
Abstract
Introduction
Acute myeloid leukemia (AML) is the most common form of acute leukemia among adults and accounts for the largest number of annual deaths from leukemia in the United States. It is characterized by a clonal expansion of myeloid blasts in the peripheral blood, bone marrow, and/or other tissues. The age-adjusted incidence rate of AML is 3.7 cases per 100,000 men and women per year, and the median age of diagnosis is 66 years. 1
The treatment of AML in adults is divided into induction and postremission (consolidation) chemothe-rapy. Without postremission therapy, patients will usually relapse within 6 to 9 months. 2 Management of adult AML is initially based on age, younger (<60 years of age) and older (≥60 years of age). 2 In patients older than 60 years of age, there is a higher prevalence of unfavorable cytogenetics, antecedent myelodysplasia, and multidrug resistance and an increased frequency of comorbid medical conditions, all of which limit the patient’s ability to tolerate intensive chemotherapy. 3
The goal of induction chemotherapy is to produce a major reduction in the leukemic burden and to restore normal hematopoiesis. 2 Although it is not fully understood if delaying treatment may affect patient outcomes, retrospective data suggest that treatment outcomes might be adversely affected when time from diagnosis to start of treatment increases beyond 5 days. 4 The induction regimens for younger patients are based off a backbone of cytarabine and an anthracycline. Daunorubicin has historically been the most commonly used anthracycline. Recently, idarubicin has shown comparable remission rates. In a study that compared idarubicin 12 mg/m2 for 3 to 4 days versus daunorubicin 80 mg/m2 for 3 days in patients 50 to 70 years old, overall survival rates were similar, with complete remission (CR) rates of 83% and 70% (P = 0.024), respectively. 5 Cytogenetics also plays a large role in the efficacy of the induction regimen. In a study with high-dose cytarabine and daunorubicin, CR rates ranged from 62% for poor-risk to 87% for favorable-risk groups. 6 However, because of longer turnaround times, they do not play a significant role in treatment selection for induction therapy.
Cytarabine
Cytarabine is a pyrimidine analog that is commonly used in leukemia and lymphoma regimens. Its primary mechanism of action is inhibiting DNA polymerase, resulting in decreased DNA synthesis and repair. The common adverse reactions of cytarabine are myelosuppression, nausea, diarrhea, rash, fever, and hepatotoxicity. Some adverse reactions of high-dose cytarabine include CNS toxicities, pulmonary edema, conjunctivitis, and cardiomyopathy. Cytarabine has been shown to be teratogenic in animals. It readily passes through the blood-brain barrier, and although no measurements have been performed in human placentas, it would also be expected to penetrate the blood-placental barrier. 7
Daunorubicin
Daunorubicin is an anthracycline that has been well studied in combination with cytarabine for AML treatment. It has a category 1 recommendation from the National Comprehensive Cancer Network (NCCN) guidelines in combination with cytarabine for first-line treatment of AML in adult patients younger than 60 years. The cytotoxic effects of daunorubicin are related to nucleotide base intercalation. Intercalation inhibits nucleotide replication and action of DNA and RNA polymerases. Daunorubicin also inhibits the topoisomerase II enzyme, forming DNA-cleavable complexes. Additionally, daunorubicin enhances the catalysis of oxidation-reduction reactions, promoting the generation of oxygen free radicals. Major adverse effects of daunorubicin include cardiotoxicity and myelosuppression. Studies in mice have shown that daunorubicin is teratogenic in mice, but to a lesser extent than doxorubicin. 8
Idarubicin
Idarubicin is an anthracycline that is also well studied in the treatment of AML. Like daunorubicin, it is also a category 1 recommendation for primary treatment of AML in adult patients younger than 60 years, when used in combination with cytarabine. 2 Idarubicin is more lipophilic compared with the other anthracyclines, which may theoretically increase the concentration crossing the placenta. 9 A summary of alternative chemotherapeutic agents that are used in the treatment of AML are listed on Table 1.
Chemotherapeutic Agents Used in the Treatment of AML.
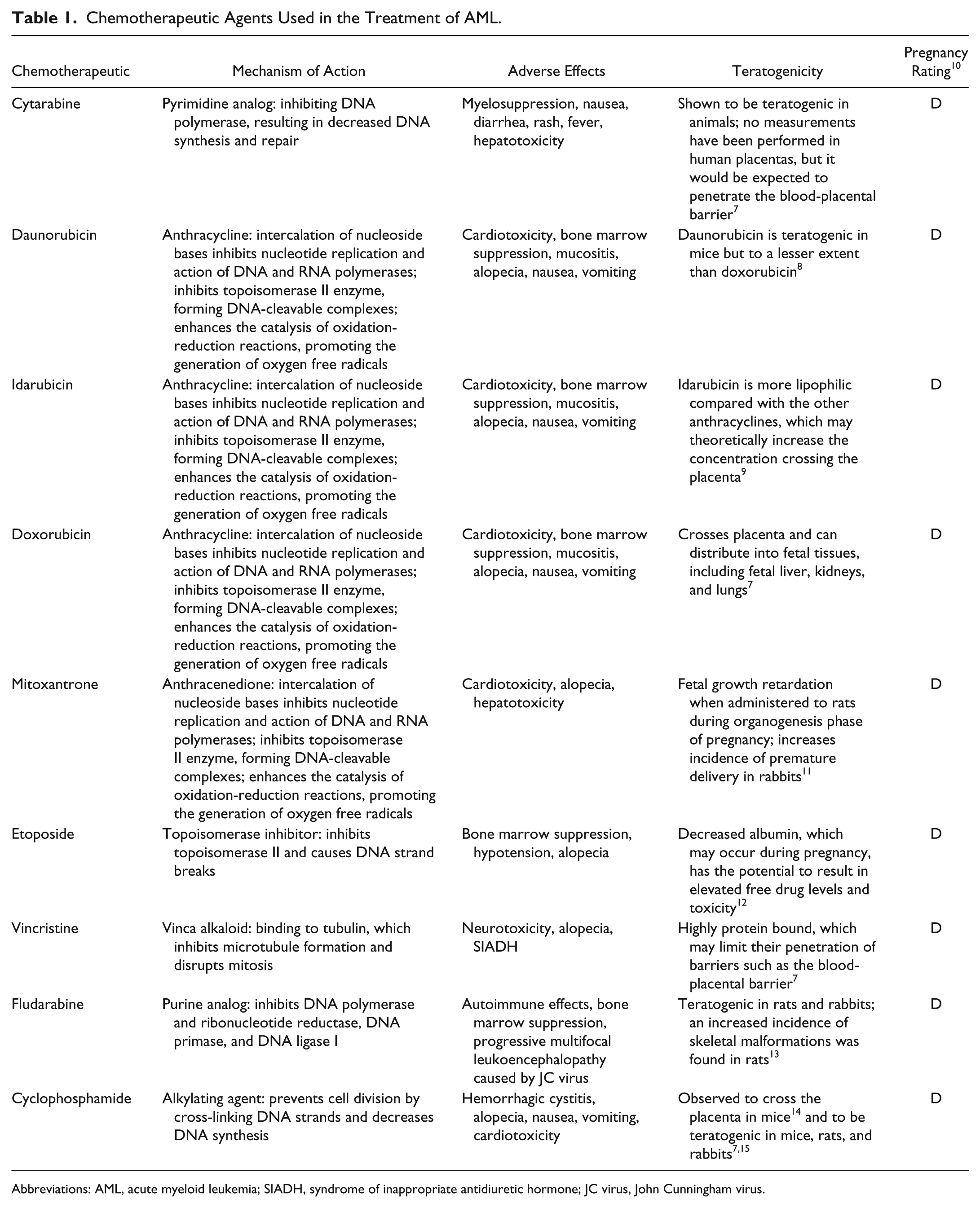
Abbreviations: AML, acute myeloid leukemia; SIADH, syndrome of inappropriate antidiuretic hormone; JC virus, John Cunningham virus.
The incidence of leukemia during pregnancy has been estimated to range from 1 case in 75,000 to 1 case in 100,000.16,17 Although the exact incidence of AML during pregnancy has not been reported, there have been many case reports in the literature that can be used to assess outcomes.
Acute leukemia during pregnancy can present a rare and challenging situation not only for health care providers but also for the mother. Although chemotherapy is widely considered teratogenic, some agents have been shown to be administered safely during pregnancy in other diseases and malignancies. 18 If the leukemia is left untreated, the patient will have a short life span, have a higher probability of spontaneous abortion or fetal death, and have a lower probability of a healthy neonate. 19 Therefore, we sought to systematically review the literature for published articles assessing the outcomes of the neonate and mother in the treatment of AML during pregnancy
Methods
We followed the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guidelines 20 for this systematic review. The objective of the review was to identify all reports published in PubMed between January 1969 and June 2014, which assessed fetal and maternal outcomes from the treatment of AML during pregnancy. The year 1969 was chosen because it was the year that cytarabine was approved by the FDA. The following PubMed search strategy was used: (Leukemia, Myeloid, Acute [Mesh]) AND (Pregnancy [Mesh]) AND (1969/01/01:2014/06/30 [dp]). Additionally, bibliographies of reports found during the search were assessed to find all available reports. After identifying all chemotherapy agents used for AML treatment during pregnancy, another search of PubMed between January 1969 and June 2014 was performed to identify reports of these agents discussing fetal and maternal outcomes in other malignancies. The following PubMed search strategy was used: (Daunorubicin [Mesh]) OR Cytarabine [Mesh]) OR (Doxorubicin [Mesh]) OR (Daunorubicin [Mesh]) OR (Idarubicin [Mesh]) OR (Mitoxantrone [Mesh]) OR (Etoposide [Mesh]) OR (Vincristine [Mesh]) OR (Fludarabine [Mesh]) OR (Cyclophosphamide [Mesh])) AND (Pregnancy [Mesh]) AND (1969/01/01:2014/06/30 [dp]).
Reports were considered eligible for inclusion in this review according to the following criteria: report published in English; report with regimens that contained chemotherapeutic agents considered active and recommended by the NCCN guidelines; and only cases in which chemotherapy was given during pregnancy. Reports that did not contain current chemotherapy regimens were excluded to allow better context of fetal outcomes among current regimens. Reports were excluded in which the mother completed chemotherapy before conception or received chemotherapy after birth or therapeutic abortion because of the inability to assess the direct effect of chemotherapy on a developing fetus.
The reports were reviewed independently by 2 investigators. The data collected and analyzed included the age of the mother at diagnosis of AML, the gestational week at diagnosis, chemotherapy regimen received, survival outcomes of mother, and survival and developmental outcomes for the fetus.
Results
In total, 421 articles were identified through the PubMed search and 31 articles through bibliography and citations of previously published articles. After excluding duplicate articles, articles that were not in the English language, and articles that did not meet inclusion or exclusion criteria based on their title and abstract, 115 articles were assessed for eligibility by full text. It was found that 29 articles did not include cases of AML, 9 articles did not treat with chemotherapy during pregnancy, 7 used nonstandard regimens, and 28 did not mention any cases. After excluding those articles, 42 articles were included in our analysis (Figure 1).
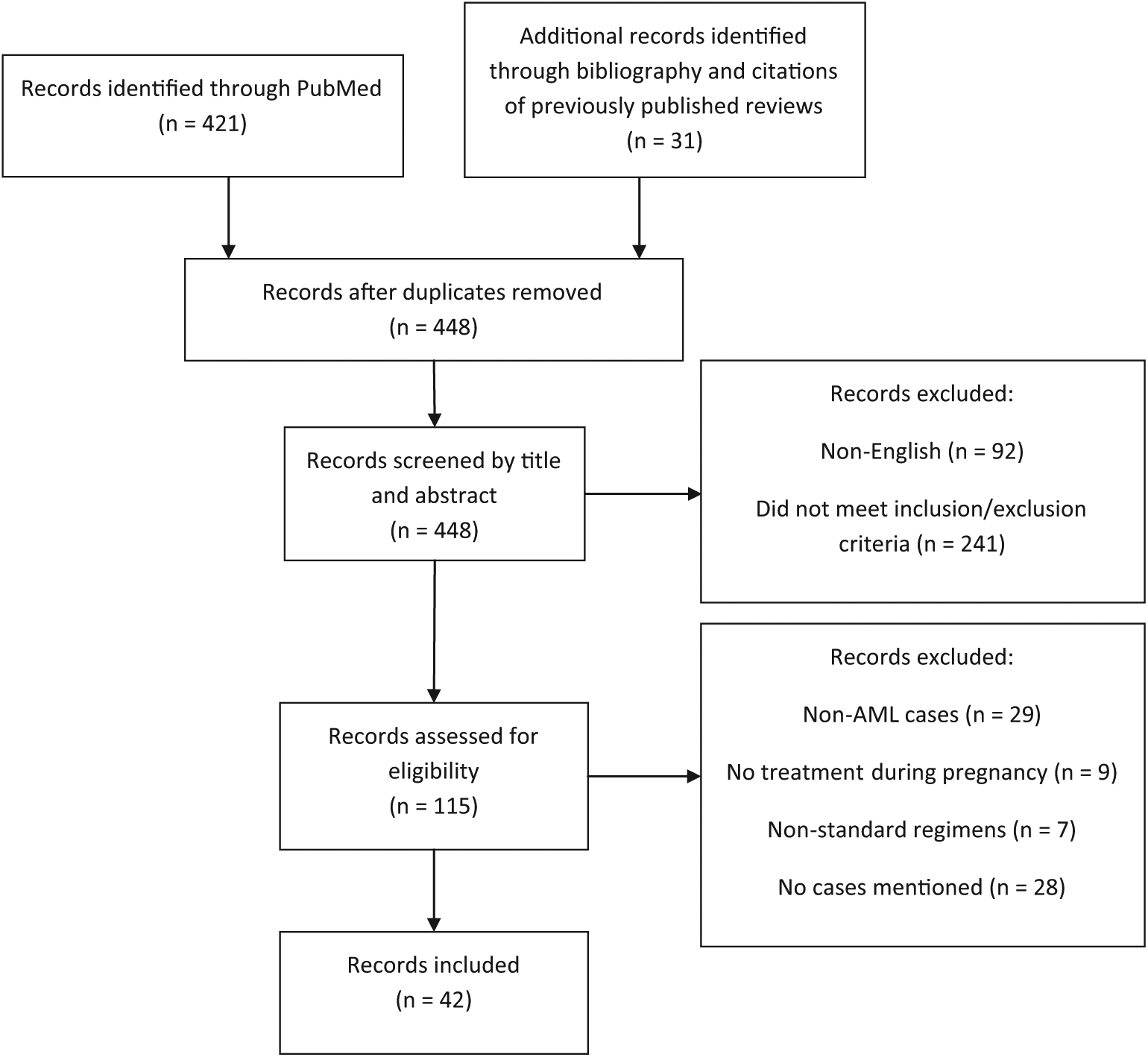
Flowchart of the systematic review process of identifying articles for the review.
A total of 85 cases of fetal exposures to chemotherapy from 83 mothers were included in our literature review, with a median age of 28 years (range = 16-45 years; ages of 11 mothers were not reported). Of these, 8 mothers (9.6%) presented in the first trimester, 61 (73.5%) mothers in the second trimester, and 14 (16.9%) in the third trimester. The regimen, gestational age when treated, mother’s outcome, and infant’s outcome are presented in Table 2. The outcomes of the mothers are presented out of a total of 83, and the outcomes of the fetuses are presented out of a total of 85.
Published Cases of AML Treated During Pregnancy, Divided by Regimen

Cytarabine
All 83 mothers received cytarabine as a component of their induction regimen during pregnancy. Because of 2 sets of twins, there were a total of 85 infants exposed to cytarabine in utero. Among the pregnancies, 9 resulted in spontaneous abortions or fetal death,23,24,27,29,39,21,51,55 of which 3 cases started induction chemotherapy during the first trimester, whereas the other 6 cases initiated chemotherapy in the second trimester.
First trimester: In all, 8 mothers received induction chemotherapy in the first trimester and 6 were reported to have CR, with 2 subsequent relapses (2 unreported). There were 5 babies born and 3 cases of fetal death.
Second trimester: In all, 61 mothers initiated chemotherapy in the second trimester; 43 achieved CR, with 9 relapses; 2 achieved partial remission (PR); 3 mothers died from disease progression; and 5 mothers died from treatment-related complications or infections (8 unreported). A total of 56 live births (including a pair of twins in case 19 36 ) and 6 fetal deaths were reported.
Third trimester: In all, 14 mothers began treatment in the third trimester, and 7 achieved CR, with no relapses. Three mothers achieved PR; 1 mother was refractory to treatment and died from disease progression. Also, 3 mothers’ statuses were not reported. All 15 babies born were alive, including a pair of twins in case 29. 27
The most common side effect that the newborns experienced was anemia. Other adverse effects to the newborn included myelosuppression, hepatopathy, elevated CK, seizures, acrocyanosis, hyaline membrane disease, moderate meningeal hemorrhage, respiratory distress symptoms, and infections. Two cases (case 17 and 19) have reported chromosomal abnormalities: Down’s syndrome 25 and inversion on chromosome 9. 36 Growth defects were observed in 4 infants. Case 51 had shallow sacral dimples, short digits and limbs, and a prominent frontal skull with mild macrognathia. 45 The infant in case 39 had 6 toes on the right foot, but this was associated with the family history of polydactyly. 39 Case 37 developed with hypospadia; he also had respiratory distress syndrome and was intubated at birth. 26 The last infant (case 20) suffered from a congenital adherence of the iris to the posterior cornea in the left eye. 37 It is difficult to ascertain whether these defects were directly caused by cytarabine because in all these cases, cytarabine was used in combination with other agents.
Case 2 was the only case of sole cytarabine exposure during pregnancy. 22 In this case, the child had normal development at the 1-year follow-up, and the mother had a CR and was alive at follow-up 4 months after delivery.
The dose of cytarabine can vary dramatically depending on regimen. Some regimens use high-dose cytarabine, whereas others may use the traditional dosing of cytarabine. With high-dose cytarabine, high concentrations can be achieved in spinal fluid to treat central nervous system leukemia. 63 Although there are no studies, it is thought that concentrations reaching the fetus may be dose dependent. 7 There were 6 cases where the use of high-dose cytarabine was reported. In these cases, the 2 births in cases 75 and 82 were uncomplicated, and there were no abnormalities in the infant.56,62 The fetus in case 4 was spontaneously aborted after chemotherapy was started in the first trimester. 24 Another infant (case 51) was born with shallow sacral dimples, short digits and limbs, and a prominent frontal skull with mild macrognathia. 45 Two other infants in cases 16 and 33 were born with hematological deficiencies.34,38
Daunorubicin
There were 48 cases of daunorubicin use in pregnancy to treat AML, and 5 cases resulted in fetal death. Of these, 2 cases of fetal death occurred when chemotherapy began in the first trimester, whereas in the other 3 cases, it was started in the second trimester.
First trimester: A total of 4 mothers were exposed to daunorubicin in the first trimester of pregnancy. There was 1 CR and 3 unreported disease results among the mothers. Two live births and 2 fetal deaths were reported.
Second trimester: A total of 38 mothers began induction therapy with daunorubicin in the second trimester. Among them, 27 mothers achieved CR, 1 achieved PR, 3 died from disease progression, 3 died from infections, and 4 mothers’ disease statuses were not reported. There were 36 live births, including a pair of twins, and 3 fetal deaths.
Third trimester: There were 6 mothers who began treatment with daunorubicin in the third trimester. Among them, 4 achieved CR, 1 died as a result of disease progression, and the results for 1 were not reported. All mothers delivered live babies.
Some reported adverse effects in the infants included anemia, myelosuppression, pancytopenia, hepatopathy, elevated CK, seizures, respiratory tract infections, and respiratory distress syndrome. The child in case 17 was reported to have Down’s syndrome 25 and another child (case 19) had an inverted chromosome 9. 36 Two patients with congenital malformations were reported in cases 20 and 37. These malformations included congenital adherence of the iris to the posterior cornea in the left eye 37 and hypospadia. 26
Idarubicin
In all, 8 cases of idarubicin were used to treat AML during pregnancy. Of the 7 mothers who started idarubicin in the second trimester, 6 mothers achieved CR, and 1 mother died from cytomegalovirus (CMV) pneumonia after delivery. 56 There were 6 live births reported, with 1 fetal death. 29 One case of idarubicin use was reported in the third trimester. 47 The mother had received 1 cycle of idarubicin and cytarabine (7 + 3) before cesarean section was performed. The baby was born alive. The mother continued induction therapy after birth, but her outcome was not reported. No cases were reported of idarubicin use in the first trimester.
Some of the reported adverse effects were myelosuppression, hepatopathy, elevated CK, acrocyanosis, and hyperbilirubinemia. Two infants had limb defects. The infant in case 51 had shallow sacral dimples, short digits and limbs, and a prominent frontal skull with mild macrognathia. 45
Doxorubicin
In all, 19 pregnant patients were exposed to doxorubicin as part of their chemotherapy regimen. In all but 2 cases, the infant survived.
First trimester: In all, 5 mothers began treatment in the first trimester, and they all achieved CR, with 1 relapse. All 5 babies born to these mothers were alive.
Second trimester: A total of 11 mothers began treatment in the second trimester; 7 mothers achieved CR, with 1 relapse; 1 mother achieved PR; 1 mother died from infection during chemotherapy; and 2 mothers’ conditions were not reported. There were a total of 9 live births and 2 fetal deaths. Case 65 resulted in a stillborn fetus with bruising and petechia over multiple areas. 51
Third trimester: There were 3 mothers who were treated with doxorubicin during their third trimester. One mother achieved CR, and the other 2 mothers achieved PR. All babies were born alive.
There were no growth defects in any of the babies exposed to doxorubicin. The only adverse effects reported at birth were hyaline membrane disease and moderate meningeal hemorrhage in case 64 52 and a left shift in blood count in case 68. 53 Both infants developed normally in subsequent follow-up.
Mitoxantrone
Mitoxantrone was used in 5 cases to treat AML during pregnancy. In the second trimester, 3 cases resulted in CR. The mothers gave birth to 1 live baby, with 2 fetal deaths. Another mother died of CMV pneumonia after a successful delivery. In the third trimester, 1 mother achieved CR and had a live birth. There were no cases of mitoxantrone use in the first trimester.
One infant in case 39 was born with 6 toes on the right foot, but this was attributed to the family’s history of polydactyly. 39 Another infant in case 16 was born with pancytopenia. 34 In the other cases with mitoxantrone in the regimen, no adverse effects were reported.
Etoposide
Etoposide has been used in 2 regimens for AML during pregnancy. Both cases were administered during the second trimester. Both mothers achieved CR and gave birth to live infants. In both cases 16 and 33, the infants were born with hematological abnormalities. One infant was born pancytopenic, 34 and the other was born anemic with profound neutropenia. 38
Vincristine
Vincristine has been used in combination regimens in 15 cases of AML during pregnancy. Of these, 13 cases resulted in live births, with 2 fetal deaths. One fetal death was when chemotherapy was initiated in the first trimester, and the other fetal death was from the second trimester.
First trimester: In all, 5 mothers were exposed to vincristine in the first trimester; there were 2 CRs reported and 3 unreported outcomes for mothers. Also, 4 live births and 1 fetal death were reported.
Second trimester: In the second trimester, 5 cases of vincristine use were reported. Of these, 3 cases resulted in CR, with all babies being born live. Two mothers died from treatment-related mortality, with 1 live birth and 1 death.
Third trimester: There were 5 cases of vincristine initiation during the third trimester; 3 patients achieved CR, and 2 achieved PR. All 6 babies were born alive. Some adverse events reported from infants born after exposure to vincristine included hyaline membrane disease with moderate meningeal hemorrhage, 52 left shift in leukocytes, 53 and anemia with mild infections. 42
Fludarabine
Fludarabine was used in case 75. It was used in the second trimester in combination with the cytarabine, idarubicin, and gemtuzumab-ozogamicin as part of the Go-Flag-Ida induction therapy. The mother died 8 months after delivery from CMV pneumonia. The infant had no abnormalities. 56
Cyclophosphamide
Cyclophosphamide was used in one case of AML during pregnancy. The mother began induction therapy with doxorubicin and cytarabine and received maintenance therapy with cyclophosphamide, cytarabine, and vincristine. The chemotherapy began during the second trimester. The mother achieved CR and delivered a healthy baby. 37
Discussion
Treatment of AML during pregnancy is a therapeutic dilemma. Any delays in therapy may harm the mother, but treatment with chemotherapy is not without considerable risk to the developing fetus. Although our study did not look at whether delays in chemotherapy initiation affected outcomes, previous studies have investigated the effect of time to diagnosis to chemotherapy initiation. Two studies in the United States 4 and Denmark 64 have found that delays in treatment past 5 to 10 days negatively affect the prognosis in younger AML patients. One study from France has found that waiting a short period of time to characterize leukemias does not harm the overall survival or response rate in the patient. 65 The first trimester is when fetal development is most active, so the infant is most sensitive to the effects of chemotherapy during this time. In the 8 reported pregnancies with chemotherapy for AML during the first trimester, 3 (37.5%) resulted in fetal death. In contrast, the outcomes for babies in the second and third trimester seem relatively favorable. Of the 62 exposures to chemotherapy in the second trimester, 6 (9.7%) cases resulted in fetal death. All 15 infants who were exposed to chemotherapy in the third trimester were born alive. This is further evidence that medication exposures during the first trimester incur more risk.66,67
Infants who are born small for gestational age or prematurely have an increased risk for perinatal morbidity and mortality. 68 In a recent analysis of pregnancies complicated by cancer, it was found that small-for-gestational-age infants were more common in hematological malignancies. 69 However, it is not known whether this is a result of the disease or the treatment. In AML, the combination of cytarabine with daunorubicin or idarubicin are both preferred as first-line induction therapy based on NCCN guidelines. 2 We noted more cases with daunorubicin use (47) over idarubicin use (8). Daunorubicin was associated with only 3 incidences of fetal death out of 47 pregnancies (6.4%), compared with idarubicin, where there was 1 death in 8 cases (12.5%). Daunorubicin was also associated with a relatively lower incidence of reported birth defects (4 cases; 8.5%) compared with idarubicin (2 cases, 28.6%). Doxorubicin is another anthracycline with activity in AML. However, it is not currently a recommended treatment. A CALGB study comparing daunorubicin with doxorubicin in AML found that daunorubicin was at least equally effective, with less toxicity. 70 One retrospective study comparing various breast cancer chemotherapy conventional and dose-dense regimens found that the overall incidence of birth defects was not higher than the overall prevalence in the noncancer population in the United States. The majority of those regimens contained doxorubicin. 18 A review by Azim et al 71 recommended using doxorubicin instead of daunorubicin or idarubicin because it has been extensively studied in gestational breast cancer. In the 19 published cases with doxorubicin, there were 2 cases (10.5%) of fetal death51,55 and 1 case (5.3%) where the baby was born with hyaline membrane disease and moderate meningeal hemorrhage. 52
For younger patients, the CR rates are 60% to 80%. In our cases, we found that the overall CR rate from induction chemotherapy in evaluable patients was 80% (100% in the first trimester, 81% in the second, and 67% in the third). This suggests that mothers receiving induction therapy during pregnancy have rates of CR comparable to that in nonpregnant patients. Delays in treatment may occur when the risk to the fetus is balanced with benefit to the mother in regard to treatment. However, it has been found that postponing chemotherapy until after delivery decreased survival for the mother compared with those who initiated chemotherapy during pregnancy. 72
Some of the chemotherapies for AML have also been used in other diseases during pregnancy. High-dose cytarabine has also been used successfully in the CODOX-M/IVAC (cyclophosphamide, vincristine, doxorubicin, methotrexate, ifosfamide, mesna, etoposide, cytarabine) regimen in the treatment of Burkitt’s lymphoma starting at 26 weeks’ gestation. 73 The cyanotic infant was delivered via cesarean section at 32 weeks’ gestation. Other than respiratory distress, the physical examination of the infant revealed no anomalies. The child’s hearing screening test and brain ultrasound were normal. At 9 months, the child showed delayed motor skills but was considered healthy. The mother had no evidence of disease 14 months after childbirth.
Daunorubicin use during pregnancy has also been reported during acute promyelocytic leukemia (APL). 74 Three cases in the first trimester resulted in live births, with 1 baby having congenital defects and respiratory distress. One case in the first trimester resulted in spontaneous abortion. In the second trimester, 9 cases resulted in live births. One of the cases in the second trimester resulted in spontaneous abortion, and another baby died 1 day after birth from pulmonary hemorrhage. Some adverse effects reported in the survivors included moderate hyperbilirubinemia and hemorrhage, bone marrow aplasia, and seizures. Two cases are reported in the third trimester. One infant was born healthy, and the other died 4 days after chemotherapy was started.
Idarubicin use has been reported in a case of rhabdomyosarcoma during pregnancy. The patient began treatment during the second trimester with the O-TIE regimen, which included oral low-dose chemotherapy containing trofosfamide (a non-FDA approved alkylating agent), idarubicin, and etoposide. A healthy infant was born 5 days after the last course of chemotherapy, and the infant showed no evidence of any malformations. The baby exhibited normal neurological development during follow-up over 2 years. 75 Idarubicin has also been used in combination with arsenic trioxide for the treatment of APL in pregnant mothers. In one case, the chemotherapy was started during the second trimester. The APL reached remission, and the child was born premature and required a 2-month stay in the hospital but developed to have good general health and neurological conditions. 76 In another APL case treated with idarubicin and arsenic trioxide, the mother was treated during the second trimester. After reaching remission, the child was born with a small patent ductus arteriosus. The ductus arteriosus spontaneously closed a week later, and the infant was found to have no clinical signs of congestive heart failure. 77
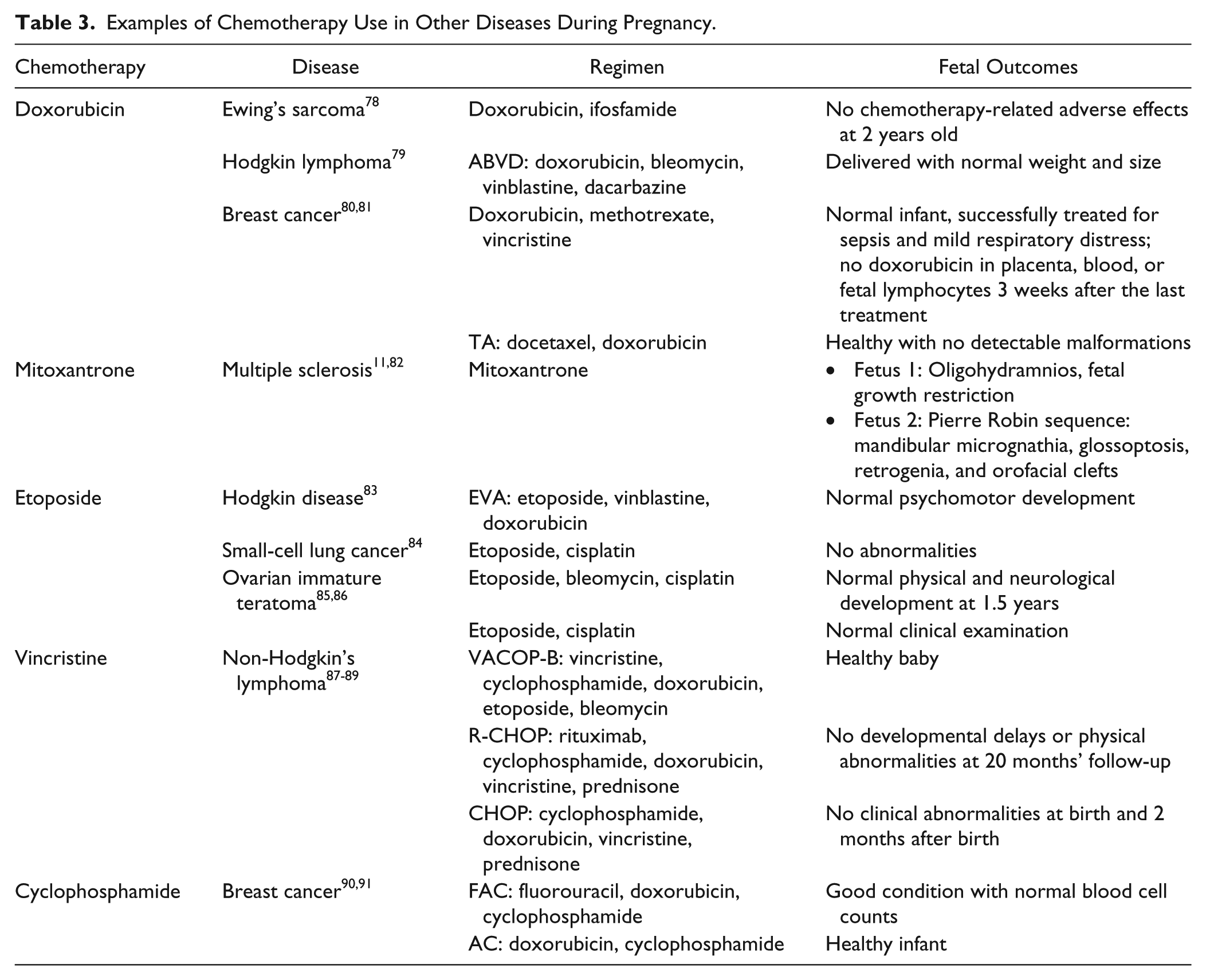
The other chemotherapy agents (doxorubicin, mitoxantrone, etoposide, vincristine, cyclophosphamide) have also been used successfully in other diseases during pregnancy, and these are summarized in Table 3.
Examples of Chemotherapy Use in Other Diseases During Pregnancy.
One limitation of this study is that there are no controlled trials assessing treatments of AML during pregnancy. The only sources of data in this study are published case reports and case series. One limitation of case reports is publication bias because negative data would be less likely to be published. This could potentially skew the incidences of fetal defects or deaths. Another limitation is that the search would only result in AML studies that specifically included pregnant patients. It would lack AML studies that included pregnant patients but without specific mention of pregnancy. One valuable piece that was missing is that only a few case reports had long-term follow-up with the children. While many infants may be healthy at initial examination, the adverse effects from chemotherapy exposure may not appear until many years after birth. The outcomes of the patient and the fetus must be considered carefully when selecting the chemotherapy regimen used to treat the leukemia. Furthermore, most of the patients received combination chemotherapy, so it is difficult to distinguish which agent may be the cause for certain birth defects or adverse effects in the infant. Additionally, many of the articles did not report the chemotherapy doses, making it difficult to assess outcomes from chemotherapies with a wide range of doses (eg, cytarabine). Some of the combination chemotherapy regimens reported in the older case reports included chemotherapeutic agents that are no longer recommended in the treatment of AML, such as 6-mercaptopurine and 6-thioguanine.
Conclusion
The diagnosis of AML as such can be challenging for many patients; however, diagnosis during pregnancy can be even more challenging for patients and health care providers. The literature on this topic is sparse, consisting only of case reports. Although it is difficult to draw strong conclusions from these reports, it was noted that treatment during the second and third trimester resulted in fewer fetal complications than the first trimester. It was also found that induction during pregnancy resulted in CR rates comparable to that in nonpregnant patients. The choice of anthracycline is still unclear, but the decision should be made with careful consideration, weighing the outcomes of the mother and the fetus.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Authors’ Note
Article’s significance: this article reviews the published literature dealing with the treatment of acute myeloid leukemia during pregnancy and reports the outcomes for the mother and fetus.