
Abstract
Keywords
Background
The prevalence of atrial fibrillation (AF) rises as the population ages.1,2 AF is associated with an increased risk of ischemic stroke and increased morbidity and mortality.1,3 Patients with nonvalvular atrial fibrillation (NVAF) are 3 to 7 times more likely than those without AF to have an ischemic stroke.4,5 Currently approved oral anticoagulants to reduce the risk of stroke in patients with NVAF include vitamin K antagonists, direct thrombin inhibitors, and factor Xa inhibitors. 6 Warfarin poses several barriers including risk of bleeding, drug-drug interactions, drug-food interactions, and frequent international normalized ratio (INR) monitoring and dose adjustments.7,8 The target-specific oral anticoagulants (TSOACs) may offer a more manageable option for patients who are unable to maintain a stable INR. Because of the shorter half-life and lack of reliable monitoring to ensure compliance, warfarin may still be preferred in patients with adherence limitations. Dabigatran compared with warfarin was associated with a statistically significant reduction in nonfatal stroke and no difference in the risk of nonfatal major extracranial bleeding, but with an increased rate of gastrointestinal (GI) bleeding. 9 Rivaroxaban was noninferior to warfarin in reducing stroke and systemic embolism. Rivaroxaban was also associated with increased GI bleeding but no difference in the rates of major bleeding or mortality. 10 Apixaban reduced the risk of stroke or systemic embolism and reduced the rate of major bleeding compared with warfarin but showed no difference in regard to major GI bleeding. 11 All 3 agents demonstrated a statistically significant lower rate of intracranial hemorrhage.9-11 Guidelines for treating AF recommend oral anticoagulation for patients with a prior stroke, transient ischemic attack, or an increased ischemic stroke risk determined by the CHA2DS2-VASc score.12,13
In patients diagnosed with acute deep-vein thrombosis (DVT) or pulmonary embolism (PE), guidelines recommend initiation of warfarin and overlapping parenteral therapy for a minimum of 5 days or until the INR is 2 for at least 24 hours. Duration of warfarin therapy is dependent on the etiology of the DVT or PE and patient’s risk for bleeding. 14 All 3 TSOACs have been demonstrated to be efficacious alternatives to warfarin therapy. It is important to note that dabigatran was studied with the use of initial low-molecular-weight heparin, whereas rivaroxaban and apixaban do not require a parenteral lead-in period.15-18 The Food and Drug Administration (FDA)-approved indications of TSOACs are included in Table 1.19-22
Comparison of TSOACs.
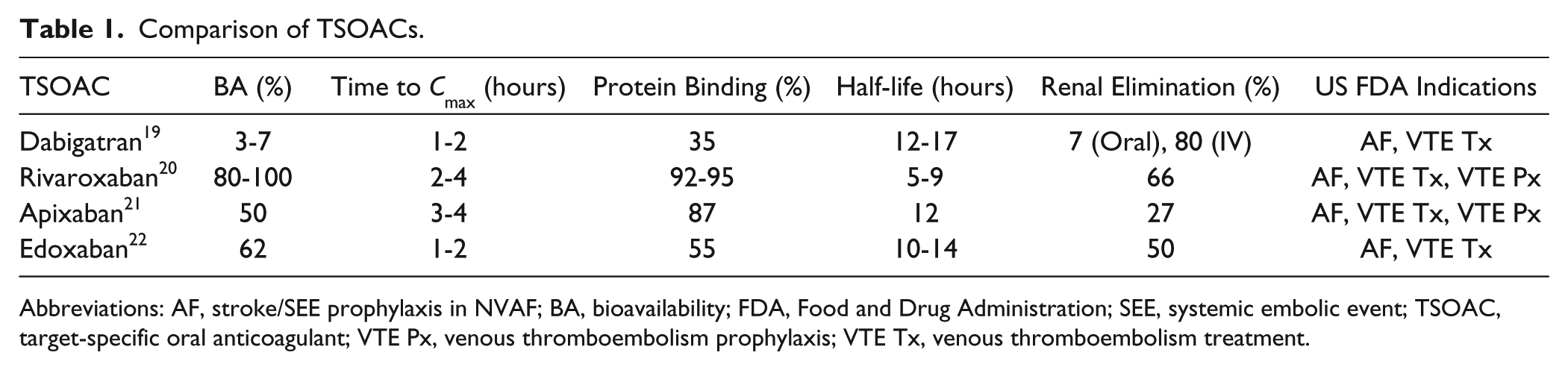
Abbreviations: AF, stroke/SEE prophylaxis in NVAF; BA, bioavailability; FDA, Food and Drug Administration; SEE, systemic embolic event; TSOAC, target-specific oral anticoagulant; VTE Px, venous thromboembolism prophylaxis; VTE Tx, venous thromboembolism treatment.
Edoxaban was approved in January 2015 by the FDA for the prevention of stroke in patients with NVAF and the treatment of DVT and PE after 5 to 10 days of parenteral anticoagulation. Edoxaban is the fourth TSOAC in its class to receive FDA approval. 22 This review examines key clinical trials and potential place in therapy.
Data Sources
A literature review was conducted in February 2015 consisting of a PubMed database and Cochrane Central Register of Controlled trials using search terms edoxaban (ordu-176b), and atrial fibrillation, deep vein thrombosis, pulmonary embolism, or venous thromboembolism. Phase II and phase III clinical trials in humans as well as pharmacokinetic (PK) and pharmacodynamic studies were included. The bibliographies were reviewed for inclusion of other pertinent articles not retrieved by the search. All references included were published between 1998 and 2015.
Pharmacology
Edoxaban, a TSOAC, binds directly to clot-bound factor Xa, leading to the reversible inhibition of platelet activation and fibrin clot formation. Factor Xa catalyzes the conversion of prothrombin to thrombin. Thrombin activates platelets and catalyzes the conversion of fibrinogen to fibrin. 23
Pharmacokinetics/Pharmacodynamics
In healthy patients, edoxaban exhibits predictable linear PK parameters and a predictable degree of anticoagulation in doses up to 120 mg. Peak plasma concentrations of edoxaban occur 1 to 2 hours after oral administration. 24 Edoxaban has an oral bioavailability of 50% to 62%. 25 There are no clinically significant effects of food on the PK of a single 60 mg dose of edoxaban. The apparent volume of distribution of edoxaban is generally greater than 300 L during the terminal phase. Plasma protein binding ranges from 40% to 59% and is relatively constant up to 12 hours. The usual plasma half-life is 8 to 10 hours (range = 5.8-10.7 hours). Edoxaban is not extensively metabolized by CYP3A, resulting in minimal drug interactions. However, it is affected by drugs that inhibit the P-glycoprotein (P-gp) transport protein, which transports edoxaban back into the intestine. Edoxaban is primarily eliminated by the kidneys (35%-50%) but also through metabolic and biliary pathways. 24 A subset of individuals was found to have geometric mean predose edoxaban exposure levels that were about 30% less in the subgroup with normal renal function compared with the subgroup with mild renal impairment. 26 Renal dose adjustments reflect the increased exposure of edoxaban with the degree of renal impairment. The risk of bleeding doubled with edoxaban 60 mg compared with warfarin in a phase II study, with the edoxaban 60 mg dose compared with warfarin in Japanese patients with a total body weight ≤60 kg. 27 The PKs of edoxaban were not significantly affected by factors such as gender, age, or ethnicity, once adjusted for weight and renal function. 26
Clinical Trials
Edoxaban in Atrial Fibrillation
Four randomized, double-blind trials evaluated the use of edoxaban for the prevention of stroke in patients with NVAF. All trials included adults with NVAF and a CHADS2 score of >1 or ≥2. Individuals were excluded for AF resulting from a reversible cause, renal impairment (creatinine clearance [CrCl] <30 mL/min or serum creatinine ≥1.5 mg/dL), high bleeding risk, or indication for dual antiplatelet therapy. Two of the trials were multinational, and 2 were conducted exclusively in Asian countries. Edoxaban doses ranged from 15 mg once daily to 60 mg twice daily and were compared with warfarin (Table 2).27-31 Three trials treated patients for 3 months. The long-term trial, ENGAGE-AF TIMI 48, treated patients for a minimum of 3 months. All 4 trials included a large proportion (62.0%-88.4%) of patients with intermediate risk of stroke, with a CHADS2 of ≤3. Time in therapeutic range (TTR) varied widely between studies (45.1%-83%).27-30 A TTR above 60% is considered adequate when comparing warfarin with alternate agents for stroke prevention in patients with NVAF.32-35
Comparison of Clinical Trials of Edoxaban.
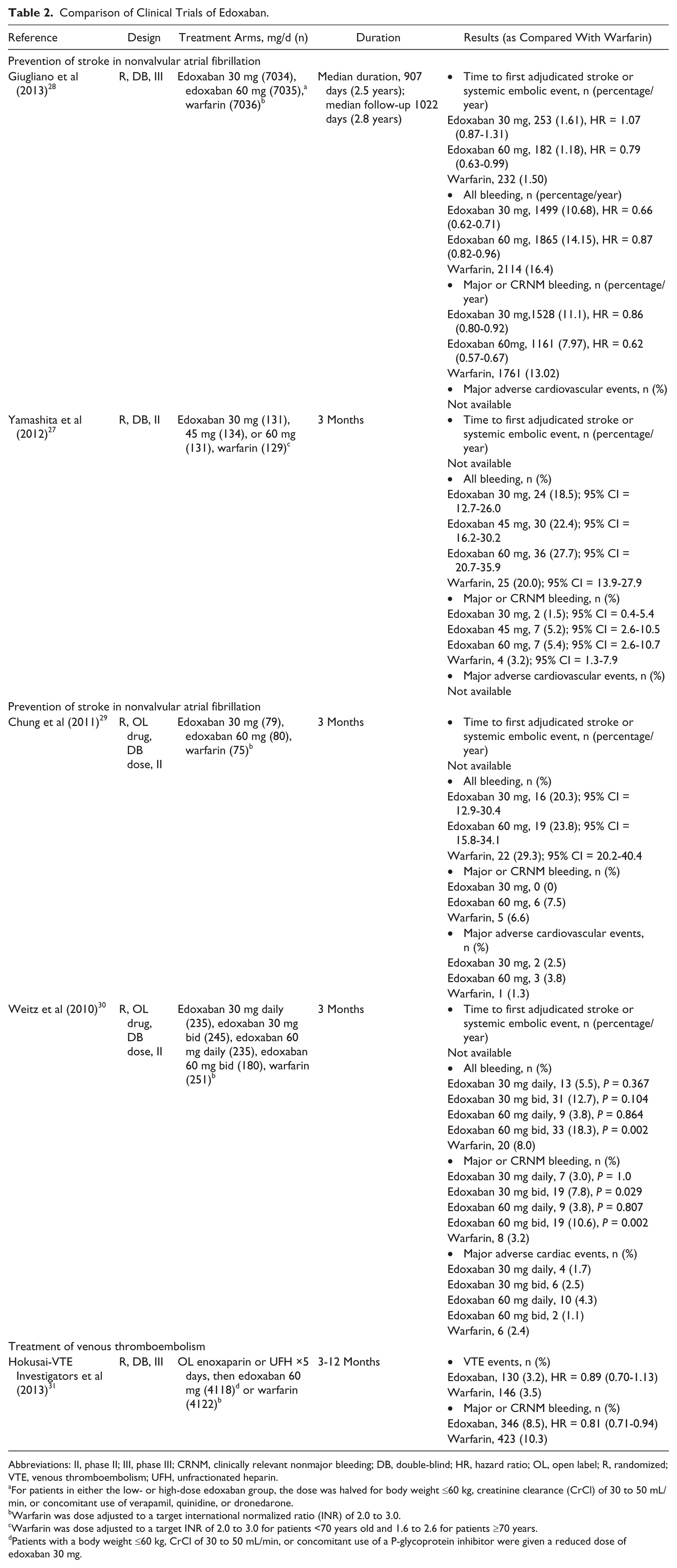
Abbreviations: II, phase II; III, phase III; CRNM, clinically relevant nonmajor bleeding; DB, double-blind; HR, hazard ratio; OL, open label; R, randomized; VTE, venous thromboembolism; UFH, unfractionated heparin.
For patients in either the low- or high-dose edoxaban group, the dose was halved for body weight ≤60 kg, creatinine clearance (CrCl) of 30 to 50 mL/min, or concomitant use of verapamil, quinidine, or dronedarone.
Warfarin was dose adjusted to a target international normalized ratio (INR) of 2.0 to 3.0.
Warfarin was dose adjusted to a target INR of 2.0 to 3.0 for patients <70 years old and 1.6 to 2.6 for patients ≥70 years.
Patients with a body weight ≤60 kg, CrCl of 30 to 50 mL/min, or concomitant use of a P-glycoprotein inhibitor were given a reduced dose of edoxaban 30 mg.
The 3 short-term trials were double-blinded to the dose of edoxaban but open label for randomization to edoxaban or warfarin (Weitz et al, 30 n = 1146; Chung et al, 29 n = 234; Yamashita et al, 27 n = 546). The primary end point was a composite of major, clinically relevant nonmajor (CRNM), and minor bleeding. None of the trials found a statistically significant reduction in all bleeding, major bleeding, CRNM bleeding, or minor bleeding between any dose of edoxaban compared with warfarin or between the various edoxaban doses despite an observed trend in dose-related increased rates of bleeding. Yamashita et al 27 found that the incidence of major and CRNM bleeding was higher in the ≤60 kg subgroup than in the >60 kg subgroup for all doses. The TTR for warfarin was 83% for patients ≥70 years old (INR = 1.6-2.6) and 73% for patients <70 years old (INR = 2.0-3.0). 27 Weitz et al 30 did find a significant increase in the incidence of major plus CRNM bleeding with the edoxaban 30 mg twice daily (7.8% vs 3.2%, P = 0.029) and edoxaban 60 mg twice daily (10.6% vs 3.2%, P = 0.002) regimens compared with warfarin. 30 For those patients receiving warfarin, TTR was 50%. Chung et al 29 saw an increased incidence of all bleeding for patients weighing ≤60 kg versus >60 kg (odds ratio = 2.38; 95% CI = 1.01-5.62; P < 0.001). Interestingly, this study had the lowest TTR, at 45.1%, even with the use of open-label warfarin. 29 The secondary end point of the short-term trials conducted by Weitz et al 30 and Chung et al 29 was a composite of all major adverse cardiovascular events (MACE), including: ischemic or hemorrhagic stroke, systemic embolic event (SEE), myocardial infarction, cardiovascular death, and hospitalization for any cardiac cause. Neither study was adequately powered to detect a difference in MACE between groups and few events were reported.
The ENGAGE-AF TIMI 48 trial was double-blinded with sham INRs generated for 21 105 patients randomized to edoxaban. The primary end point was time to first adjudicated stroke or SEE. Patients were randomized to high-dose edoxaban (60 mg), low-dose edoxaban (30 mg), or warfarin. The dose of edoxaban was halved if any of the following characteristics was present at the time of randomization or during the study: estimated CrCl of 30 to 50 mL/minute, body weight ≤60 kg, or the concomitant use of verapamil, dronedarone or quinidine. Groups had similar baseline characteristics: median age was 72 years, and 77% had a CHADS2 score of 2 or 3. TTR was adequate for those patients receiving warfarin at 68.4%. There was a statistically significant reduction of stroke or SEE in the modified intention-to-treat (ITT) analysis between high-dose edoxaban (60 mg daily; 1.18%) and warfarin (1.50%; hazard ratio [HR] = 0.79; 97.5% CI = 0.63-0.99; P < 0.001 for noninferiority). The low-dose (30 mg) edoxaban group did not demonstrate a statistically significant reduction when compared with warfarin. Neither group showed a significant reduction in stroke or SEE in the prespecified ITT superiority analysis. The primary outcome favored warfarin in a subgroup analysis of patients with normal renal function compared with high-dose (HR = 1.41; 95% CI = 0.97-2.05) and low-dose (HR = 1.61; 95% CI = 1.12-2.32) edoxaban groups. 28 The risk of stroke and SEE was also examined as a function of continuous CrCl levels using a Cox Proportional Hazard Model. The predicted HR comparing edoxaban with warfarin for first stroke or SEE increases as renal function improves. The HR crosses over the HR = 1 line at a CrCl of ~95 mL/min, indicating a benefit with warfarin (HR = 1.02; 0.76-1.38). 26 Major bleeding was statistically reduced in high-dose (2.75% vs 3.43%; HR = 0.80; 95% CI = 0.71-0.91; P < 0.001) and low-dose (1.61% vs 3.43%; HR = 0.47; 95% CI = 0.41 to 0.55; P < 0.001) edoxaban groups compared with warfarin. An additional analysis was conducted on the patient factors requiring dose adjustments in patients receiving high-dose edoxaban. The HR for the primary end point for patients randomized to edoxaban 60 mg who had their dose adjusted for factors such as moderate renal impairment (CrCl = 30-50 mL/min), low body weight (≤60 kg), or a need for concomitant treatment with P-gp inhibitors was similar to that of the individuals who received the full dose—0.81 and 0.78, respectively. There was an increased risk of major GI bleeding in the high-dose group compared with warfarin. 26
Edoxaban in Venous Thromboembolism
The Hokusai VTE Trial, a randomized, double-blind study, evaluated the use of edoxaban in the treatment of symptomatic VTE in 8240 patients. The study included patients with a diagnosis of an acute, symptomatic DVT, a PE, or both. 31 Patients were excluded if they had a contraindication to heparin or warfarin, received therapeutic doses of heparin for more than 48 hours, received more than 1 dose of warfarin, were on aspirin therapy >100 mg or dual antiplatelet therapy, or had a CrCl < 30 mL/min. All patients received open-label enoxaparin or unfractionated heparin (UFH) for at least 5 days and then were randomized to receive edoxaban 60 mg daily or warfarin. The dose of edoxaban was decreased to 30 mg at randomization in patients with a CrCl of 30 to 50 mL/min, body weight ≤60 kg, or concomitant treatment with a potent P-gp inhibitor. Dose adjustments for these factors or a 20% decrease in CrCl from baseline were allowed during the study. Sham INR values were generated for patients randomly assigned to edoxaban. Treatment was continued for at least 3 months. Treating physicians were allowed to extend therapy up to 12 months based on the patient’s risk of recurrent VTE, risk of bleeding, and patient preference. The study attempted to follow all patients for 12 months. For those patients receiving warfarin, TTR was 63.5%. This represents an adequate control of warfarin for the treatment of VTE. 35
The primary end point was the incidence of symptomatic recurrent VTE (composite of DVT or nonfatal or fatal PE). The principal safety end point was a composite of major or CRNM bleeding. Groups had similar baseline characteristics, with 65.7% of patients presenting with a provoked DVT or PE, and 17.6% of patients receiving a reduced dose at randomization. All patients who underwent randomization and received at least 1 dose of the study drug were included in the modified ITT and safety analysis. Edoxaban was noninferior to warfarin in preventing a recurrent VTE (3.2% vs 3.5%; HR = 0.89; 95% CI = 0.70-1.13; P < 0.001). Edoxaban was superior to warfarin in reducing the incidence of major or CRNM bleeding (8.5% vs 10.3%; HR = 0.81; 95% CI = 0.71-0.94; P = 0.004). These results were consistent in the 30 mg edoxaban subgroup analysis. 31
Dosage Recommendations
Edoxaban is available as 15, 30, and 60 mg tablets. The recommended starting dose of edoxaban for treatment of NVAF in patients with a CrCl between 50 and 95 mL/min and for the treatment of DVT and PE is 60 mg daily. Edoxaban should be taken once daily by mouth without regard to meals. A 50% dose reduction is recommended for patients treated for a DVT or PE, with any of the following characteristics: CrCl of 30 to 50 mL/min based on the Cockcroft-Gault formula, body weight ≤60 kg, or concomitant use of a P-gp inhibitor, except amiodarone. A 50% dose reduction in patients treated for NVAF is only warranted for a CrCl of 30 to 50 mL/min. 22
Drug-Drug Interactions
An open-label trial of healthy volunteers evaluated the PK interactions of edoxaban with known P-gp substrates/inhibitors used in the management of AF. Edoxaban exposure, measured as area under the curve, was increased when administered with quinidine (76.7%), verapamil (52.7%), amiodarone (39.8%), and dronedarone (84.5%). Mean concentrations of edoxaban 24 hours postdose were increased by the coadministration of quinidine (11.8%), verapamil (29.1%), and dronedarone (157.6%) and decreased by the coadministration of amiodarone (25.7%). Coadministration of atorvastatin or digoxin had only minor PK effects. 36 The ENGAGE-AF TIMI trial required a dose adjustment with dronedarone, quinidine, and verapamil. No dose adjustment was required with amiodarone, and edoxaban 60 mg had no increased bleeding risk compared with warfarin.26,28 Concomitant use of edoxaban and rifampin should be avoided because of decreased serum concentrations. 22
Contraindications, Precautions, and Monitoring
Edoxaban is contraindicated in patients with active pathological bleeding. Edoxaban has a boxed warning related to reduced efficacy in NVAF patients with CrCl >95 mL/min. An assessment of renal function should be performed prior to initiation. The rate of ischemic stroke was higher in patients when treated with edoxaban compared with warfarin because edoxaban exposure levels are decreased in patients with normal renal function.26,28 A boxed warning also exists related to the premature discontinuation of edoxaban because of increased risk of ischemic events immediately following discontinuation. Caution should be exercised with therapy cessation. There is also a risk of spinal hematoma in patients who are receiving neuraxial anesthesia or undergoing spinal puncture. These 2 warnings are similar to that for other TSOACs. Patients should be monitored for bleeding while taking edoxaban. Because of lack of study data, patients with mechanical heart valves or moderate to severe mitral stenosis should not receive edoxaban. 22 Use of edoxaban should be avoided in patients with moderate or severe hepatic impairment because of intrinsic coagulation abnormalities. 22 Edoxaban prolongs clotting time tests such as prothrombin time (PT), INR, and activated partial thromboplastin time. Changes observed at the expected therapeutic dose are small and subject to a high degree of variability and not useful in monitoring the anticoagulant effect of edoxaban. 22 In the study by Yamashita et al, 27 edoxaban dose dependently prolonged PT-INR at 1 to 3 hours postdose in treatment weeks 4 and 12 (P < 0.001).
Adverse Effects
The most prevalent adverse effect observed was the risk of bleeding, which was comparable to that for warfarin. Incidence of bleeding was significantly higher with twice-daily dosing; however, this is not an approved dosing regimen. 30 Overall, edoxaban was found to be safe, with no significant increases in unexpected toxicities.28,31
Reversal
Hemodialysis does not significantly contribute to edoxaban clearance. Protamine sulfate, vitamin K, and tranexamic acid are not expected to reverse the anticoagulant activity of edoxaban. 22 A phase I study conducted in health volunteers administered 4-factor prothrombin complex concentrate (4F-PCC) at doses of 50 IU/kg (n = 33), 25 IU/kg (n = 28), or 10 IU/kg (n = 30) following administration of a 60 mg dose of edoxaban. Utilizing punch biopsy, 4F-PCC resulted in complete reversal of bleeding duration, whereas other dosing schemes only resulted in partial reversal. A similar trend was noted for blood volume and endogenous thrombin potential; however, a complete reversal was not noted for PT. A dose response was evident, with the higher concentrations of 4F-PCC producing a greater reduction in PT prolongation than the lowest dose. 37
Place in Therapy
Edoxaban joins 3 other TSOACs (dabigatran, rivaroxaban, and apixaban) approved by the FDA for reducing stroke and SEE in patients with NVAF, in addition to treatment of DVT and PE. Efficacy for both approved indications was established by large, randomized controlled trials.9-11,15-18 A potential limitation to consider for patients with NVAF is noninferiority to warfarin in safety and efficacy when previously approved medications such as dabigatran and apixaban were superior to warfarin for the primary efficacy end point.9,11 Patients treated with edoxaban for a VTE must be treated with 5 to 10 days of a parenteral anticoagulant, unlike rivaroxaban and apixaban, which were studied without an initial run-in phase. However, edoxaban is the first TSOAC to be approved for once-a-day dosing without dietary considerations or restrictions. Clinical decisions related to anticoagulation have become increasingly complex. Similar to other novel agents, there is currently no FDA-approved reversal agent available. Although this is the first agent to receive 2 simultaneous approvals from the FDA, it still lacks an indication for thromboprophylaxis for orthopedic surgery patients. For institutions attempting to use a single TSOAC, edoxaban, at this time, would not be a viable option.
Conclusion
Edoxaban is a direct oral factor Xa inhibitor, the newest TSOAC to be approved by the FDA. It has demonstrated efficacy for both approved indications in addition to similar bleeding rates to other available TSOACs. One important contraindication is the use in patients with a CrCl >95 mL/min, for the prevention of stroke in patients with NVAF. Edoxaban appears to be an alternative option for anticoagulation but does not appear to have any clear advantages over other TSOACs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Tellor participated in Pfizer’s Midwest Atrial Fibrillation Advisory Board meeting; Ms Minor has no conflicts of interest; Dr Armbruster has no conflicts of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.