
Abstract
Awake craniotomy is a reliable method of ensuring neural integrity during the excision of lesions located within or near eloquent areas. 1 Currently, the “asleep–awake–asleep” technique using general anesthesia with intraoperative wake-up is considered to be the most popular pattern for awake craniotomy.2-4 Although a variety of medications have been used in awake craniotomy over the past few decades, the ideal medication for conscious sedation in this specific procedure is yet to be proven by appropriate prospective randomized, double-blind clinical trials. 5
Propofol (PRO), a γ-amino-butyric acid A (GABAA) agonist, the medication commonly used for conscious sedation in awake craniotomy, 6 has the advantages of rapid onset and antiemetic and antiepileptic properties. 3 However, numerous studies have demonstrated the shortcomings of PRO, including longer arousal time (39 minutes), higher total incidence of intraoperative complications/complaints (64%), and interference with the monitoring of intraoperative mapping.6-11
Dexmedetomidine (DEX), a highly selective agonist of α2-adrenergic receptors, produces dose-titrated sedation, which resembles natural sleep, decreases anxiety, pain3,12,13 and cerebral blood flow. 14 These properties make DEX a potentially advantageous sedative agent in awake craniotomy. 12 Ard et al 15 reported the first use of DEX as an adjunct to an asleep–awake–asleep technique in awake craniotomy. Subsequent patient series have also reported on the successful use of DEX in different age-groups, in varied airway management techniques, and combined with different anesthetics. All previous studies have indicated that DEX appears to be a useful sedative agent for conscious sedation in awake craniotomy.5,7,16-18
The advantage of remifentanil (RF) is a rapid reversal of narcosis when intraoperative consciousness is required, it appears to have emerged as the most appropriate narcotic in awake craniotomy. 5,6 Other medication in conjunction with RF for conscious sedation in awake craniotomy is common.5,6
Till date, little research has been conducted comparing DEX and PRO for conscious sedation in awake craniotomy. To compare the efficacy and safety of DEX versus PRO, we performed a prospective, double-blind, randomized, and controlled study. We hypothesized that DEX would be a more suitable sedative agent in awake craniotomy, both in efficacy and safety. Efficacy was measured by arousal time, quality of revival during the awake period and degree of satisfaction of surgeons and patients. Safety measurements included the incidence of adverse events during the awake period and vital signs immediately before, during, and after the awake period.
Methods
Design and Participants
The study was approved by the Ethics Committee of the Zhejiang Provincial People’s Hospital and conducted in the operating room of Zhejiang Provincial People’s Hospital. Patients were enrolled in the study after they provided written informed consent. All patients scheduled for awake craniotomy were diagnosed with brain glioma near or within the motor cortex areas (some with secondary seizure). Exclusion criteria included known history of cardiovascular, pulmonary, or renal disease, psychiatric illness, communication difficulties, known allergies to the drugs being used, chronic exposure to opioids, women with body mass index (BMI) >35 kg/m2, men with BMI >42 kg/m2, and American Society of Anesthesiologists (ASA) physical status of III to V. 19
Thirty eligible patients were randomly assigned to 2 groups (D or P) according to a randomization list. All anesthetic procedures were performed by the same anesthesiologist. All surgical procedures were performed by the same surgical team, and all data were collected by the same investigator. Patients, surgeons, and the investigator were blinded to group assignment.
Study Intervention
All patients underwent “asleep–awake–asleep” technique and received detailed instruction about the technique prior to being anesthetized (Figure 1). No premedication was used. Patients’ vital signs were continuously monitored (S/5TM Entropy Module Datex-Ohmeda Division) in the perioperative period. These included heart rate (HR), electrocardiogram, pulse oxygen saturation (SpO2), noninvasive blood pressure (BP), response entropy index (RE), central venous pressure (CVP, from right internal jugular vein), and mean arterial pressure (MAP, from left radial artery). The Observer Assessment of Alertness/Sedation (OAA/S) score of patients also was observed and recorded. 20 Preoperative baseline values of the aforementioned vital signs were recorded 5 minutes after patients were brought to the operating room.
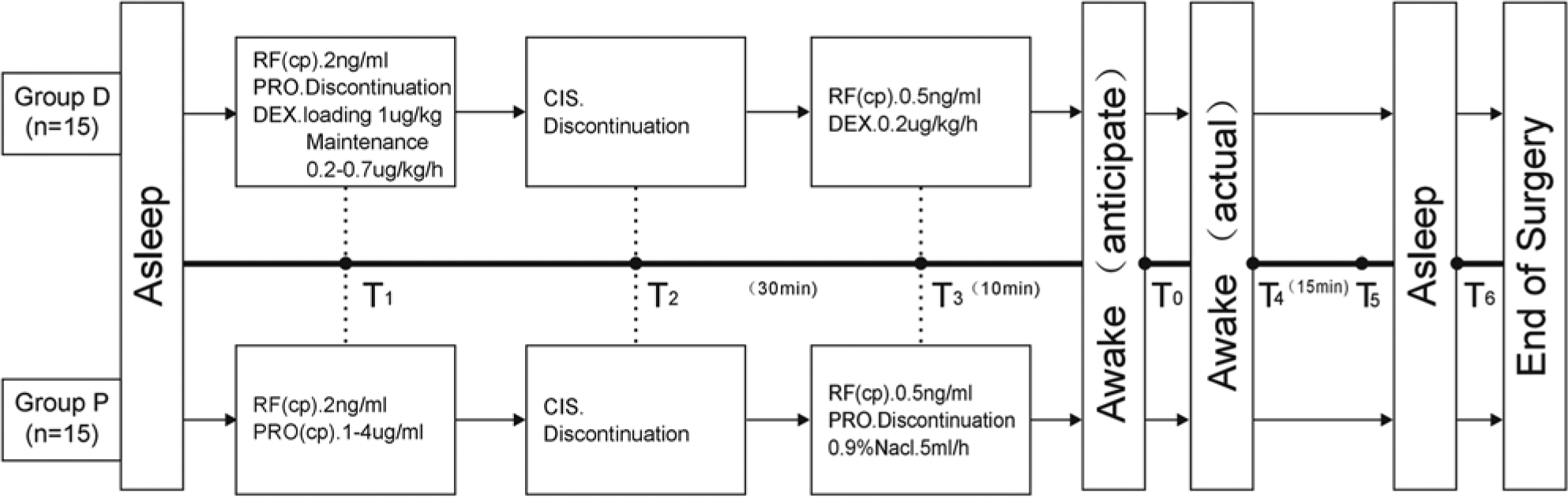
Timeline of events and medications.
General anesthesia was induced in both groups with PRO (target-controlled infusion [TCI] Marsh modal, target plasma concentration [Cp] 4 µg/mL), cisatracurium besylate (CIS, 0.2 mg/kg, followed by a maintenance dose of 0.1 mg/kg/h), RF (TCI, Minto modal, Cp 3 ng/mL). Following adequate neuromuscular relaxation, laryngoscopy was performed and 2% tetracaine was used for topical anesthesia of glottis and subglottic region. The trachea was intubated with a cuffed endotracheal tube (lidocaine gel was put on the first one third of the tube), and the lungs were mechanically ventilated, using tidal volumes of 8 to 10 mL/kg at a rate of 10 to 12 per minute, to maintain end tidal CO2 (PETCO2) of 35 to 40 mm Hg. Two minutes after intubation (T1), RF was titrated down to 2 ng/mL (Cp) in both groups; PRO was also titrated down to 1 to 4 µg/mL (Cp) in group P but was discontinued in group D, where DEX was then administered using a loading dose of 1.0 µg/kg over 10 minutes followed by a maintenance dose of 0.2 to 0.7 µg/kg/h. The rates of infusion of DEX and PRO were adjusted accordingly to maintain RE between 40 and 60. 21
Combination of 3 methods (scalp nerve block, infiltration of incision, and superficial anesthesia of dural) of local anesthesia was used with 0.25% 60mL ropivacaine hydrochloride by the surgeon. The surgeon preset the anticipated awake point in time preoperatively (T0). CIS was discontinued 40 minutes before T0 (T2) in both groups. RF was titrated down to 0.5 ng/mL (Cp) 10 minutes before T0 (T3) in both groups. At the same time (T3), DEX was titrated down to 0.2 µg/kg/h in group D. In group P, PRO was discontinued and normal saline (placebo) 5 mL/h was infused. The anesthesia ventilator rate was reduced to permit return of spontaneous ventilation at T3. After spontaneous ventilation returned and sedative level diminished as measured by RE >80, the patient’s name was shouted and repeated every 30 seconds followed by the request to open and close their fingers. When the patients moved their fingers, they were asked to move both feet. Actual awake point was defined as a patient’s ability to respond to all commands (T4). T5 was measured 15 minutes after T4. Anesthesia was again induced (T6) when the surgeon decided to stop monitoring the intraoperative mapping. PRO 0.5 mg/kg was administered intravenously for rescue sedation when cough or spontaneous movement occurred during T3–T6. Patients were transferred to postanesthetic care unit after surgery. Following the surgery, the surgeon was questioned about his degree of satisfaction with the awake period by the investigator. All patients, regardless of whether they were eligible or excluded, were interviewed 24 hours postoperatively. They were asked about their degree of satisfaction with the sedation technique, their recollection of the intraoperative events, and any sensations of pain that were felt during the awake period.
Adverse hemodynamic responses were recorded and classified as “hypertension” (MAP >20% above preoperative baseline value) or “hypotension” (MAP <20% below preoperative baseline value) and “tachycardia” (HR >20% above preoperative baseline values) or “bradycardia” (HR <50 beats/min). 19 Dopamine, urapadil, atropine, or esmolol were used if needed. During the awake period, the oxygen concentration delivered was 100%, and SpO2 ≤ 95% and/or PETCO2 ≥ 50 mm Hg were classified as “respiratory depression.”
Medication Assessment
The time from T3 to T4 was defined as arousal time. The period from T4 to T6 was defined as the awake period. The period from T1 to T6 was defined as the period of time immediately before, during, and after the patient was awake.
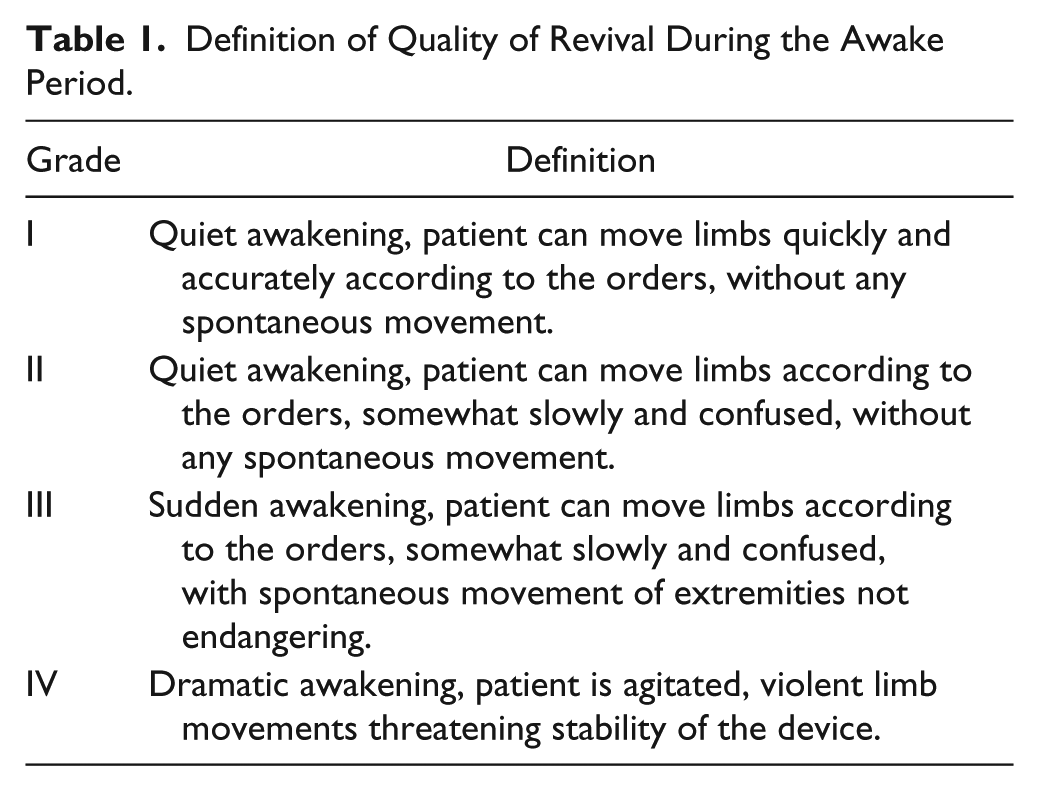
Arousal time, quality of revival during the awake period (according to speed and accuracy of the response of patients to the commands, was evaluated on a 4-grade scale 22 ; Table 1), adverse events during the awake period (hypertension, hypotension, tachycardia, bradycardia, spontaneous movement, cough, nausea, brain swelling [judged by surgeon during the surgery], respiratory depression, recall of intraoperative events and recall of pain during the awake period), vital signs during the period of time immediately before, during, and after the patient was awake (MAP, HR, RE, SpO2, PETCO2, and OAA/S), degree of satisfaction of surgeons and patients (visual analogue scale, scored from 0 to 100, a continuum from extreme dissatisfaction to extreme satisfaction), were recorded by the investigator. The degree of surgeon’s satisfaction was measured by arousal time, quality of revival, and quantity of adverse events (brain swelling, spontaneous movement, cough, nausea) during the awake period. The degree of patients’ satisfaction was measured by quantity of intraoperative events recalled and degree of pain felt during the awake period. If the surgeon and/or investigator could speculate on the assignment of a particular patient, that case was excluded from analysis.
Definition of Quality of Revival During the Awake Period.
Sample Size and Statistical Data Analysis
Because arousal time is an important scale of the efficacy, it was the primary outcome measured. The range of likely arousal time and the median of arousal time with the use of propofol have been reported to be 5 to 25 minutes and 15 minutes, 11 respectively. Because in most observation 99% of the range are within ±3 SD (standard deviation), so 1/6 × range = 1 SD = 3.33 minutes. 23 To achieve a 25% (3.75 minutes) reduction of arousal time, we calculated that 14 patients per group would suffice to detect statistical significance (α = .05, power = 90%).
The secondary outcomes measures included the quality of revival and incidence of adverse events during the awake period and the degree of satisfaction of surgeons and patients.
The data are presented as mean (SD) for continuous parametric values, as median (25th/75th percentiles) for continuous nonparametric values (the degree of satisfaction of surgeons, the degree of satisfaction of patients), or as numbers with percentage for categorical data (gender, cases with seizure, quality of revival during the awake period, incidence rate of adverse events during the awake period). For continuous data, statistical tests (Student’s t-test, and the Mann–Whitney U test) were used as appropriate. Categorical data were analyzed using the χ2 test or Fisher’s exact test. In addition, for 2 × 4 contingency table, we calculated Somers’s D and tested whether it was equal to zero.
As parametric data, MAP, HR, RE, SpO2, PETCO2, and OAA were analyzed using analysis of variance (ANOVA) with Dunnett’s test and Student–Newman–Keuls method. Because of the data type of OAA, before ANOVA we transformed OAA to
Results
Patient progress is summarized in Figure 2. Thirty-five consecutive patients were initially enrolled in the study. Five patients were excluded because of prior history of cardiovascular disease (1 case), renal diseases (1 case), BMI >42 kg/m2 (2 cases), and chronic exposure to opioids (1 case). Of the 30 patients randomized between January 2012 and November 2012, 15 were assigned to group D and 15 were assigned to group P. No exclusions were made due to the surgeon and/or investigator speculating on the patient’s assignment. Therefore, all 30 cases were eligible for analysis.
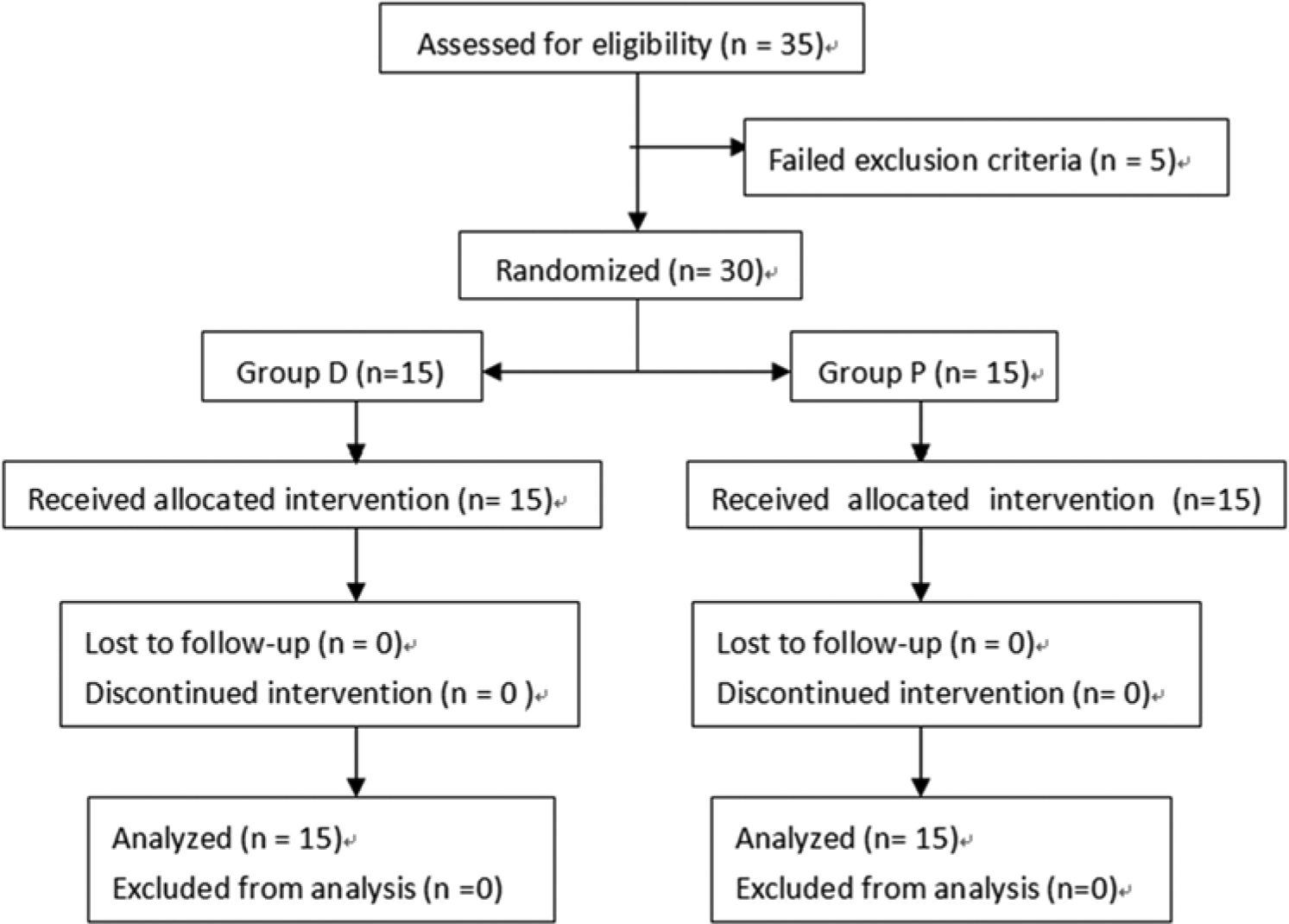
CONSORT diagram of flow of patients.
There were no differences in demographics and data related to surgery between the 2 groups (P > .05; Table 2).
Demographic Characteristic and Time Related to Surgery.

Abbreviations: ASA, American Society of Anesthesiologists; BMI, body mass index; SD, standard deviation.
t Value and the corresponding degree of freedom for t test.
Statistics of Wilcoxon 2-sample 2-sided exact test.
P value of the Fisher exact test.
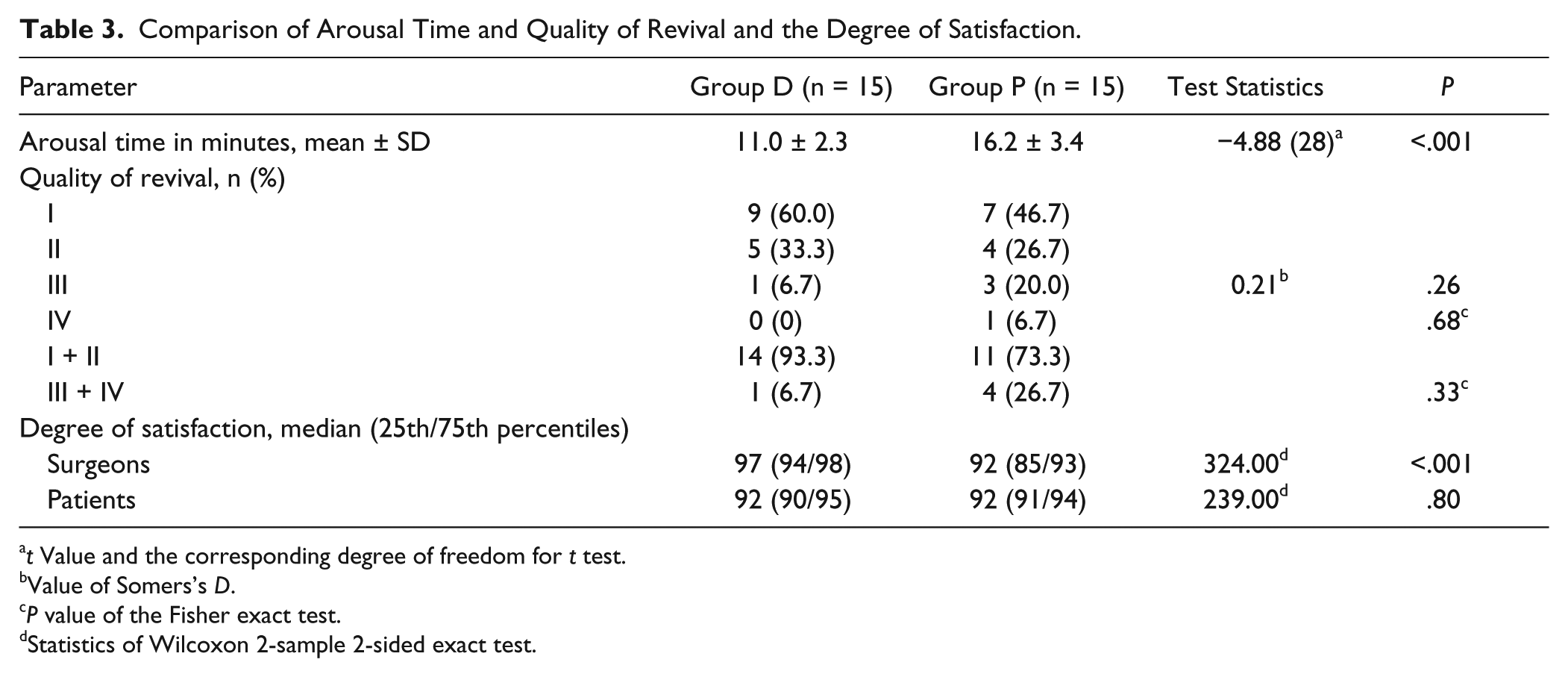
Arousal time was significantly shorter in group D than in group P (P < .001). The quality of revival in group D was similar to that in group P (P = .68 for Fisher’s exact test of 4 × 2 contingency table, P = .33 for 2 × 2 contingency table). The degree of satisfaction of surgeons was significantly higher in group D than in group P (P < .001), but no difference was found between the 2 groups with respect to the degree of satisfaction of the patients (P = .80; Table 3).
Comparison of Arousal Time and Quality of Revival and the Degree of Satisfaction.
t Value and the corresponding degree of freedom for t test.
Value of Somers’s D.
P value of the Fisher exact test.
Statistics of Wilcoxon 2-sample 2-sided exact test.
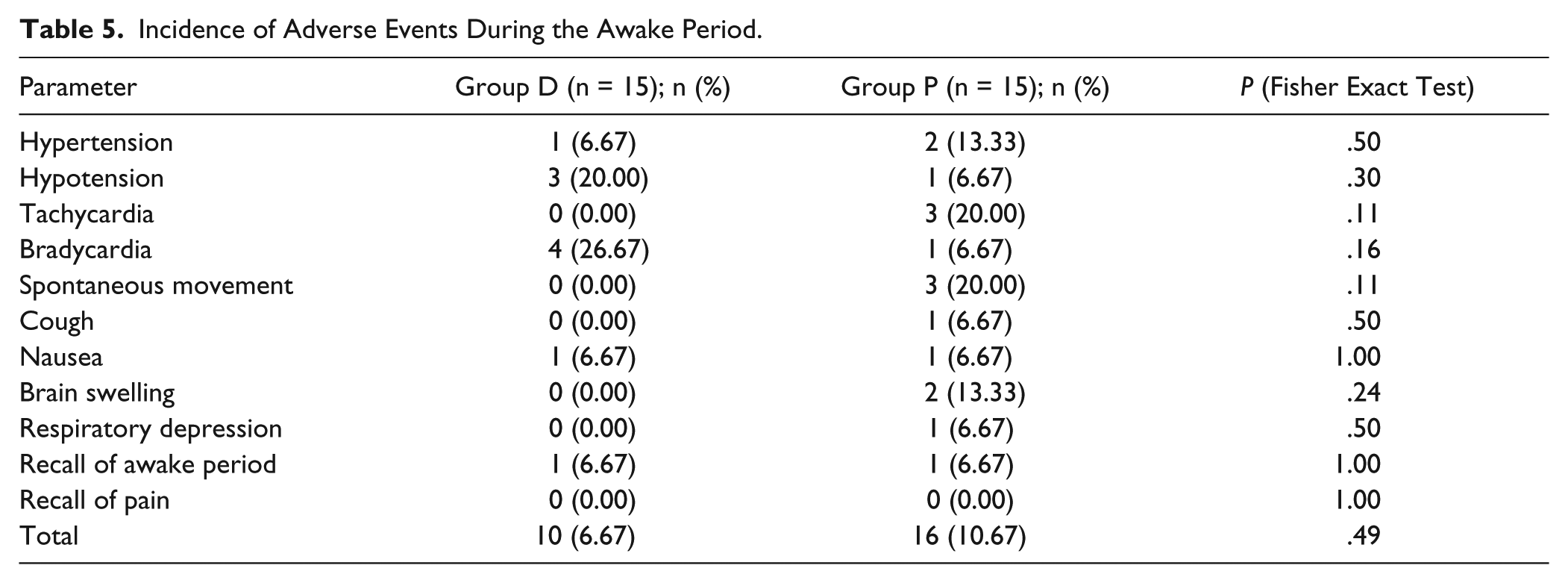
The distribution of adverse events is shown in Table 4. The incidences of all adverse events during the awake period were not different between the 2 groups (P > .05; Table 5).
Distribution of Adverse Events During the Awake Period. a
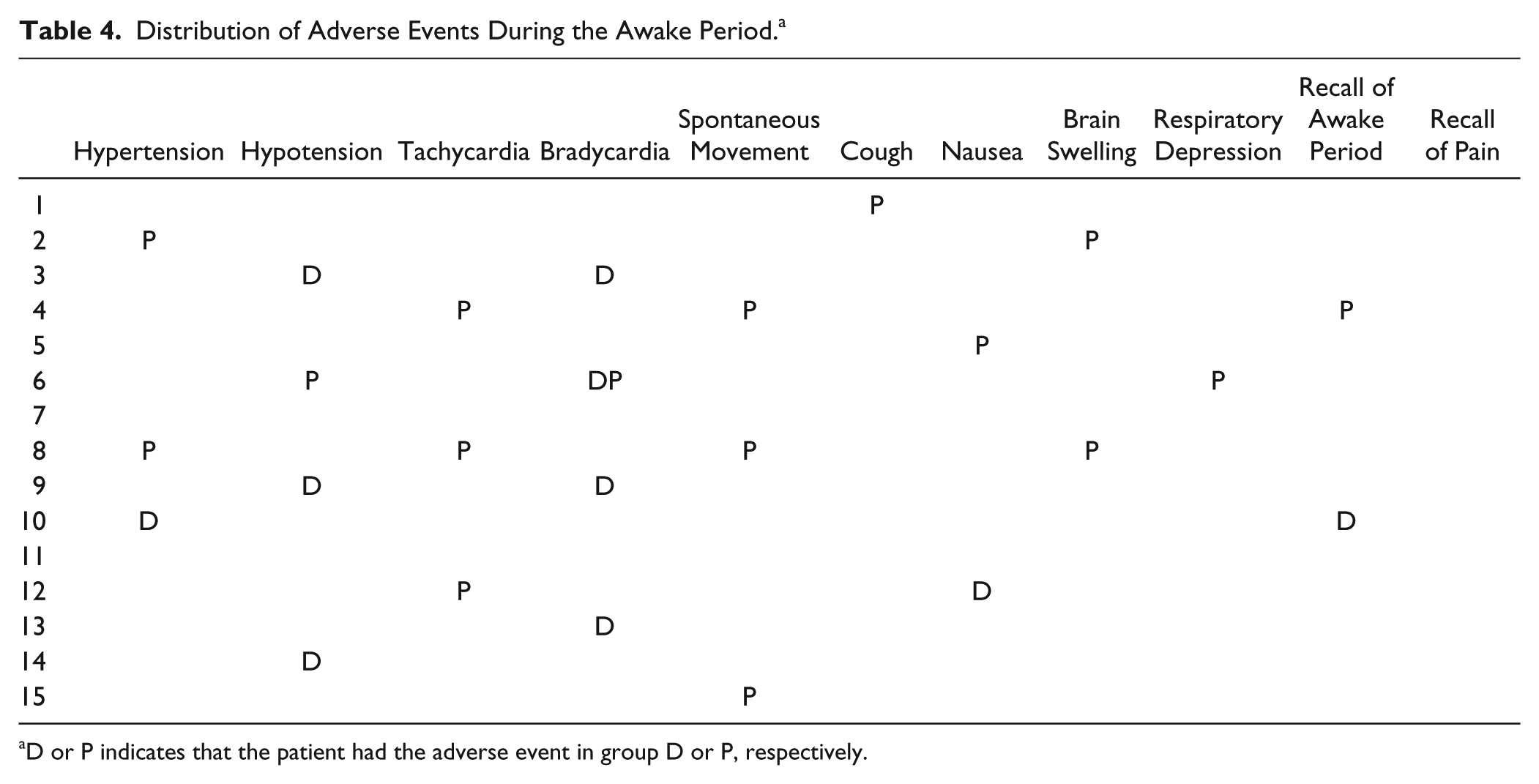
D or P indicates that the patient had the adverse event in group D or P, respectively.
Incidence of Adverse Events During the Awake Period.
Heart rate was significantly slower at times T2, T3, T4, T5, and T6 compared with baseline (T1) in group D (ANOVA with Dunnett’s post hoc test). HR was significantly slower at times T4, T5, and T6 in group D compared with group P (ANOVA with Student–Newman–Keuls post hoc test). RE, PETCO2, and OAA/S were significantly higher at T4–T6 than T1 in both groups (from Student–Newman–Keuls test and Dunnett’s test; Figure 3).
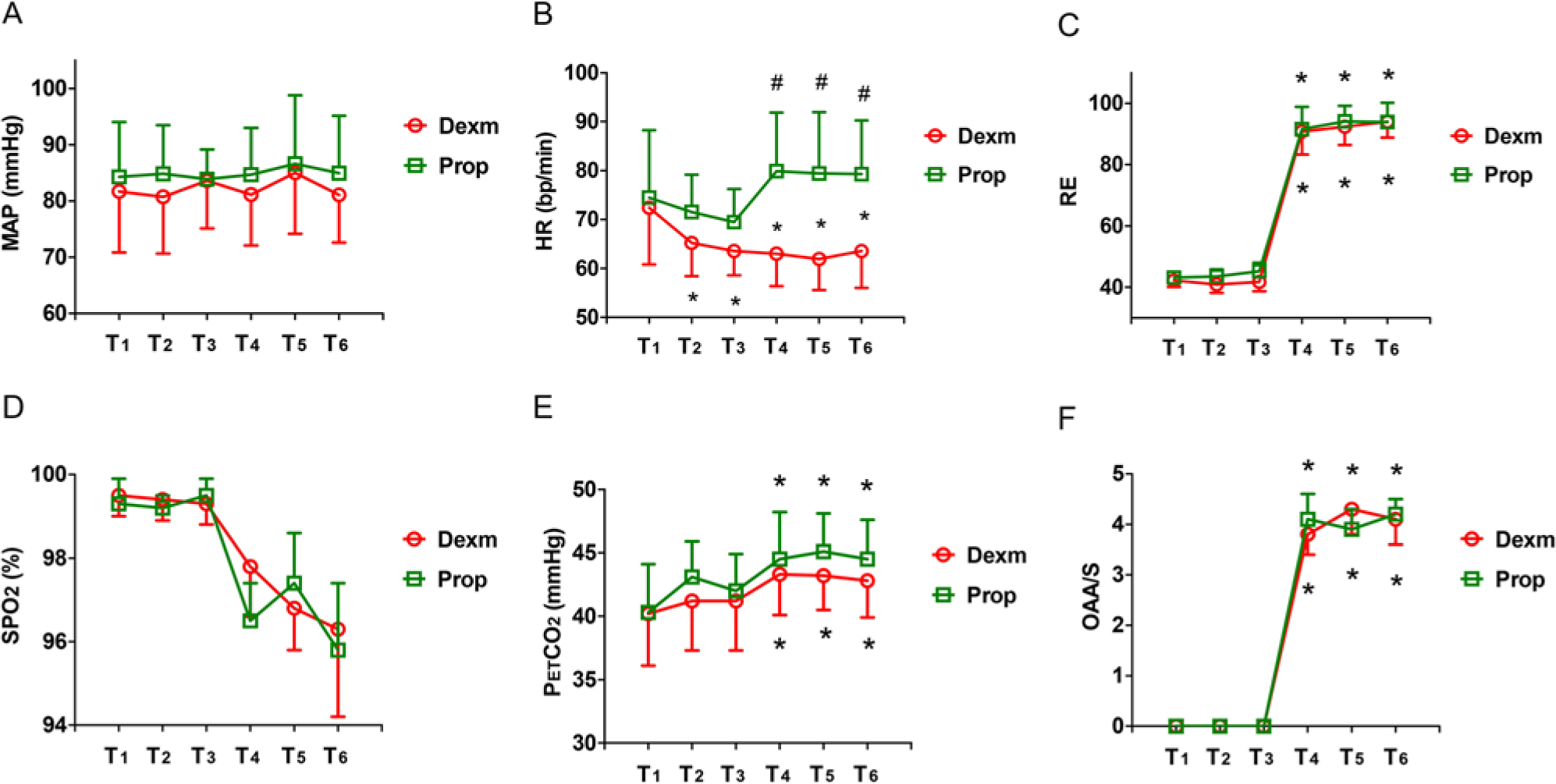
(A) Mean arterial pressure (MAP; mm Hg), (B) heart rate (HR; beats/min), (C) response entropy index (RE; numeric value), (D) pulse oxygen saturation (SpO2; percentage), (E) end tidal CO2 (PETCO2; mm Hg), and (F) Observer Assessment of Alertness/Sedation (OAA/S; numeric value) were measured as mean (standard deviation) at different points in time from T1 to T6.
No patients from group D required rescue sedation with PRO boluses during T3–T6, whereas group P yielded 4 such cases. Three cases from group D and 1 case from group P required treatment for bradycardia or hypotension.
Discussion
During the past decade, PRO was commonly used for conscious sedation in awake craniotomy. 6 However, accumulating literature showed that patients with PRO conscious sedation usually had relative longer arousal time and higher incidence of adverse events.6-11 In our study, arousal time for group P was 16.2 minutes, incidence of quality of revival (ASA III + IV) was 26.7%, and total incidence of adverse events was 10.67%, consistent with the aforementioned reports.6-11 Recent studies have indicated that DEX appears to be a useful sedative agent in this type of neurosurgery procedure.13-16 Our aim was to compare the efficacy and safety of DEX versus PRO for conscious sedation in awake craniotomy.
In our study, significant difference of arousal time was found between the patients in the DEX and PRO groups (11 vs 16.2 minutes), which is consistent with our hypothesis. The major site of noradrenergic innervation in the brain with the highest concentration of presynaptic α2-adrenergic receptors is the locus ceruleus, which is responsible for arousal, sleep, and anxiety. DEX acts at the locus ceruleus areas but does not involve the GABA receptors. Consequently, DEX provides a sedation that resembles natural sleep without cognitive impairment. 12 As a result, despite the 120-minute elimination half-life of DEX, 12 patients may be easily awakened by verbal stimulation without having to stop the drug infusion. 24 PRO is a GABAA agonist and provides a sedation that affects recall and verbal communication. Consequently, despite PRO’s considerably shorter elimination half-life of 2 to 8 minutes, 25 an additional period of time was required to awaken the patient even after infusion was stopped.
Shorter arousal time is essential for patient safety. Adverse events, such as hemodynamic fluctuations, limb movement, and nausea, may occur during this period. Theoretically, a shorter arousal time will decrease the likelihood of these adverse events. In addition, decreased arousal time enhances the surgeon’s satisfaction. The degree of surgeon satisfaction was found to be significantly higher in group D. This can be attributed to a variety of factors. Group D patients experienced less limb movement and brain swelling. Administration of neural function test within a predetermined time was easier with shorter arousal time. Furthermore, in theory, shorter arousal time will decrease the total operative time. The mean arousal time of group D was 5.2 minutes shorter than that of group P, while the 15-minute shorter time in total operative time for group P was not statistically significant. Details of the surgery and a modest sample size may have contributed to the lack of significance.
The pharmacological properties of DEX offer a better quality of revival and decreased risk of adverse events than PRO theoretically. The sedation properties of DEX, which resembles natural sleep, allow patients to stay somnolent without distress or confusion. 16 DEX can then act on presynaptic α2 receptors and negative feedback regulation of the release of adrenaline. This results in a role similar to the peripheral ganglion blocker, giving it sympatholytic properties that provide hemodynamic stability and reduced surgically induced anxiety and agitation.3,12 Meanwhile, the mild antinociceptive properties of DEX can reduce the discomfort caused by nociceptive stimulation. 17 Moreover, DEX can decrease cerebral blood flow by 30% and potentially reduce brain swelling. 18 However, no significant difference was found between the 2 groups with regard to revival quality and adverse events, which was inconsistent with our hypothesis. The modest sample size and quality of revival scale involved in our study may not have been comprehensive enough to explore these differences.
The usage of DEX for conscious sedation in awake craniotomy has several disadvantages as well. Transfusion of DEX can result in bradycardia and hypotension, as found in our study, which is consistent with previous studies. 27 Bradycardia and hypotension triggered by DEX were dose dependent 3 and had no remarkable detrimental effect on cardiac function. Both conditions were readily treated with vasoactive agents. 28 Additionally, administration of DEX may produce respiratory depression and obstruction. Although the concept that DEX does not have direct respiratory depression has been widely accepted, 29 a recent study 30 demonstrated severe respiratory depression for DEX following general anesthesia. It was proposed that DEX may enhance the respiratory depression of the GABA-mimetic sedatives due to a decreased volume of distribution of the anesthetics. DEX can also produce respiratory obstruction by relaxation of the pharyngeal muscle tone and lead to indirect respiratory depression. 31 Moreover, the usage of DEX may develop subclinical seizure12,20 and interrupt intraoperative electrocorticograpy monitoring. 3
The optimal dose regimen of DEX for conscious sedation during the awake period is still unknown. 11 Souter et al 20 suggested that a single DEX infusion 0.2 to 0.5 µg/kg/h allows successful sedation for awake craniotomy with epileptic foci and motor mapping. Bustillo et al 26 found that, in conjunction with midazolam, DEX infusion for sedation significantly prevented neurologic and cognitive testing at infusion rate recommended by manufacturer (0.2-0.7 µg/kg/h). The case reported by Bekker et al 13 showed that, in conjunction with sevoflurane, they had to reduce the DEX infused concentration to half of the lowest infusion rate recommended (0.1 µg/kg/h) to perform cognitive testing. In our study, 0.2 µg/kg/h of DEX infusion rate was selected, and all testing on patients was completed smoothly. One reason for this may be the combined infusion of RF. The other may be that the motor mapping we used required a relatively lower revival level than cognitive testing.
The primary limitation of our study was the relatively small sample size. Although it was sufficient for evaluating arousal time, a larger sample size is necessary to detect possible differences in total operative time, revival quality, and adverse events during the awake period. Another limitation was blinding of the treatment. The placebo (normal saline) was used after PRO was discontinued and nontransparent paper wrapped transfusion syringes were used, which blinded the surgeon and investigator but not the anesthesiologist. As a result, the anesthesiologist’s behavior may have influenced the objectivity of the surgeon and investigator.
In summary, our preliminary data support a proposal that either DEX or PRO can be effectively and safely administered for conscious sedation in awake craniotomy. Shorter arousal time and higher degree of surgeon satisfaction suggest that DEX might be a more suitable sedative agent in awake craniotomy. Future studies should be performed to further examine the differences in revival quality and incidence of adverse events in a larger sample size.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) declared receipt of the financial support for the research, authorship, and/or publication of this article: Our research was granted by Clinical Research Funding of Zhejiang Medical Association (No. ZYC-A04).