
Abstract
Introduction
Basal cell carcinoma (BCC) is a nonmelanoma skin cancer arising from the basal layer of the epidermis. Already the most common malignancy reported in the United States, its incidence continues to rise.1,2 BCC is typically a slow-growing, superficial tumor with metastasis occurring in 0.5% of patients. 3 Surgery and radiation are effective treatments for early-stage disease, with an estimated 5-year recurrence rate following surgery of 1% to 5%. 4 Previously, if treatments such as surgery and radiation failed or were not options in patients with advanced or metastatic BCC (mBCC), therapies were limited to systemic treatment with platinum agents or a clinical trial. 5
Exposure to ultraviolet radiation is thought to be the major causative factor in the development of BCC; others include fair complexion, family history of skin cancer, and immunosuppression. 6 Additionally, certain genetic conditions are associated with increased risk of developing BCC, including basal cell nevus syndrome (BCNS), also known as Gorlin syndrome. 6 BCNS is a rare, autosomal dominant disease where patients develop numerous BCCs, not all of which are large enough to be considered for surgical resection. 7 Patients with BCNS, and a majority of patients with sporadic BCC, were found to have alterations on chromosome 9q in the area encoding the human homolog of the PATCHED (PTCH1) receptor. 8 This gene was identified as part of the Hedgehog (Hh) signal transduction pathway during study of Drosophila development. 9 Current literature suggests that activation of Hh signaling occurs in >85% of all BCCs and >25% of medulloblastomas. Upregulation of Hh signaling has also been observed in pancreatic, breast, prostate, colorectal, and gastrointestinal tumor models. 10
The approval of this agent represents a successful example of targeted drug development for the treatment of cancer. This article will review vismodegib (Erivedge), the first Hh pathway inhibitor to be approved for clinical use by the US Food and Drug Administration (FDA), in the treatment of recurrent, locally advanced BCC (laBCC) or mBCC.
Data Sources
MEDLINE and PubMed were searched using the terms vismodegib, GDC-0449, RG3616, and basal cell carcinoma for relevant clinical trials through September 2013. FDA submissions were reviewed for otherwise unpublished data. The National Clinical Trials Registry (www.clinicaltrials.gov) was searched using the terms vismodegib and GDC-0449 to identify ongoing studies and studies with unpublished results. The same terms were also utilized in a search of American Society of Clinical Oncology (ASCO) meeting abstracts. All articles published in the English language, containing human clinical trial data and pharmacological information, were evaluated and included if appropriate.
Pharmacology
Hh signaling (illustrated in Figure 1) is critical in vertebrate embryogenesis and early development but is not commonly active during adulthood.11,12 Three mammalian homologs to the Hh ligand originally discovered in Drosophila include Sonic Hh, Desert Hh, and Indian Hh. 13 In the absence of the Hh ligand, PTCH1 inhibits the activity of Smoothened (SMO), a 7-transmembrane G-protein-coupled receptor-like protein. When present, Hh ligand binds to PTCH1 on the surface of primary cilia, ending SMO inhibition and resulting in a cascade of transduction events. This includes activation of zinc finger transcription factors, called glioma-associated oncogenes (GLIs), which localize to the nucleus where they control the expression of Hh target genes involved in cell survival, cell proliferation, angiogenesis, and the epithelial-mesenchyme transition associated with metastasis. A negative regulator of the pathway, Suppressor of fused (SUFU), binds to GLIs to prevent their entry into the nucleus. 10 The first identified Hh signaling inhibitor, cyclopamide, was isolated from Veratrum californicum after it was observed that female sheep who ingested the plant gave birth to congenitally malformed and often cyclopic lambs. 14 Cyclopamide was found to exert its teratogenic effects through Hh signaling inhibition via direct binding and antagonism of SMO.15,16 Cyclopamide demonstrated promising data in tumor models; however, its success was hindered by low potency, poor pharmacokinetics (PK), and poor tolerability. 17 Continued small-molecule screening and modifications to increase the potency and PK of potential compounds resulted in the identification of vismodegib. 18 Vismodegib can be chemically described as 2-Chloro-N-(4-chloro-3-(pyridine-2-yl)phenyl)-4-(methylsulfonyl)benzamide (C19H14Cl2N2O3S).
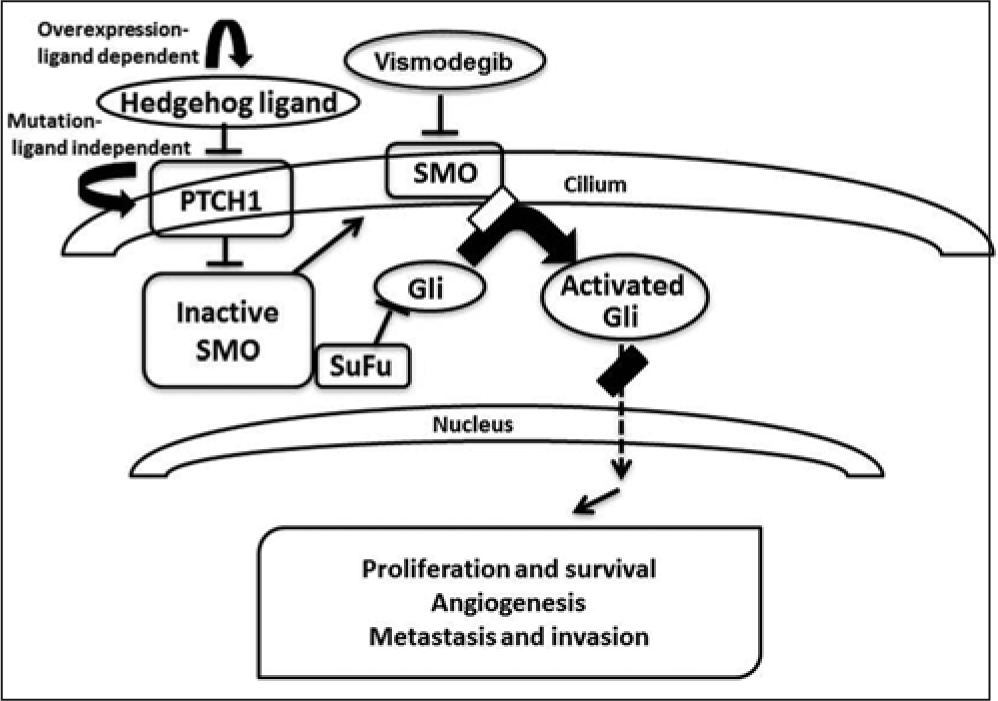
Overview of the hedgehog signaling pathway: in the absence of Hedgehog (HH) ligand, Patched (PTCH1) inhibits Smoothened (SMO). When HH is present, PTCH1 inhibition of SMO is released, and SMO goes on to activate glioma-associated oncogenes (GLIs). GLIs can be inhibited directly by Suppressor of fused (SUFU). If activated, GLIs serve as transcription factors that upregulate genes involved in cell proliferation and survival.
Vismodegib inhibits Hh signaling by binding and inhibiting SMO. A phase 1 study with vismodegib evaluated GLI expression, using samples of normal skin and hair follicles as a surrogate marker of pharmacodynamic efficacy. A greater-than 2-fold downregulation of GLI1 expression was observed in 73.5% of patients evaluated with skin biopsy and 30% of patients with hair follicle assessment. 19
The extent to which vismodegib inhibits tumor growth in preclinical models is affected by the type of Hh pathway activation. In BCCs and medulloblastomas, the pathway is constitutively active because of a loss-of-function PTCH1 mutation in chromosome 9q. 8 The resulting dysfunction prevents PTCH1 from inhibiting SMO. In these ligand-independent models, vismodegib causes tumor regression. However, in other cancer types, such as pancreatic, ovarian, and colorectal, activation of the Hh pathway appears to be stimulated by stromal or tumor production of the Hh ligand. 20 In murine models of ligand-dependent tumors, vismodegib delayed tumor growth but did not cause regression, despite adequate pathway suppression as measured by GLI mRNA levels. 21
Pharmacokinetics
Vismodegib demonstrates pH-dependent solubility, with a solubility of 0.1 µg/mL at a pH of 7 and 0.99 mg/mL at a pH of 1. 22 The bioavailability of a single dose of vismodegib is 31.8%, and absorption occurs over 24 hours. Consistent with saturable absorption, bioavailability decreases with multiple doses to 7.36%. 23 Vismodegib demonstrates nonlinear PK with regard to dose and time.19,24 The volume of distribution of vismodegib ranges from 16.4 to 26.6 L. Vismodegib is 99% protein bound in human plasma. 22
Phase 1 studies in patients with refractory solid tumors evaluated 3 doses of vismodegib: 150, 270, and 540 mg orally once daily. At all dose levels, maximum concentrations of vismodegib were reached within 2 days after a single dose, with little decline in concentrations over a 6-day washout period. A lower mean Cmax for the total drug (3.58 µmol/L) was observed for the 150 mg/d group, whereas similar levels (6.34 and 6.81 µmol/L) were observed for the 270 and 540 mg/d groups, respectively. Despite the long half-life observed with single doses of vismodegib, steady state concentrations were reached within 7 to 14 days with once daily dosing, and similar steady state concentrations were detected in plasma at all dose levels.19,25 The total plasma concentration of vismodegib was tightly correlated with levels of α1-acid glycoprotein (AAG), an acute phase reactant protein that may be elevated up to 5-fold in patients with malignancies, thus displaying saturable AAG binding. 24 In vitro studies also suggest that vismodegib also binds to serum albumin, although with less binding affinity than to AAG. 26
Vismodegib does not undergo extensive metabolism, existing as >98% parent drug in human plasma. Several minor metabolites undergo oxidation, glucuronidation, or pyridine ring cleavage. 27 In vitro studies suggest that CYP3A4/5 and CYP2C9 likely contribute to the formation of the most common oxidative metabolites. In vitro data also suggest that vismodegib has moderate potential to inhibit CYP2C8/9 and CYP2C19 and is a substrate of the efflux transporter P-glycoprotein.22,28 Excretion of vismodegib occurs primarily through the feces (82.2%), with minor excretion in the urine (4.4%). 27 The elimination half-life of vismodegib is 12 days after a single dose and 4 days after continuous daily dosing. 22
Based on the nonlinear pharmacokinetic profile and long elimination half-life observed in phase 1 studies, a phase 1b study was designed to evaluate the feasibility of less-frequent dosing of vismodegib. In this study, 63 patients with advanced solid malignancies were given vismodegib for a loading period of 11 days and then randomized to receive vismodegib daily (n = 20), 3 times weekly (n = 21), or once weekly (n = 22). Randomization was stratified with regard to baseline AAG levels. The authors observed similar levels of adverse events (AEs) regardless of the frequency of dosing. Unbound steady-state vismodegib concentrations were 60% and 85% lower in the 3-times-weekly and once-weekly dosing groups, respectively, prompting concern for decreased efficacy with these dosing regimens. 29
Clinical Trials
An open-label, multicenter, phase 1 study was conducted to establish the dosing, safety, and tolerability of vismodegib in patients with solid tumors refractory to standard treatment or for whom no standard treatment existed. The first stage of the study evaluated the maximum tolerated dose of vismodegib in a cohort of 20 patients. Toxicities were assessed and graded using the Common Toxicity Criteria for Adverse Events, version 3.0. No dose-limiting toxicities were reported at any of the evaluated dosage levels (150, 240, or 540 mg once daily). Based on the inability of the higher doses to provide greater steady-state drug concentrations, 150 mg once daily was recommended for further study. The second stage of the study further evaluated safety and tolerability, bringing the total number of patients treated to 68. Among the participants, 33 had metastatic or laBCC, 1 patient had medulloblastoma, and 34 patients had other solid tumors. The majority of AEs were mild to moderate (grade 1-2), with muscle spasms, dysgeusia, fatigue, alopecia, and decreased appetite occurring in >30% of patients; 20 patients (29.4%) experienced severe (grade 3) AEs, and 6 (8.8%) experienced life-threatening or disabling (grade 4) AEs. Also, 5 deaths were reported during the study, all attributed to disease progression.19,25
In all, 62 patients were evaluable for tumor response. Only patients with BCC or medulloblastoma demonstrated a tumor response; stable disease (SD) was the best outcome for 4/28 of patients with other solid tumors. The patient with medulloblastoma had a partial response but progressed after 3 months of therapy. Patients with BCC demonstrated an overall response rate (ORR), including complete and partial response, of 55%, with SD observed in 33%. Of the 33 patients, 12 had continued response at initial study closure. As of January 2010, the median duration of response observed in patients with BCC was 12.8 months (range = 3.7-26.4 months). Conversely, patients with other solid tumors had a median time on study of 1.4 months.19,25
Based on these results, an international, multicenter, nonrandomized phase 2 clinical trial was undertaken to further assess the safety and efficacy of vismodegib in BCCs. Given the lack of treatment options for patients with advanced BCC, the study did not include a control group. The study included 2 cohorts: mBCC and laBCC for which surgery and/or radiation were not options. Patients received 150 mg of vismodegib once daily until disease progression, unacceptable toxicity, or study withdrawal. The primary outcome of the study was ORR, with a secondary outcome of duration of response. The study enrolled 104 patients, 33 with mBCC and 71 with laBCC. Both groups had a median age of 62 years, and all participants were white. Independent data review found a 30% ORR in mBCC (95% CI = 16%-48%) and 43% ORR in laBCC (95% CI = 30%-56%). SD was observed in 64% patients with mBCC and 38% patients with laBCC. The median duration of response was 7.6 months in both cohorts, with a median progression-free survival (PFS) of 9.5 months. The median duration of treatment was 10 months, and 51 patients continued after the prespecified data cutoff point. All patients on study experienced at least 1 AE. Consistent with the findings of the phase 1 study, the majority of patients experienced mild to moderate (grade 1-2) events. Serious AEs (grades 3-4) were reported in 25% of patients, with 7 deaths occurring on study that were not drug related. However, 9.1% of patients in the mBCC cohort and 40.9% of patients in the laBCC cohort discontinued therapy as a result of their own decision or an AE. 30
An additional phase 2, multicenter, double-blind, randomized, placebo controlled trial was undertaken to determine the safety and efficacy of vismodegib in patients with BCNS. The primary end point for this study was the number of new BCC growths that were eligible for surgical resection. Patients in the treatment group received vismodegib 150 mg daily for up to 18 months. Patients in the treatment (n = 26) and placebo (n = 16) groups had a mean age of 54 and 53 years and a baseline mean of 44 and 37 surgically resectable BCCs, respectively. After 3 months, vismodegib significantly reduced the mean number of new, surgically eligible BCCs compared with placebo (2 vs 29; P < .001). Additionally, vismodegib significantly reduced the size of existing surgically eligible BCCs (−65% vs −11%; P = .003) and patients underwent fewer surgeries (mean 0.31 vs 4.4; P < .001). Despite the observed benefit in the treatment group, 54% of patients on the study drug discontinued treatment early because of intolerable mild to moderate (grade 1-2) AEs, with only 1 patient able to tolerate 18 months of vismodegib as planned. The results of this study suggest a possible role for vismodegib in patients with BCNS, although its long-term utility may be limited by its AE profile. 31
Dosage Recommendations
Vismodegib is administered at a dose of 150 mg once daily, without regard to food.22,32 The only currently available dosage form is a 150-mg capsule, which should not be opened or crushed. There are no recommendations for dose reduction of the medication for AEs, drug-drug interactions, or patient intolerance. 22 Studies to evaluate PK and recommended doses in patients with renal or hepatic impairment are planned, but there are currently no data to recommend dosage changes in these patients. 33
The dosage of vismodegib for pediatric patients younger than 18 years has not been established but is currently being evaluated in clinical trials. In preclinical animal studies, transient inhibition of Hh signaling resulted in permanent bone defects, including premature fusion of the epiphyseal plate. 34 Vismodegib is pregnancy category D and was teratogenic in rats at 20% of the recommended human dosage. A negative pregnancy test should be confirmed in female patients initiating vismodegib therapy, and effective contraception should be utilized in both male and female patients as per a block box warning. 22
Adverse Effects and Drug Interactions
Adverse effects of vismodegib are generally mild to moderate but occur in a majority of patients. Muscle spasms, alopecia, dysgeusia, and weight loss occurred most frequently in all studies reviewed (Table 1). Serious AEs occurred in 25% of patients in the phase 2 BCC study, although not all were drug related. The most common severe (grade 3/4) AEs (occurring in >1 patient) include muscle spasms, fatigue, decreased appetite, weight loss, thromboembolism, pneumonia, and cardiac failure. Severe hyponatremia was observed in 8 cases during phase 1 testing but was not reported in further studies. Amenorrhea occurred in 3/10 premenopausal women while receiving vismodegib.19,22,30,31 Although most AEs with vismodegib are considered mild-moderate, patients frequently discontinued vismodegib as a result of intolerable side effects. The side-effect profile of vismodegib reflects a small but continued presence of normal Hh signaling in adults. This is especially evident by observation of dysgeusia in greater than 40% of patients in all clinical studies and a growing body of evidence that suggests that Hh signaling is not only involved in patterning and development of the tongue during embryogenesis but is also involved in regulating progenitor cell turnover in the adult tongue epithelium. 35 The development of keratoacanthomas has been reported with the use of vismodegib. 36
Clinical Studies of Vismodegib in BCCs.
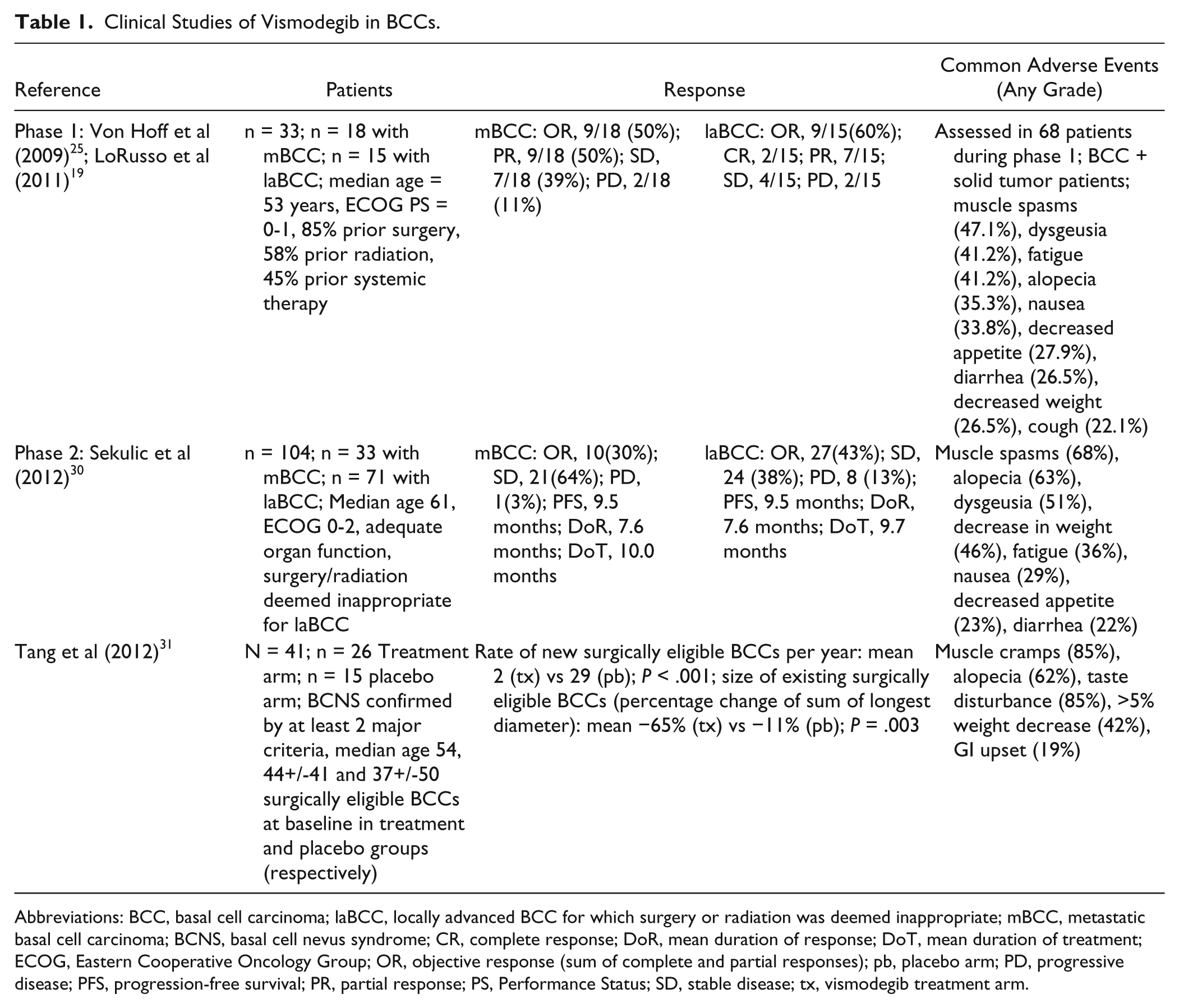
Abbreviations: BCC, basal cell carcinoma; laBCC, locally advanced BCC for which surgery or radiation was deemed inappropriate; mBCC, metastatic basal cell carcinoma; BCNS, basal cell nevus syndrome; CR, complete response; DoR, mean duration of response; DoT, mean duration of treatment; ECOG, Eastern Cooperative Oncology Group; OR, objective response (sum of complete and partial responses); pb, placebo arm; PD, progressive disease; PFS, progression-free survival; PR, partial response; PS, Performance Status; SD, stable disease; tx, vismodegib treatment arm.
Despite metabolism by CYP2C9 and CYP3A4, in vitro studies showed no increase in vismodegib concentrations when given with CYP3A4 inhibitors or inducers. A drug-drug interaction study in advanced cancer patients suggests that there was no impact on levels of the CYP2C8 substrate rosiglitazone or combined oral contraceptives (ethinyl estradiol/norethindrone). 37 Coadministration with P-glycoprotein inhibitors may increase drug vismodegib plasma levels, thus increasing the occurrence of AEs. Conversely, because of its pH solubility, concurrent use of pH-lowering agents may decrease serum concentrations of vismodegib. 22 Steady-state concentrations of the drug do not appear to affect the QTc interval in healthy volunteers. 38
Formulary Considerations
Few treatment options exist for patients with laBCCs or mBCCs. Surgery is the gold standard for treatment of BCCs, although substantial disfigurement or loss of function may result. Radiation increases the risk of secondary malignancies, and thus is inappropriate in young patients or those with genetic predispositions to skin cancer. Topical agents (imiquimod, 5-fluorouracil, and photodynamic therapy) are effective only in early-stage disease. In addition to vismodegib, the National Comprehensive Cancer Network (NCCN) guidelines recommends clinical trial as a possible treatment option in laBCC or in mBCC where surgery and radiation are not feasible options. 5 The role of chemotherapy in this setting is uncertain. Some evidence suggests that platinum agents may be utilized in the treatment of BCCs. The efficacy of platinum agents remains unclear because there are no prospective studies to evaluate response rates. A review of 53 available case reports observed a complete response rate of 37% and an ORR of 83% in patients treated with platinum agents (cisplatin or carboplatin). The median time to progression was 18 months. However, this review likely overestimates the response rate, given a publication bias toward case reports with positive outcomes. 39 Descriptions of AEs and reasons for discontinuation other than progressive disease were not reported, but it should be noted that platinum agents are associated with multiple toxicities (including nausea and vomiting, myelosuppression, renal dysfunction, and neuropathy) that may affect tolerability of therapy.
In contrast to platinum agents, treatment with vismodegib is associated with mainly mild-moderate AEs and is administered orally once daily. Vismodegib is the first agent to show an ORR in laBCCs and mBCCs in a prospective study. The NCCN guidelines recommend vismodegib as a treatment option for patients with high-risk or recurrent disease not amenable to localized therapies. 5 Currently, access to the drug is restricted to specialty pharmacies. The average wholesale price of vismodegib is estimated at $9000 per month at the recommended dosage. Patient assistance programs through the manufacturer, Genentech, are in place for those who qualify (http://www.genentech-access.com/erivedge/hcp/see-how-we-can-help/our-services/patient-assistance).
Future Directions
Vismodegib is being investigated in further phase 2 studies to evaluate its use in operable BCCs and in patients with BCNS. 40 As part of the accelerated approval process, the FDA has requested studies in renal and hepatic impairment, a drug-drug interaction study with agents that affect gastric pH, and carcinogenicity studies in mice to better clarify the use of this drug in special populations. 33
The role of vismodegib in the treatment of Hh ligand-dependent malignancies remains to be elucidated. Hh signaling in the absence of specific pathway-activating mutations has been observed in preclinical tumor models, thus suggesting a role for Hh pathway inhibition as a treatment strategy. 10 A randomized, double-blind placebo-controlled trial evaluated vismodegib as maintenance therapy in 104 patients with ovarian cancer in a second or third complete remission. Treatment with vismodegib did not significantly improve the primary outcome of PFS (7.5 vs 5.8 months with placebo; hazard ratio [HR] = 0.79, 95% CI = 0.46-1.35, P = .39). 41 Vismodegib was also studied in combination with first-line treatment (FOLFOX or FOLFIRI plus bevacizumab) for metastatic colorectal cancer in a randomized, double-blind study in 195 patients. The primary outcome of PFS was not improved in the treatment arm compared with placebo (median 9.3 vs 10.1 months, respectively; HR = 1.25, 90% CI = 0.89-1.76, P = .28). Notably, treatment intensity for all regimen components was lower in patients who received vismodegib compared with placebo. 42 Other trials looking at the addition of vismodegib to front-line treatment in metastatic pancreatic cancer and advanced gastric and gastroesophageal junction carcinoma have also shown no improvement in PFS when compared with front-line treatment alone in an unselected patient population (median = 4.0 vs 2.5 months, HR = 0.81, CI = 0.54-1.21, P = .30; median = 7.3 months vs 8.0 months, 95% CI = 4.6-10.1 vs 5.1-11.0, P = .64, respectively).43,44 The lack of clinical response to vismodegib in these cancers raises questions about its value in Hh ligand–dependent malignancies. Nonetheless, there are currently numerous active clinical trials investigating vismodegib in other malignancies, including pancreatic, breast, lung, and head and neck cancer as well as acute leukemia and sarcoma. 40
Medulloblastoma, a brain malignancy that occurs most commonly in childhood, represents an attractive setting in which Hh inhibition may provide clinical benefit, given that about one-third of tumors demonstrate alterations in the Hh pathway, and a transient response was observed in an adult patient with medulloblastoma.45-47 However, given the importance of Hh signaling in development, the use of vismodegib in pediatric patients may uncover additional toxicities not documented in adults. Pharmacokinetic studies of vismodegib in pediatric patients are under way and, in light of the poor prognosis for patients who experience medulloblastoma recurrence, there are currently multiple trials evaluating the use of vismodegib in pediatric populations.37,48
The development of drug resistance is a concern with the use of vismodegib, based on a medulloblastoma patient who initially displayed rapid shrinkage of the tumor followed by disease progression within several months and reports of tumor regrowth in patients with BCCs.46,49 When tissue samples before and after treatment were compared, a missense mutation in SMO preventing vismodegib binding was identified, which conferred vismodegib resistance. 50 Preclinical models have identified other possible mechanisms of resistance, including other SMO mutations, upregulation of downstream effectors in the Hh signaling cascade (such as GLI1), and activation of the phosphatidylinositol 3-kinase pathway. 51 Given the median duration of response of 7.6 months observed in phase 2 studies, continued research into the incidence and mechanisms of acquired resistance to vismodegib therapy are warranted.
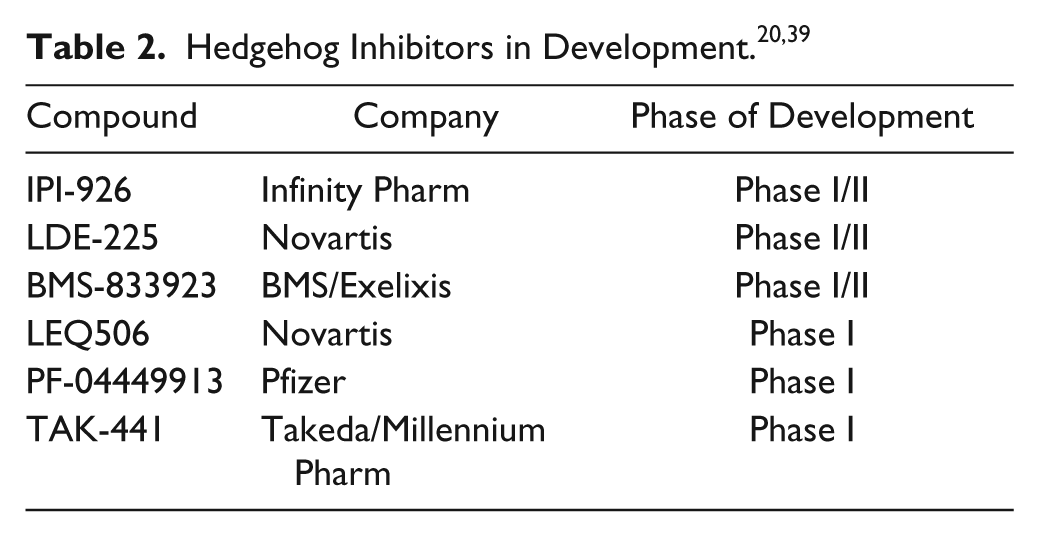
Other Hh inhibitors are being developed in an effort to improve efficacy and tolerability and to address possible resistance (Table 2). All agents currently utilized in clinical trials target SMO.17,40
Conclusion
Vismodegib is the first drug to show a response rate in prospective studies of advanced BCCs. The NCCN guidelines have incorporated vismodegib as a treatment option for both primary and recurrent BCCs. However, further studies are required to determine the utility of Hh inhibition in the setting of other malignancies. Patient tolerance and the possible development of resistance will also contribute to determining the effectiveness of vismodegib. Nonetheless, the development of the first Hh inhibitor is another model of targeted drug design in the treatment of cancer patients and provides a validated option for patients with advanced BCC.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.