
Abstract
Introduction
Therapeutic anticoagulation is common in patients requiring heart transplant because these patients are on warfarin for indications such as atrial fibrillation, venous thromboembolism (VTE), and the presence of mechanical heart valves or ventricular assist devices (VADs). Prior to heart transplant, anticoagulant reversal is often necessary to avoid significant intraoperative and perioperative bleeding. Reversal is commonly achieved with vitamin K, which competes with warfarin for the vitamin K reductase enzyme, as well as fresh frozen plasma (FFP), which contains clotting factors, including those depleted by warfarin. 1 Limitations, however, exist with both strategies, such as time to international normalized ratio (INR) normalization with vitamin K. In addition, limitations of FFP include time necessary for thawing the product, large volumes necessary for adequate reversal, and the possibility of transfusion-related lung injury. Transfusion of blood products in the transplant population also increases the risk of allosensitization with the introduction of antibodies leading to possible organ rejection. Another option for reversal is prothrombin complex concentrate (PCC), which contains the vitamin K–dependent clotting factors depleted by warfarin (factors II, VII, IX, and X). 2 Heart transplant guidelines include PCC among the modalities for warfarin reversal; however, supportive evidence is minimal. 3
At our institution in the summer of 2013, representatives from the departments of cardiothoracic surgery, hematology, and pharmacy developed a warfarin reversal protocol for patients undergoing heart transplant with a presenting INR of 1.5 or greater with low-dose PCC. The protocol was created in an effort to reduce blood product use and was based on a thorough review of relevant clinical trials using PCC for INR reversal as well as internal expert opinion. Our intent was to produce a protocol that limited PCC doses to minimize exposure and avoid thrombotic events in a potentially high-risk population. The protocol, shown in Figure 1, utilizes both a weight-based and INR-specific dosing scheme and allows a maximum of 3 doses to be administered to patients. This study evaluated the effectiveness and safety of this protocol for warfarin reversal prior to heart transplant using PCC and compared the results related to blood product use, the need for reoperation for bleeding, and adverse events post-implementation with a historical control group prior to implementation. To our knowledge, this is the first study evaluating a warfarin reversal protocol utilizing low-dose PCC with dosing based on weight (units/kg) and baseline INR.
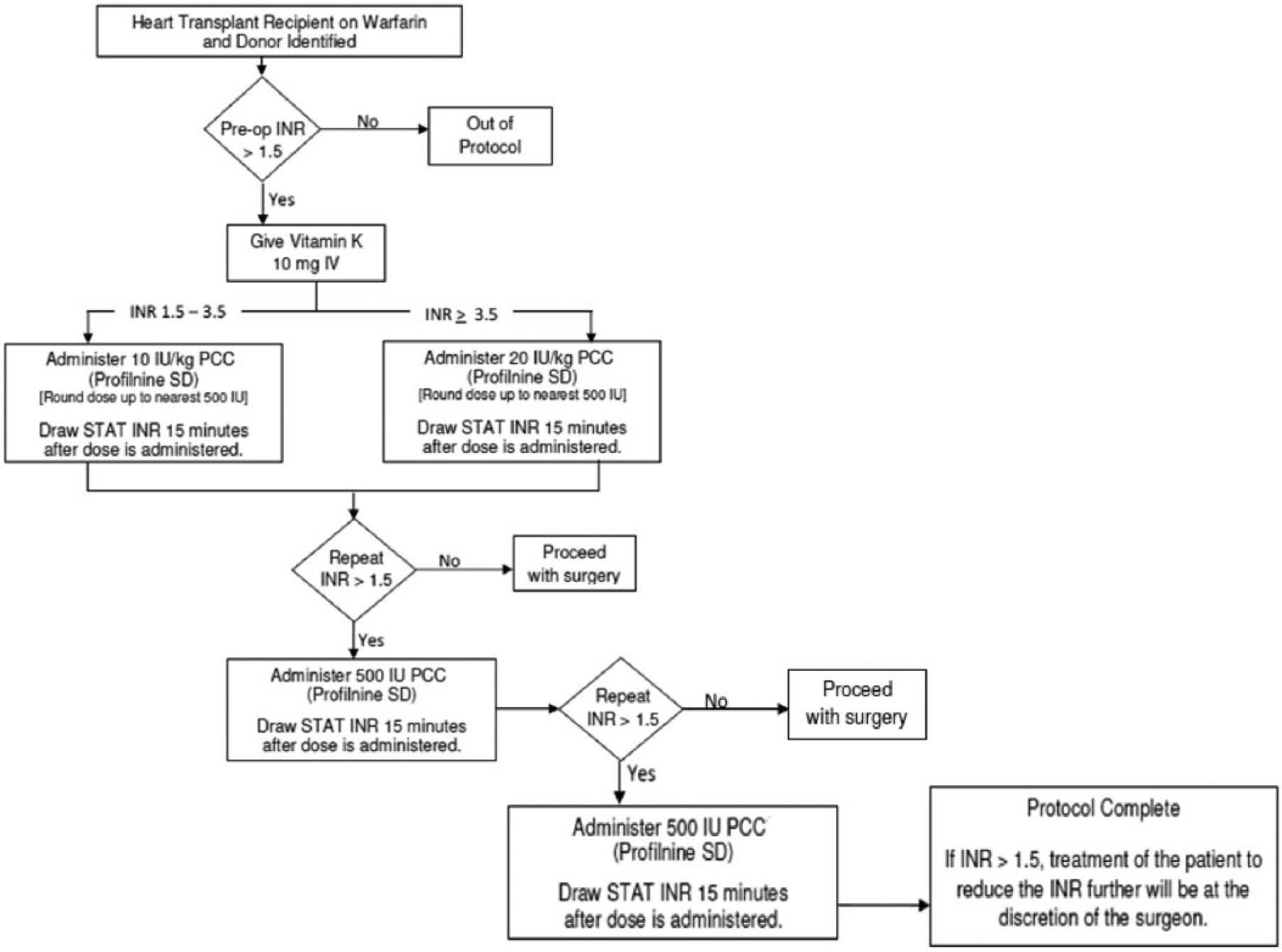
Heart transplant warfarin reversal protocol.
Methods
This was a single-center, non-interventional, retrospective cohort study approved by the institutional review board, which waived the requirement for individual informed consent. All data were gathered from the electronic medical record and collected and managed using REDCap (Research Electronic Data Capture) electronic data capture tools hosted at Cleveland Clinic. 4
Patients were included in the PCC cohort if they underwent heart transplant after June 2013 when the warfarin reversal protocol was implemented, presented for transplant with an INR of ≥1.5, and received at least 1 dose of PCC. To be included in the historical control cohort, patients had to have undergone heart transplant, been on warfarin prior to surgery, and presented with an INR of ≥1.5 and should not have received PCC. Historical control patients were identified from the institution’s heart transplant master list starting immediately prior to the initiation of the warfarin reversal protocol (June 2013) and going backward in time until a 2.5:1 ratio of historical control patients to PCC patients was reached. The 2.5:1 ratio of patients was decided on by the study authors a priori to improve the chances of finding a difference within the study arms without a power analysis. The standard of care for warfarin reversal in the historical control group included vitamin K and FFP without the use of other reversal agents. Blood product administration in both study groups was at the sole discretion of the transplant surgeon. There was no standardization for blood product administration; thus, no limitations or set number of units of a product were mandated to be administered. Finally, there were no major differences in surgical coagulation monitoring between cohorts.
The co-primary objectives of the study were to assess the use of each specific blood product associated with the use of PCC in addition to vitamin K for warfarin reversal prior to heart transplant as compared with a historical control group. Blood product use was defined as the use of packed red blood cells (pRBCs), FFP, cryoprecipitate, or platelets and was measured in units of each product. Blood product use data came from the blood bank to ensure accuracy. Secondary outcomes included the incidence of in-hospital mortality, the need for reoperation for bleeding, all types of thromboembolic events (confirmed by imaging), duration of chest tube use, time to extubation, intensive care unit (ICU) length of stay, and hospital length of stay. Data on blood product use were collected from postoperative day (POD) 0 to POD 2 to ensure accurate collection of pre-transplant, intraoperative, and post-transplant blood products for both cohorts; data on thromboembolic events and reoperation for bleeding were collected from POD 0 to POD 14. POD 0 was defined as beginning at midnight on the day of surgery. The secondary end points of duration of chest tube use, time to extubation, ICU length of stay, and hospital length of stay were assessed starting from POD 0.
PCCs are available in multiple formulations, including activated PCC, 3-factor PCC, and 4-factor PCC, which was recently approved by the Food and Drug Administration (FDA). The main differences between these products are the content of factor VII in each formulation and whether or not factor VII is in an activated or inactivated state (factor VII vs factor VIIa). 4 The product utilized in our study was factor IX complex, also known as Profilnine SD (Grifols Biologicals Inc, Los Angeles, CA), a 3-factor PCC consisting of no more than 150, 35, and 100 units of factors II, VII, and X, respectively, for every 100 units of factor IX.5,6
Normalcy was determined using the Shapiro-Wilk test. Continuous variables were evaluated using t tests or Mann-Whitney U tests, and categorical variables were evaluated using χ2 or Fisher’s exact tests as appropriate. Descriptive statistics were utilized to present patient baseline characteristics. A significance value (α) of 0.05 was used for all statistical calculations and was set a priori.
Results
The study enrolled both adult and pediatric patients; however, the majority of patients included were adults. In all, 16 patients taking warfarin who underwent heart transplant after the introduction of the warfarin reversal protocol were included in the PCC cohort. Two of the patients were adolescents aged 12 and 16, respectively. Of the 16 patients in the PCC cohort, 11 had LVADs as a bridge to transplant. Patients in the PCC cohort underwent surgery between July 2013 and December 2013. The historical control cohort included 50 patients, including 1 5-year-old pediatric patient, all of whom underwent heart transplant between June 2010 and April 2013. Baseline characteristics among groups are outlined in Table 1. Similar to the PCC cohort, most patients in the historical control cohort were on warfarin prior to transplant because of the presence of a VAD. Other indications for anticoagulation in both cohorts included VTE and atrial fibrillation, which was the most common indication. The historical control group had a higher rate of VADs present compared with the PCC group (74% vs 69%). In addition, 1 patient in the historical control group was administered recombinant factor VIIa in the operating room to correct a coagulopathy; unfortunately, the patient died during surgery because of bleeding complications and was included in the analysis because the administration of the other factor product did not have an influence on the patient’s outcome.
Patient Baseline Characteristics. a
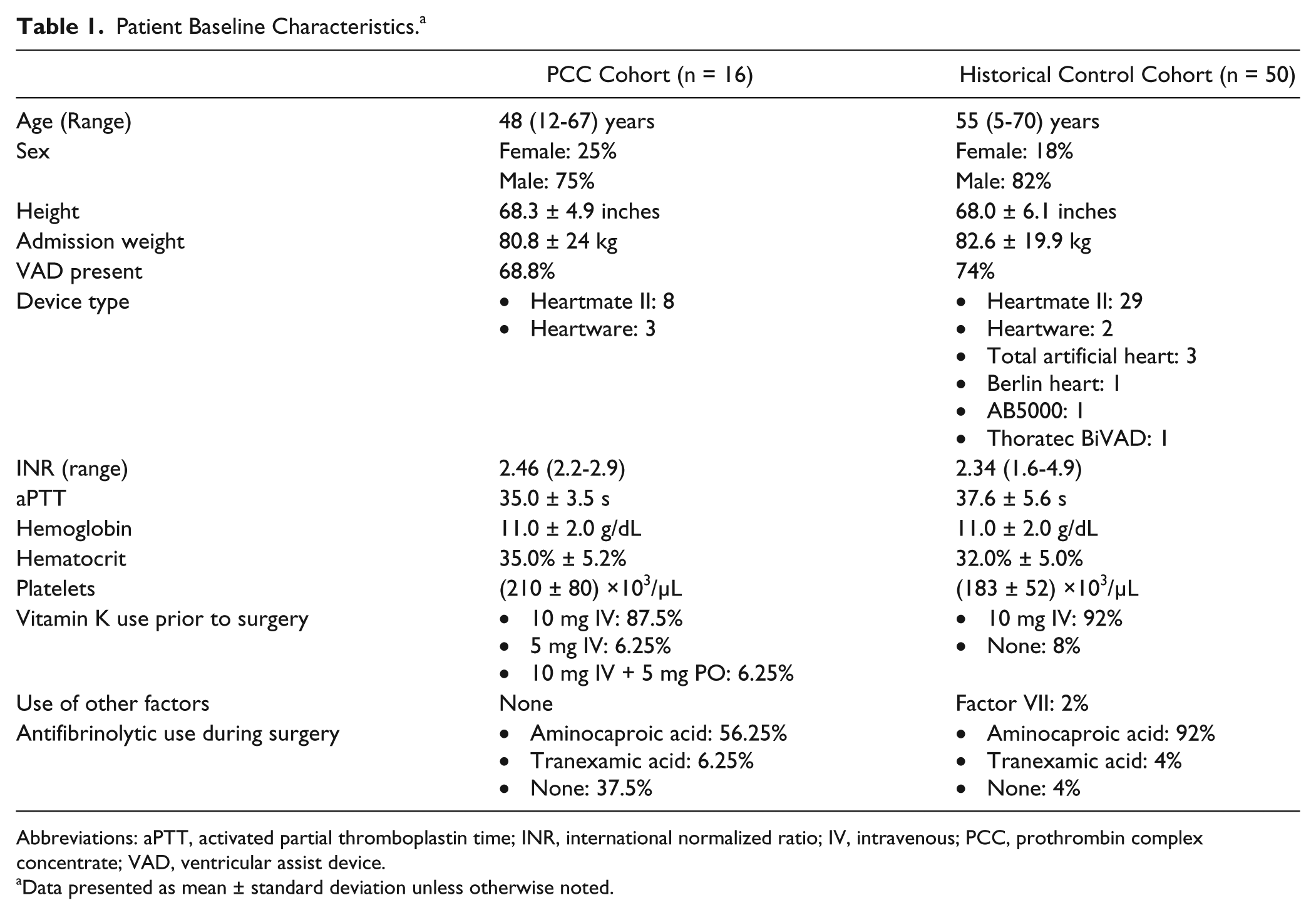
Abbreviations: aPTT, activated partial thromboplastin time; INR, international normalized ratio; IV, intravenous; PCC, prothrombin complex concentrate; VAD, ventricular assist device.
Data presented as mean ± standard deviation unless otherwise noted.
The PCC cohort utilized a mean of 2.1 (standard deviation [SD] = 0.86) doses and 1605 (SD = 649) International Units (IU) per patient prior to surgery at a weight-based mean dose of 19.6 (SD = 5.6) IU/kg. Per our protocol, the goal INR was <1.5; however, that was only achieved in 12% of patients. Three-fourths of patients in the PCC cohort did, however, have an INR of <1.7 prior to transplant. Information regarding INR immediately prior to transplant was not available for the historical control group.
The use of PCC showed a non–statistically significant trend toward reduced use of all blood products (Figure 2). The primary end point of blood product use was not significantly different for pRBCs, cryoprecipitate, or platelets between the PCC cohort and the historical control group; however, a significantly lower use of FFP was seen in the PCC cohort when compared with historical controls (P = 0.0239).
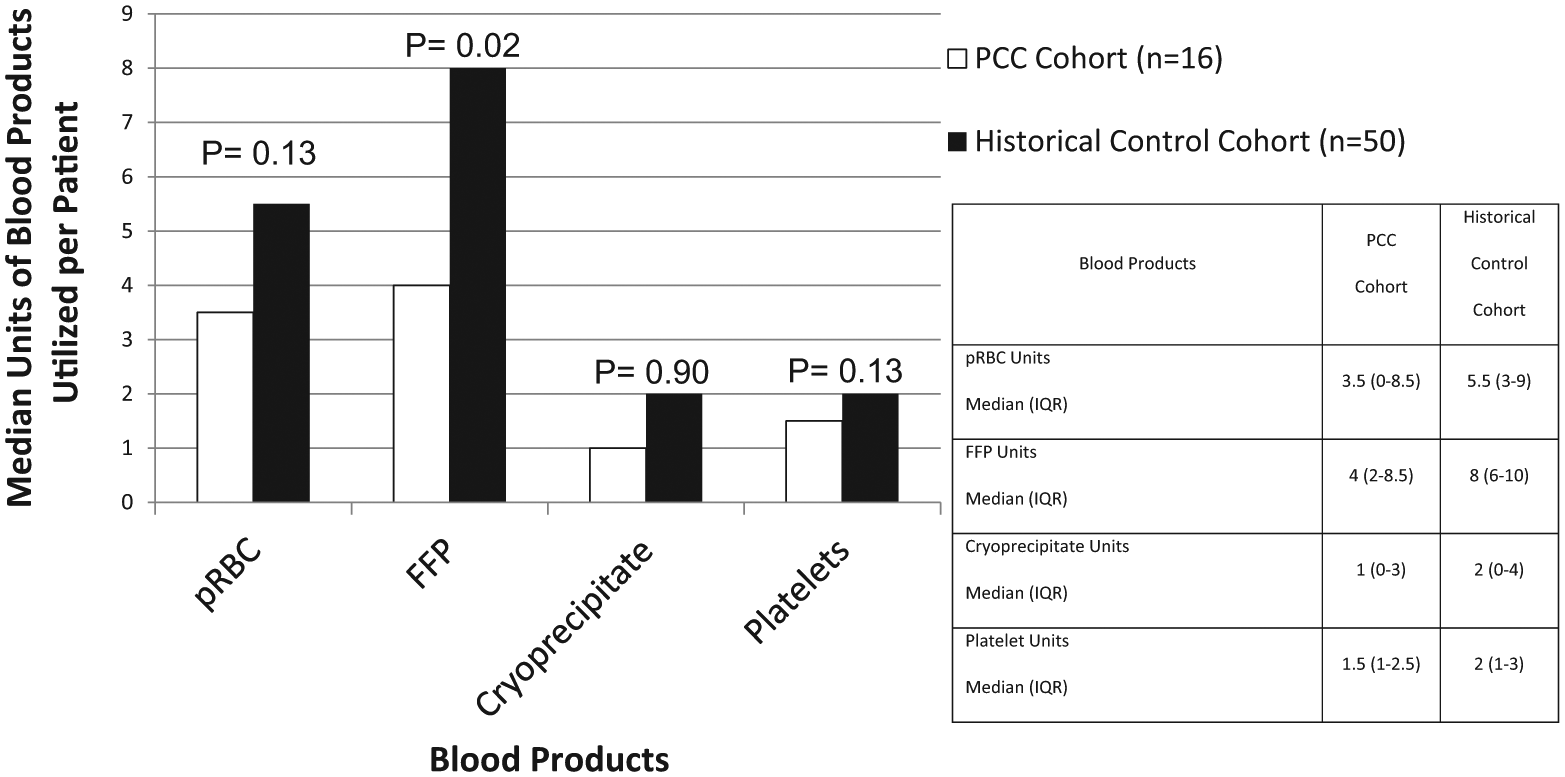
Blood Product Use in Heart Transplant Recipients.
There were no differences between the cohorts regarding any secondary end points (Table 2), including reoperation for bleeding with the use of PCC. There was one reoperation in the PCC cohort, which was attributed to a surgical cause; there were no surgical causes of bleeding identified in the historical control group. Three thrombotic events, all deep venous thromboses (DVTs), were discovered in the PCC cohort on POD 7, 9, and 14, respectively; 5 thrombotic events, 1 left atrial thrombus and 4 DVTs, were discovered in the historical control cohort, with the DVTs being discovered on POD 6, 6, 13, and 14, respectively. Thrombosis rates were not significantly different between cohorts.
Secondary End Points.
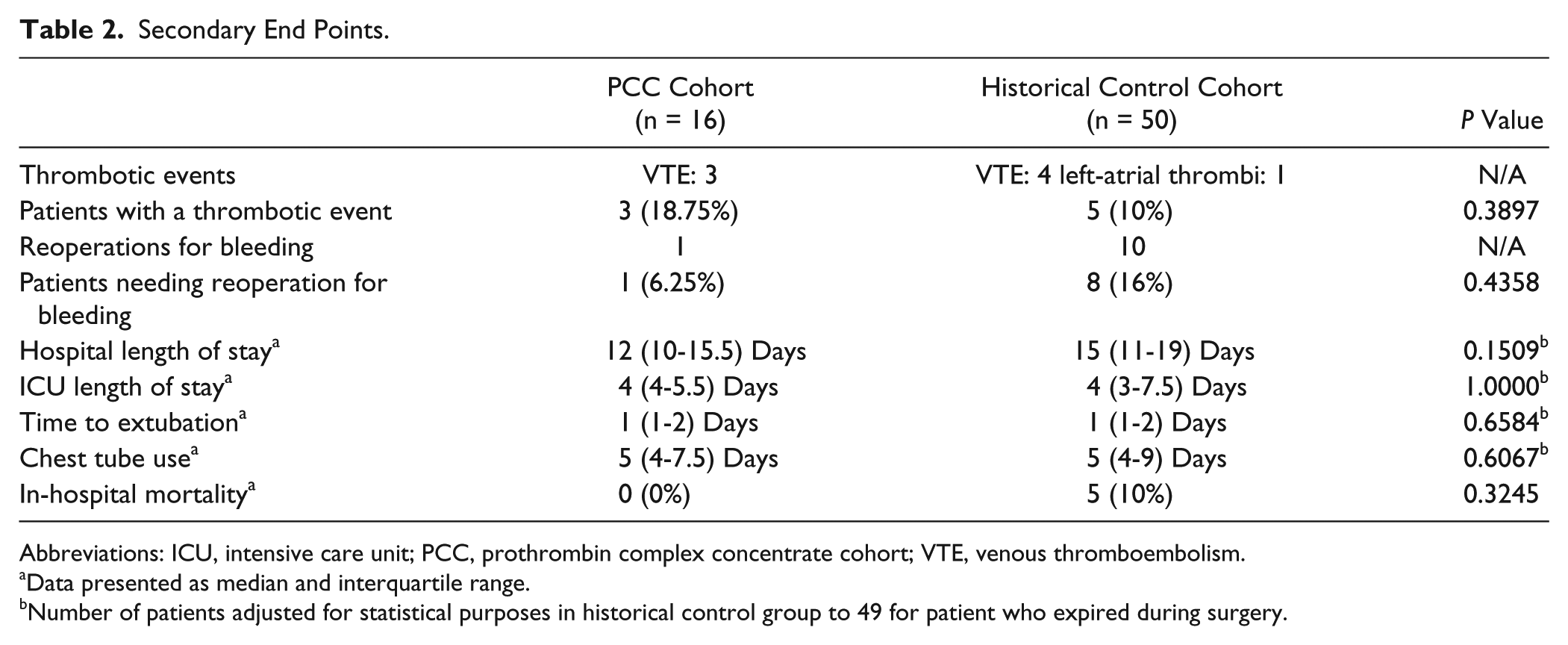
Abbreviations: ICU, intensive care unit; PCC, prothrombin complex concentrate cohort; VTE, venous thromboembolism.
Data presented as median and interquartile range.
Number of patients adjusted for statistical purposes in historical control group to 49 for patient who expired during surgery.
The cost of PCC utilized was approximately $2000 per patient. The mean cost of blood product use per patient was higher in the historical control group compared with the PCC cohort ($4033 vs $2880); however, when adding the cost of PCC utilized, the overall per patient cost was higher in the PCC cohort ($4033 vs $4903).
Discussion
Most PCC data come from use in warfarin reversal for intracranial hemorrhage, but multiple studies have evaluated PCC use prior to surgical procedures. A majority of these studies have evaluated 4-factor PCCs, but Profilnine SD has been reviewed in 2 trials, one of which focused on use prior to heart transplant.7,8 Baggs et al 7 evaluated 50 patients who received Profilnine SD, including 14 where use was for unknown types of emergent surgery. The primary outcome was the difference in initial INR between patients whose INR was adequately reversed (INR <1.5) and those who were not adequately reversed. The median initial dose in patients was approximately 25 IU/kg; some patients did require redosing of PCC, and the primary end point demonstrated that patients with higher INRs are less likely to achieve adequate INR reversal with Profilnine SD and may require higher doses than used in the study. Mathia et al 8 conducted a retrospective chart review comparing historical controls receiving blood products plus vitamin K with those receiving additional PCC per a protocol after its institution at their facility. Patients undergoing heart transplant would receive a standard Profilnine SD dose based on weight and baseline INR. The authors found significant reductions in use in units of pRBCs, FFP, and desmopressin as an adjunctive hemostatic agent. The authors reported a statistically significant reduction in in-hospital mortality in the patients’ post-protocol implementation compared with the pre-protocol controls; however, a limited amount of patients were recruited for the study.
Several limitations exist in our study, including the retrospective nature of this analysis, which inherently introduced bias into the results. As a result of its retrospective nature, our study was unable to identify baseline characteristics in both cohorts that may have influenced outcomes, such as pre-operative antiplatelet use, number of prior sternotomies, surgical approach to transplant, need for anticoagulation post-operatively, type and use of VTE prophylaxis post-operatively, and use of other hemostatic agents post-operatively. Other limitations include differences between the cohorts, such as the use of antifibrinolytic agents. During the evaluation of the PCC cohort, aminocaproic acid was on national shortage. Thus, tranexamic acid temporarily replaced aminocaproic acid in some instances, but antifibrinolytic use varied among surgeons. Also, 38% of patients in the PCC cohort did not receive an antifibrinolytic during surgery compared with just 4% in the control group, which may have led to increased use of blood products in the perioperative period in the PCC group and confounded the results. Also, patients in the historical control cohort had various types of VADs unlike the PCC cohort, which included patients only with the Heartmate II Left Ventricular Assist Device (Thoratec Corporation; San Diego, CA) and the Heartware Ventricular Assist System (Heartware International; Framingham, MA). Bleeding rates may vary among different VAD types during explantation, which may have played a role in blood product use.9-11 Similar differences may be evident with thrombotic complications between devices, which may have been discovered after surgery. Although an increasing rate of pump thrombosis in patients with the Heartmate II LVAD has recently been reported, no incidents of pump thrombosis occurred in either group prior to the time of transplant. 12 Finally, the study was not powered to detect a difference in either the primary or secondary end points.
Profilnine SD was the PCC product utilized for the warfarin reversal protocol. During the study period, Kcentra, a 4-factor PCC became available in the United States. Although, our study protocol did not change with the approval of Kcentra, its effect on warfarin reversal in this population may differ from that of Profilnine SD because of a higher amount of factor VII present in the formulation. 2 Recently, Kcentra added a labeled indication for warfarin reversal prior to urgent surgery or invasive procedures, the only PCC to have such an indication. 13 In addition, studies have evaluated 4-factor PCC use, including those in cardiac surgery, with favorable results. 14 Our institution utilizes Profilnine SD for warfarin reversal prior to heart transplant, but other therapies, including Kcentra, are available. The use of these PCCs has not been explicitly studied in the heart transplant population and warrants further investigation.
Our intent was to produce a protocol that limited PCC doses to minimize exposure and avoid thrombotic events in a potentially high-risk population. The thrombotic events in the PCC cohort were all identified at least 7 days after drug administration. Although PCC may have played a role in the development of these clots, all patients did have multiple other risk factors for the development of VTE. Of the 3 patients who had a thrombotic event in the PCC cohort, only 1 received 3 doses of PCC (mean = 27.4 units/kg). There were no other trends we could identify with the 3 patients that would lead them to have thrombosis compared with the other 13. In addition, intraoperative transesophageal echocardiography and visual inspection of the pump and heart after explantation did not reveal thrombus in any of these patients. Despite PCC being used in multiple patients with VADs, who are at high risk of thrombosis, no patient experienced a thromboembolic event during surgery. Ultimately, our PCC use at 19.6 IU/kg was very similar to that in the study by Mathia et al, 8 which saw a mean PCC dose of 21 IU/kg. Most patients did utilize the second and third doses of PCC available to them in the protocol because INR targets were rarely attained after the initial dose. Even with the administration of the allowable repeat doses, only 12% of patients achieved an INR of <1.5 after PCC administration. Most patients who did not achieve an INR <1.5 did have INRs between 1.5 and 1.7. This finding may lead to alterations in our protocol, with patients not receiving PCC initially unless their INR is >1.7. Another confounding factor was that vitamin K use did not follow protocol in all instances in the PCC cohort. One pediatric patient received only 5 mg of vitamin K, whereas another patient received 15 mg of vitamin K. It is unknown why an extra dose of vitamin K was administered in that patient.
Two major aspects not analyzed in our study which deserve discussion are fluid burden in patients receiving blood products compared with PCC and the immunogenicity of blood products given to patients before or after organ transplant. PCC is usually administered by IV push in very small volumes compared with blood products, which range from 150 to 350 mL per unit. 1 Introducing large volumes of blood products in these patients may lead to increased use of diuretics postoperatively, prolonged ICU and hospital lengths of stay, and respiratory issues. Our study found no differences in ICU and hospital length of stay or time to extubations. Finally, transfusions can cause sensitization after transplant. Introducing donor antibodies post-transplant increases the risk of acute as well as delayed rejection. Although, the use of leukoreduced transfusions reduces the risk, it does not fully eliminate it. 15
Finally, the rapidly changing criteria for selection of heart transplant recipients must be addressed. Choosing the ideal candidate for transplant is a predominant common practice today, compared with transplanting more critically ill patients years ago. This is likely a result of the advances made in mechanical circulatory support in the past decade. With the ever-evolving process of candidate selection biasing toward more stable patients, rates of survival, bleeding, thrombosis, and many others, including the outcomes that we evaluated in our study, are also inherently affected. Our study enrolled patients in the historical control arm from as early as 2009 compared with our PCC cohort who all received transplants in 2013. Although, our 4-year transplant window likely had less of an impact than if patients were selected from the early to mid-2000s, differences likely did still exist that may have influenced outcomes.
Conclusion
This study found that the use of our warfarin reversal protocol significantly reduced the use of FFP compared with a historical control group of patients undergoing heart transplant, without a statistically significant increase in thromboembolic events. Other benefits of utilizing PCC compared with blood products were not evaluated in this study, including blood product immunogenicity and volume issues with transfusions. The overall per patient cost was slightly higher in the PCC cohort, but notwithstanding, our institution now routinely utilizes PCC for warfarin reversal prior to heart transplant. Further studies addressing PCC use prior to heart transplant should be undertaken evaluating other PCC preparations and dosing regimens to optimize dose, administration timing, and cost benefit.
Footnotes
Acknowledgements
The authors would like to acknowledge Larry Kilgore for his assistance in helping obtain accurate blood product counts.
Authors’ Notes
Parts of this study were presented at the 2014 ISHLT Annual Meeting in San Diego, California.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.