
Abstract
Keywords
Introduction
Hepatitis C is one of the most common blood-borne viral infections in the United States, affecting approximately 3.2 million people. 1 The infection is often asymptomatic, but once established, at least 75% of infected patients develop chronic hepatitis C virus (HCV). 2 Until recently, the recommended first-line treatment for chronic HCV infection was pegylated interferon alfa (peg-IFN 2a or 2b) plus ribavirin (RBV) lasting 48 weeks for HCV genotypes 1 and 4 (G1/4). 3 However, sustained virological response (SVR), defined as undetectable viral load 24 weeks after therapy completion and indicating eradication of the HCV infection, was achieved in only about half of HCV monoinfected patients and in even fewer HCV/HIV coinfected patients.4-6 Many of the failures were a result of patients’ poor adherence (taking medications as directed, at prescribed frequency, and dosage strength) or persistence (taking medications for the prescribed duration) 7 with dual therapy, which in turn were often a result of the therapy’s adverse effects.5,8,9 However, there was also a certain percentage of patients whose virus simply did not respond to the regimen.5,8,9
Nonresponse to peg-IFN and RBV, or lack of efficacy (LOE), has been explored from many angles, and its cause is likely multifactorial. Observational studies of historical data have identified viral factors influencing LOE, such as baseline viral load, 10 viral kinetics in response to treatment,11-13 and the virus’s genetic diversity. 14 Patient, or host, factors that have been examined include general patient characteristics14-19 and laboratory markers such as serum proteins.20-23 Several studies have used US veteran databases to evaluate nonresponse and the likelihood of treatment discontinuation. Two studies, by Huckans et al 24 and Kramer et al, 25 have used Veterans Affairs (VA) data sets to calculate discontinuation among HCV-infected patients as a result of LOE; however, neither study identified individual factors associated with LOE. Backus et al 26 examined viral and host factors (ie, viral load, demographics, baseline laboratory values, and comorbidities) contributing to achievement of SVR but provide no insight into the relationship between these factors and LOE discontinuation. Beste et al 11 performed a robust analysis, using data from genotype 1–infected US veterans, of viral and host factors contributing to discontinuations. However, these authors excluded patients who discontinued as a result of LOE. 11
The studies described above report rates of LOE discontinuation, predictors of non-LOE discontinuation, and predictors of nonresponse to HCV dual therapy. No study, to date, has identified host factors as predictors of LOE discontinuation. Our study fills this gap by using a national electronic medical record (EMR) database to evaluate patient characteristics that predict discontinuation of dual therapy as a result of LOE. In the new era of triple therapy, in which clinical guidelines27,28 recommend adding protease inhibitors to peg-IFN and RBV to improve SVR rates in genotype-1 HCV,29-34 understanding factors related to treatment LOE discontinuation of peg-IFN may shed light on clinical decision making with regard to nonresponse stopping rules.
Materials and Methods
Design and Data Sets
This historical cohort study used data from a national cohort of United States (US) veterans obtained from the VA Informatics and Computing Infrastructure environment. Specific data sets included Corporate Data Warehouse (CDW) data for height, weight, pharmacy records, and laboratory test results and Medical SAS data sets for death dates as well as inpatient and outpatient visits, including procedures and diagnosis codes. Patient care notes for all liver-clinic patients nationwide were also obtained from CDW, and natural language processing techniques were applied to extract additional information from these narrative records. The information obtained from clinic notes for the current analysis included HCV genotype in patients with missing laboratory data. Genotype laboratory results were extracted directly into discrete fields for analysis to augment other sources of laboratory data.
Patient Selection
Included in the cohort were all US veterans (a) with an International Classification of Diseases, 9th Revision (ICD-9) HCV diagnosis code (ie, 070.41, 070.44, 070.51, 070.54, 070.70, 070.71, or V02.62); (b) with an inpatient/outpatient encounter between January 1, 2004, and December 31, 2009, as documented in Medical SAS data; (c) who initiated therapy with peg-IFN 2a or 2b plus RBV (each drug within 30 days of the other) during this study period, as documented in CDW pharmacy record data; and (d) who had viral genotype lab result indicating HCV genotypes 1 or 4. The date of the first prescription fill for peg-IFN during the study period was defined as the index date.
Excluded from the cohort were patients who did not demonstrate a pattern of receiving routine care in the VA for at least 6 months (defined as at least 1 outpatient visit more than 180 days prior, found in Medical SAS data), so as to ensure that patients were truly HCV treatment naïve for at least 6 months. We also excluded (a) patients whose pharmacy data contained missing or invalid National Drug Code numbers, quantities dispensed, or days supplied, such that we could not determine the true duration of therapy; (b) patients who died before the end of the target treatment duration of 44 weeks; and (c) patients with insufficient HCV-RNA viral load laboratory data to determine virological responses to therapy, which were used to classify discontinuations in patients who persisted beyond 10 weeks.
Institutional review board (IRB) approval for this study was obtained through the University of Utah’s IRB and the VA’s Office of Research and Development. This work was conducted in compliance with the requirements of the University of Utah’s IRB. All relevant ethical safeguards have been met in relation to patient or subject protection.
Independent Variables
Independent variables were those available in structured electronic medical records that had known or theoretical associations with discontinuation or nonresponse and were captured in the 6 months prior to index date.14,35,36 They comprised demographics (age, body mass index, marital status, race, and sex); comorbid diagnoses (alcohol abuse, chronic fatigue, cirrhosis, chronic obstructive pulmonary disorder [COPD], cerebrovascular disease, dementia, depression/anxiety/psychosis, drug abuse, HIV, cancer/malignancies, myocardial infarction/congestive heart failure, osteoarthritis, plegia, renal disease, rheumatoid arthritis, sleep apnea, other sleep disorders, and ulcers); laboratory observations (albumin, alanine aminotransferase, bilirubin, creatinine, hemoglobin, low-density lipoprotein [LDL], and platelet counts); and drug exposures (alcohol addiction treatment, cancer, COPD, dementia, depression, diabetes, drug abuse, HIV, insomnia, opioids, rheumatoid arthritis, sleep somnolence, smoking cessation, and ulcer).
Outcome
The outcome in our analysis was LOE discontinuation. All patients who failed to complete at least 44 weeks of peg-IFN were classified as either LOE or non-LOE discontinuers, according to the discontinuation classification rule shown in Table 1, which is based on current HCV treatment guidelines.27,28 Each patient’s classification depended on (a) persistence with therapy, as demonstrated by pharmacy refills (ie, persistence condition), and (b) the HCV-RNA viral load results subsequently ordered by clinicians at recommended milestones27,28 to determine whether the patient’s virus was responding to therapy (ie, laboratory condition). Essentially, patients were considered to have discontinued for LOE reasons if they (a) persisted/received refills for at least 10 weeks and (b) had subsequent HCV-RNA viral load results indicating that the virus was not responding to therapy, after week 10 and before discontinuing. Patients who completed at least 44 weeks of peg-IFN (according to pharmacy refill records) were classified as completed. Patients who died before the end of 44 weeks of treatment and those with insufficient HCV-RNA viral load laboratory data to determine response to therapy were excluded (see Patient Selection subsection and Table 1).
Discontinuation Classification Rule. a
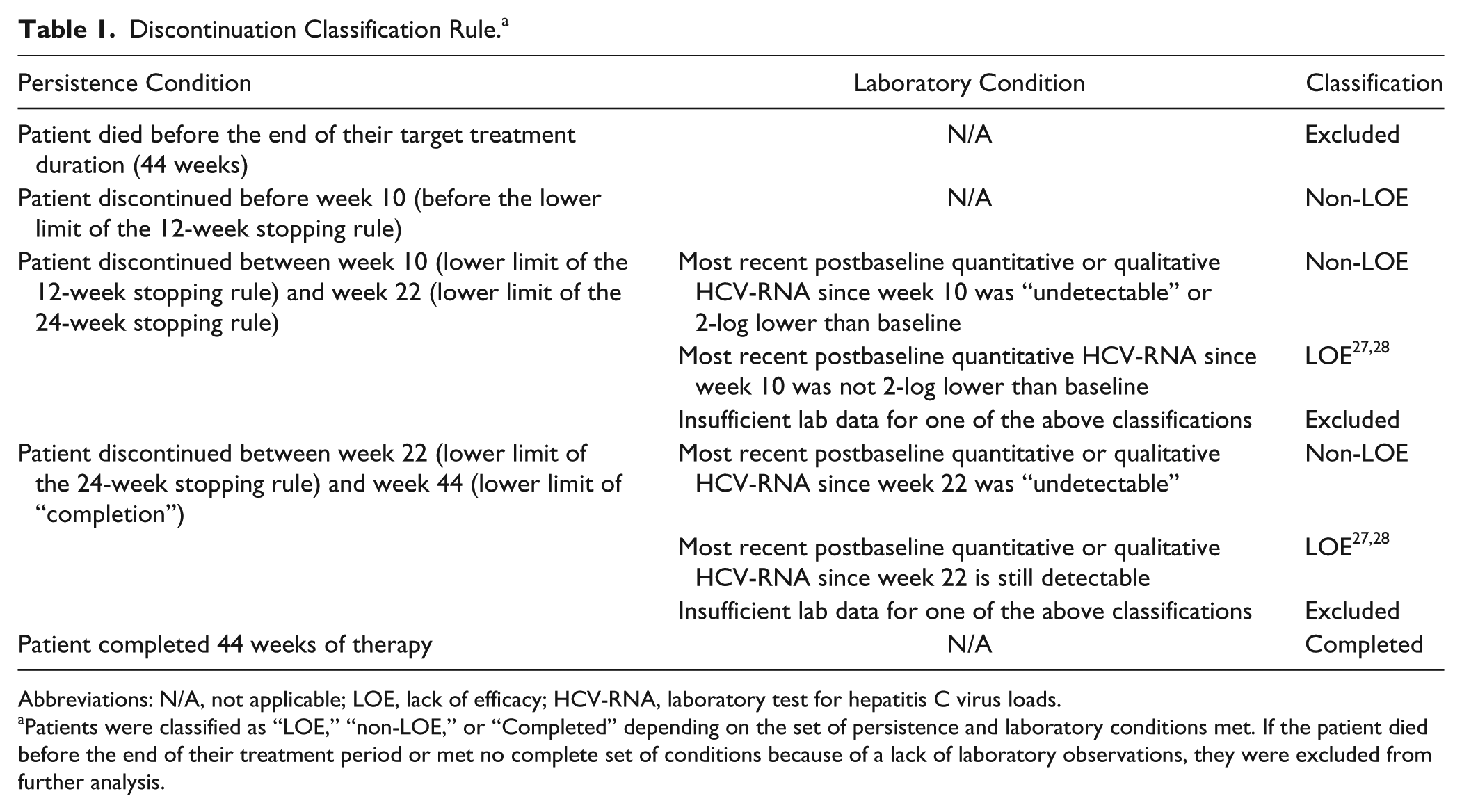
Abbreviations: N/A, not applicable; LOE, lack of efficacy; HCV-RNA, laboratory test for hepatitis C virus loads.
Patients were classified as “LOE,” “non-LOE,” or “Completed” depending on the set of persistence and laboratory conditions met. If the patient died before the end of their treatment period or met no complete set of conditions because of a lack of laboratory observations, they were excluded from further analysis.
Statistical Analysis
We built univariate and multivariable Cox proportional hazards regression models (using continuous time-to-discontinuation data) to identify the independent variables that were predictors of LOE discontinuation. We used a combination of forward stepwise and backward selection for the multivariable models, with stepwise elimination if P >0.1. Variables were added one at a time, and all previously included variables were retested at each iteration; those with P <0.1 remained in the model. Statistical analyses were conducted using SAS version 9.2 and Stata version 12.
Results
An attrition summary for cohort selection is shown in Figure 1. Out of 321 238 HCV patients with an ICD-9 code for HCV infection, 31 215 (9.7%) initiated dual therapy with peg-IFN plus RBV; 10 333 (3.2%) met all inclusion criteria and were included in the Cox regression analysis. Of these 10 333, 152 patients (1.5%) were genotype 4, and 10 181 (98.5%) were genotype 1. The mean age of the Cox regression cohort was 53.4 (SD = 6.0) years, and 96.0% were male (Table 2). As summarized in Figure 2, 13.6% of patients discontinued therapy as a result of LOE. The mean (SD) duration of therapy was 33.7 (22.5) weeks.
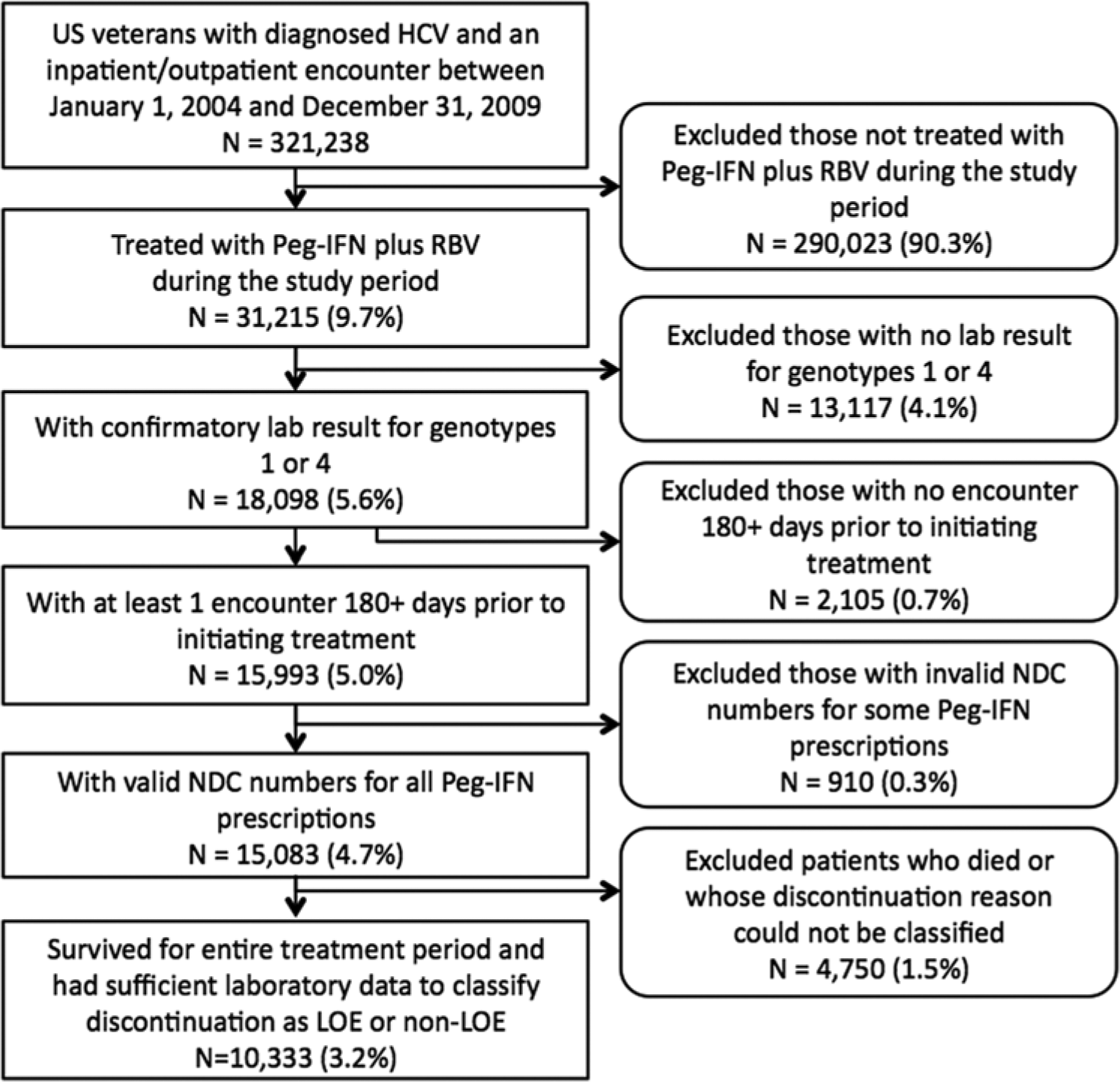
Attrition summary.
Patient Characteristics of the Cohort (n = 10 333).
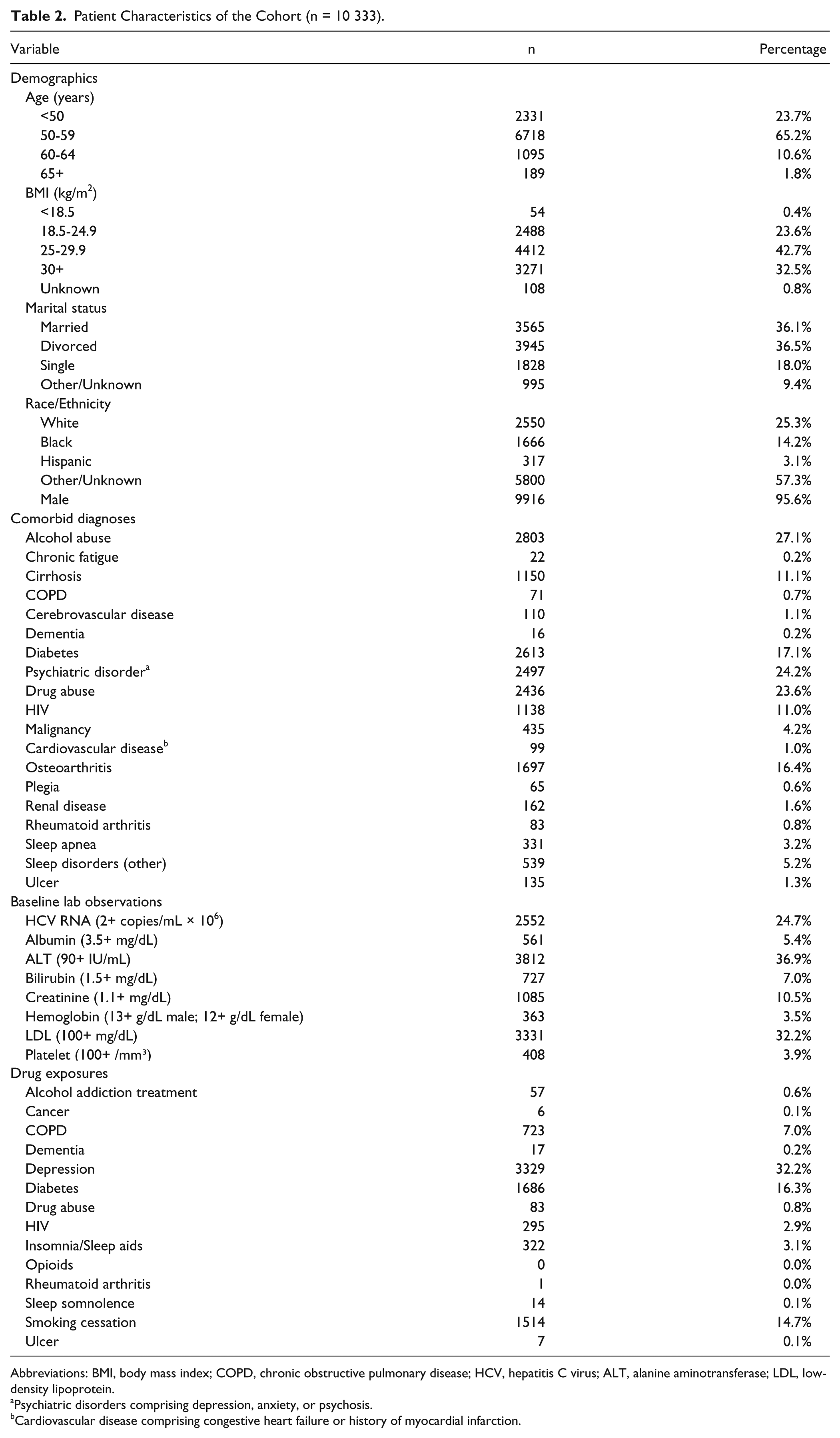
Abbreviations: BMI, body mass index; COPD, chronic obstructive pulmonary disease; HCV, hepatitis C virus; ALT, alanine aminotransferase; LDL, low-density lipoprotein.
Psychiatric disorders comprising depression, anxiety, or psychosis.
Cardiovascular disease comprising congestive heart failure or history of myocardial infarction.
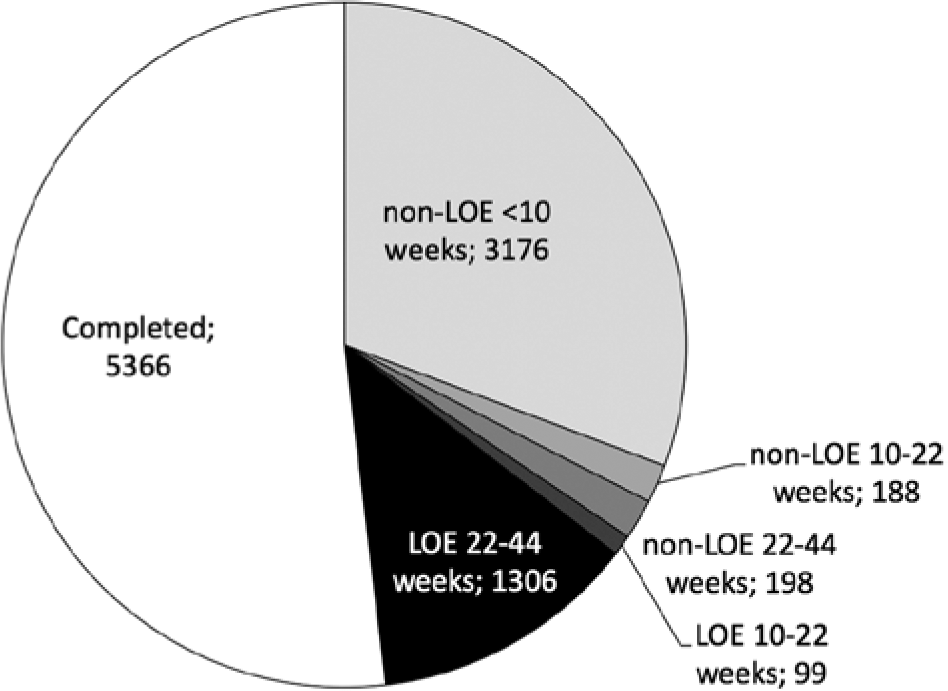
Summary of patient discontinuation outcomes by genotype, discontinuation type, and time to discontinuation.
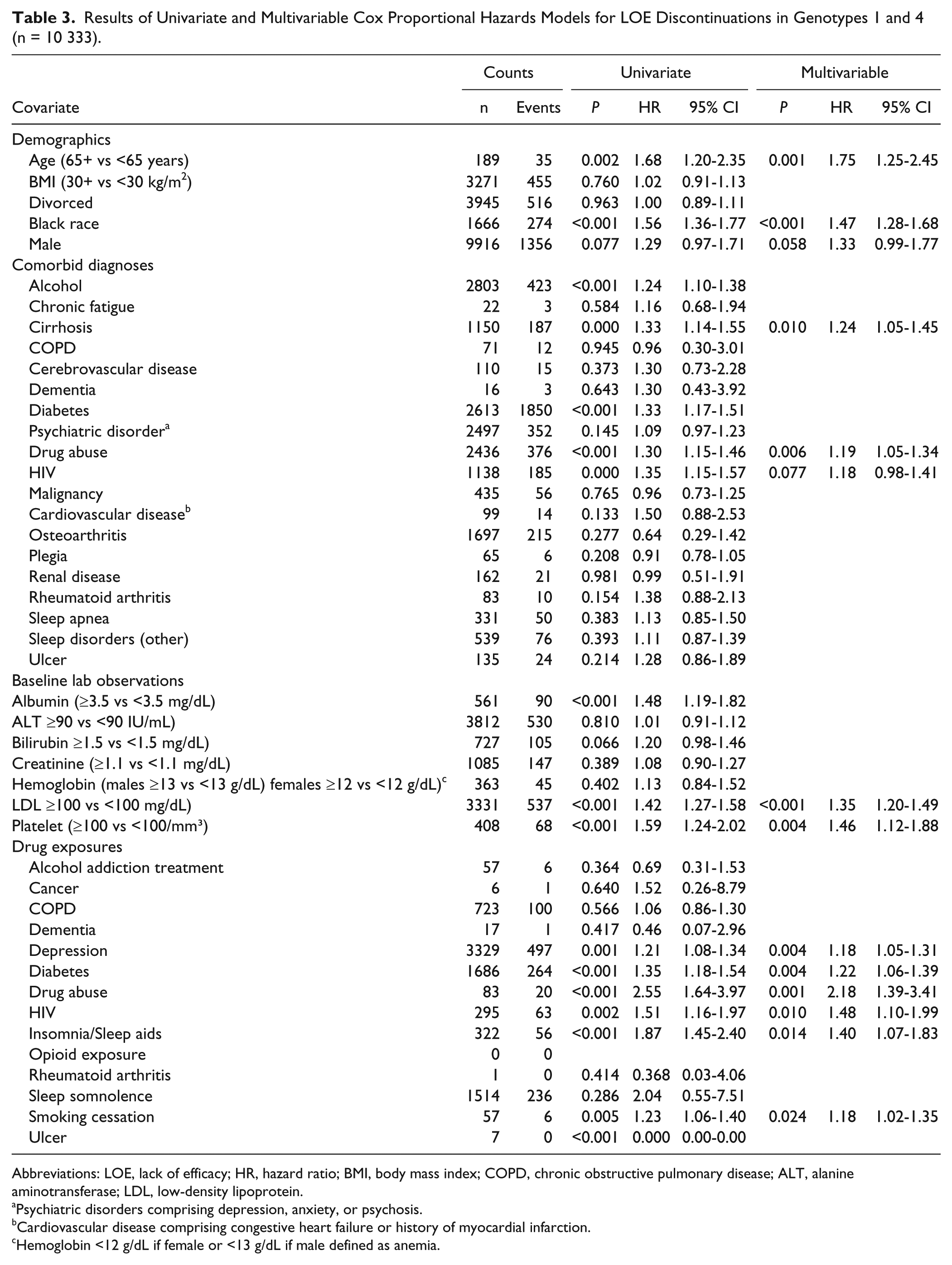
The results of multivariable models for predicting LOE discontinuation are summarized in Table 3. The strongest predictors of LOE discontinuation in terms of the magnitude of hazard ratio (HR) were treatment for drug abuse (HR = 2.18), age >65 years (HR = 1.75), antiretroviral therapy for HIV (HR = 1.48), black race (HR = 1.47), platelet count >100/mm3 (HR = 1.46), and drug therapy for insomnia (HR = 1.40). Additional significant risk factors included comorbidities of cirrhosis (HR = 1.24) and drug abuse (HR = 1.19), LDL ≥100 mg/dL (HR = 1.35), and medication taken for depression (HR = 1.18), diabetes (HR = 1.22), and smoking cessation (HR = 1.18). Many laboratory observations were not significant predictors of LOE discontinuation, including low albumin, high alanine aminotransferase, high bilirubin, high serum creatinine, and low hemoglobin.
Results of Univariate and Multivariable Cox Proportional Hazards Models for LOE Discontinuations in Genotypes 1 and 4 (n = 10 333).
Abbreviations: LOE, lack of efficacy; HR, hazard ratio; BMI, body mass index; COPD, chronic obstructive pulmonary disease; ALT, alanine aminotransferase; LDL, low-density lipoprotein.
Psychiatric disorders comprising depression, anxiety, or psychosis.
Cardiovascular disease comprising congestive heart failure or history of myocardial infarction.
Hemoglobin <12 g/dL if female or <13 g/dL if male defined as anemia.
Discussion
Whereas many studies have evaluated predictors of nonresponse to dual therapy, ours is the first to characterize LOE-related discontinuation using real-world data and to identify associated predictors for genotypes 1 and 4.
Our rate of LOE discontinuation was 13.6% of all patients who initiated therapy and had sufficient laboratory data to classify discontinuation reason, which is at the bottom of the range of documented LOE rates. It is worth noting that our LOE discontinuation rate (13.6% in genotypes 1 and 4) is comparable to that found in the study by Beste et al 11 (16.5% in genotype 1), particularly considering our more stringent definition of LOE discontinuation (completion of less than 44 out of 48 weeks of therapy and considering a gap length of longer than 60 days as a “discontinuation,” versus <80% of the recommended duration in Beste et al 11 ). Clinical trials have consistently shown higher nonresponse rates, ranging from 14% to 40%.5,37,38 One potential reason for low LOE rates in our study (compared with clinical trials) was the high early non-LOE discontinuation rate that we observed; 30.3% of patients discontinued treatment in the first 10 weeks, before persisting long enough to determine if they would have a virological response. Another reason may be that the patients included in the clinical trials are those with much more severe disease than those who were treated in a real-world setting and were captured in our data. Even though the mean baseline HCV RNA level for patients in our study (3.5 copies/mL × 106) was within the range of values reported in clinical trials (1.7-6.0 copies/mL × 106), only 55% of the patients in our study had nonmissing values for this laboratory measure, thus making it difficult to truly compare the study populations.
Factors significantly associated with LOE discontinuation were demographics, such as age >65 years and black race; comorbidities, such as cirrhosis and drug abuse; lab values of platelets >100/mm3 and LDL ≥100 mg/dL; and medications used to treat depression, diabetes, drug withdrawal, HIV, insomnia, and smoking cessation. In contrast, we had expected that most factors associated with LOE discontinuation would be biological/pathological factors, such as baseline laboratory abnormalities.39-42 Although certain demographics such as older age and black race appear to have a biological connection to viral response,43-45 we also identified many behavioral factors as independent predictors, such as drug abuse, depression, and smoking, which are traditionally associated with disease-state independent adherence and persistence behaviors.46-49
Several of the factors found to be significantly associated with LOE discontinuation deserve additional comment. First, advanced age significantly increased the risk of ineffective therapy. This is especially concerning because the number of older HCV patients is projected to increase at least through the next decade.50,51 Triple therapy will help in this regard because several studies have shown that adding a protease inhibitor to peg-IFN and RBV should increase SVR across all age brackets.29-34 Second, platelet count >100 mg/dL was found to increase the risk of LOE discontinuation. High platelet count may be an indicator for other conditions such as inflammatory bowel disease or serious infection.52-54
The high correlation between behavioral-type factors and LOE discontinuation suggests several potential hypotheses. The first is that patients with these characteristics were less adherent in the weeks prior to their LOE discontinuation, diminishing viral response, and the consequence was LOE discontinuation. In fact, we calculated an average medication possession ratio, a commonly used method for measuring adherence that has been used in several published studies dealing with HCV,55-57 in the first 10 weeks for LOE discontinuers of 96%, compared with 97% among completers; the difference was minimal and is thus unlikely to be an explanation for our findings. A second potential hypothesis is that clinicians’ LOE discontinuation decisions may not be based on laboratory response data alone, but may also be based on their perceptions about patient behaviors and characteristics. Clinicians may simply be more likely to recommend discontinuation in patients with an underwhelming response to therapy depending on these characteristics.
Although ours is the first to predict LOE discontinuation in G1/4, numerous multivariable models attempting to predict nonresponse (independently of discontinuation behavior) have preceded ours.10,12,14,16,17,36,58,59 The small scale and relative diversity of candidate predictors (some of which are rather obscure) identified in most of these models make them minimally useful in a clinical setting. Although viral genotype 60 and baseline viral load 10 are constituent data in the clinical management of HCV, clinicians have little reason to routinely test for other potential predictors such as viral genetic diversity, 14 gene expression,59,61,62 or obscure laboratory or histological markers such as interferon-γ inducible protein 1063 or anti-NS4a antibodies. 64 Testing for these factors is currently time-consuming, expensive, or both, largely without substantial support that they consistently predict response to treatment. An exception to this is IL28B genotype testing, which is becoming a frequently used, cost-effective predictor of response to treatment in chronic HCV patients with G1/4. 65 This test was not available during the time period of our study and was thus not included in this analysis.
Because peg-IFN will remain a component of triple therapy, along with RBV and a protease inhibitor, we expect that our prediction model will remain useful in the current era of triple therapy, despite the improved SVR rates documented in clinical trials. 29-34 It is worth noting that interferon-free therapies—comprising various polymerase inhibitors designed to directly target the virus rather than the patient’s immune system—are being developed, with SVRs projected to be 90%.66-69 These therapies are expected to be available in 2014 or 2015. The near certainty of SVR may be enough to overcome some of the seemingly behavioral or adherence-pattern predictors of LOE found in our study.
Limitations
This analysis is subject to some limitations. First, we only captured patient information within the VA health care system. Although we made efforts to ensure that patients were receiving routine care in the VA by looking for encounters at least 6 months prior to the index date, some patients could have received prescriptions and follow-up outside the VA, although the very low copays in the VA act as an incentive for veterans to fill their interferon prescriptions in the VA. In addition, whereas the VA setting was chosen for this study in part because of the richness of the available EMR data and the wide geographical representation, veterans with HCV may not be representative of the general US population of HCV patients.
A major limitation, perhaps not of the study methodology but of the data sources, was the necessity of excluding more than 5000 patients because of our inability to find data on treatment response. Some patients may have had laboratory results that were not in the structured data and were never incorporated into clinic notes that we mined using natural language processing. If these patients had been nonresponders, then the proportion of LOE discontinuers we observed could well have been much higher. However, a plausible mechanism for the missing data is that many patients whose laboratory response data were never entered into the medical record were, in fact, never tested for a response, suggesting that a majority of them might have been non-LOE discontinuers.
In using historical EMR data in each aspect of our study, we explicitly assumed that patients took the medications that were in the prescriptions they filled; we identified discontinuation dates based on fill dates and days supplied for prescriptions in the patients’ pharmacy records. An implication of this is that we were unable to adjust our discontinuation outcome for missed doses. Our data source also required us to use ICD-9 codes to determine the presence of comorbid conditions. This may be inaccurate because some patients’ recorded diagnoses may not be completely accurate in their health records. Although these assumptions likely led to misclassification of some patients (as being discontinuers in the case of pharmacy records and as having or not having certain comorbid conditions in the case of ICD-9 codes), these are common concerns with any observational studies using historical electronic records. We feel that with the ability to conduct this study in a cohort that is national in scope, to include medication exposures and laboratory results as additional independent variables, and to supplement genotype information found in structured lab data with that embedded in unstructured clinical narrative, the benefits of using electronic data from the VA far outweigh the costs.
Conclusions
We found that 13.6% of patients in our cohort of treated HCV patients discontinued because of nonresponse, which was much lower than the proportion of patients who discontinued for other reasons (30%). Factors significantly associated with LOE discontinuation were demographics, such as age >65 years and black race; comorbidities, such as cirrhosis and drug abuse; lab values of platelets >100/mm3 and LDL ≥100 mg/dL; and medication used to treat depression, diabetes, drug withdrawal, HIV, insomnia, and smoking cessation. Our results suggest that many host factors may contribute to LOE discontinuation rates in veterans. Future work should focus on determining whether these characteristics are also predictive of triple-therapy LOE discontinuations.
Footnotes
Authors’ Note
A preliminary version of this work was presented at the Liver Meeting of the American Association for the Study of Liver Diseases in San Francisco, California, in November 2011.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: RH is an employee of the sponsor and owns stock in Genentech and Roche. EK is an employee of the sponsor and owns stock in Genentech and Roche. SDV has received research grants from Anolinx LLC, Genentech Inc, F Hoffmann-La Roche Ltd, Amgen Inc, Shire PLC, Mylan Specialty LP, and Merck & Co, Inc, and was a partner in 2010-2011 for Clinical Methods. CLH is an employee of the University of Utah Department of Internal Medicine. KK is an employee of the University of Utah Department of Pharmacotherapy. TM has received research funding to perform clinical trials from Roche, Merck, Bristol-Myers-Squibb, Genentech, Gilead, and Vertex. PP has been a speaker at Onyx/Bayer, Vertex, and Genentech and has received research support from Genentech, Roche, and Merck. JH is an employee of the sponsor and owns stock in Genentech and Roche. JLF has been sponsored by Agency for Healthcare Research and Quality (AHRQ; HS018582), Department of Defense Congressionally Directed Medical Research Programs, ASHP Foundation Federal Services Junior Investigator Research Grant Program, University of Utah Center on Aging Pilot Grant Program, Center for Medicare Medicaid Services Medicaid Transformation Grant, Veterans Affairs Rocky Mountain Acquisition Center, Anolinx, Amgen, Clinical Methods, Centers for Disease Control, Genentech, Norvartis, and Utah Department of Health.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was sponsored by a grant from Genentech. REN was supported in part by funding from the National Institutes of Health and the National Cancer Institute Grant 1 KM1CA156723 and the National Institutes of Health Office of the Director Grant \5TL1RR025762-03. He has also been funded by Anolinx, Genentech, Centers for Disease Control and Prevention (CDC), VA Health Services Research & Development (HSR&D), Agency for Healthcare Research and Quality (AHRQ), and VA Office of Rural Health (ORH).