of the newer oral anticoagulant options.
Conclusion
To our knowledge, this is the first study to assess the impact of psychiatric disorders on anticoagulation control in patients taking warfarin for a variety of indications. Although this study has limitations because of the nature of the retrospective design, it does support the hypothesis that patients with psychiatric disorders spend less time in the therapeutic range and may need additional support. Health care providers should consider these findings when designing monitoring plans for patients receiving oral anticoagulation with a history of psychiatric disorders or depression.
Footnotes
Acknowledgements
The authors would like to thank Marie Walker for allowing the use of ClotFree (![]() ) online software in the analysis of this study. In addition, the authors would like to recognize Jeff Jutting and his assistance with statistical analysis. We would also like to thank the numerous students who assisted with data collection.
) online software in the analysis of this study. In addition, the authors would like to recognize Jeff Jutting and his assistance with statistical analysis. We would also like to thank the numerous students who assisted with data collection.
Authors’ Note
The methods used in this study were presented as a student poster at the 2007 ASHP Midyear Clinical Meeting by Dr Matthew Pitlick.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.