
Abstract
Cardiac transplant patients are at risk for developing cardiac allograft vasculopathy (CAV), and dyslipidemia in this patient population has been associated with increased risk.1-3 Hydroxymethylglutaryl-coenzyme A reductase inhibitors (statins) are recommended by the International Society for Heart and Lung Transplantation in all cardiac transplant recipients, regardless of cholesterol concentrations, to delay the onset of CAV. 1 The European Society of Cardiology (ESC) recommends statins as the first-line lipid-lowering therapy in all solid organ transplant patients. 2 Although a specific goal for low-density lipoprotein cholesterol (LDL-C) is not specified by either organization, both guidelines recommend conservative initial dosing of statins secondary to the increased risk of myopathy when coadministered with calcineurin inhibitors (CNIs).1,2 Because many cardiac transplant centers target LDL-C concentrations of less than 100 mg/dL, as recommended by the Canadian Cardiovascular Society transplantation guidelines, 3 the combination of ezetimibe, which reduces LDL-C by an additional 15% to 18% is a therapeutic option. 4 Ezetimibe is recommended by the ESC as second-line lipid-lowering therapy in cardiac transplant patients with either statin intolerance or with elevated LDL-C while receiving maximally tolerated statin doses. 2
Many statins are metabolized by CYP3A isoenzymes, as are CNIs, and coadministration may lead to increased statin concentrations and risk of myopathy (fluvastatin, pravastatin, rosuvastatin, and pitavastatin have less potential for interaction).6,7 Both cyclosporine and tacrolimus, and many statins (and their metabolites) are also inhibitors of the hepatic organic anion transport protein 1B1 (OATPIBI), which may also account for observed increases in statin plasma concentrations. 5 Coadministration of ezetimibe with cyclosporine has been reported to increase ezetimibe area under the curve up to 3-fold and cyclosporine exposure by 15%.4,8 Ezetimibe product labeling cautions on an increased risk of myopathy when ezetimibe is coadministered with a statin. 4 Currently, there are only 3 published clinical trials evaluating the effects ezetimibe in cardiac transplant recipients in a total of 117 patients: 1 retrospective observational study, 9 1 prospective observational study, 10 and 1 randomized, placebo-controlled trial. 11 The purpose of our retrospective observational study was to assess the impact of ezetimibe on lipid levels and the frequency of adverse effects, alone or in combination with other lipid-lowering agents (statins, niacin, gemfibrozil, fenofibrate, bile acid resins, and fish oil), in cardiac transplant recipients receiving CNIs. Our study is the largest published report to date of ezetimibe safety in a cardiac transplant population.
Methods
Study Design
This study was a retrospective chart review, and the clinical research was determined to be exempt by our center’s Committee on Studies Involving Human Beings. Medical records of cardiac transplant patients were included in the study if they were prescribed ezetimibe, either alone or in combination with other lipid-lowering agents (statins, niacin, gemfibrozil, fenofibrate, bile acid resins, and fish oils) and evaluated at least once in a 12-month period at the cardiac transplantation clinic of an 800-bed teaching hospital and regional transplant referral center that performs more than 50 cardiac transplants per year. Patients may have been concurrently treated with nucleotide blocking agents, corticosteroids, and sirolimus during the study period. For patients taking sirolimus, doses remained unchanged during the study period. Data were included in the analysis for all included patients from the start of their clinic medical record and for at least 8 months following study inclusion.
Patient data were included in the efficacy analysis if they had baseline LDL-C blood concentrations recorded within 1 year prior to the start of ezetimibe and at least 1 additional LDL-C recorded between 4 weeks and 1 year following the start of ezetimibe with no change in lipid-lowering therapy between the 2 determinations. Patients were included in the safety analysis if they had received at least 1 dose of ezetimibe. The primary outcome of the study was the mean change in fasting LDL-C. Secondary outcomes included mean change in total cholesterol (TChol), triglycerides (TG), high-density lipoprotein cholesterol (HDL-C), and percentage of patients achieving LDL-C <100 mg/dL following ezetimibe treatment. Secondary outcomes related to safety included the incidence of gastrointestinal complaints (defined as abdominal pain, nausea, vomiting, and diarrhea) requiring discontinuation of ezetimibe, myalgia (defined as muscle pain, weakness, or cramping with or without CK elevations of <10 times the upper limit of the normal range), myopathy (defined as symptoms of myalgia in combination with increased creatine kinase blood concentrations >10 times the upper limit of the normal range), liver toxicity (defined as transaminases greater than or equal to 3 times the upper limit of the normal range), and mean changes in blood trough concentrations or doses of CNI following ezetimibe treatment.
Statistical Analysis
Summary statistics are reported as number (percentage), range, mean ± standard deviation, or median (interquartile range) as appropriate. Mean change in LDL-C, TChol, TG, HDL-C, liver transaminases, and blood concentration and doses of CNIs were analyzed using the Student t test for paired data or the Wilcoxon rank sum test for nonparametric variables. The percentage of patients achieving LDL-C <100 mg/dL was analyzed using McNemar’s test. A P value of ≤.05 was considered statistically significant. Statistical analyses were performed using SPSS version 15.0 (SPSS Inc, Chicago, IL).
Results
Out of 541 patients in the transplant program, 71 (13% of the transplant population at our center) were prescribed ezetimibe and were assessed for adverse events, whereas 35 (6.5% of the transplant population at our center and 49.3% of patients prescribed ezetimibe) were included in the assessment of LDL-C lowering (Figure 1). Baseline patient characteristics are described in Table 1. The average age of the overall population was 61 years. Most patients were Caucasian, and two-thirds were male. The average time since transplant was 7.7 ± 5.1 years, and the mean duration of follow-up while receiving ezetimibe was 19.7 ± 13.1 months. The average daily dose of ezetimibe was 10.1 mg ± 2.6 (range = 5-30 mg/d). Of the patients assessed for LDL-C lowering, 25 were prescribed ezetimibe plus a statin with or without other lipid-lowering therapy, 8 patients were prescribed ezetimibe alone, and 2 patients were prescribed ezetimibe plus nonstatin lipid-lowering therapy. Average doses of statins prescribed during the study are shown in Table 2, with most patients receiving low- to medium-LDL-lowering doses. At the time of this study, the majority of patients were receiving cyclosporine as the CNI. Patients who were excluded from LDL-C assessment had similar baseline characteristics compared with those included in the assessment for adverse effects, with the exception of slightly higher baseline hepatic transaminases (Table 1).
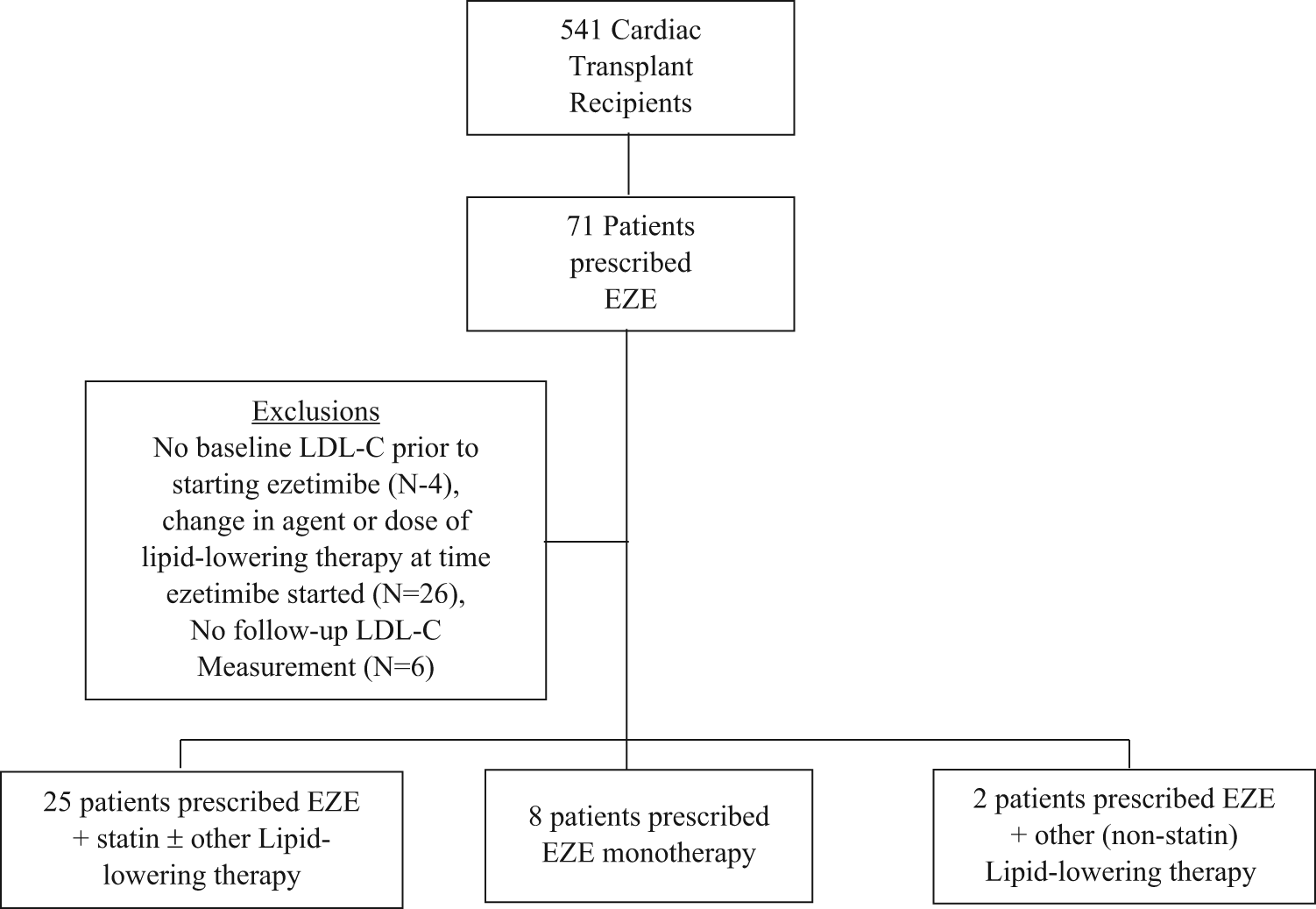
Study profile.
Patient Characteristics.
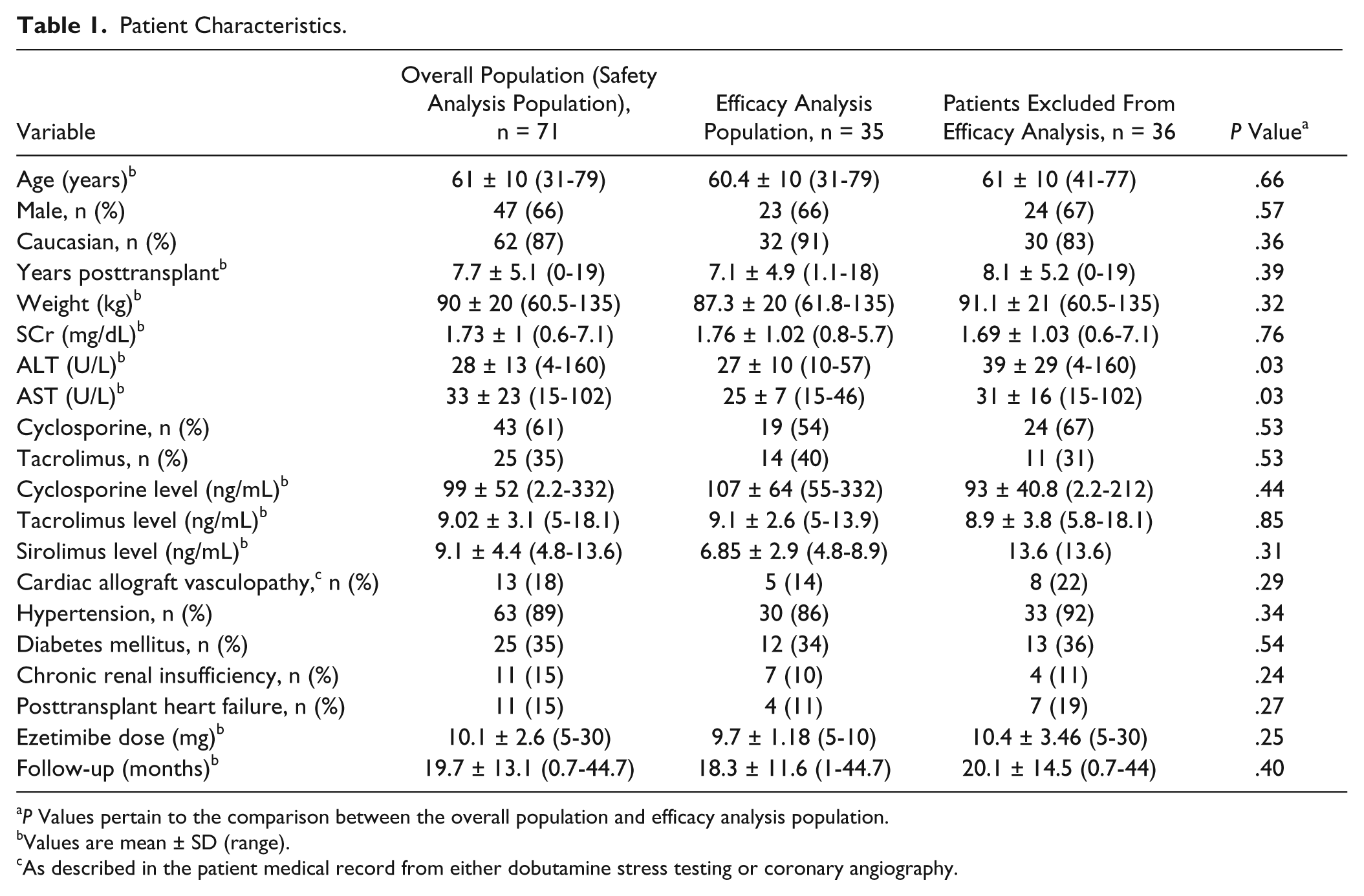
P Values pertain to the comparison between the overall population and efficacy analysis population.
Values are mean ± SD (range).
As described in the patient medical record from either dobutamine stress testing or coronary angiography.
Prescribed Statins and Dosing. a
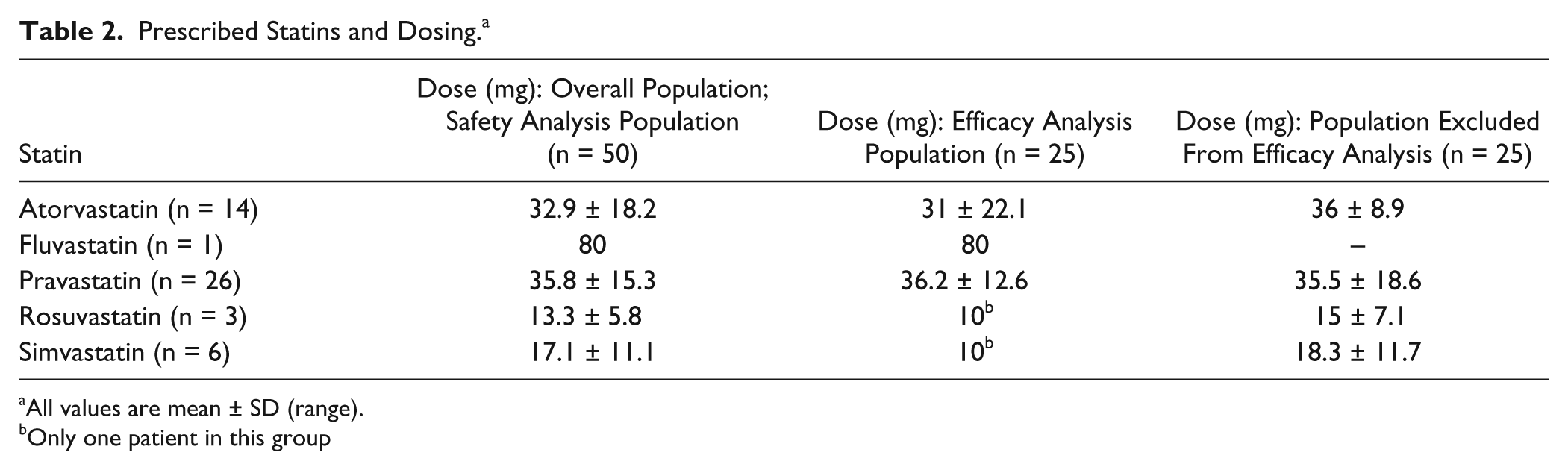
All values are mean ± SD (range).
Only one patient in this group
Ezetimibe was associated with significantly reduced LDL-C (129 mg/dL vs 94mg/dL, P < .0001), non-HDL-C (170 mg/dL vs 127.5 mg/dL, P = .0058), and TChol (236 mg/dL vs 200 mg/dL, P < .0001; Table 3). There was no significant difference in HDL-C compared with baseline. There was also no significant difference in TG. (There were 2 patients with very high TG of ≥600 mg/dL at baseline who were excluded from the analysis). The proportion of patients achieving a goal LDL of <100 mg/dL significantly increased from 11.5% at baseline to 60.5% following the addition of ezetimibe (P < .0001).
Effect of Ezetimibe on the Lipid Panel.
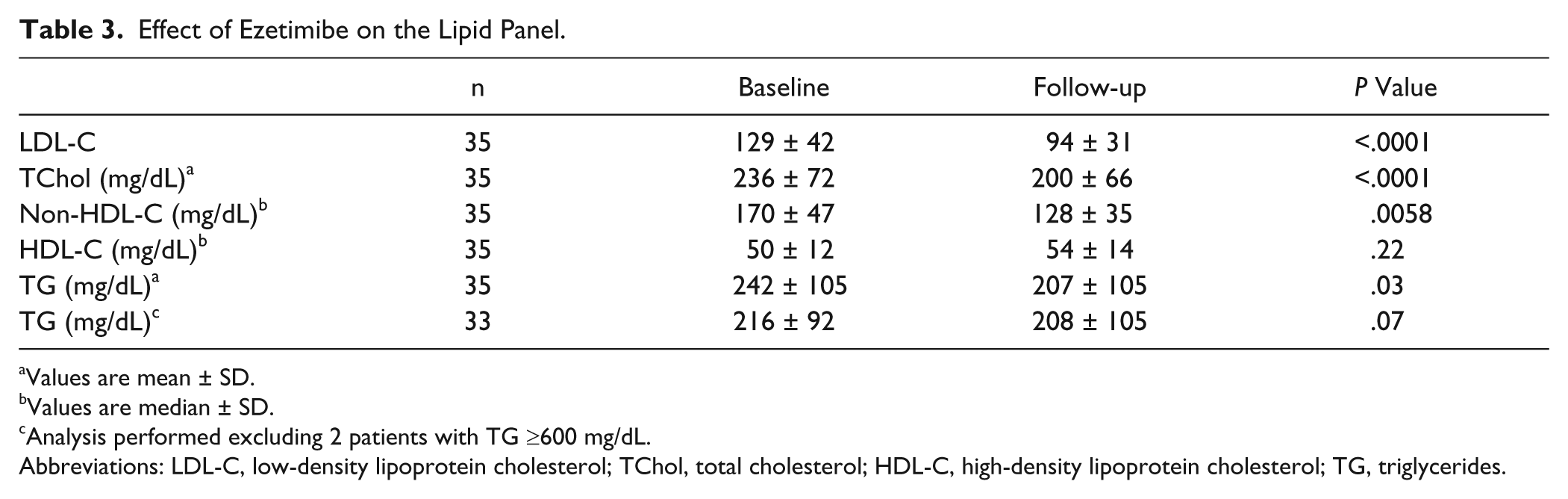
Values are mean ± SD.
Values are median ± SD.
Analysis performed excluding 2 patients with TG ≥600 mg/dL.
Abbreviations: LDL-C, low-density lipoprotein cholesterol; TChol, total cholesterol; HDL-C, high-density lipoprotein cholesterol; TG, triglycerides.
Ezetimibe had no measureable effect on blood CNI concentrations or doses (Table 4).
Effect of Ezetimibe on Calcineurin Inhibitor Dose and Blood Concentrations. a
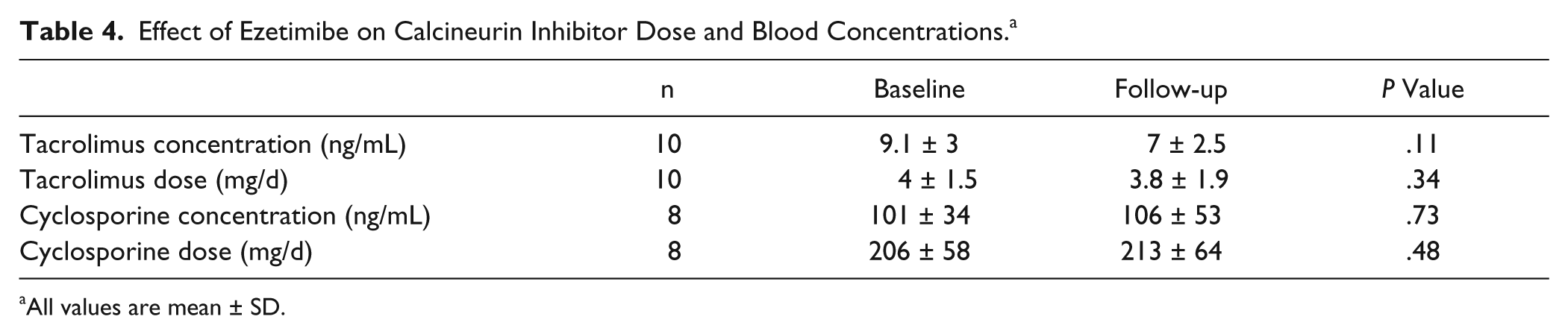
All values are mean ± SD.
Of the 71 patients assessed for adverse effects, 11 patients (15.5%) reported that they were present; 3 of these patients discontinued ezetimibe because of adverse effects (Table 5). The most common complaints were gastrointestinal intolerance and myalgia (occurring in 5.8% and 4.2% of patients, respectively). There was 1 report of myopathy with concurrent statin use where ezetimibe and the statin were temporarily stopped but eventually restarted.
Adverse Events Reported During Ezetimibe Treatment (N = 71).
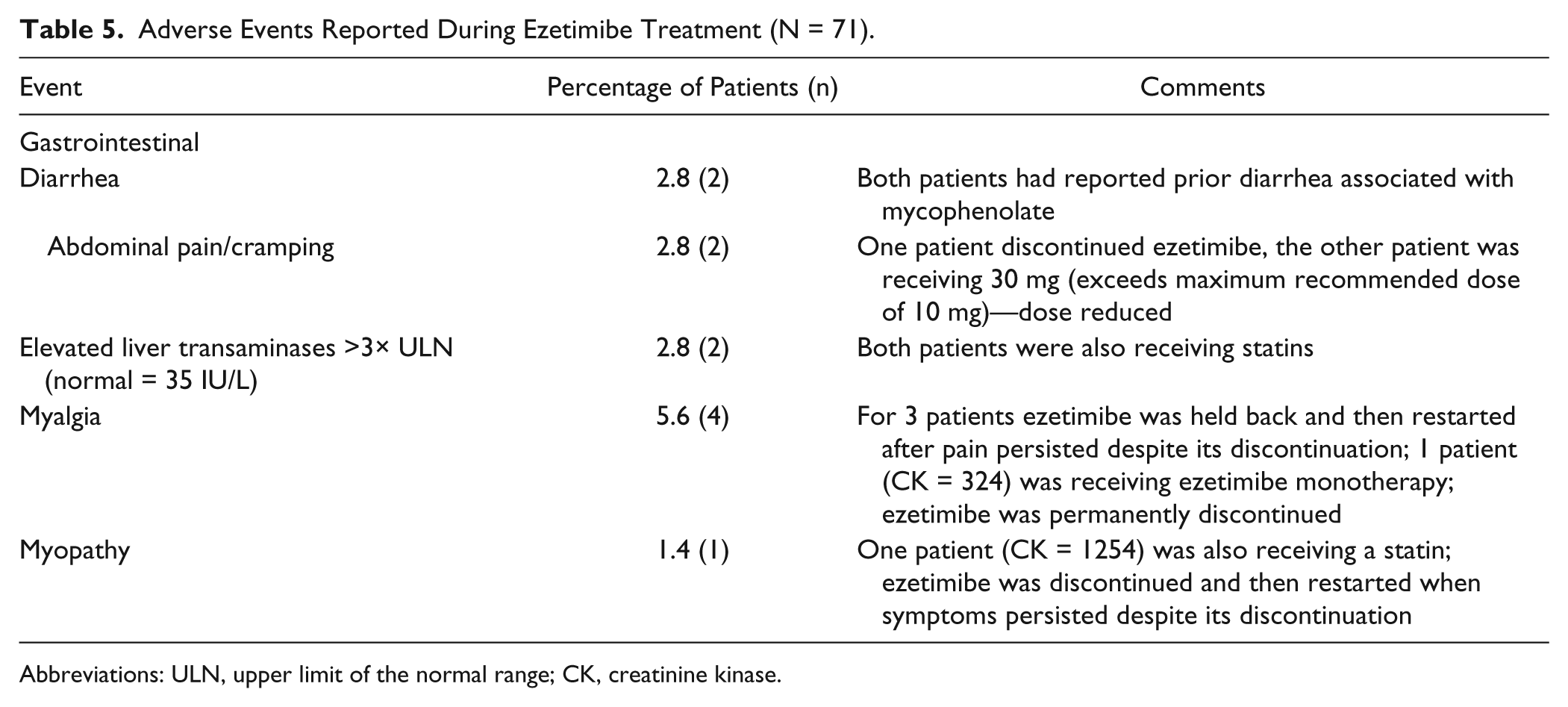
Abbreviations: ULN, upper limit of the normal range; CK, creatinine kinase.
Discussion
Our study has shown that ezetimibe is associated with lower LDL-C and a low frequency of side effects in cardiac transplant recipients. Our results demonstrated a 27% reduction in LDL-C compared with baseline. Our institutional goal LDL-C reflects that established by the Canadian Cardiovascular Society guidelines for the treatment of dyslipidemia in cardiac transplant patients (LDL-C < 100 mg/dL). 3 Ezetimibe use in our population was associated with a 6-fold increase in the number of patients achieving this goal. The results of our study are similar to those seen in a study by Shaw et al, 11 the only randomized, controlled trial published to date, of 59 cardiac transplant recipients receiving cyclosporine. In their 6-month study, ezetimibe reduced LDL-C by approximately 26%, as compared with placebo. Tolerability was the same between both groups, and no patient receiving ezetimibe withdrew from the study because of myalgias. As in our study, ezetimibe had no effect on blood concentrations of cyclosporine or dose. 11 Our results also resemble those seen in 2 previously published observational studies, 3 months and 12 months in duration, showing improvements in patient lipid profiles, with minimal occurrence of adverse effects when used as monotherapy for the management of dyslipidemia or in combination with other lipid-lowering agents in cardiac transplant recipients.9,10 In comparison, our study extends safety follow-up to more than 18 months. Data on the use of ezetimibe in other types of transplant recipients, mainly renal transplant patients, also suggest that the combination of ezetimibe and statins is safe.12-18
Our study also evaluates the effects of ezetimibe on tacrolimus blood concentrations. In the 10 patients with stable tacrolimus dose information noted for consecutive blood concentrations, we did not observe any changes following the addition of ezetimibe. Although this information is reassuring, further pharmacokinetic studies are necessary to confirm this finding. Although sirolimus can increase LDL-C, TC, and TGs, we included 3 patients who were receiving sirolimus throughout the study period because they were receiving stable sirolimus doses. 19
The impact of statins on CAV is most likely mediated by a variety of factors, including lipids, inflammation, and immune-mediated effects. Although statins have been shown to affect each of these pathways, it is unknown whether lipid lowering alone with ezetimibe will have the same beneficial effects as statins in preventing CAV. Nonetheless, these patients should receive added measures for lipid-lowering because of a high incidence of dyslipidemia in this patient population and the propensity for CNIs to worsen this common comorbidity.
Limitations of this study are that it is an observational study, and patients were not randomized to ezetimibe or placebo. In addition, it was a retrospective chart review, which may underestimate safety because we relied on clinicians to document adverse drug events in the patient’s medical record. We did not have access to baseline lipid panels prior to any lipid-lowering medications being started and immediately prior to ezetimibe initiation for all patients. Long-term outcomes, including CAV and malignancy, were not assessed.
Ezetimibe was associated with lower LDL-C in cardiac transplant recipients either as combination therapy or as monotherapy in patients who are intolerant of a statin. Future work should evaluate the addition of ezetimibe to a statin or ezetimibe monotherapy in patients with CAV and rejection.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.