
Abstract
Introduction
Cardiovascular (CV) drug shortages rank among the top 5 drug classes for active drug shortages nationally and, therefore, pose a major threat to patient care and public health. The Food and Drug Administration (FDA) defines drug shortages as products used to prevent or treat a serious or life-threatening disease or medical condition for which there is no other available source with sufficient supply of that product or alternative drug available. Consequences of these shortages include changes in the way the drug is prepared or a need to change patient care management that requires providers to select a less-than-desirable therapeutic alternative. There were 294 active drug shortages nationally in the third quarter of 2013 with a mean duration of 19 months (Erin Fox, personal communication, June 11, 2013). 1 In 2012, there was a minor decrease in new shortages, with 204 identified compared with 267 in 2011 (see Figure 1). Identifiable causes for shortages include unknown etiologies (44%), manufacturing issues (36%), supply/demand incongruities (8%), discontinuations (8%), and lack of raw materials (4%; Erin Fox, personal communication, June 11, 2013).
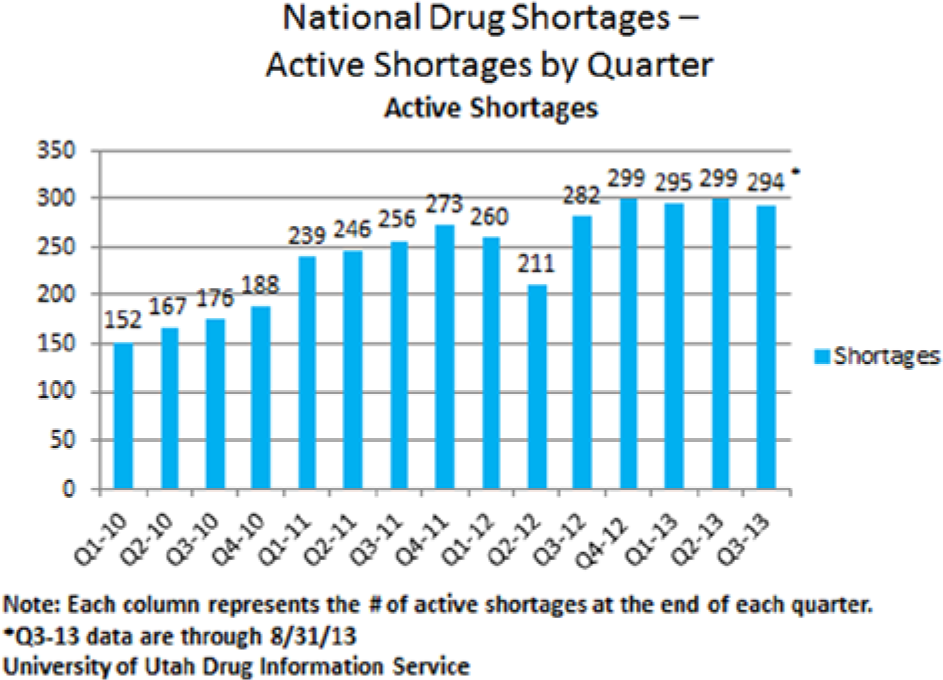
Incidence of drug shortages within the United States since 2010.
Drug shortages span all major therapeutic classes, including central nervous system (17%), anti-infectives (12.5%), parenteral nutrition (10.5%), oncology (9.6%), and CV (8.9%). Of all shortages, 25 active CV drug shortages have been identified as of August 31, 2013 (Erin Fox, personal communication, June 11, 2013). Compared with national shortage trends, CV shortages consist mainly of generic sterile injectables but differ in that the majority are manufactured by more than 4 pharmaceutical companies (most products that usually suffer from a shortage are made by fewer than 2 drug manufacturers). Drugs shortages within other classes may have a direct impact on CV patient care, including anesthesia (propofol, atropine, and succinylcholine) and parenteral nutrition (calcium, trace elements, electrolytes, and multivitamin). However, for the purpose of this article, we have identified 13 critical direct CV shortages and their alternatives (Table 1) that either have or are likely to have a significant impact on the care of patients with CV disorders.
Historical and Current Cardiovascular Drug Shortages.
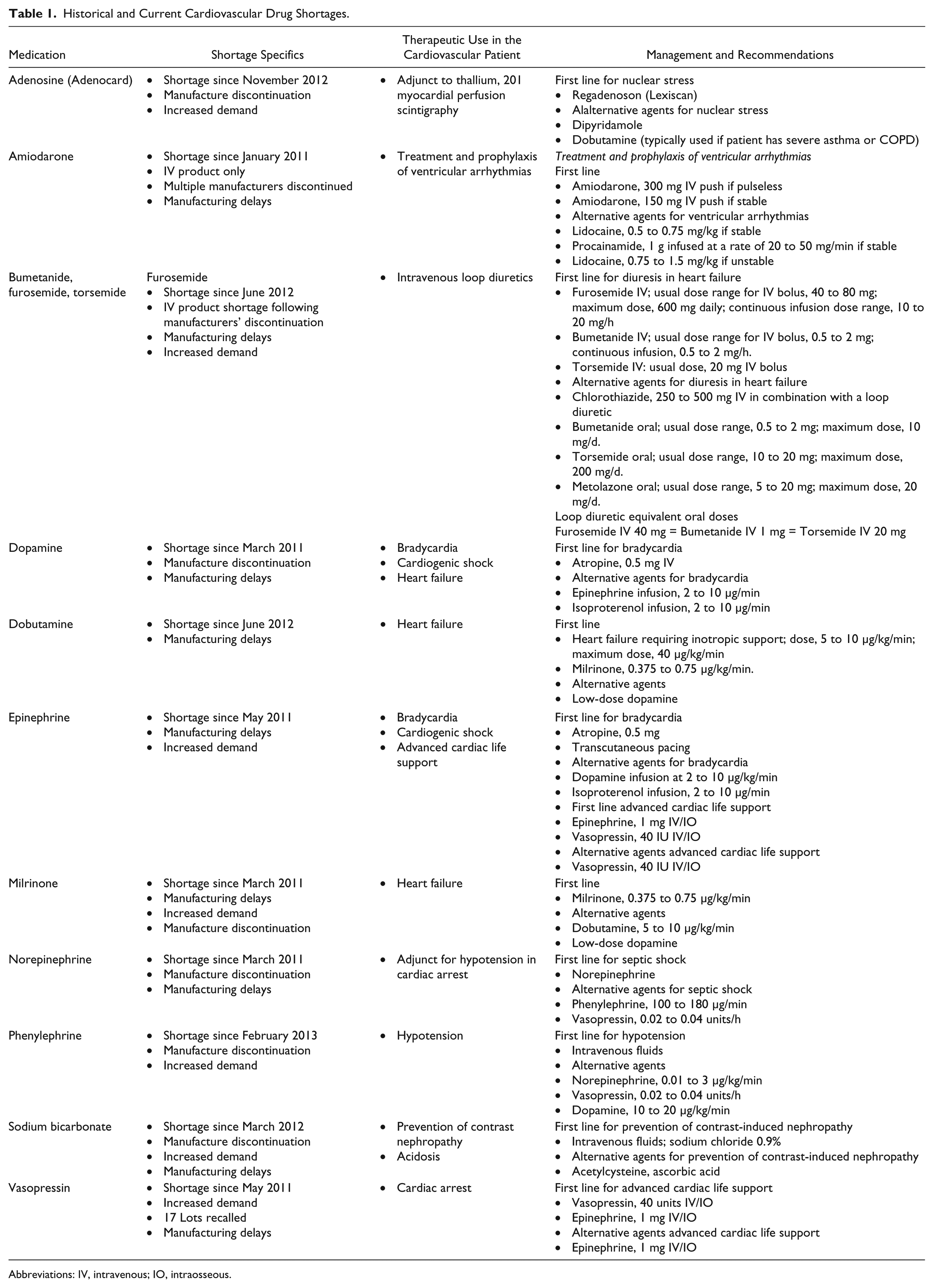
Abbreviations: IV, intravenous; IO, intraosseous.
Shortages have posed both minor and major disruptions to hospitals and clinics depending on the limited availability of the products and whether there are adequate therapeutic alternatives. According to the Institute for Safe Medication Practices (ISMP), 15 patient deaths occurred that were directly attributed to errors, which in turn were directly attributed to drug shortages. 2 In a 2010 ISMP survey, providers indicated that they experienced a near miss (35%), actual error (25%), or adverse patient outcome (20%). 3
As a direct result of drug shortages, managing the constant movement of inventory levels, backorders, order sets, and communication to physicians, pharmacists, nurses, and other allied health professionals presents significant challenges. Statistics demonstrate that the overall labor costs associated to oversee a drug shortage program is estimated to be $216 million annually. 4 A report from the University of Utah Hospitals and Clinics noted that 13% of shortages at their institution resulted in increased costs and 33% in decreased costs, and 54% had an unknown or neutral effect. 5 A Premier Healthcare Alliance survey in 2011 estimated that drug shortages cost hospitals $200 million per year. 6
In response to this growing issue, there was a Presidential Executive Order released in October 2011 for drug shortages that allows the FDA to broaden reporting of potential shortages, expedite regulatory reviews, and increase staffing resources for the FDA’s shortage program. 7 In July 2012, President Obama signed The Food and Drug Administration Safety and Innovation Act. This legislation required manufacturers to notify the FDA of production interruptions and discontinuations at least 6 months in advance, gives the FDA authority to speed approval of products and new drug applications, and creates a generic user fee program intended to stimulate FDA approval of generics. 8 Thus, voluntary early notification from manufacturers allowed the FDA to prevent 295 drug shortages in 2012. 9 In March 2013, the American College of Cardiology (ACC) responded to FDA Commissioner Margaret Hamburg’s request for comments to the FDA’s Drug Shortages Task Force and Strategic Plan. The ACC “urged the FDA to act swiftly to reduce the Agency-related causes of drug shortages and to work with manufacturers to address the manufacturing-related causes of drug shortages.” 10
With the ongoing shortages of CV medications, clinicians need to continue to proactively manage the shortage and alternative product supplies for this patient population. The purpose of this review is to discuss CV drug shortages and provide recommendations for managing each specific shortage. The overarching management and strategies to optimize care surrounding shortages will also be discussed.
Specific CV Medication Shortages
Antiarrhythmic Agents
Adenosine
Adenosine is utilized as an antiarrhythmic agent as well as for myocardial perfusion scintigraphy. As an antiarrhythmic, adenosine (Adenocard) is primarily used for the treatment of paroxysmal supraventricular tachycardia (PSVT) and works by slowing impulse formation in the sinoatrial node as well as slowing conduction time through the atrioventricular node. Additionally, adenosine can interrupt reentry pathways through the atrioventricular node. As a diagnostic tool, adenosine (Adenoscan) is used as an adjunct to a thallium stress test in patients who are unable to exercise. In this capacity, adenosine is used to enhance coronary blood flow through coronary vasodilation to aid in the identification of areas within the coronary arteries that have reduced uptake and slower washout of the thallium to aid in the identification of stenotic lesions. Several manufacturers have discontinued Adenocard for the management of PSVT. However, existing manufacturers have been able to maintain ample supply. On the other side, Adenoscan is in short supply secondary to a manufacture back-order that was propagated by an increase in demand. Fortunately, there are reasonable alternatives to Adenocard, including dipyridamole, dobutamine, and regadenoson (Lexiscan). This shortage is likely to have more of a financial impact rather than an impact on patient care. Although regadenoson is often the preferred agent, in large part because of the convenience secondary to a longer half-life, and it can be given via a bolus over an infusion, its cost is substantially higher. The average wholesale price of regadenoson is $262.84 compared with $42.34 for adenosine. 11 Institutions may be limiting the use of regadenoson in an effort to decrease expenditures; however, the shortage may ultimately drive costs upward.
Amiodarone
Intravenous amiodarone is a class III antiarrhythmic that possesses electrophysiological properties of all 4 of the Vaughn Williams classes. This agent is one of the most commonly used antiarrhythmic agents. Intravenous amiodarone is utilized for the acute management of stable and unstable ventricular tachycardia, ventricular fibrillation, and shock-refractory ventricular tachycardia. Although there are alternatives such as lidocaine and procainamide, only lidocaine is an alternative in the management of unstable ventricular tachycardia and ventricular fibrillation. Procainamide has to be administered as an infusion and is, therefore, only indicated in stable ventricular tachycardia. Despite having additional options, the efficacy of amiodarone is superior to lidocaine for shock-resistant ventricular tachycardia and is considered first-line therapy. 12 The use of intravenous amiodarone has been shown to improve survival to hospital admission in patients suffering from out-of-hospital cardiac arrest by 26% compared with placebo. 13 The shortage of intravenous amiodarone is secondary to a number of manufacturers discontinuing the product and the remaining companies being unable to keep up with the demand. The impact of this shortage will force health care providers to use alternative agents that are less efficacious, ultimately affecting their ability to provide one of the best treatment options available. This shortage may seem crucial, but one must take into consideration that although amiodarone has been shown to increase survival to hospital admission, it is unclear if that correlates to an increase in survival to discharge with a good neurological outcome. Additionally, when it comes to the management of life-threatening arrhythmias, the fundamentals included in the chain of survival (early recognition, early CPR with emphasis on initiation of chest compressions with minimal interruptions before ventilations, rapid defibrillation, effective advanced life support, and postresuscitation care that may include therapeutic hypothermia) are paramount and are the initial treatment modalities, many of which should be used prior to antiarrhythmic therapy administration. 14 This shortage may help reinforce these principles that are necessary to optimize outcomes.
Intravenous Loop Diuretics
Furosemide and Bumetanide
The loop diuretics are considered the cornerstone of therapy in the management of volume overload in patients with heart failure. These medications work by blocking sodium and water reabsorption in the ascending limb of the loop of Henle. The amount of sodium reabsorption blocked is approximately 20% to 25%. Intravenous furosemide is often utilized in the hospital setting in patients who present with significant volume overload. The reason is 2-fold: (1) patients with heart failure and significant volume overload often suffer from gut edema, thus affecting absorption, and (2) oral furosemide is approximately 40% bioavailable. Both these issues combined result in decreased efficacy and the need for intravenous therapy. The furosemide shortage occurred as a result of temporary suspension of production as well as manufacturing delays and manufacture discontinuation. This shortage led clinicians to use other available intravenous loop diuretics—bumetanide and torsemide. This in turn led to shortages of these drugs. One strategy to manage the shortage is to use whatever intravenous loop diuretic can be obtained. Comparable doses of these agents are not completely understood; however, a ratio of 40:20:1 (furosemide:torsemide:bumetanide) is frequently used as a starting point when using an alternative agent. 15 Outside of the loop diuretics, there are few alternatives for managing this patient population. Chlorothiazide, a thiazide diuretic, is available as an intravenous formulation. However, it is expensive and works in the distal tubule inhibiting only 10% to 15% of sodium reabsorption compared with the 20% to 25% that is inhibited by the loop diuretic class. Therefore, these agents are not as effective as a loop diuretic when used as monotherapy. Additionally, in the setting of reduced renal function (creatinine clearance < 30 mL/min), the efficacy of chlorothiazide is minimal. Metolazone, an oral thiazide diuretic has better efficacy when renal function is reduced and may be an alternative to chlorothiazide in this setting. The combination of an oral loop diuretic, such as bumetanide or torsemide, along with a thiazide, such as chlorothiazide or metolazone, can be very effective in achieving diuresis. Both bumetanide and torsemide are approximately 96% bioavailable when administered orally and can be used if intravenous therapy is not available.16,17 However, oral as well as intravenous torsemide is significantly more expensive (oral $8.21/20-mg tablet; $9.30/2-mL vial) compared with bumetanide (oral $4.96/1-mg tablet; IV $1.81/10-mL vial). 11
Ethacrynic acid is another loop diuretic that has been in use for more than 50 years; however, because of its high cost (oral $6.17/25-mg tablet; IV $1138/50-mg vial) and adverse effects, it is rarely used. Ultrafiltration, although inferior to pharmacological therapy, may also be considered if adequate diuresis is not achieved with pharmacological agents, although it may not be available at all institutions. 18
Vasoactive Agents
Dopamine
Dopamine is a vasoactive agent that stimulates both adrenergic and dopaminergic receptors in a dose-dependent fashion. At low doses of 1 to 3 µg/kg/min, dopamine stimulates primarily dopaminergic receptors that results in mesenteric and renal vasodilation. At medium doses of 4 to 10 µg/kg/min, both β and α receptors are stimulated, and doses above 10 µg/kg/min stimulate primarily α receptors. Dopamine is used for the management of hypotension secondary to septic or cardiogenic shock unresponsive to fluid resuscitation as well as for symptomatic bradycardia. The shortage of dopamine was created secondary to discontinuation by one manufacturer, who cited raw material supply issues as well as manufacturing delays by other suppliers. Septic or cardiogenic shock is a life-threatening problem commonly seen in intensive care settings. Many different vasoactive agents are available, including norepinephrine, phenylephrine, epinephrine, and vasopressin. There is debate as to which agent provides the most benefit in the setting of septic shock. However, recent guidelines on the management of severe sepsis and septic shock recommend norepinephrine as the drug of first choice. 19 Epinephrine or vasopressin can be added if norepinephrine does not maintain an adequate mean arterial pressure. Dopamine is not recommended except in patients at low risk for tachyarrhythmia and absolute or relative bradycardia. 19 For the treatment of symptomatic bradycardia, a continuous infusion of epinephrine may be used in the place of dopamine after atropine and transcutaneous pacing have failed. Because of the array of vasoactive agents available and because dopamine is not considered first-line therapy, the clinical impact of this shortage in this setting is likely to be minimal.
Norepinephrine
Norepinephrine acts on β-1 and α adrenergic receptors. However, the effect of norepinephrine on α receptors leading to vasoconstriction predominates over the β effects. The usual dose is 0.05 to 0.1 µg/kg/min as a continuous infusion up to a maximum dose of 2 µg/kg/min. As with many of the other medication shortages, norepinephrine has been in short supply secondary to manufacturer discontinuation as well as an increase in demand. Although there are alternative vasoactive agents, norepinephrine is considered first-line therapy for septic shock refractory to fluid resuscitation. 19 Alternatives to norepinephrine include dopamine, phenylephrine, and vasopressin. Secondary to the shortage, supply across the country reached critical levels. Institutions have been forced to remove the medication from automated dispensing cabinets and implement restrictions on who can order the medication, with some requiring attending physician approval. The overall clinical impact of this shortage is not yet known; however, the overall mortality from septic shock ranges from 13% to 50%. 20 Norepinephrine has been shown to preserve tissue perfusion in this patient population. 21
Phenylephrine
Phenylephrine is a direct-acting α-adrenergic agonist with little to no β-adrenergic activity. The usual dose of phenylephrine is 100 to 180 µg/min, administered as a continuous infusion. The shortage is related to discontinuation of phenylephrine by 3 manufacturers, with the remaining one not being able to keep up with demand. As with the other vasoactive agents, there are alternatives to phenylephrine, which include norepinephrine, dopamine, vasopressin, and epinephrine. Phenylephrine is not considered first-line therapy for septic shock, except when norepinephrine use results in cardiac arrhythmias and when blood pressure continues to be low despite good cardiac output or as salvage therapy when other agents fail to achieve hemodynamic goals. Because of many alternative agents to phenylephrine and limited data on its benefits in this setting, the clinical impact of this shortage should be minimal. 19
Epinephrine
Epinephrine stimulates β1, β2, and α1 receptors in a dose-dependent fashion. Epinephrine is utilized in the CV setting as an intravenous bolus for the management of pulseless ventricular tachycardia/ventricular fibrillation, asystole, and pulseless electrical activity (dose = 1 mg) and as a continuous infusion in the management of symptomatic bradycardia (dose = 2 to 10 µg/min). The shortage with epinephrine was primarily with the emergency syringes used in advanced cardiac life support (ACLS). Alternative dosage forms are available, such as 1-mg/mL 1-mL ampoules or vials and 1-mg/mL 30-mL vials as well as a 1-mg/10-mL emergency syringe with an attached intracardiac needle. The intracardiac syringes have a nonremovable needle that is not compatible with needless systems and, therefore, cannot be used as a substitute. Even though a 30-mL vial is available, the strength is different: 1 mg/mL versus 0.1 mg/mL, which is the strength of the emergency syringes. Attempting to use this as a replacement can lead to serious adverse events. The ISMP has reported fatal events secondary to dosing errors. Using a 30-mL vial could result in a 10-fold overdose of epinephrine if the difference in strength is not recognized. Also, epinephrine syringes cannot be prepared extemporaneously because of the fact that it is sensitive to light, air, and pH. It also has a short stability time that makes it unsuitable to be prepared in bulk. As a result of the shortage, epinephrine emergency syringes must be restricted to emergency response teams and code carts. The 30-mL syringes should not be used as a substitute for the emergency syringe because of the high risk for error. Vasopressin 40 IU may be used as an alternative to epinephrine should supplies run critically low. The clinical impact of this shortage is unknown because neither epinephrine nor vasopressin has been shown to improve outcomes in cardiac arrest, and in some cases, epinephrine may in fact reduce survival. This shortage may help enhance focus on the fundamentals of cardiopulmonary resuscitation. For use in symptomatic bradycardia, epinephrine is not considered first-line therapy, and several alternative options are available, including a dopamine infusion and transcutaneous pacing. 22
Inotropic Agents
Dobutamine and Milrinone Dobutamine stimulates β1, β2, and α receptors
However, the predominant effect is stimulation of β1 adrenergic receptors, resulting in increased heart rate and contractility. This agent is most frequently used in the treatment of decompensated heart failure. The usual dose of dobutamine is 2.5 to 20 µg/kg/min. The shortage of dobutamine has been precipitated by manufacturing delays and the temporary suspension of manufacturing by one manufacturer. The alternatives to dobutamine include milrinone and low-dose dopamine. Although milrinone is an inotrope, it has several different properties compared with dobutamine that do not always make these agents interchangeable. When compared with dobutamine, milrinone produces more vasodilation and is sometimes referred to as an inodilator. Milrinone is excreted primarily by the kidney and has a half-life of approximately 2½ hours in patients with normal renal function and may be significantly prolonged in patients with severe renal insufficiency. When shortages of dobutamine occur, if milrinone is not a suitable alternative because of concerns with blood pressure or renal function, low doses of dopamine (<4 µg/kg/min) can provide similar hemodynamic responses. 23 If higher doses of dopamine are warranted and systemic vascular resistance becomes excessive, then an additional vasodilator such as nitroprusside may be added to offset the α adrenergic effect of the high-dose dopamine.
Electrolytes
Sodium Bicarbonate
The use of sodium bicarbonate has been widely adopted for the prevention of contrast-induced nephropathy (CIN) in high-risk patients undergoing cardiac catheterization. Contrast nephropathy is defined as an increase in serum creatinine of ≥0.5 mg/dL or an increase by 25% within 28 to 72 hours following contrast exposure. This condition is the third most common cause of hospital-acquired acute renal failure. The usual dose is 3 mL/kg/h, beginning an hour prior to contrast administration and continued at a rate of 1 mL/kg for 6 hours following the procedure. 24 The initial study evaluating 119 patients receiving sodium bicarbonate compared with normal saline demonstrated that sodium bicarbonate was superior to IV hydration in preventing contrast nephropathy. However, the REMEDIAL trial evaluated several different methods of preventing CIN, including sodium bicarbonate, N-acetylcysteine, and 0.9% sodium chloride, and demonstrated that there was no benefit over normal saline in CIN prevention compared with the other methods. 25 Additional studies have corroborated these findings.26,27 Despite the results of these trials showing no benefit of sodium bicarbonate infusions in preventing CIN, many institutions have adopted its use. However, the shortage has become critical, requiring significant restrictions on the use of sodium bicarbonate, so that it can be reserved for life-threatening situations such as metabolic acidosis. As a result, cardiologists have reverted back to hydration with normal saline for CIN prevention. Institutions that monitor CIN incidence have actually found lower rates of CIN despite the shortage as a result of proper hydration. Therefore, this shortage will assist with steering clinicians back to proven therapies that will lead to positive patient outcomes.
Preparing for Drug Shortages
Because it is not feasible to predict drug shortages, it is imperative to have a plan in place that can be efficiently enacted once a drug shortage occurs. This section will review how to develop and implement such a plan within a hospital system. 28
The initial process of the plan is to ensure a strategy that can efficiently identify potential drug shortages as soon as possible (see Figure 2). Usually, this occurs by having the pharmaceutical procurement experts within the hospital cultivate a close affiliation with the drug manufacturers and product distributors. Specifics to achieve this include having direct lines of communication with the drug suppliers for the institution while also utilizing technology, such as electronic inventory monitoring systems. The procurement specialist should also monitor publicly reported drug shortages through the FDA and ASHP (American Society of Health System Pharmacists) Web sites. This, coupled with setting accurate par levels based on real-time use allows hospitals the ability to rapidly identify drug shortage issues before supplies are completely depleted. When fully operational, a system such as this usually allows for 1 to 2 weeks of lag time, although recalls may induce instantaneous shortages. Following the identification of such an issue, it is imperative that the supply experts develop a system for early communication of these issues to the multidisciplinary team.
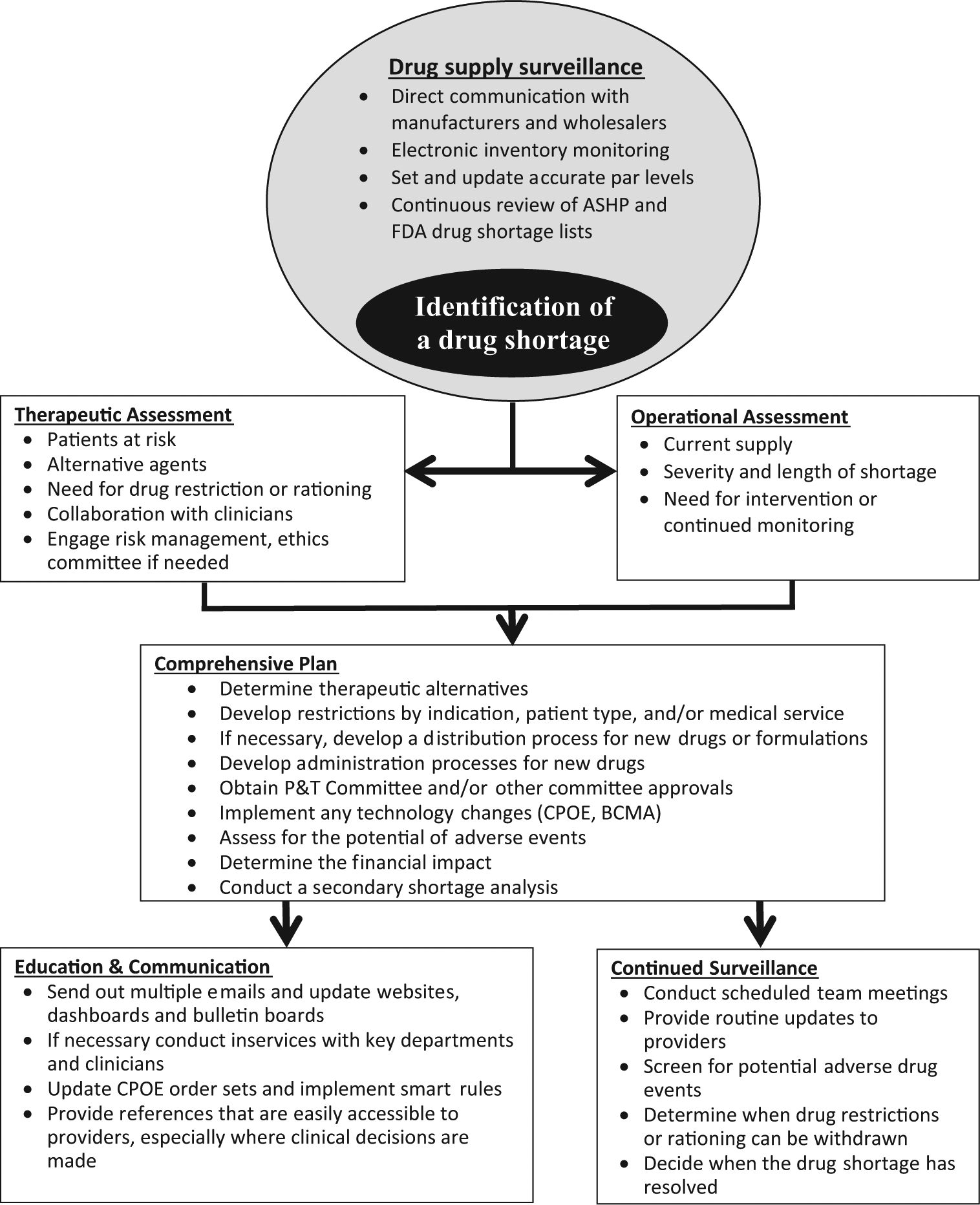
Strategic management flowchart for drug shortages.
Once a shortage is identified, operational assessment is required to determine the severity of the shortage, the remaining supply levels, and the potential duration of the shortage. This will provide detailed information that can be used to determine if interventions are required or if the shortage only requires closer survellience. 28 Following operational assessment, if deemed necessary, therapeutics evaluation commences. These evaluations will determine which patient populations will be affected by the drug shortage while also identifying any appropriate alternative therapies. The operational assessment is ideally spearheaded by the drug distribution experts; the therapeutic assessments are best directed by an interdisciplinary team of health care providers, which should include cardiologists, cardiac surgeons, radiologists, intensivists, pharmacists, and nurses. To minimize the time gap between the operational and therapeutic assessments, having a standing preidentified team that can be quickly activated is ideal.
Following the completion of these 2 assessments, the comprehensive protocol for managing the drug shortage should be developed. This protocol should include a list of therapeutic alternatives, with very detailed information, including indication, dose, route, schedule, duration, monitoring parameters, and contraindications. The protocol should also include any formulary-related issues, including restrictions (either by indication or service type) and patient-specific selection criteria. An example of this would be to use adenosine only for PSVT and restrict use in cardiac imaging while a severe shortage is being experienced. The plan should also include the process needed to ensure appropriate distribution of the alternatives to prevent medication safety issues. An example of this would be if a recommended alternative is changing how a medication is supplied, such as a small vial size or pharmacy repackaging. Additional considerations that should be included within the protocol include drug administration issues (changing from one route to another), cost-related decision trees (if the alternative product is substantially more expensive), and the potential for secondary shortages (ie, if norepinephrine is on shortage and hospitals start using more phenylephrine as an alternative, will this lead to a shortage of phenylephrine).
Education and communication are the final and probably one of the most crucial components of the drug shortage planning process. This is likely also one of the difficult parts of this plan, one that if not conducted appropriately can lead to medication errors. Any health care provider who may be affected by the shortage should be well educated regarding the above-mentioned comprehensive protocol, especially as it related to alternative therapeutic regimens. This list of personnel can include physicians, physician extenders, pharmacists, nurses, and other allied health disciplines. Medication errors have occurred from drug shortages. Hydromorphone was used by a hospital system when morphine was on shortage, leading to a clinically significant overdose. Specific to cardiology, there was a significant epinephrine overdose encountered by a hospital system when a higher-concentration syringe was used as an alternative to a low-concentration vial that was on shortage.29,30 At our institution, shortages of vasoactive drugs caused significant issues related to dosing misunderstandings when prescribers ordered alternative products with which they had limited experience. Therefore, education strategies need to include information that providers can easily access within patient care units, where clinical decisions are often made. References that provide information regarding the specifics on how to dose and monitor the new regimen are ideal. The use of technology, especially computerized physician order entry prescribing algorithms can be a key component of these education and communication plans. As clinicians utilize different methods to update themselves on current health system issues, the communication and education strategies need to be multidimensional and utilize different podiums, which may include e-mails, staff meetings, bulletin boards, Web sites, dashboards, and face-to-face in-services. Education and communication are crucial steps in preventing drug shortages from inducing medication safety events that can lead to direct patient harm. 28
Conclusions
Drug shortages will continue to be a significant challenge for the US health care system. The causes of these issues demonstrate that the medication manufacturing and distribution system is at times convoluted and prone to disruption. Thus, health care providers need to understand the best practices surrounding this issue to optimize patient care. Proactive planning, which includes a multidisciplinary approach, is a key component of this issue and will help prevent medication safety issues when a drug shortage occurs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.